Embed Size (px)
Citation preview

Determinants of Colorectal Cancer Screening inWomen Undergoing MammographyDavid H. Stockwell, M.D., Paula Woo, M.D., Brian C. Jacobson, M.D., M.P.H., Renee Remily, M.D.,Sapna Syngal, M.D., M.P.H., Jacqueline Wolf, M.D., and Francis A. Farraye, M.D., M.Sc.Division of Gastroenterology and Department of Internal Medicine, Brigham and Women’s Hospital; DanaFarber Cancer Institute; Division of Gastroenterology, Beth Israel Deaconess Medical Center; Section ofGastroenterology, Boston University Medical Center, Boston, Massachusetts
OBJECTIVES: Women who participate in screening forbreast cancer are more likely to participate in screening forcolorectal cancer. We studied such a motivated group ofwomen to identify predictors of, and barriers to, participa-tion in colorectal cancer screening by endoscopy.
METHODS: We distributed surveys to 551 women� 50 yr ofage while they were awaiting mammography at four sites inand around Boston, MA from June to September, 2000. The40-question survey assessed knowledge, attitudes, and be-liefs about, and behaviors toward, breast and colorectalcancer screening. Regression models were used to deter-mine factors associated with having had sigmoidoscopy orcolonoscopy.
RESULTS: Seventy-nine percent of the women completed allor part of the survey. Half (221/438) reported ever havinghad sigmoidoscopy or colonoscopy. Of these, 93% did so atthe recommendation of their primary care provider. Factorsassociated with participation in endoscopic screening in-cluded compliance with annual fecal occult blood testing, afamily history of colorectal cancer, and indifference towardthe gender of the doctor performing the endoscopy.
CONCLUSIONS: Women undergoing mammography over-whelmingly cite the recommendation of their primary careprovider as the reason for participating in colorectal cancerscreening by endoscopy. Women who preferred a femaleendoscopist were less likely to have been screened. When-ever possible, primary care providers should offer womenthe choice of a female endoscopist for colorectal cancerscreening. (Am J Gastroenterol 2003;98:1875–1880. ©2003 by Am. Coll. of Gastroenterology)
INTRODUCTION
Colorectal cancer is the second leading cause of cancer-related death overall and the third most common cause ofcancer-related death among women in the United States (1).
Despite established and well-publicized colorectal cancerscreening guidelines (2–5), recent studies show that lessthan half of the population participates in colorectal cancerscreening and that women are less likely than men to havehad endoscopic screening with flexible sigmoidoscopy orcolonoscopy (6, 7). Despite the fact that women are as likelyto die from colorectal cancer as men, many women continueto believe that colorectal cancer predominantly affects men(8).
By contrast, during the past decade, women have gainedgreater awareness of breast cancer and have dramaticallyincreased their use of mammography (9–11). Women whoparticipate in breast cancer screening are more likely toparticipate in colorectal cancer screening as well (12). Arecent survey of women in Massachusetts found that currentscreening by mammography was an independent predictorof colorectal cancer screening (13). Even among womenwho undergo mammography, however, colorectal cancerscreening rates are low (12, 13).
We studied a group of women undergoing mammographyto determine their knowledge, attitudes, and beliefs aboutand behaviors toward colorectal cancer screening. Our goalwas to identify determinants of colorectal cancer screeningin women already participating in cancer screening in thehope of discovering motivational factors that might apply toall women.
MATERIALS AND METHODS
We offered surveys to 551 women 50 yr of age and olderwhile they were attending mammography clinics betweenJune and September, 2000. Sites of recruitment included awomen’s health clinic in an affluent Boston suburb (TheSpence Center, Wellesley, MA), two multispecialty officesin urban communities (Harvard Vanguard Medical Associ-ates, West Roxbury and Quincy, MA), and a tertiary carehospital (Brigham and Women’s Hospital, Boston, MA). Acover letter explained the nature and purpose of the study,and informed consent was granted by completion of thesurvey. The study was approved by the institutional reviewboard at each location. The survey was available in English-
Portions of this study were presented at Digestive Diseases Week, May 20–23,2001, in Atlanta, Georgia and published in abstract form (Gastroenterology 2001;120(suppl 1):AB3067 and AB3072).
THE AMERICAN JOURNAL OF GASTROENTEROLOGY Vol. 98, No. 8, 2003© 2003 by Am. Coll. of Gastroenterology ISSN 0002-9270/03/$30.00Published by Elsevier Inc. doi:10.1016/S0002-9270(03)00426-X

and Spanish-language versions and consisted of 40 ques-tions assessing 1) patient demographics, 2) screening be-haviors for breast, cervical, and colorectal cancer, 3) per-sonal and family histories of cancer, colonic polyps, andinflammatory bowel disease, 4) general knowledge aboutbreast and colorectal cancer, 5) overall health and utilizationof health care, 6) knowledge of cancer screening guidelines,and 7) reasons for participating or not in endoscopic screen-ing for colorectal cancer. Each question was followed bythree to six possible responses. Several questions specifi-cally stated that more than one correct answer could bechosen. Questions that were left unanswered were consid-ered to be negative responses.
In univariate analysis, Fisher’s exact test was used to testthe relationship between each independent variable and theoutcome of colorectal cancer screening status by sigmoid-oscopy or colonoscopy. Logistic regression was used tomodel the association between colorectal cancer screeningstatus and the covariates that were related to the outcome inunivariate analysis with a p value � 0.05. In the logisticregression model, two-sided p values � 0.05 were consid-ered significant, and the results are presented as odds ratioswith 95% confidence intervals. Calculations were performedwith SAS version 6.12 software (SAS Institute, Cary, NC).
RESULTS
Patient DemographicsOf 551 women aged 50 yr or older who underwent mam-mography during the study, 438 (79%) completed part or allof the survey and were included in our analysis. The medianage was 58.4 yr (range 50–87). Study population charac-teristics are shown in Table 1.
History of Cancer ScreeningThe purpose of the current mammogram was routine cancerscreening for 83% of the study population, and 75% re-ported having mammograms on an annual basis. Nearly half(45%) had fecal occult blood testing before age 50 yr, 47%had fecal occult blood testing on an annual basis, and 69%had undergone fecal occult blood testing at least once. Halfhad undergone sigmoidoscopy or colonoscopy at least once.Of those who had undergone sigmoidoscopy or colonoscopy(n � 221), 25% had done so before age 50 yr, and 53% haddone so between the ages of 50 and 60 yr. Just over half(54%) of the women who reported ever having had sigmoid-oscopy or colonoscopy reported having repeat sigmoidos-copy or colonoscopy at least every 5 yr.
History of CancerExcluding skin cancer, 9% of the study population reporteda personal history of cancer. Overall, 4% reported a personalhistory of breast cancer, and 1% reported a personal historyof colorectal cancer. In first-degree relatives, 16% reporteda family history of breast cancer, and 9% reported a familyhistory of colorectal cancer.
Knowledge of Breast and Colorectal Cancer andScreening Recommendations
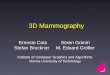
To assess their knowledge about cancer risk, we askedsurvey participants to estimate the average American wom-an’s lifetime risk of developing breast and colorectal cancer,and the results are presented in Figure 1. We also askedgeneral questions about breast and colorectal cancer. Atleast 75% said that colorectal cancer was not more commonin men, that colorectal cancer could be cured if detected atan early stage, that colorectal cancer screening saves lives,and that colorectal cancer may be asymptomatic. More than80% were correct when asked similar questions about breastcancer. However, only 49% agreed with the statement, “Re-moval of noncancerous polyps prevents colorectal cancer.”
Many thought that mammography and fecal occult bloodtesting should begin at younger ages than are actually rec-ommended. Half (52%) thought that mammography shouldfirst be done between the ages of 30 and 40 yr, and 46%thought that fecal occult blood testing should first be done atage 40 yr. The majority thought that mammograms (74%)and fecal occult blood testing (73%) should be repeatedevery year. Slightly more than half (55%) knew that sig-moidoscopy or colonoscopy is first recommended at 50 yr ofage for average-risk individuals, and 57% said that sigmoid-oscopy or colonoscopy should be repeated every 5 yr. Only19% thought that sigmoidoscopy or colonoscopy shouldfirst be done at age 40 yr.
Table 1. Patient Characteristics
Variable n (%)
Age (yr)50–59 245 (56)60–69 120 (27)70–79 62 (14)80� 11 (3)
Race/ethnicityCaucasian 346 (79)African American 47 (11)Hispanic 7 (1)Asian 8 (1)Other 30 (7)
Education levelGrade school 27 (6)High school 158 (36)College or higher 241 (55)Other 12 (3)
Annual household income�$15,000 28 (6)$15–$25,000 36 (8)$25–$50,000 89 (20)$50–$75,000 96 (22)�$75,000 115 (26)Not reported 74 (17)
Type of insurancePrivate 350 (80)Medicaid/Medicare 31 (7)Other 57 (13)
1876 Stockwell et al. AJG – Vol. 98, No. 8, 2003

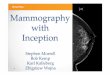
Motivation for Colorectal Cancer ScreeningOf women who had sigmoidoscopy or colonoscopy (n �221), 93% did so at the recommendation of their primarycare provider. The remainder did so at the recommendationof the media (3%), a family member (3%), or a friend (1%)(Fig. 2). Conversely, women who had not had sigmoidos-copy or colonoscopy (n � 217) most often cited lack of arecommendation from their doctor as the reason (36%).Other reasons for not having sigmoidoscopy or colonoscopyincluded fear of pain or discomfort (25%), embarrassment(14%), inconvenience (11%), expense (3%), and fear of theresults (2%).
Half (221) of the women that we surveyed said they hadbecome more aware of the risks of colorectal cancer and ofthe importance of screening in the previous year. Of thosewho reported recent increased awareness, 58% had not beenscreened, 34% had already been screened, and 12% saidthey had, as a result of increased awareness, been screened.
Preference for Gender of Physician PerformingSigmoidoscopy/ColonoscopyMost (69%) did not care about the gender of the doctorperforming their endoscopy. However, 30% preferred hav-
ing a female doctor perform their endoscopy. Only 1%preferred a male doctor.
Factors Associated With Endoscopic Colorectal CancerScreeningUnivariate predictors of ever having had sigmoidoscopy orcolonoscopy are presented in Table 2. Having had fecaloccult blood testing by age 60 yr and having fecal occultblood testing on an annual basis were both associated withhaving had sigmoidoscopy or colonoscopy. Both a personaland a family history of cancer in a first-degree relative wereassociated with having had sigmoidoscopy or colonoscopy.Women who agreed with the statement, “Removal of non-cancerous polyps prevents colorectal cancer” were signifi-cantly more likely to have had sigmoidoscopy or colonos-copy than were those who did not. Finally, women whoeither preferred a male endoscopist or who did not careabout the gender of the doctor performing their sigmoidos-copy or colonoscopy were significantly more likely to havebeen screened than were those who preferred to have afemale endoscopist perform the test.
In multivariate analysis, independent predictors of everhaving had sigmoidoscopy or colonoscopy were compliancewith annual fecal occult blood testing, a family history ofcancer, and indifference toward the gender of the doctorperforming the test (Table 3).
DISCUSSION
We surveyed a large group of relatively affluent women atleast 50 yr of age who were undergoing mammography andfound high rates of fecal occult blood testing and sigmoid-oscopy or colonoscopy. As in other studies of the relation-ship between breast and colorectal cancer screening, wefound that women undergoing mammograms had a rate ofcolorectal cancer screening by fecal occult blood testing andsigmoidoscopy or colonoscopy higher than the national av-
Figure 1. Study subjects’ responses to the question, “What, would you guess, is the average American woman’s lifetime risk of can-cer?” .
Figure 2. Study subjects’ responses to the question, “ If you havehad sigmoidoscopy or colonoscopy, who recommended it?” .
1877AJG – August, 2003 Colorectal Cancer Screening and Mammography

erage (12, 13). Nearly half (47%) of the women surveyedreported compliance with annual fecal occult blood testing.Half had undergone sigmoidoscopy or colonoscopy at leastonce, and 54% of those reported ongoing use of sigmoid-oscopy or colonoscopy at 5-yr intervals. These women wereknowledgeable about both breast and colorectal cancer and,in fact, tended to overestimate cancer risk and to underes-timate the age at which cancer screening should begin. Theoverwhelming majority of women who had been screenedfor colorectal cancer with sigmoidoscopy or colonoscopydid so at the recommendation of their primary care provider.In multivariate analysis, women who preferred a femaleendoscopist were less likely to have been screened by sig-moidoscopy or colonoscopy.
These women cited the recommendation of their primarycare provider overwhelmingly as the reason for undergoingsigmoidoscopy or colonoscopy. Conversely, women whohad not had sigmoidoscopy or colonoscopy most commonlyidentified the lack of a doctor’s recommendation as thereason. The critical role of the primary care provider inmotivating women to participate in colorectal cancer screen-ing has been demonstrated previously (14–16). By contrast,only a small number of the women we surveyed cited themedia as the most important influence on their behavior.However, half said they had recently become more aware ofthe risks of colorectal cancer, and 12% of these had beenscreened as a result. In the months before our survey, therewas an important increase in publicity surrounding colorec-tal cancer screening (17). Indeed, a recent report trackingnationwide rates of colonoscopy credits this publicity, high-lighted by Katie Couric’s live colonoscopy on NBC’s TodayShow in March, 2000, with a near 20% increase in thenumber of people undergoing colonoscopy (18). Still, thewelcome influence of high-profile celebrity attention should
not diminish the importance of the primary care provider’srecommendation as the main determinant of screening be-havior for the vast majority of women.
Recent studies have shown that high-risk women with thehighest risk perception may actually participate in screeningfor both breast and colorectal cancer at lower than expectedrates (19, 20). The prevalence of breast and colon cancerreported by the women in our study is similar to the nationalaverage. Even though these women overestimated the riskof breast and colorectal cancer, they participated in cancerscreening at high rates. They also thought that screening foraverage-risk people, especially fecal occult blood testing,should begin earlier than the 50 yr of age that is actuallyrecommended. Indeed, other investigators have found that,in some populations, cancer screening is initiated at inap-propriately young ages. A recent study of primary carephysicians in Florida found that, for average-risk womenless than 50 yr old, recommendation was high for both fecaloccult blood testing (82%) and sigmoidoscopy (28%) (21).It is quite possible, therefore, that in highly motivated,educated, urban, and affluent groups of women such asthese, further general education about colorectal cancer riskand the importance of screening may not significantly im-prove screening behavior.
Male physicians are reported to be less likely than femalephysicians to refer their female patients for cervical andbreast cancer screening (22, 23). Other studies have showna gender bias in terms of rates of referral for both diagnosticand screening sigmoidoscopy (24, 25). We did not ask aboutthe gender of the referring providers and, therefore, cannotevaluate this potential bias. However, we did identify an-other type of bias that stems from the patient rather thanfrom the physician. A significant minority of women havebeen shown to prefer female primary care physicians, breast
Table 2. Univariate Predictors of Colorectal Cancer Screening by Sigmoidoscopy/Colonoscopy
Variable
Screened(n � 221)
n (%)
Not Screened(n � 217)
n (%) p
Annual fecal occult blood testing 122 (64) 53 (36) 0.005Preference for a female endoscopist 39 (23) 44 (38) 0.01Family history of cancer 124 (65) 73 (50) 0.01Personal history of cancer 40 (21) 15 (10) 0.01Agreement with the statement, “Removal of noncancerous polyps
prevents colorectal cancer”113 (60) 63 (45) 0.01
Fecal occult blood testing by age 60 yr 147 (77) 91 (65) 0.02
Table 3. Multivariate Predictors of Colorectal Cancer Screening by Sigmoidoscopy/Colonoscopy
Variable Odds Ratio (95% CI) p
Annual fecal occult blood testing 4.0 (2.2–7.3) 0.005Preference for a female endoscopist 0.4 (0.2–0.8) 0.01Family history of cancer 2.0 (1.1–3.6) 0.02Personal history of cancer 1.7 (0.8–3.9) 0.19Agreement with the statement, “Removal of noncancerous polyps
prevents colorectal cancer”1.6 (0.9–2.8) 0.12
Fecal occult blood testing by age 60 yr 1.1 (0.6–2.3) 0.72
1878 Stockwell et al. AJG – Vol. 98, No. 8, 2003

cancer surgeons, and gynecologists (26–28). In two previ-ous studies of patient preferences in the setting of colonos-copy, investigators found that 43% and 48% of womenpreferred a female endoscopist, whereas very few men hada gender preference (29, 30). We found not only that manywomen preferred a female endoscopist but that women whopreferred a female endoscopist were significantly less likelyto have been screened. Because we did not ask this subgroupof women why they had not been screened, it remainsunclear whether the barrier to screening resulted primarilyfrom their own attitudes and perceptions or if it resultedfrom shortcomings in the delivery of sigmoidoscopy andcolonoscopy. Women comprise only a small minority ofgastroenterologists, despite a slow increase in recent years(31). In many places, it is very likely that there simply arenot enough female endoscopists to meet the needs of allwomen who would prefer one. However, our study popu-lation was mainly served by a group of gastroenterologistsin which 31% (5/16) were women. Therefore, some womenmay not have been screened for colorectal cancer simplybecause they were not asked if they preferred a femaleendoscopist.
Despite purposefully selecting women undergoing breastcancer screening, our findings are consistent with priorstudies that identified primary care physician recommenda-tion, perceived risk, and family history of cancer as impor-tant motivators for colorectal cancer screening (16, 32, 33).Still, our study does have several important limitations.Despite attempting to recruit a more diverse population, therespondents to the survey were largely urban, educated,insured, affluent, and white. In addition, in women who hadhad sigmoidoscopy or colonoscopy, we did not ask whetherthe test was done for screening, surveillance, or other pur-poses, and we did not distinguish between sigmoidoscopyand colonoscopy. We did not ask about other, less commonmethods of colorectal cancer screening, such as bariumenema or “virtual colonoscopy,” and we did not assess theimpact of less invasive and experimental technologies thatmay soon be available, such as stool DNA testing. Finally,the instrument that we created for this study has not beentested in other populations. Although the results may notapply to women who do not participate in breast cancerscreening, our very high response rate suggests that thesefindings are generalizable to similar populations of highlymotivated women.
In summary, we confirmed that women undergoing mam-mography participate in screening for colorectal cancer athigher than average rates. These women were knowledge-able about colorectal cancer, but they tended to overestimatethe risk of cancer and to underestimate the age at whichcancer screening is recommended. Although half of ourrespondents reported increased awareness of the importanceof colorectal cancer screening in the months before thesurvey, almost all cited the recommendation of their primarycare provider as the reason for undergoing sigmoidoscopyor colonoscopy. Finally, women who preferred to have a
female endoscopist perform their sigmoidoscopy orcolonoscopy were significantly less likely to have beenscreened. Whenever possible, women should be offered thechoice of a female endoscopist.
ACKNOWLEDGMENTS
Financial support for this research was provided by anunrestricted gift to J. W. from her patient, Mrs. PhyllisLeBoff, and her husband, Mr. Gerald LeBoff. We thankthem for their support. We also thank Peter Gaccione for hishelp with the statistical analysis, and the staff and patients inthe mammography units at Brigham and Women’s Hospital,Harvard Vanguard Medical Associates, and the Spence Cen-ter who made this study possible.
Reprint requests and correspondence: David H. Stockwell,M.D., Brigham and Women’s Hospital, Division of Gastroenter-ology, 75 Francis Street, Boston, MA 02115.
Received Oct. 15, 2002; accepted Feb. 6, 2003.
REFERENCES
1. Greenlee RT, Hill-Harmon MB, Murray T, Thun M. Cancerstatistics, 2001. CA Cancer J Clin 2001;51:15–36.
2. US Preventive Services Task Force. Screening for colorectalcancer. Guide to clinical preventive services. 2nd edition.Washington, DC: US Government Printing Office, 1996:89–103.
3. Smith RA, von Eschenbach AC, Wender R, et al. AmericanCancer Society guidelines for the early detection of cancer:Update of early detection guidelines for prostate, colorectal,and endometrial cancers. CA Cancer J Clin 2001;51:38–75.
4. Winawer SJ, Fletcher RH, Miller L, et al. Colorectal cancerscreening: Clinical guidelines and rationale. Gastroenterology1997;112:594–642.
5. Rex DK, Johnson DA, Lieberman DA, et al. Colorectal cancerprevention 2000: Screening recommendations of the AmericanCollege of Gastroenterology. Am J Gastroenterol 2000;95:868–77.
6. Centers for Disease Control and Prevention. Screening forcolorectal cancer—United States, 1997. MMWR Morb MortalWkly Rep 1999;48:116–21.
7. Centers for Disease Control and Prevention. Trends in screen-ing for colorectal cancer—United States, 1997 and 1999.MMWR Morb Mortal Wkly Rep 2001;50:162–6.
8. Donovan JM, Syngal S. Colorectal cancer in women: Anunderappreciated but preventable risk. J Womens Health1998;7:45–8.
9. Centers for Disease Control and Prevention. Self-reported useof mammography among women aged � 40 years—UnitedStates, 1989 and 1995. MMWR Morb Mortal Wkly Rep 1997;46:937–41.
10. Centers for Disease Control and Prevention. Surveillance foruse of preventive health-care services by older adults, 1995–1997. MMWR Morb Mortal Wkly Rep 1999;48:51–88.
11. Blackman DK, Bennett EM, Miller DS. Trends in self-re-ported use of mammograms (1989–1997) and Papanicolaoutests (1991–1997)—Behavioral Risk Factor Surveillance Sys-tem. MMWR Morb Mortal Wkly Rep 1999;48(suppl 6):1–22.
12. Shapiro JA, Seeff LC, Nadel MR. Colorectal cancer-screening
1879AJG – August, 2003 Colorectal Cancer Screening and Mammography

tests and associated health behaviors. Am J Prev Med 2001;21:132–7.
13. Lemon S, Zapka J, Puleo E, et al. Colorectal cancer screeningparticipation: Comparisons with mammography and prostate-specific antigen screening. Am J Public Health 2001;91:1264–72.
14. Burke W, Beeker C, Kraft JM, Pinsky L. Engaging women’sinterest in colorectal cancer screening: A public health strat-egy. J Womens Health Gend Based Med 2000;9:363–71.
15. Ruffin MT, Gorenflo DW, Woodman B. Predictors of screen-ing for breast, cervical, colorectal, and prostatic cancer amongcommunity-based primary care practices. J Am Board FamPract 2000;13:1–10.
16. Vernon SW. Participation in colorectal cancer screening: Areview. J Natl Cancer Inst 1997;89:1406–22.
17. NCI Press Office. The National Cancer Institute presents KatieCouric with second annual Eleanor Nealon extraordinary com-municators award at NIH on May 18, 2001. Bethesda, MD:NCI Office of Communications.
18. Abergavenny RD. Broadcast of star’s colonoscopy boostsscreening [in bmj.com news roundup]. Br Med J 2002;324:1118.
19. Blalock SJ, DeVellis BM, Afifi RA, Sandler RS. Risk percep-tions and participation in colorectal cancer screening. HealthPsychol 1990;9:792–806.
20. Lerman C, Lustbader E, Rimer B, et al. Effects of individu-alized breast cancer risk counseling: A randomized trial. J NatlCancer Inst 1995;87:286–92.
21. Richards C, Klabunde C, O’Malley M. Physicians’ recom-mendations for colon cancer screening in women: Too muchof a good thing? Am J Prev Med 1998;15:246–9.
22. Levy S, Dowling P, Boult L, et al. The effect of physician and
patient gender on preventive medicine practices in patientsolder than fifty. Fam Med 1992;24:58–61.
23. Lurie N, Slater J, McGovern P, et al. Preventive care forwomen: Does the sex of the physician matter? N Engl J Med1993;329:478–82.
24. Herold AH, Riker AI, Warner EA, et al. Evidence of genderbias in patients undergoing flexible sigmoidoscopy. CancerDetect Prev 1997;21:141–7.
25. Schapira DV, Pamies RJ, Kumar NB, et al. Cancer screening:Knowledge, recommendations, and practices of physicians.Cancer 1993;71:839–43.
26. Kerssens JJ, Jozien MB, Andela MG. Patient preferences forgender of health professionals. Soc Sci Med 1997;44:1531–40.
27. Reid I. Patient’s preference for male or female breast sur-geons: Questionnaire study. Br Med J 1998;317:1051.
28. Haar E, Halitsky V, Stricker G. Factors related to the prefer-ence for a female gynecologist. Med Care 1975;13:782–90.
29. Fidler H, Hartnett A, Cheng Man K, et al. Sex and familiarityof colonoscopists: Patient preferences. Endoscopy 2000;32:481–2.
30. Varadarajulu S, Petruff C, Ramsey W. Patient preferencesfor gender of endoscopists. Gastrointest Endosc 2002;56:170 –3.
31. Elta GH. Women are different from men [editorial]. Gastroi-ntest Endosc 2002;56:308–9.
32. Kelly RB, Shank JC. Adherence to screening flexible sigmoid-oscopy in asymptomatic patients. Med Care 1992;30:1029–42.
33. Lewis SF, Jensen NM. Screening sigmoidoscopy: Factorsassociated with utilization. J Gen Intern Med 1996;11:542–4.
1880 Stockwell et al. AJG – Vol. 98, No. 8, 2003