Embed Size (px)
DESCRIPTION
Fetomaternal Hemorrhage
Citation preview

Detection of fetomaternal hemorrhageYeowon A. Kim* and Robert S. Makar
The prevention of Rhesus D alloimmunization through Rh immune globulin (RhIg) administration is themajor indication for the accurate detection and quantification of fetomaternal hemorrhage (FMH). In the set-ting of D incompatibility, D-positive fetal cells can sensitize the D-negative mother, resulting in maternalanti-D alloantibody production. These anti-D alloantibodies may lead to undesirable sequelae such as he-molytic disease of the newborn (HDN). Since the widespread adoption of FMH screening and RhIg immuno-prophylaxis, the overall risk of Rh alloimmunization and infant mortality from HDN has substantiallydecreased. The rosette screen, the initial test of choice, is highly sensitive in qualitatively detecting 10 mLof fetal whole blood in the maternal circulation. As the screen is reliant on the presence of the D antigen todistinguish fetal from maternal cells, it cannot be used to detect FMH in D-positive mothers or in D-negativemothers carrying a D-negative fetus. The Kleihauer-Betke acid-elution test, the most widely used confirma-tory test for quantifying FMH, relies on the principle that fetal RBCs contain mostly fetal hemoglobin (HbF),which is resistant to acid-elution whereas adult hemoglobin is acid-sensitive. Although the Kleihauer-Betketest is inexpensive and requires no special equipment, it lacks standardization and precision, and may notbe accurate in conditions with elevated F-cells. Anti-HbF flow cytometry is a promising alternative, althoughits use is limited by equipment and staffing costs. Hematology analyzers with flow cytometry capabilitiesmay be adapted for fetal cell detection, thus giving clinical laboratories a potentially attractive automated al-ternative for quantifying FMH. Am. J. Hematol. 87:417–423, 2012. VVC 2011 Wiley Periodicals, Inc.
IntroductionThe accurate detection and quantification of fetal red
blood cells (RBCs) in the maternal circulation are neces-sary for the prevention of Rhesus D alloimmunizationamong D-negative women because of fetomaternal hemor-rhage (FMH). In the setting of D incompatibility, D-positivefetal cells may result in sensitization of the D-negativemother and subsequent maternal anti-D alloantibody pro-duction. These anti-D alloantibodies may be clinically silentor lead to severe consequences such as hemolysis, fetalanemia, hydrops fetalis, or even death for the current and/or future pregnancies. Although this paper focuses specifi-cally on the detection of FMH for the prevention of D-alloimmunization, FMH testing is also used in the obstetric-gynecological setting for determining the presence of occultbleeding associated with various obstetrical events andconditions [1]. Commercially available Rh immune globulins(RhIg), which are human immunoglobulin preparations fromplasma of donors with high-titer anti-D antibodies, havebeen shown to be effective in reducing D-sensitization andsubsequent hemolytic disease of the newborn (HDN).Before the widespread adoption of FMH screening andimmunoprophylaxis with anti-D immunoglobulin, the inci-dence of infant mortality from HDN in England and Walesin 1970 was 1.2 per 1,000 births. By 1989, this figuredropped to 0.02 per 1,000 births [2]. As appropriate dosingis calculated based on the volume of FMH, the prompt andaccurate laboratory assessment of FMH is highly desirable.One vial (300 lg) of RhIg is sufficient to protect against
30 mL of fetal whole blood or 15 mL of fetal RBCs. At 20weeks gestational age, the fetoplacental blood volume isestimated to be 30 mL [1]. Since transplacental hemor-rhage exceeding 1 mL of fetal RBCs during the antenatalperiod is extremely unlikely [3,4], it is thought that a singlevial is sufficient for antenatal prophylaxis at 28 weeks ges-tational age. In contrast, FMH during term delivery canexceed 30 mL of fetal whole blood, albeit at a low fre-quency (0.3% of pregnancies), requiring accurate quantifi-cation and more than one vial of RhIg to prevent alloimmu-nization [5]. Ramsey, on behalf of the College of AmericanPathologists Transfusion Medicine Resource Committee,
evaluated the results of the College of American Patholo-gists’ (CAP) proficiency testing for fetal RBC detection sub-mitted by nearly 1,600 laboratories. He found that 20%–30% of laboratories underestimated the necessary dose ofRhIg and concluded that laboratories should re-examinetheir protocols and training for calculating RhIg dosage [6].The purpose of this brief review article is to provide a tar-geted overview of the current methods available for thedetection and quantification of FMH and their diagnosticlimitations, as well as special circumstances which mayinfluence test selection and the interpretation of results.
Qualitative Screens for Detection of Fetal RBCs inMaternal Circulation
Rosette screenThe rosette screen is a highly sensitive method to quali-
tatively detect 10 mL or more of fetal whole blood, or 0.2%fetal cells (volume/volume) in the maternal circulation. Ithas largely replaced the microscopic weak D test for thispurpose because of its superior sensitivity [7–9] and is cur-rently the only screening test that is FDA-approved for clini-cal use in the United States. In 1982, Sebring and Poleskyfirst described the formation of microscopic fetal D1 aggre-gates upon incubation of fetal cells with enzyme-treatedgroup O D-positive indicator RBCs and reagent anti-Dserum [10]. The fetal cells must be D-positive and thematernal cells D-negative for the test to be valid. In therosette screen, a maternal blood sample is first incubated
Conflict of interest: Nothing to report.
*Correspondence to: Yeowon A. Kim, Department of Pathology, Warren 2,Massachusetts General Hospital, Boston, MA 02114.E-mail: [email protected]
Department of Pathology, Massachusetts General Hospital, Harvard MedicalSchool, Boston, Massachusetts
Received for publication 28 October 2011; Revised 8 November 2011;Accepted 10 November 2011
Am. J. Hematol. 87:417–423, 2012.
Published online 16 November 2011 in Wiley Online Library (wileyonlinelibrary.com).DOI: 10.1002/ajh.22255
AJH Educational Material Test of the Month
VVC 2011 Wiley Periodicals, Inc.
American Journal of Hematology 417 http://wileyonlinelibrary.com/cgi-bin/jhome/35105
with anti-D and then washed. The indicator D-positiveRBCs are added and the sample is examined under a lightmicroscope. In the presence of fetal D-positive cells, the in-dicator cells will form aggregates (or rosettes) around thefetal cells (Fig. 1). The rosette test may be falsely positiveif the mother has a variant of the D antigen known as weakD, and falsely negative if the fetus/neonate is weak D (vari-ant D antigens are discussed at greater length below in thesection describing flow cytometry to detect D-positiveRBCs). In addition, if the mother has a positive direct anti-globulin test (DAT) such as in the presence of an RBC au-toantibody, the screening test may be false positivebecause of crosslinking and agglutination of the mother’santibody coated cells.If the rosette test is negative, one vial (300 lg) of RhIg is
sufficient to prevent immunization in 99% of patients [11]. Apositive rosette test, which indicates a FMH exceeding 10mL, requires quantification of the FMH by either the Kleiha-uer-Betke acid elution test or flow cytometry to determinethe dose of RhIg required for prophylaxis. In the case of aknown weak D phenotype of the fetus/neonate, a quantita-tive test that does not rely on the level of expression of theD antigen, such as the Kleihauer-Betke test or flow cytome-try using anti-fetal hemoglobin (anti-HbF) antibodies, shouldbe conducted rather than the rosette test. Among motherswith the O blood group carrying fetuses with the A, B, orAB blood group, naturally occurring isohemagglutinins willexpedite the clearance of fetal cells in the maternal circula-tion prior to testing. Therefore, in the setting of anticipatedABO incompatibility, prompt testing around the time of sus-pected FMH is recommended.The rosette test is inexpensive, straightforward and easy
to perform, and does not require special equipment beyonda waterbath, centrifuge, and light microscope. Hence, it canbe conducted around-the-clock with a turnaround time of1–2 hr. FDA-approved, commercially available kits includethe Fetal Bleed Screening Test (ImmucorGamma, Nor-cross, GA), which is the most widely used kit in the UnitedStates, and the FetalScreen II/Fetal Maternal ScreeningTest (Ortho-Clinical Diagnostics, Raritan, NJ) [12]. As therosette test is reliant on the presence of the D antigen todistinguish fetal from maternal cells, it cannot be used todetect FMH in D-positive mothers, or D-negative motherscarrying a D-negative fetus.
Quantitative Tests for Measuring Fetal RBCsin Maternal Circulation
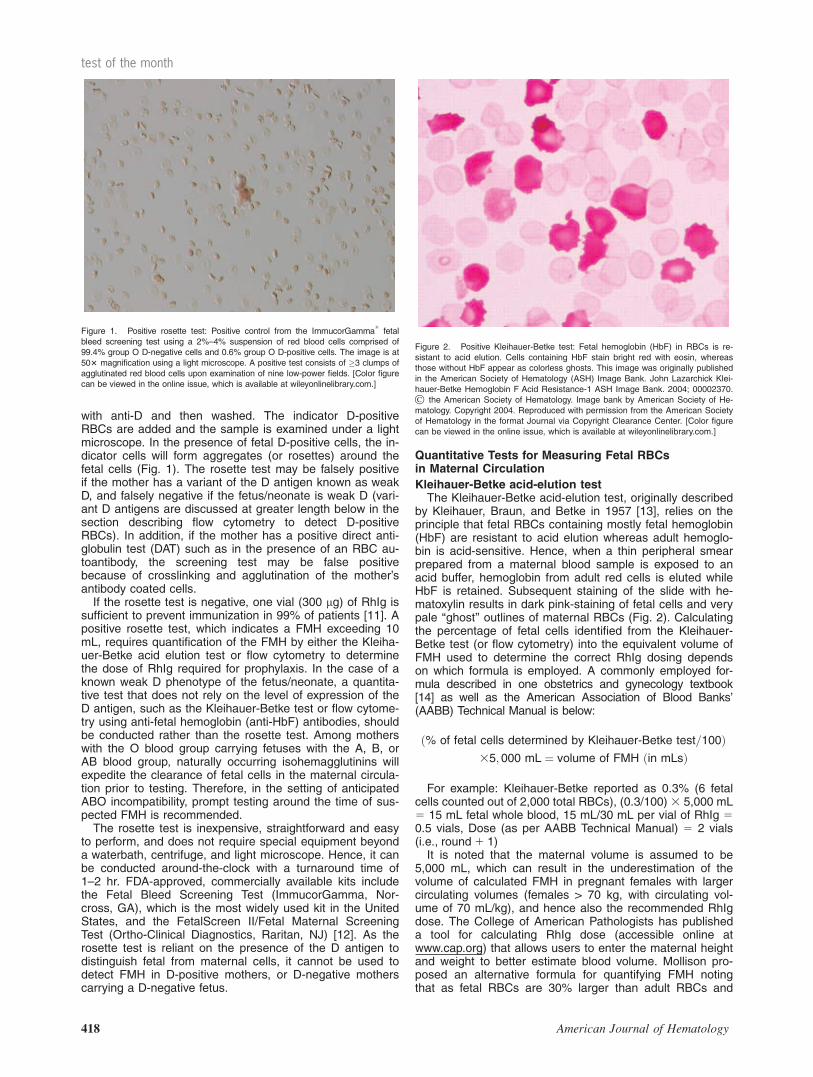
Kleihauer-Betke acid-elution testThe Kleihauer-Betke acid-elution test, originally described
by Kleihauer, Braun, and Betke in 1957 [13], relies on theprinciple that fetal RBCs containing mostly fetal hemoglobin(HbF) are resistant to acid elution whereas adult hemoglo-bin is acid-sensitive. Hence, when a thin peripheral smearprepared from a maternal blood sample is exposed to anacid buffer, hemoglobin from adult red cells is eluted whileHbF is retained. Subsequent staining of the slide with he-matoxylin results in dark pink-staining of fetal cells and verypale ‘‘ghost’’ outlines of maternal RBCs (Fig. 2). Calculatingthe percentage of fetal cells identified from the Kleihauer-Betke test (or flow cytometry) into the equivalent volume ofFMH used to determine the correct RhIg dosing dependson which formula is employed. A commonly employed for-mula described in one obstetrics and gynecology textbook[14] as well as the American Association of Blood Banks’(AABB) Technical Manual is below:
ð% of fetal cells determined by Kleihauer-Betke test=100Þ35; 000 mL ¼ volume of FMH ðin mLsÞ
For example: Kleihauer-Betke reported as 0.3% (6 fetalcells counted out of 2,000 total RBCs), (0.3/100) 3 5,000 mL5 15 mL fetal whole blood, 15 mL/30 mL per vial of RhIg 50.5 vials, Dose (as per AABB Technical Manual) 5 2 vials(i.e., round1 1)It is noted that the maternal volume is assumed to be
5,000 mL, which can result in the underestimation of thevolume of calculated FMH in pregnant females with largercirculating volumes (females > 70 kg, with circulating vol-ume of 70 mL/kg), and hence also the recommended RhIgdose. The College of American Pathologists has publisheda tool for calculating RhIg dose (accessible online atwww.cap.org) that allows users to enter the maternal heightand weight to better estimate blood volume. Mollison pro-posed an alternative formula for quantifying FMH notingthat as fetal RBCs are 30% larger than adult RBCs and
Figure 1. Positive rosette test: Positive control from the ImmucorGamma1
fetalbleed screening test using a 2%–4% suspension of red blood cells comprised of99.4% group O D-negative cells and 0.6% group O D-positive cells. The image is at503 magnification using a light microscope. A positive test consists of �3 clumps ofagglutinated red blood cells upon examination of nine low-power fields. [Color figurecan be viewed in the online issue, which is available at wileyonlinelibrary.com.]
Figure 2. Positive Kleihauer-Betke test: Fetal hemoglobin (HbF) in RBCs is re-sistant to acid elution. Cells containing HbF stain bright red with eosin, whereasthose without HbF appear as colorless ghosts. This image was originally publishedin the American Society of Hematology (ASH) Image Bank. John Lazarchick Klei-hauer-Betke Hemoglobin F Acid Resistance-1 ASH Image Bank. 2004; 00002370.
� the American Society of Hematology. Image bank by American Society of He-matology. Copyright 2004. Reproduced with permission from the American Societyof Hematology in the format Journal via Copyright Clearance Center. [Color figurecan be viewed in the online issue, which is available at wileyonlinelibrary.com.]
418 American Journal of Hematology
test of the month

only 90% of fetal RBCs stain darkly, simply using the pro-portion of darkly-staining cells can underestimate the vol-ume of FMH by a third [15]. The formula assumes that thematernal circulating red cell volume is 1,800 mL at termand applies a correction factor by multiplying the proportionof darkly-staining cells by 4/3 to obtain the volume of fetalRBCs:
Volume of fetal red cells ¼ð1; 800=ratio of unstained : darkly�stained RBCsÞ3ð4=3Þ ¼ 2; 400=ðratio of unstained : darkly�stained RBCsÞ
Mollison also suggested doubling the dose of RhIg to 50lg per 1 mL of fetal RBCs to allow for the possibility of atwofold underestimation. Table I displays variations in theestimated volume of FMH by using five published formulas,which reflects different assumptions regarding maternalblood volume, maternal hematocrit, fetal hematocrit, fetalmean corpuscular volume (MCV) relative to maternal MCV,and % of fetal cells that stain positive on acid elution. With0.3% fetal cells observed in the maternal circulation, theestimated fetal whole blood volume ranges from 10.8 to31.6 mL. A modified version of the Kleihauer-Betke testwas proposed by Clayton et al., who found that preparingthe citric acid-phosphate buffer at pH 3.2 resulted in opti-mal detection of FMH as small as 0.5 mL [19–21]. Subse-quently, this modified version has been widely adopted.
Although the manual Kleihauer-Betke test is the mostwidely used test to quantify the volume of FMH (95% oflaboratories participating in the 2009 CAP proficiency test-ing for fetal RBC detection used the Kleihauer-Betke testfor fetal RBC quantification) [12], it is not without its limita-tions. Aside from being laborious to perform (counting aminimum of 2,000 RBCs is recommended), the accuracyand precision of the test can be suboptimal because oflack of standardization leading to slight variations in testcharacteristics (i.e. thickness of blood smear, pH variationsin the buffer used), interobserver and interhospital varia-tions in result interpretation, and statistical imprecisionassociated with rare event analysis. In addition, differencesin methods for calculating the volume of FMH from % fetalcells identified by the Kleihauer-Betke test as well as therecommended RhIg dose further add to the variability. Cit-ing statistical imprecision of the Kleihauer-Betke test indetermining the dose of RhIg, the AABB Technical Manualrecommends rounding up and adding one vial if the calcu-lated dose to the right of the decimal point is �0.5 orrounding down and adding one vial if the calculated doseto the right of the decimal point is <0.5.Both over- and underestimation of FMH have been
reported [15,22–25], but most of the studies report thetendency of the Kleihauer-Betke test to overestimate FMH.Variables potentially contributing to both under- and overes-timation are listed in Table II. Overestimation is preferredrather than underestimation, as the latter can result in inad-equate RhIg dosing and subsequent sensitization. How-
TABLE I. Variation in Estimated Volume of Fetomaternal Hemorrhage for Kleihauer-Betke Test Result of 0.3% Using Published Formulas (Adapted from Wylie
and D’Alton [1])
Author Formula
FMH in mL of fetal whole blood
Cunningham et al [16] (HCTmaternal/HCTnewborn) 3 %fetal RBCs 3 MBV 5(0.36/0.50) 3 0.003 3 5,000 510.8 mLAssumptions:HCTmaternal 5 36%HCTnewborn 5 50%MBV 5 5,000 mL
Kleihauer (HCTmaternal/HCTnewborn) 3 %fetal RBCs 3 MBV 5(0.35/0.45) 3 0.003 3 5,800 513.5 mLAssumptions:HCTmaternal 5 35%HCTnewborn 5 45%MBV 5 5,800 mL
Creasy et al [14] and AABBTechnical Manual [17]
%fetal RBCs 3 MBV 50.003 3 5,000 515.0 mLAssumptions:MBV 5 5,000 mL
FMH in mL of fetal RBCsMollison [15] (1,800/ratio of unstained:darkly-stained RBCs) 3 (4/3) 5[1,800/(1,994/6)] 3 (4/3) 57.2 mL or 14.2 mL
of fetal whole bloodaAssumptions:MRBCV 5 1,800 mLMCV of fetal RBCs is 30% larger than that of adult RBCsOnly 90% of fetal RBCs stain dark pink on acid-elution
Foley et al [18] (# Fetal RBCs/# adult RBCs) 3 MRBCV 5(6/1,994) 3 75 3 70 515.8 mL or 31.6 mLof fetal whole bloodaAssumptions:
MRBCV 5 75 mL/kgAverage term woman weighs 70 kg
aAssuming fetal HCT of 50%.
Abbreviations: FMH, fetomaternal hemorrhage; HCT, hematocrit; MBV, maternal blood volume; MCV, mean corpuscular volume; MRBCV, maternal red blood cell volume;and RBC, red blood cell.
TABLE II. Variables Potentially Contributing to Over- or Underestimation of Fetomaternal Hemorrhage by the Kleihauer-Betke Test
Factors leading to overestimation Factors leading to underestimation
Presence of F-cells that also stain dark pink Failure to adjust for larger maternal circulating volume (for womenweighing > 70 kg)
‘‘Ghost’’ outlines of acid elution-sensitive adult RBCs which may bedifficult to pick up and increase the ratio of fetal RBCs:adult RBCs
Incomplete staining of fetal cells (only 90% stain dark pink)Failure to correct for differences in MCVs of fetal and adult RBCs (MCV of
fetal RBCs are 30% greater than that of adult RBCs)
Abbreviations: MCV, mean corpuscular volume; RBC, red blood cell.
American Journal of Hematology 419
test of the month

ever, overestimation itself is not desirable, as it carries risksrelated to plasma-derived products and results in excesscosts. Lafferty et al., in reporting the results of the ExternalQuality Assessment conducted in Ontario in 2000 and2001, observed that the poor reliability of the Kleihauer-Betke test may have resulted in underdosing RhIg in 19.4%of patients with FMH >10 mL [25]. If there is truth to thesereports, the underestimation of large FMH by the Kleiha-uer-Betke test undermines its function in quantitating largevolume FMH that may necessitate additional RhIg. Raafatet al. reported that standardizing the Kleihauer-Betke test,including recommendations for calculating the RhIg dose,resulted in an improvement in FMH quality assurance test-ing in Scotland [26]. In the end, the best estimate of mater-nal blood volume should probably be used to calculate thevolume of FMH.Variations of the modified Kleihauer-Betke test have
been proposed, including the substitution of the original378C elution for a convenient room temperature elution andautomated detection. Various commercial kits and reagentsare available. Pelikan et al. developed an automated read-out of the Kleihauer-Betke test using an automated micro-scope equipped with a scanning stage and an image analy-sis system (Applied Imaging Corporation, Santa Clara, Cali-fornia) connected to a personal computer. By scanning1,517 low power (103 objective) fields, the automated KBTshowed strong correlation between theoretical and detectedconcentrations of fetal cells (R2 5 0.999) and improved ac-curacy of fetal cell detection in the range of 0.0001%–1%FHM compared to standard manual evaluation [27].As the Kleihauer-Betke test is reliant on the visual dis-
crimination of fetal and adult RBCs by staining intensity(dark pink fetal vs. minimally stained adult RBCs), the pres-ence of F-cells containing intermediate concentrations ofHbF can complicate the interpretation. F-cells are RBCscontaining 20%–25% HbF and are present in normal adultsat a range of 0.5%–7.0% of circulating RBCs [28–30]. F-
cells are elevated in inherited hemoglobinopathies includingsickle cell disease and b-thalassemia, hereditary persist-ence of fetal hemoglobin (HPFH), acute stress erythropoie-sis, and pregnancy. In 25% of pregnant women, HbFbegins to increase at 8 weeks’ gestation and peaks at 18–22 weeks, and may reach levels as high as 7% by 32weeks [31,32]. Hence, the presence of F-cells may give ei-ther a false-positive test result or may overestimate themagnitude of a true FMH. Such cases of elevated F-celllevels presenting as FMH on Kleihauer-Betke testing haveoccurred in the setting of maternal HPFH, HPFH/sickletrait, and b-thalassemia [33–38]. In cases of known mater-nal history of elevated HbF and/or the presence of associ-ated conditions (such as thalassemia or HPFH), it isadvised that an alternative method to quantitate FMH suchas flow cytometry be used.
Flow cytometryAcknowledging the limitations of the Kleihauer-Betke test,
flow cytometry-based methods for the quantification of fetalcells in the maternal circulation have been developed.These methods fall into two main categories depending onthe target antigen of interest: HbF and RhD. FDA-approvedreagents for both methods are commercially available.Flow cytometry using anti-fetal hemoglobin antibodies.
Flow cytometry using monoclonal antibodies directedagainst HbF has some important advantages over the Klei-hauer-Betke test in the quantitation of FMH: (1) cytometricmethods can accurately distinguish adult F-cells from fetalRBCs (Fig. 3); (2) flow cytometry rapidly analyzes a greaternumber of cells (�50,000), improving quantitative accuracy;(3) as flow cytometry is automated, it has greater reprodu-cibility. Hence flow cytometry has broader clinical andresearch applicability, including the quantification of F-cellsin conditions such as sickle cell disease which may beused to guide prognosis and monitor treatment. Althoughthere are reports of elevated adult F-cells falsely increasing
Figure 3. Positive anti-fetal hemoglobin (anti-HbF) flow cytometry: Fetomaternal hemorrhage detection using anti-HbF antibody by flow cytometry (FMH QuikQuantAssay, Trillium Diagnostics, Bangor, Maine). Depending on anti-HbF fluorescence intensity, HbF-negative cells, F-cells, and fetal red blood cells (RBCs) can be distin-guished. Various samples showing increased fetal RBCs of 1.7% and 6.5% (panels A and C, respectively), increased adult F cells (panel B), and no fetal red cells (panelD). Flow histograms courtesy of Dr. Bruce Davis, Trillium Diagnostics. [Color figure can be viewed in the online issue, which is available at wileyonlinelibrary.com.]
420 American Journal of Hematology
test of the month

the fetal cell estimate by flow cytometry, the extent of theincrease is mild (contributing <0.1% to the fetal RBC per-centage) and has not been shown to contribute to clinicallyrelevant false-positive results [23]. Currently there is onlyone FDA-approved commercially available kit consisting ofpurified murine monoclonal anti-human HbF IgG1 antibody(Invitrogen, Camarillo, CA), as well as a separate fetal redcell control kit (Fetaltrol, Trillium Diagnostics, Portland, ME).The antibodies are conjugated to either fluorescein isothio-cyanate (FITC), R-phycoerythrin (R-PE), or indodicarbocya-nine dye (tri-color); however, FITC-conjugated antibodieshave been used in the majority of published studies.For analysis by flow cytometry, an EDTA anticoagulated
maternal blood sample is obtained from which the erythro-cyte count is determined. In a typical protocol, 2.5 3 107
red cells are briefly fixed in 0.05% glutaraldehyde and thenpermeabilized with a detergent (Triton X-100) that enablesthe antibodies to penetrate the cellular membranes andbind to the intracellular HbF [23]. Davis and colleagues firstdescribed this permeabilization technique using brief glutar-aldehyde and Triton X-100 treatments, which allowed for atotal assay time of 1 hr for five to six samples. This was incontrast to other reported permeabilization methods involv-ing acetone and alcohol washes that required either over-night incubations or numerous temperature-dependentsteps with a tendency for cell aggregate formation [23].Antibody stained cells are subsequently analyzed by a flowcytometer. Positive and negative controls are concurrentlyrun and help differentiate fluorescence attributed to fetalRBCs from non-specific background staining of autofluores-cent leukocytes and cellular debris. The positive control isalso instrumental in setting the fetal cell gating parameters.Prior CAP proficiency surveys have repeatedly shown
that flow cytometry using anti-HbF antibodies is more pre-cise (coefficient of variation (CV) <20%) than the Kleiha-uer-Betke methods (CV, 32%–80%) and has greater accu-racy. The 1999 and 2001 CAP surveys included samplesflanking the threshold of 0.6% fetal cells or 30 mL of fetalwhole blood (15 mL of fetal RBCs), which is the amount offetal whole blood that one vial (300 lg) of RhIg is purport-edly sufficient to protect against. For the 0.4% fetal cellsample, laboratories using either the Kleihauer-Betke testor anti-HbF flow cytometry performed similarly, in that 50%
of the laboratories overestimated FMH, reporting values>0.6%. For the 0.8% fetal cell sample, more than 10% ofthe labs using the Kleihauer-Betke test underestimatedFMH, reporting results <0.6%, but laboratories using anti-HbF flow cytometry, all correctly determined the FMH vol-ume [39].Available data indicate that anti-HbF flow cytometry is
better than the Kleihauer-Betke test as a confirmatory testfor FMH. Although good correlation has been reportedbetween the Kleihauer-Betke test and anti-HbF flow cytom-etry for both small and large FMH, published studies are inagreement with the CAP proficiency surveys that anti-HbFflow cytometry displays greater test and interlaboratory pre-cision than the Kleihauer-Betke method [23,40-42]. Thereis interest in using anti-HbF flow cytometry also as an initialscreening test for FMH, especially because of its potentialbroader clinical application; however, data regardingwhether flow cytometry has sufficient sensitivity to detectlow concentrations of fetal cells (<0.1%) is mixed. Moststudies report that flow cytometry accurately and preciselyquantifies FMH volumes �0.1% [23,41,43]. At present,flow cytometry is not used for screening primarily becauseof the fact that most hospitals do not have access to a flowcytometer or resources to staff a flow cytometer around-the-clock. However, anti-HbF flow cytometry appears to bean appropriate confirmatory test for hospitals with adequateresources and staffing.Flow cytometry using anti-D antibodies. Anti-D anti-
bodies can also be used in quantitating FMH, but theirapplicability is limited to the clinical scenario of D antigenincompatibility. Initial studies demonstrating the feasibilityof flow cytometry for fetal cell quantification targeted the Dantigen. Using this method, FMH as small as 0.1–0.2%can be quantitated [9,40,44]. FDA approved monoclonalanti-D antibodies are commercially available (Quant-Rho,Alba Bioscience, Edinburgh, UK). The advantages ofusing anti-D over anti-HbF antibodies are two-fold: thepermeabilization step used in the anti-HbF method is omit-ted as the D antigen is expressed on the RBC surface,and F-cells do not interfere with the calculation of fetalcells. Importantly, flow cytometry cannot reliably detect theRh variants, weak D and partial D, from D-negative cells,resulting in false-negative results [45]. The Rh blood groupsystem is highly polymorphic and its variants are catego-rized into two groups: partial D and weak D phenotypes.Partial D variants are characterized by mutations in theextracellular domains leading to altered epitopes. In com-parison, weak D variants are due to mutations in the intra-cellular or transmembrane domains resulting in adecreased number of qualitatively normal D antigens onthe RBC surface. Although it is thought that weak D RBCsare highly unlikely to cause primary anti-D alloimmuniza-tion [46,47], a case report of alloimmunization by partial Dantigen in pregnancy has been reported [48]. Administra-tion of prophylactic RhIg to the mother prior to obtainingthe blood specimen can also complicate cytometric analy-sis using anti-D antibodies because the RhIg may bind toand block antibody binding sites on fetal RBCs, preventingtheir detection. Kumpel et al proposed a double stainingprocedure with FITC-conjugated anti-D antibodies followedby a FITC-conjugated anti-human IgG to ensure optimallabeling of D1 cells, regardless of the blocking effects byin vivo RhIg binding [49]. The FITC-conjugated anti-humanIgG binds to the RhIg that is present on the D1 RBC sur-face. However, the labor involved in the extra incubationstep would negate the advantage of the one-step anti-Dmethod.There is a paucity of data directly comparing cytometric
methods using anti-HbF or anti-D, but one study showed
Figure 4. Suggested testing algorithm for detection of fetomaternal hemorrhage.*In case of known maternal elevation of fetal hemoglobin (i.e., HPFH, HPFH/sicklecell trait, b-thalassemia), proceed to either anti-HbF or anti-D flow cytometry.
American Journal of Hematology 421
test of the month

that anti-HbF labeling significantly underestimates the vol-ume of massive FMH (�1% fetal cells) in comparison toanti-D labeling. In samples containing �0.6% fetal cells, nosignificant difference between the two methods was seen[50]. The reason for the difference is unknown, but theauthors postulated that this may be because of potentialvariability in HbF concentration within fetal erythrocytes.The fetal-to-adult hemoglobin switch starts several weeksbefore birth [50], in contrast to the D antigen, which isdetected on all erythrocytes in D-positive individuals by 6weeks gestation [51]. Additional studies are needed to ver-ify the potential of anti-HbF flow cytometry to underestimatemassive FMH, as well as to directly compare the perform-ance of the anti-HbF and anti-D methods with the Kleiha-uer-Betke test.Combined flow cytometric methods. A combined flow
cytometric method using both anti-D and anti-HbF antibod-ies is available and has been shown to correlate well withthe Kleihauer-Betke test [52]. The strength of this assay isits capacity to distinguish fetal cells from maternal cells forboth D1 and D2 women, although this is also true of theHbF method. However, in clinical situations where themother may have increased circulating F-cells, the dualantibody method may still allow quantitation of fetal cells ifthere is a detectable disparity in the maternal and fetal Dphenotypes. As the dual method can be broadly applied toall cases of FMH and the laboratory does not have to knowthe fetus/neonate’s D status a priori, only one quantitativetest can be offered. However, the use of multiple antibodiesresults in additional costs. The precise clinical circumstancein which the dual platform makes sense, such as a preg-nant woman who has sickle cell disease and is D-negative,is fairly uncommon and probably does not justify the addedcomplexity of testing (which may result in additional errorsand cost). Other combined flow cytometric methods havebeen described, including the use of anti-HbF and anti-car-bonic anhydrase (anti-CA) antibodies. Since fetal cells havelittle or no carbonic anhydrase (CA) compared to adult cellswhich show abundant expression of the enzyme, fetalRBCs (HbF1, CA2) can be easily distinguished from F-cells (HbFlow1, CA1) and normal adult RBCs (HbF2, CA1)[24]. A similar approach can be applied for the i and I anti-gens, which are expressed by fetal and adult RBCs,respectively.Alternative antibody-based methods to flow cytometry.
Although flow cytometry has been shown to have greaterprecision and broader clinical applicability than the Kleiha-uer-Betke test, fewer than 5% of participating laboratoriesin CAP’s 2009 proficiency testing for fetal red blood celldetection reported using it to quantify fetal cells [12]. Thereasons for the low utilization of flow cytometry includestaffing and equipment costs. The requirement for flowcytometry services to be offered around-the-clock is prohib-itive for most hospitals. Alternative antibody-based methodsto conventional flow cytometry include immunofluorescencemicroscopy and the use of a hematology analyzer for auto-mated immunofluorescent enumeration of antibody labeledfetal cells. Ochsenbein-Imhof et al. found that flow cytome-try and immunofluorescence microscopy were comparablyaccurate and precise in enumerating fetal cells stained withanti-D and phycoerythrin-conjugated anti-human IgG [44].However, the microscopic method would still entail manualcounting. Little et al. evaluated the use of a hematology an-alyzer (Abbott Cell-Dyn CD4000) for the quantification ofFMH by immunofluorescence using a FITC-labeled mono-clonal anti-D antibody. They analyzed a range of samplesconsisting of 0.04% to 1.50% fetal cells. They reportedexcellent agreement and correlation (R250.99) betweenobserved and expected fetal cell percentages. Additionally,
the predicted lower limit for the quantitation of FMH was1.6 mL with a maximum CV of 15%, which is well-belowthe 15 mL threshold for additional RhIg dosing [53]. Theapplication of a hematology analyzer for the quantitation ofFMH is especially appealing, as it is fully automated, pre-cise, and has a wide range of linearity. Additional studies tosee if other antibodies, such as anti-HbF, are suitable forthis platform are needed.
SummaryRhIg prophylaxis has reduced the overall risk of Rh im-
munization from 13.2% to 0.2%, and testing for large FMHhas further decreased the risk to 0.14%. The few cases ofRh immunization have been mostly attributed to the occur-rence of events prior to 28 weeks gestation [54]. The ro-sette screen has been shown to be a highly sensitivemethod to qualitatively detect large FMHs of �10 mL (0.2%fetal cells), with 15 mL serving as the threshold forincreased RhIg dosing. As the test is designed to give anegative result when the amount of FMH is small (i.e. <2mL or 0.04% fetal cells), which is the case in the vastmajority of pregnancies [4], only few cases will necessitateconfirmatory quantitative testing.The two well-established confirmatory tests are the Klei-
hauer-Betke acid-elution assay and flow cytometry.Although the Kleihauer-Betke test is inexpensive andrequires no special equipment, allowing it to be performedaround-the-clock, it has several disadvantages: it is labori-ous to perform, lacks standardization, is imprecise, andmay not be accurate in conditions with elevated F-cells.Flow cytometry has been shown to have greater precisionand accuracy than the Kleihauer-Betke test. In addition, fe-tal cells can be distinguished from F-cells in conditions withelevated HbF. Despite these advantages, it has not beenbroadly implemented as it requires a flow cytometer, atrained technician, and is more expensive and difficult tooffer around-the-clock. Flow cytometry is not without its lim-itations, as the anti-D method is limited to the clinical sce-nario of D antigen incompatibility and may not reliablydetect weak and partial D. Although anti-HbF flow cytome-try can better distinguish F-cells from fetal cells comparedto the Kleihauer-Betke test, concerns have been raisedwhether anti-HbF labeling underestimates massive FMH[50]. The limitations of the one-antibody approach can beaddressed by using two antibodies (i.e. anti-D and anti-HbF, or antibodies to some other antigen expressed differ-entially on fetal and adult cells, such as i or CA). This way,one test can be ordered for all patients, regardless of Dstatus or history of F-cell elevations. However, the use ofan additional antibody increases the cost of testing, andthe relatively infrequent need to quantify FMH may make itcumbersome to maintain quality control and proficiency.From both resource allocation and cost-effectiveness stand-points as well as questionable sensitivity to serve as ascreening test, flow cytometry seems best suited as a con-firmatory test for FMH. However, it (or the Kleihauer-Betketest) may be useful as the first-line test in the case of aknown weak D phenotype of the fetus/neonate or in lieu ofthe Kleihauer-Betke test in the setting of elevated HbF.Theapplication of hematology analyzers that have features sim-ilar to multiparameter flow cytometers may enable labs toadopt a fully automated and precise antibody-basedmethod for quantifying FMH. With around-the-clock avail-ability and a short 30-minute turn-around time, confirmatoryFMH testing can be integrated into routine hematology test-ing menu. Equivalent results to flow cytometry have beenshown for both the anti-HbF and anti-D antigen methods
422 American Journal of Hematology
test of the month

using one model [53]. With the trend of integratingextended applications into routine hematology analyzers,the automated reticulocyte count being a notable example,additional platform options and broader clinical use is pre-dicted to follow.
AcknowledgmentsThe authors are indebted to Drs. Michael Greene and
Elizabeth Van Cott for critical review of the manuscript, toDr. Bruce Davis for supplying the anti-HbF flow histograms,and Amy Slater for technical assistance.
References1. Wylie BJ, D’Alton ME. Fetomaternal hemorrhage. Obstet Gynecol 2010;
115:1039–1051.2. Daniels G. Human Blood Groups. Chichester, England: Wiley-Blackwell;
2002. pp 247.3. MacKenzie IZ, Roseman F, Findlay J. The kinetics of routine antenatal pro-
phylactic intramuscular injections of polyclonal anti-D immunoglobulin. BJOG2006;113:97–101.
4. Controlled trial of various anti-D dosages in suppression of Rh sensitizationfollowing pregnancy. Report to the Medical Research Council by the workingparty on the use of anti-D-immunoglobulin for the prevention of isoimmuniza-tion of Rh-negative women during pregnancy. Br Med J 1974;2:75–80.
5. Sebring ES, Polesky HF. Fetomaternal hemorrhage: Incidence, risk factors,time of occurrence, and clinical effects. Transfusion 1990;30:344–357.
6. Ramsey G. Inaccurate doses of R immune globulin after rh-incompatible feto-maternal hemorrhage: Survey of laboratory practice. Arch Pathol Lab Med2009;133:465–469.
7. Polesky HF, Sebring ES. Evaluation of methods for detection and quantitationof fetal cells and their effect on RhIgG usage. Am J Clin Pathol 1981;76(4Suppl):525–529.
8. Stedman CM, Baudin JC, White CA, Cooper ES. Use of the erythrocyte ro-sette test to screen for excessive fetomaternal hemorrhage in Rh-negativewomen. Am J Obstet Gynecol 1986;154:1363–1369.
9. Bayliss KM, Kueck BD, Johnson ST, Fueger JT. Detecting fetomaternal hem-orrhage: A comparison of five methods. Transfusion 1991;31:303–307.
10. Sebring ES, Polesky HF, Detection of fetal hemorrhage in Rh immune globu-lin candidates. A rosetting technique using enzyme-treated Rh2Rh2 indicatorerythrocytes. Transfusion 1982;22:468–471.
11. Klein HG, Anstee DJ, eds. Mollison’s Blood Transfusion in Clinical Medicine.11th ed. Malden, MA: Blackwell; 2005.
12. Sandler SG, Sathiyamoorthy S. Laboratory methods for Rh immunoprophy-laxis: A review. Immunohematology 2010;26:92–103.
13. Kleihauer E, Braun H, Betke K. [Demonstration of fetal hemoglobin in erythro-cytes of a blood smear]. Klin Wochenschr 1957;35:637–638.
14. Creasy RK, Resnik R, Iams JD. Maternal-Fetal Medicine, 5th ed. Philadel-phia, PA: W.B. Saunders Co.xviii; 2004.1362 p.
15. Mollison PL. Quantitation of transplacental haemorrhage. Br Med J1972;3:31–34.
16. Cunningham FG, Williams JW. Williams Obstetrics, 20th ed. Stamford, CT:Appleton & Lange.viii; 1997. p 1448.
17. American Association of Blood Banks, Technical Manual of the AmericanAssociation of Blood Banks, 16th ed. Washington, DC: AABB; 2008. p 985.
18. Foley MR, Strong TH, Garite TJ. Obstetric Intensive Care Manual,2nd ed.New York: McGraw-Hill Medical; 2004.
19. Clayton EM Jr, Feldhaus WD, Phythyon JM. The demonstration of fetal eryth-rocytes in the presence of adult red blood cells. Am J Clin Pathol1963;40:487–490.
20. Clayton EM Jr, Foster EB, Clayton EP. New stain for fetal erythrocytes inperipheral blood smears. Obstet Gynecol 1970;35:642–645.
21. Clayton EM Jr, Robertson JC, Feldhaus WD. Antepartum and postpartumdetection of fetal erythrocytes in maternal circulation. Obstet Gynecol1962;20:608–610.
22. Clayton EM Jr, Birdwell ED, Gregory MG. Fetal cell counting as a guide toprevention of Rh sensitization. Transfusion 1973;13:425–427.
23. Davis BH, Olsen S, Bigelow NC, Chen JC. Detection of fetal red cells in feto-maternal hemorrhage using a fetal hemoglobin monoclonal antibody by flowcytometry. Transfusion 1998;38:749–756.
24. Porra V, Bernaud J, Gueret P. Identification and quantification of fetal redblood cells in maternal blood by a dual-color flow cytometric method: Evalua-tion of the fetal cell count kit. Transfusion 2007;47:1281–1289.
25. Lafferty JD, Raby A, Crawford L. Fetal-maternal hemorrhage detection in On-tario. Am J Clin Pathol 2003;119:72–77.
26. Raafat A, Fraser N, Main R, Urbaniak SJ. A quality assurance scheme for theKleihauer test: The Scottish experience 1988–1996. Transfus Med1997;7:221–226.
27. Pelikan DM, Mesker WE, Scherjon SA. Improvement of the Kleihauer-Betketest by automated detection of fetal erythrocytes in maternal blood. CytometryB Clin Cytom 2003;54:1–9.
28. Franco RS, Yasin Z, Palascak MB. The effect of fetal hemoglobin on the sur-vival characteristics of sickle cells. Blood 2006;108:1073–1076.
29. Garner C, Tatu T, Reittie JE. Genetic influences on F cells and other hemato-logic variables: A twin heritability study. Blood 2000;95:342–346.
30. Wood WG, Stamatoyannopoulos G, Lim G, Nute PE. F-cells in the adult: Nor-mal values and levels in individuals with hereditary and acquired elevations ofHb F. Blood 1975;46:671–682.
31. Popat N, Wood WG, Weatherall DJ, Turnbull AC. Pattern of maternal F-cellproduction during pregnancy. Lancet 1977;2:377–379.
32. Duguid JK, Bromilow IM. Laboratory measurement of fetomaternal hemor-rhage and its clinical relevance. Transfus Med Rev 1999;13:43–48.
33. Stropnicky EM, MacKenna J, Larkin E. Persistent hemoglobin F in donorblood may give falsely elevated acid-elution test in Rh-negative patient. Am JObstet Gynecol 1982;142:109–110.
34. Krauss JS, Fadel HE, Squires J, Baisden CR. Detection of fetal-maternalhemorrhage in a mother with sickle trait and hereditary persistence of fetalhemoglobin. Transfusion 1983;23:530–531.
35. Weaver DL, Barthold JC, Hamill B. Hereditary persistence of fetal hemoglobinpresenting as fetal-maternal hemorrhage. Am J Clin Pathol 1990;93:277–280.
36. Patton WN, Nicholson GS, Sawers AH. Assessment of fetal-maternal haem-orrhage in mothers with hereditary persistence of fetal haemoglobin. J ClinPathol 1990;43:728–731.
37. Goldman M, Blajchman MA, Ali MA. Overestimation of fetomaternal haemor-rhage by the acid-elution technique in mothers with beta-thalassaemia minor.Transfus Med 1991;1:129–132.
38. Iyer R, McElhinney B, Heasley N. False positive Kleihauer tests and unnecessaryadministration of anti-D immunoglobulin. Clin Lab Haematol 2003;25:405–408.
39. Davis BH. Laboratory assessment of fetomaternal hemorrhage is improvedusing flow cytometry. LabMedicine 2007;38:365–371.
40. Bromilow IM, Duguid JK. Measurement of feto-maternal haemorrhage: Acomparative study of three Kleihauer techniques and two flow cytometrymethods. Clin Lab Haematol 1997;19:137–142.
41. Chen JC, Davis BH, Wood B, Warzynski MJ. Multicenter clinical experiencewith flow cytometric method for fetomaternal hemorrhage detection. Cytome-try 2002;50:285–290.
42. Chen JC, Bigelow N, Davis BH. Proposed flow cytometric reference methodfor the determination of erythroid F-cell counts. Cytometry 2000;42:239–246.
43. Pelikan DM, Scherjon SA, Mesker WE. Quantification of fetomaternal hemor-rhage: A comparative study of the manual and automated microscopic Kleiha-uer-Betke tests and flow cytometry in clinical samples. Am J Obstet Gynecol2004;191:551–557.
44. Ochsenbein-Imhof N, Ochsenbein AF, Seifert B. Quantification of fetomaternalhemorrhage by fluorescence microscopy is equivalent to flow cytometry.Transfusion 2002;42:947–953.
45. Lloyd-Evans P, Guest AR, Voak D, Scott ML. Detection of weak D and D(VI)red cells in D-negative mixtures by flow cytometry: Implications for feto-maternalhaemorrhage quantification and D typing policies for newborns. Br J Haematol1999;104:621–625.
46. Kumpel B. Are weak D RBCs really immunogenic? Transfusion2006;46:1061–1062; discussion 1062–1066.
47. Schmidt PJ. Are weak D red blood cells really immunogenic? Transfusion2006;46:2029–2030.
48. Mayne K, Bowell P, Woodward T. Rh immunization by the partial D antigen ofcategory DVa. Br J Haematol 1990;76(4):537–539.
49. Kumpel BM. Labeling D1 RBCs for flow cytometric quantification of fetoma-ternal hemorrhage after the RBCs have been coated with anti-D. Transfusion2001;41:1059–1063.
50. Kennedy GA, Shaw R, Just S. Quantification of feto-maternal haemorrhage(FMH) by flow cytometry: Anti-fetal haemoglobin labelling potentially underes-timates massive FMH in comparison to labelling with anti-D. Transfus Med2003;13:25–33.
51. Urbaniak SJ. The scientific basis of antenatal prophylaxis. Br J Obstet Gynae-col 1998;105 (Suppl 18):11–18.
52. Radel DJ, Penz CS, Dietz AB, Gastineau DA. A combined flow cytometry-based method for fetomaternal hemorrhage and maternal D. Transfusion2008;48:1886–1891.
53. Little BH, Robson R, Roemer B, Scott CS. Immunocytometric quantitation offoeto-maternal haemorrhage with the Abbott Cell-Dyn CD4000 haematologyanalyser. Clin Lab Haematol 2005;27:21–31.
54. Bowman J. Thirty-five years of Rh prophylaxis. Transfusion 2003;43:1661–1666.
American Journal of Hematology 423
test of the month





























