Embed Size (px)
Citation preview
REVIEW Open Access
Delayed initiation of antenatal care andassociated factors in Ethiopia: a systematicreview and meta-analysisGezahegn Tesfaye1,2* , Deborah Loxton1, Catherine Chojenta1, Agumasie Semahegn2 and Roger Smith3
Abstract
Background: Antenatal care uptake is among the key indicators for monitoring the progress of maternal outcomes.Early initiation of antenatal care facilitates the timely management and treatment of pregnancy complications toreduce maternal deaths. In Ethiopia, antenatal care utilization is generally low, and delayed initiation of care is verycommon. We aimed to systematically identify and synthesize available evidence on delayed initiation of antenatalcare and the associated factors in Ethiopia.
Methods: Studies published in English from 1 January 2002 to 30 April 2017 were systematically searched fromPubMed, Medline, EMBASE, CINAHL and other relevant sources. Two authors independently reviewed the identifiedstudies against the eligibility criteria. The included studies were critically appraised using the Joanna Briggs-MAStARIinstrument for observational studies. Meta-analysis was conducted in RevMan v5.3 for Windows using a Mantel–Haenszelrandom effects model. The presence of statistical heterogeneity was checked using the Cochran Q test, and its level wasquantified using the I2 statistics. Pooled estimate of the proportion of the outcome variable was calculated. Pooled OddRatios with 95% CI were calculated to measure the effect sizes.
Result: The pooled magnitude of delayed antenatal care in Ethiopia was 64% (95% CI: 57%, 70%). Maternal age (OR = 0.70; 95% CI: 0.53, 0.93), place of residence (OR = 0.29, 95% CI: 0.16, 0.50), maternal education (OR = 0.49; 95% CI: 0.38, 0.63),husband’s education (OR = 0.44; 95% CI: 0.23, 0.85), maternal occupation (OR = 0.75; 95% CI: 0.61, 0.93), monthly income(OR = 2.06; 95% CI: 1.23, 3.45), pregnancy intention (OR = 0.49; 95% CI: 0.40, 0.60), parity (OR = 0.46; 95% CI: 0.36, 0.58),knowledge of antenatal care (OR = 0.40; 95% CI: 0.32, 0.51), women’s autonomy (OR = 0.38; 95% CI: 0.15, 0.94), partnerinvolvement (OR = 0.24; 95% CI: 0.07, 0.75), pregnancy complications (OR = 0.23; 95% CI: 0.06, 0.95), and means ofidentifying pregnancy (OR = 0.50; 95% CI: 0.36, 0.69) were significantly associated with delayed antenatal care.
Conclusion: Improving female education and women’s empowerment through economic reforms, strengthening familyplanning programs to reduce unintended pregnancy and promoting partner involvement in pregnancy care couldreduce the very high magnitude of delayed antenatal care in Ethiopia.
Trial registration: CRD42017064585.
Keywords: Delayed antenatal care, Associated factors, Ethiopia, Systematic review, Meta-analysis
* Correspondence: [email protected]; [email protected] Centre for Generational Health and Ageing, Faculty of Health andMedicine, University of Newcastle, Newcastle, Australia2School of Public Health, College of Health and Medical Sciences, HaramayaUniversity, Harar, EthiopiaFull list of author information is available at the end of the article
© The Author(s). 2017 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Tesfaye et al. Reproductive Health (2017) 14:150 DOI 10.1186/s12978-017-0412-4

Plain English summaryA professional care provided to women during preg-nancy is called antenatal care. Antenatal care plays agreat role in the improvement of maternal health. InEthiopia and other sub-Saharan African countries, ante-natal care utilization among pregnant women was low.Moreover, the pregnant women in Ethiopia and otherdeveloping countries tend to postpone their first ante-natal care clinic visit into the later months of pregnancy.This study summarized the existing evidence on thelevel of late antenatal care visit and its contributing fac-tors among pregnant women in Ethiopia. Using differentdatabases and other sources, this review identifiedtwenty two relevant studies that reported late antenatalcare clinic visit and its influencing factors among preg-nant women in Ethiopia. We summarized and analysedthe reports from the twenty two studies and put a com-bined assessment result on the level of late antenatalcare and associated factors. Based on our review, nearlytwo thirds of the pregnant women in Ethiopia madetheir first antenatal care clinic visit late in their preg-nancy. Women’s non-attendance of education, husband’snon-attendance of education, women’s older age, ruraldwelling, having previous births, unintended pregnancy,women’s unemployment, low monthly income, lack ofknowledge about antenatal care, lack of women’s decisionmaking power, no partner involvement, and not facingproblems during pregnancy were factors associated withhigher level of women’s late appearance to antenatal care.Nationwide all rounded efforts targeting the major contrib-uting factors should be established to alleviate women’s lateantenatal care utilization in the country.
BackgroundThe burden of maternal mortality remains hugely variedbetween developing and developed countries [1]. In de-veloping countries, the overall life time risk of woman’sdeath due to pregnancy and related causes is estimatedto be 1 in 180, while for developed countries it is about1 in 4900 [2]. The maternal mortality ratio in Ethiopia isstill high at 353 per 100,000 live births in 2015 [3], andit remains among the highest in the world. In developingcountries like Ethiopia, obstetric complications duringpregnancy and childbirth are the leading causes of deathamong reproductive aged women [3, 4]. It is generallyrecognized that a lack of access to, and inadequateutilization of, antenatal care (ANC) during pregnancycontributes to adverse maternal health outcomes such asmaternal mortality [5, 6], something which is more com-mon in resource-poor settings. Antenatal care uptake isone of the key indicators for monitoring the progress ofimproving maternal outcomes. Early initiation of ANCfacilitates the timely management and treatment of preg-nancy complications to reduce maternal deaths [7].
In Ethiopia, the main direct causes of maternal mortal-ity are haemorrhage, hypertensive disorders of preg-nancy, unsafe abortion and puerperal sepsis [8, 9]. Thesecomplications can be averted or otherwise treatedthrough providing skilled care during pregnancy, childbirth and in the postnatal period [2]. In 2002, the WorldHealth Organization (WHO) recommended that preg-nant women make at least four ANC visits [10]; in 2016this recommendation was modified to at least eight visits[11], with the first ANC visit to be undertaken before the12th week of pregnancy. While there has been markedprogress in the uptake of at least one ANC attendance inEthiopia [12–17], there has been suboptimal attendance ofthe recommended visits [4, 13, 18, 19]. Of even more con-cern was the substantial proportion of women who de-layed their first ANC visit to the second or third trimesterof pregnancy [5, 19–21]. According to the NationalDemographic and Health Survey Report of Ethiopia [20],in 2014 more than three quarters of pregnant women ini-tiated their first visit after 16 weeks of pregnancy. Earlyinitiation of ANC plays a paramount role in enhancingmaternal health as it provides an opportunity for the earlyscreening, treatment and referral of pregnancy complica-tions [11]. Evidence has shown that pregnant women whoinitiate ANC early were less likely to develop unfavourableobstetric outcomes as compared to women who enteredinto care after the first trimester [22, 23].The key challenges that women face when seeking ma-
ternal health services were clearly explained in the threedelays model [24]. This model described the barriers toutilizing maternal health services at three interrelatedlevels before the occurrence of maternal death. At thefirst level, the home or community level, women may bedelayed from seeking ANC due to factors such as thelow social status of women in relation to decision-making, poor awareness of pregnancy or birth complica-tions, previous poor experience of care, traditional orsocial practices during pregnancy or childbirth, acceptanceof maternal death as normal and financial dependency. InEthiopia, there is huge gap in the level of income amongwomen and men especially in rural parts of Ethiopia, andwomen are less empowered to access and control house-hold resources [25]. This could influence their capacity tomake decisions about utilization of maternal care. More-over, the financial burden associated transportation to andfrom the facility and the costs incurred for the maternalcare itself profoundly diminished the uptake of the care[26]. In the second level, there may be a delay in reachinga health facility which might be due to distance, unavail-ability of infrastructure (road or transportation) or difficultterrain. The third level of delay (delay in receiving ad-equate care) might be related to a shortage of, or inad-equately trained health staff, and unavailability of medicalsupplies and equipment.
Tesfaye et al. Reproductive Health (2017) 14:150 Page 2 of 17

Several studies [27–33] have investigated factors af-fecting delayed attendance of ANC in Ethiopia. None-theless, none of these studies have systematicallyreviewed the factors to show their overall pooled effecton delayed initiation of ANC at the national level. Inaddition, there were inconsistencies in attributing theinfluence of the factors on late initiation of ANC acrossvarious studies. For instance, there were incongruent find-ings on the influence of maternal education [34–37], ma-ternal age [32–34, 36], place of residence [28, 32, 38, 39],maternal occupation [30, 34, 37, 40], marital status[32, 36, 37], husband’s education [31, 32, 41], previousexperience of using ANC [32, 33, 35] and history ofabortion [31, 32, 42] on delayed initiation of ANCamong many other factors. Hence, demonstrating apooled effect of the factors on delayed initiation ofANC was warranted.Previous systematic reviews conducted in developing
[43, 44] and developed [45] countries have mainlyreviewed evidence on the adequacy of the utilization ofANC and its related factors. In particular, the reviewscovered larger geographical regions and hence failed toreflect country specific situations. Moreover, these re-views did not centre on delayed initiation of ANC as aprimary outcome of interest. The objective of this reviewis to systematically identify and synthesize existing evi-dence to understand the level of delayed initiation ofANC and associated factors among reproductive agedwomen in Ethiopia.
MethodDevelopment of the review methodThe methodology of this systematic review was developedbased on the Preferred Reporting Items for SystematicReviews and Meta-Analyses Protocols (PRISMA-P) 2015Statement [46] and the items in the PRISMA-P checklistwere addressed (Additional file 1). The four phases thatwere drawn from the PRISMA flow chart ( [47]) were doc-umented in the results to show the study selection processfrom initially identified records to finally included studies.The protocol for this systematic review and meta-analysiswas registered in international prospective register of sys-tematic reviews (PROSPERO) and obtained the registra-tion number (CRD42017064585).
Search strategyThe literature search was carried out by the primary au-thor (GT). The search was limited to papers publishedin English from 1 January 2002 to 30 April 2017. Theyear 2002 was selected, since WHO had introduced theFocused ANC model [10] by this year. We appliedMeSH terms, Emtree, CINAHL headings and combinedkey words to identify studies in the databases. Majormedical electronic databases such as PubMed, Medline
(OVID interface), Excerpta Medica (Embase) (OVIDinterface), and CINAHL (EBSCO host) were used toidentify relevant literature for the review. To cover greyliterature, we hand-searched literature using the Googlesearch engine and Google Scholar; official WHO websites;online libraries of academic and government institutionsand references of electronically identified articles. Thesearch strings or terms were stemmed from the followingkey words: delayed initiation, ANC, associated factors,and Ethiopia. The search terms were used to retrieverelevant literature in combined form adapted to therequirement of the specific database. Further informa-tion regarding the search strategy of the selected da-tabases is attached (Additional file 2).
Eligibility criteriaWe included all observational studies as well as Demo-graphic and Health Surveys (DHS) reports. We consideredstudies that examined the level and factors associated withdelayed initiation of ANC among reproductive agedwomen (15–49 years) who were pregnant or gave birth atleast once and who live in Ethiopia. We included studiesthat defined the main outcome variable “delayed initiationof ANC” as entry into care after at least 12 weeks of preg-nancy, including studies that defined delayed initiation ofANC as entry into the care after 16 weeks of gestation.Studies that had been conducted in either a community orfacility setting and which involved analysis of primary orsecondary data were included. We included studies thathad measure of association statistics or had test statisticthat explicitly demonstrated the influence of the predic-tors on delayed initiation of ANC or had a crosstab show-ing the difference in magnitude of the outcome variable inthe categories of the predicting variables. We excluded re-views, editorials, case series and case reports on delayedinitiation of ANC. We also excluded studies that only re-ported qualitative findings on delayed ANC initiation. Instudies that reported both quantitative and qualitative re-sults, we only considered the quantitative findings.
Study selection procedureScreeningFirst studies were identified through applying the searchstrings and the filters in the databases as well as otherrelevant sources. The identified studies were exported tothe citation manager (EndNote) [48] and duplicates wereexcluded. The two authors (GT and AS) independentlyscreened the studies based on the information containedin the titles and abstracts according to the inclusion cri-teria. Based on this screening, the titles and abstracts ofthe studies were classified as included, excluded, andundecided. We then obtained the full texts of all theincluded and the undecided studies for further eligi-bility assessment.
Tesfaye et al. Reproductive Health (2017) 14:150 Page 3 of 17

Eligibility of studiesThe two authors (GT and AS) independently reviewed thefull texts of the included and undecided categories of thestudies against the eligibility criteria for final inclusion.Studies that were not eligible based on the examin-ation of the full-text were excluded and the reasonsfor the exclusion were described. Disagreements be-tween the two reviewers were resolved through dis-cussion and consensus.
Quality assessmentAll of the included studies were critically appraised fortheir validity. The two authors (GT and AS) checked themethodological robustness and validity of the findingsusing the JBI (Joanna Briggs Institute) Meta-Analysis ofStatistics Assessment and Review Instrument (MAStARI)[49]. Particular attention was given to a clear statement ofthe objective of the study, inclusion criteria, randomnessof subject selection, identification of the study subjects,and preciseness of measurement of outcomes of interestand use of appropriate statistical analysis method, as wellas documentation of sources of bias or confounding. Un-certainties were resolved by joint discussion between thereviewers. The level of agreement between the two re-viewers was judged using the Cohen’s Kappa (K) coeffi-cient statistics. To calculate “K” a two by two contingencytable was constructed with “High” and “Low” categories ofquality assessment provided independently by the two re-viewers based on set of criteria. We obtained “K” value of(0.80), and thus the level of agreement was satisfactory. Inorder to minimize publication bias, we searched and in-cluded both published and unpublished literature. We ob-tained unpublished literatures (grey literatures) throughhand-searching of online libraries of academic institutions,government organizations, and agencies in addition tousing Google search engine and Google scholar. We alsocontacted an author to seek data that was not clearly re-ported in the article.
Data extraction processA structured data extraction template in the form ofsummary table was constructed for the data abstraction.The two authors (GT and AS) systematically used thedata extraction template to abstract data. The summarytable contained list of items pertaining to the study char-acteristics to concisely present all the included studies.The specific list of items included; study year, design ofthe study, study setting, sample size, study subjects, datacollection method, and study specific predicting factors.A quantitative data of cross-tabulation between the sub-ject’s characteristics (predicting factors) and the outcomevariable was also systematically abstracted. During thedata extraction of the exposure variables, we categorizedthe individual classifications shown for each variable in
the studies into two (exposed with the outcome andnon-exposed with the outcome). The non-exposed cat-egory was considered as the reference category of thevariables (e.g for place of residence, urban was the ex-posed and rural was the non-exposed category). Wethen put the corresponding combined numerical valueto make it ready for the quantitative synthesis. Duringthe data extraction, one of the papers (Bayou et al.2016) reported missing and incomplete data, and theprincipal author of the publication was contacted torequest further data via email. We received a re-sponse from the author, and were provided with therequested data. Disagreements between the two re-view authors were resolved by face to face discussionand reached a consensus.
Data synthesis and statistical analysisThe individual studies were concisely described using asummary table. The summary table particularly de-scribed the characteristics of the included studies andthe main findings. We conducted the quantitative syn-thesis using the Cochrane community Review ManagerSoftware (RevMan version 5.3 for windows) [50]. Sum-mary statistics (pooled effect sizes) in Odds Ratios with95% confidence intervals were calculated. We classifiedthe factors that showed significant association with theoutcome variable into three groups based on the threedelays model, though some overlapping exist betweenthem. Forest plots were used to graphically present themeta-analysis results. The presence of statistical hetero-geneity was checked by using the Chi2 test (Cochran Qtest) at p-value ≤0.05. The level of heterogeneity amongthe studies was quantified using the I2 statistics [51]where substantial heterogeneity was assumed if the I2
value was ≥50%. We conducted meta-analysis usingMantel–Haenszel random effects model when the studieswere substantially heterogeneous (I2 statistic ≥50%). Pooledestimate of the magnitude of the primary outcome variablewas conducted using stats direct (http://www.statsdirect.com) statistical software [52] using Stuart-Ord (inversedouble arcsine square root) method. We hypothesizedthat there could be variation in the factors that leadto delayed ANC between studies that defined delayedANC based on the WHO [10] recommendation with(≥12 weeks) and country specific recommendation[53] (≥16 weeks) due to the obvious difference inmagnitude of the outcome variable. Hence, subgroupanalysis was conducted based on comparison of outcomesfor studies that defined delayed initiation of ANC basedon (≥12 weeks) and (≥16 weeks), provided an adequatenumber of studies were available in the two groups. Theresult of the review was reported according to thePRISMA guideline for reporting [54].
Tesfaye et al. Reproductive Health (2017) 14:150 Page 4 of 17

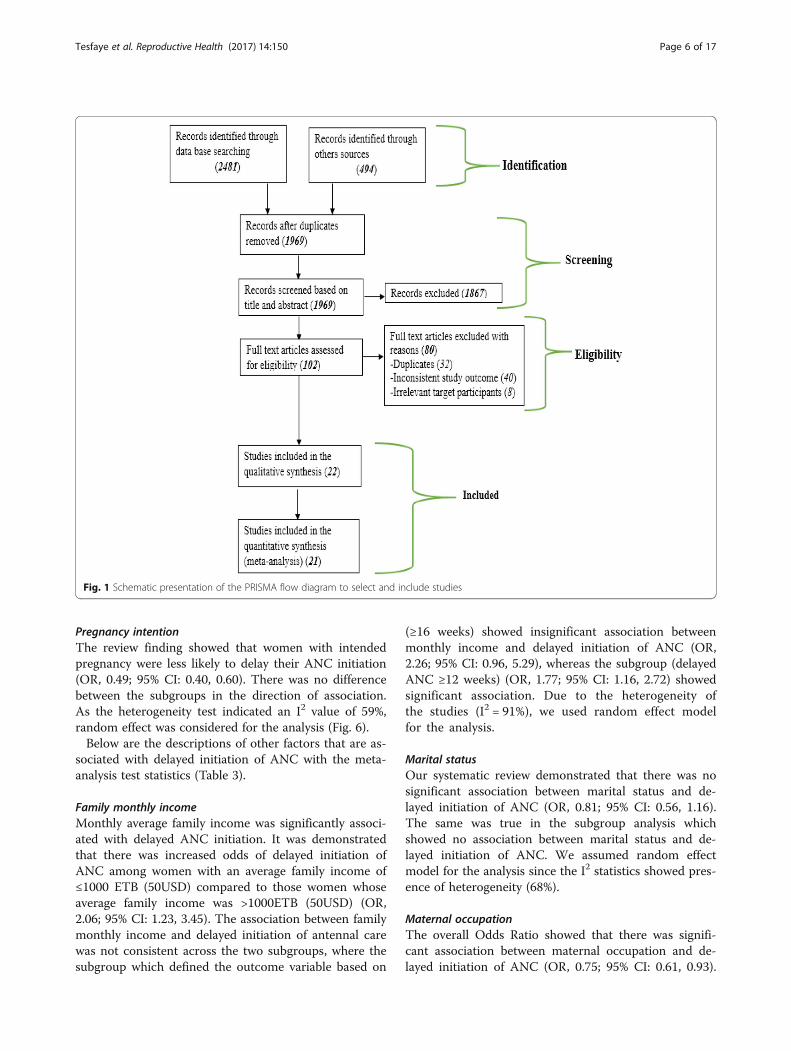
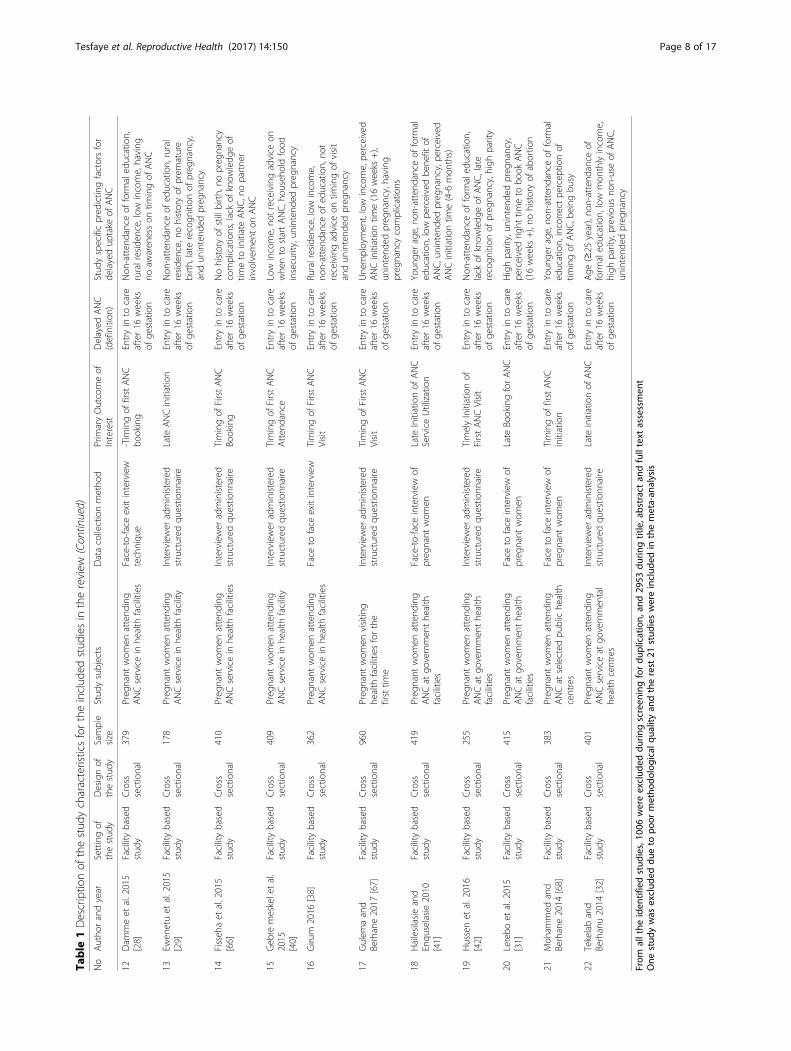
ResultsDescription of the studiesWe retrieved 2975 studies through searching the majorhealth and medical electronic databases and other rele-vant sources. From all the identified studies, 1006 arti-cles were removed due to duplication while 1969 studieswere retained for further screening. The remaining 1969studies were then screened for their eligibility based onthe title and abstract. Accordingly, 1867 studies were ex-cluded because of the incompatibility of the content pre-sented in the title and abstract of the studies with ourreview topic. Hence, the full text of the remaining 102studies were assessed for eligibility. During the full text as-sessment, 80 studies were excluded from the review be-cause of duplication, inconsistent study outcome, orirrelevant target participants. The remaining twenty twostudies were critically appraised and included in the re-view. After the critical appraisal of the studies, we ex-cluded one study from the quantitative synthesis due tothe relatively poor methodological quality and inconsistentstatistical report. Finally, twenty one studies were includedfor the pooled estimation of delayed initiation of ANCand factor analysis (Fig. 1). Among the included studies,there were seventeen published articles, three master the-ses, and one Ethiopian Demographic and Health Survey(DHS data). All of the included studies were cross-sectional by design and seventeen of the studies wereconducted in a facility setting (Table 1). Ten of the studiesincluded in the quantitative synthesis reported delayed ini-tiation of ANC based on (≥ 12 weeks), and the remainingstudies reported it based on (≥ 16 weeks).With regards to the demographic characteristics, the
study participants in the included studies were pregnantwomen or women who have at least had one birth in thefive or three years prior to the studies. The age of theparticipants’ were ranged from 15 to 49 years. Large ma-jority of the participants in the included studies wereurban residents. Moreover, higher proportion of the par-ticipants in the included studies were married andattended formal education (primary school and above).
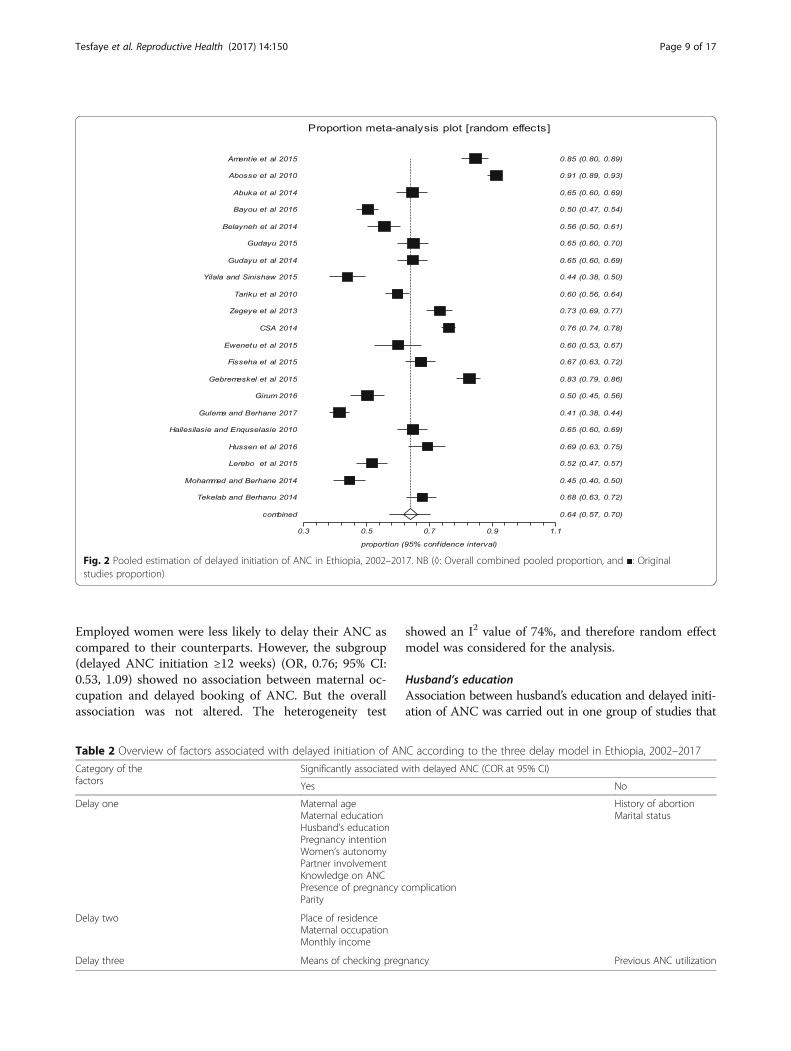
Magnitude of delayed initiation of ANCThe pooled estimate of the magnitude of delayed initi-ation of ANC in Ethiopia was 64% (95% CI: 57%, 70%)(Fig. 2). The result of the analysis for the magnitude ofdelayed initiation of ANC based on the studies that re-ported the outcome variable with (≥ 12 weeks) was 66%(95% CI: 56%, 76%), whereas based on the studies thatdefined the outcome variable with (≥ 16 weeks) it was62% (95% CI: 52%, 71%).
Factors associated with delayed initiation of ANCThe current review revealed various factors associatedwith delayed initiation of ANC in Ethiopia. Significantly
associated delay one factors include maternal age, mater-nal education, husband’s education, pregnancy intention,women’s autonomy, knowledge on ANC, partner involve-ment, pregnancy complication, and parity. Significantlyassociated delay two factors were maternal occupation,monthly income and place of residence. Means of checkingpregnancy was the only delay three factor that showed sta-tistically significant association with delayed ANC. The re-view also demonstrated that delay one factors such maritalstatus and history of abortion, and delay three factor (pre-vious use of ANC) were not significant predictors of de-layed attendance of ANC services (Table 2).
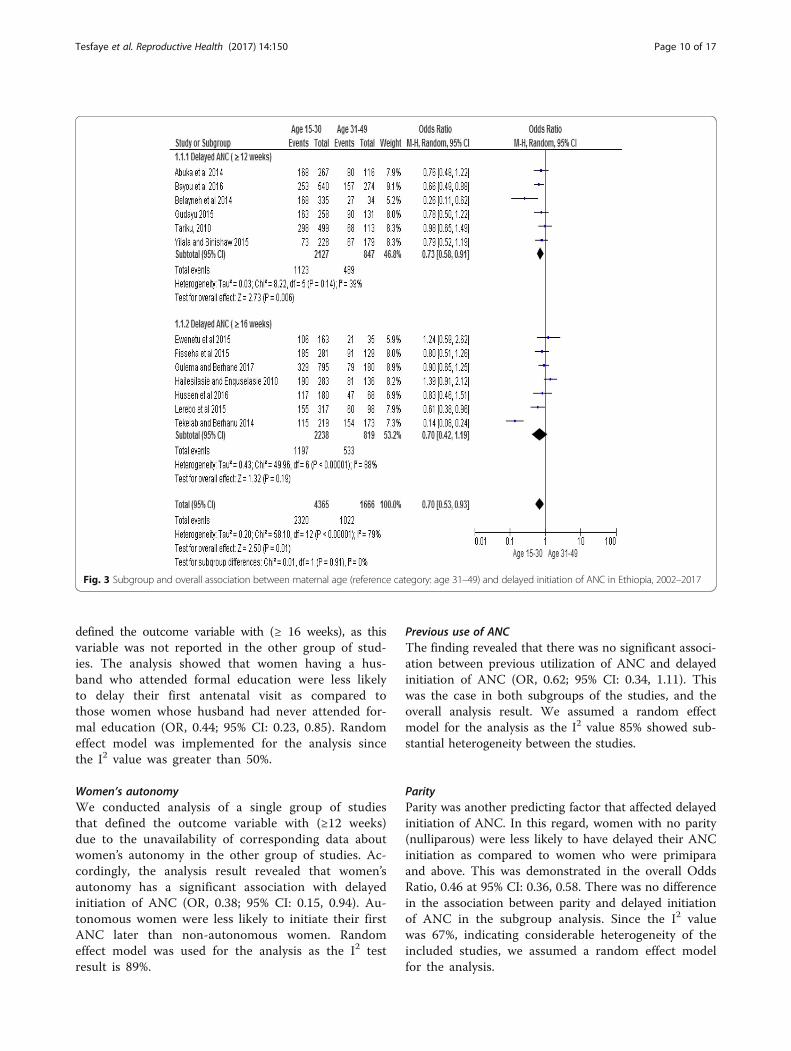
Maternal ageMaternal age was significantly associated with delayedinitiation of ANC. Women aged between 15 and 30 wereless likely to have delayed their first ANC booking ascompared to women aged 31 to 49 years of age (OR, 0.70;95% CI: 0.53, 0.93). However, the subgroup (delayed initi-ation ≥16 weeks) showed no association between maternalage and delayed booking of ANC (OR, 0.70; 95% CI:0.42, 1.19). But it did not affect the overall association.Random effect model was employed for the analysis as theI2 value was >50% (Fig. 3).
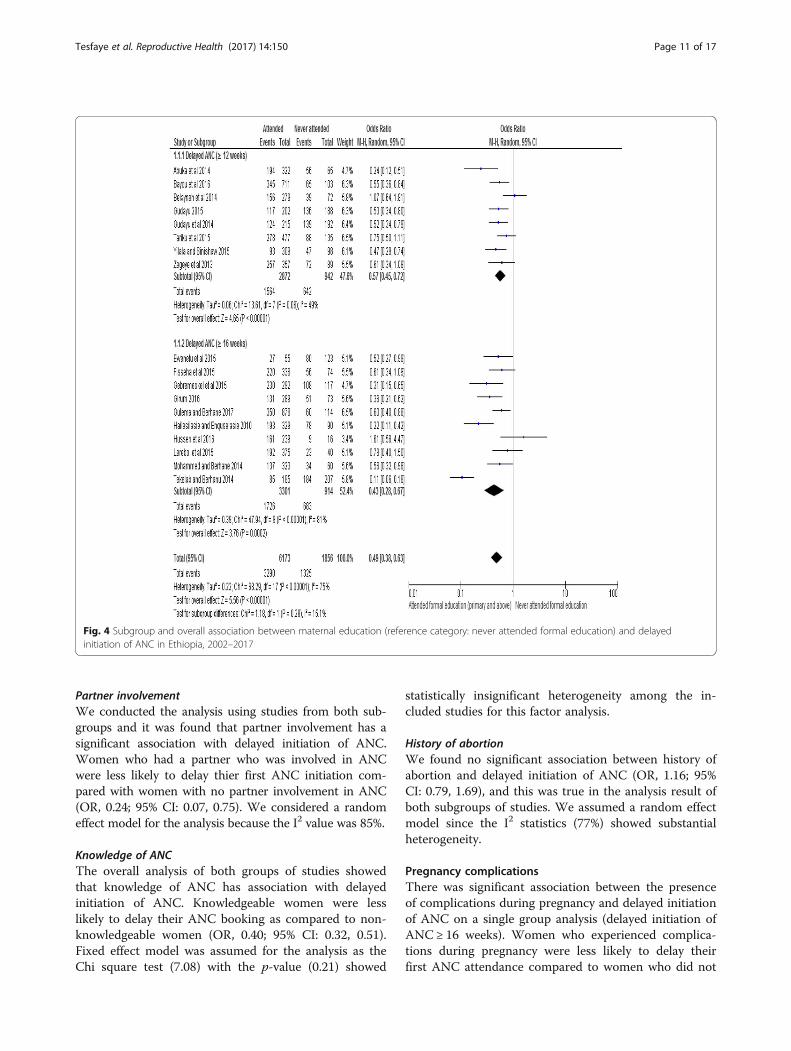
Maternal educationThe meta-analysis showed that maternal education wassignificantly associated with delayed ANC initiation. Theoverall Odds Ratio 0.49 at 95% CI: 0.38, 0.63 indicatedthat women who have attended primary or above levelof education were less likely to delay their first ANC visitas compared to women without formal education. Inspite of the heterogeneity of the studies, the findingshowed statistically significant association. The subgroupanalysis for studies with (≥12 weeks) (OR, 0.57; 95% CI:0.45, 0.72) and studies (≥16 weeks) (OR, 0.43; 95% CI:0.28, 0.67) both showed significant association betweenthe maternal educational status and delayed initiation ofANC. We used random effect model for the analysissince the I2 value was 75% (Fig. 4).
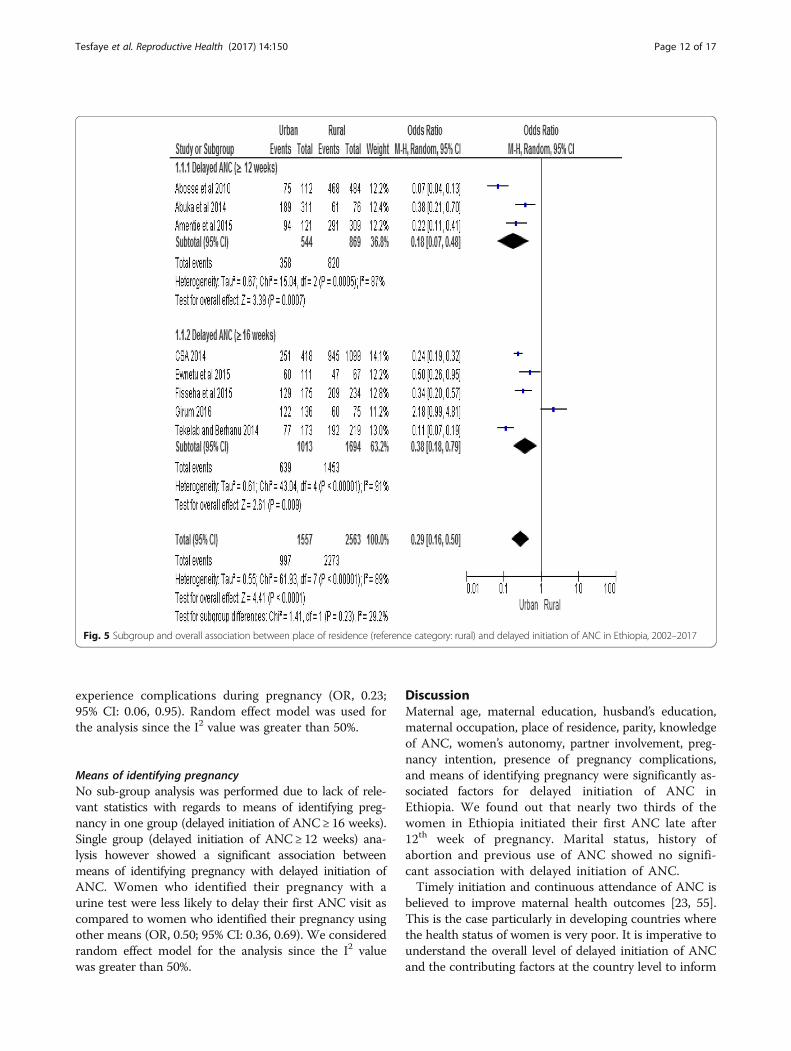
Place of residenceAccording to the factor analysis of the included studies,place of residence was significantly associated with de-layed initiation of ANC. Women who live in urban areawere less likely to have delayed initiation of ANC (OR,0.29, 95% CI: 0.16, 0.50). No difference was found interms of the direction of association between place ofresidence and delayed initiation of ANC in the sub-groups analysis. Random effect model was used for theanalysis since the heterogeneity test showed an overall I2
value of 89% (Fig. 5).
Tesfaye et al. Reproductive Health (2017) 14:150 Page 5 of 17
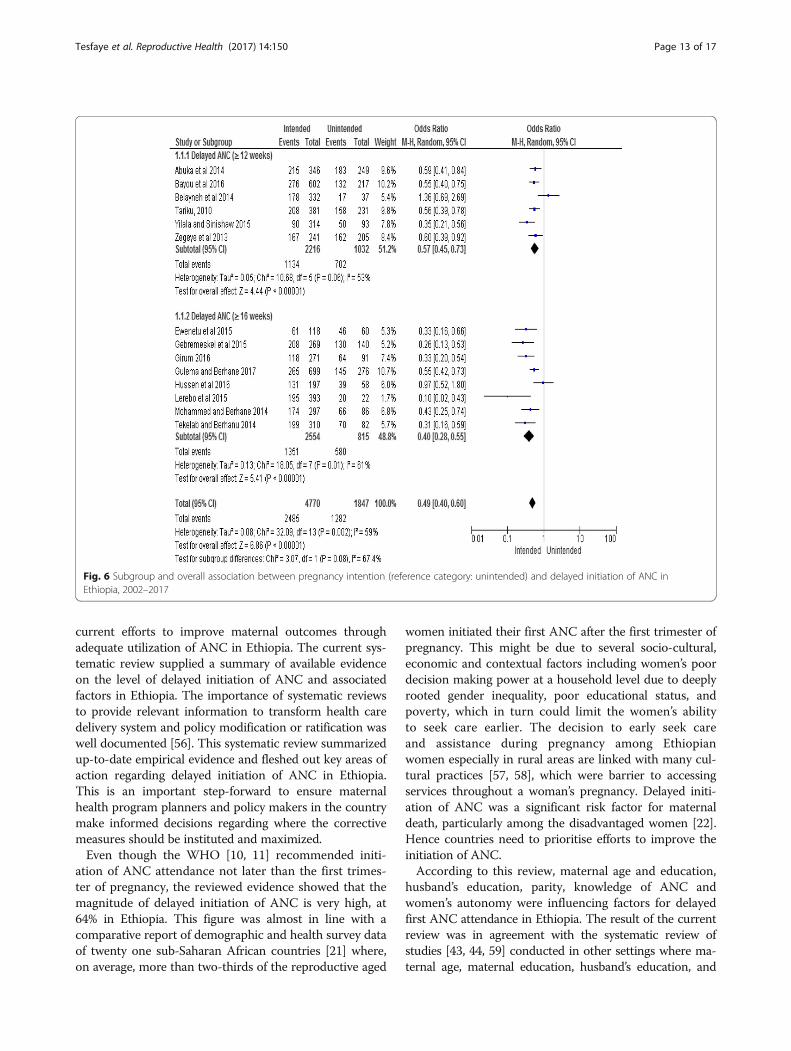
Pregnancy intentionThe review finding showed that women with intendedpregnancy were less likely to delay their ANC initiation(OR, 0.49; 95% CI: 0.40, 0.60). There was no differencebetween the subgroups in the direction of association.As the heterogeneity test indicated an I2 value of 59%,random effect was considered for the analysis (Fig. 6).Below are the descriptions of other factors that are as-
sociated with delayed initiation of ANC with the meta-analysis test statistics (Table 3).
Family monthly incomeMonthly average family income was significantly associ-ated with delayed ANC initiation. It was demonstratedthat there was increased odds of delayed initiation ofANC among women with an average family income of≤1000 ETB (50USD) compared to those women whoseaverage family income was >1000ETB (50USD) (OR,2.06; 95% CI: 1.23, 3.45). The association between familymonthly income and delayed initiation of antennal carewas not consistent across the two subgroups, where thesubgroup which defined the outcome variable based on
(≥16 weeks) showed insignificant association betweenmonthly income and delayed initiation of ANC (OR,2.26; 95% CI: 0.96, 5.29), whereas the subgroup (delayedANC ≥12 weeks) (OR, 1.77; 95% CI: 1.16, 2.72) showedsignificant association. Due to the heterogeneity ofthe studies (I2 = 91%), we used random effect modelfor the analysis.
Marital statusOur systematic review demonstrated that there was nosignificant association between marital status and de-layed initiation of ANC (OR, 0.81; 95% CI: 0.56, 1.16).The same was true in the subgroup analysis whichshowed no association between marital status and de-layed initiation of ANC. We assumed random effectmodel for the analysis since the I2 statistics showed pres-ence of heterogeneity (68%).
Maternal occupationThe overall Odds Ratio showed that there was signifi-cant association between maternal occupation and de-layed initiation of ANC (OR, 0.75; 95% CI: 0.61, 0.93).
Fig. 1 Schematic presentation of the PRISMA flow diagram to select and include studies
Tesfaye et al. Reproductive Health (2017) 14:150 Page 6 of 17
Table
1Descriptio
nof
thestud
ycharacteristicsfortheinclud
edstud
iesin
thereview
No
Autho
randyear
Settingof
thestud
yDesignof
thestud
ySample
size
Stud
ysubjects
Datacollectionmetho
dPrim
aryOutcomeof
Interest
Delayed
ANC
(definition
)Stud
yspecificpred
ictin
gfactorsfor
delayedup
take
ofANC
1Amen
tieet
al.2015
[39]
Com
mun
itybasedstud
yCross
sectional
536
Reprod
uctiveaged
wom
enwho
hadat
leaston
ebirthin
thefiveyearspriorto
thestud
y
Interviewer
administered
questio
nnaire
-Utilizationof
ANC
(uptake)
-Tim
ingof
firstANC
initiation
Entryin
tocare
after12
weeks
ofge
station
Placeof
reside
nce(living
inruralarea)
2Abo
sseet
al.2010
[27]
Com
mun
itybasedstud
yCross
sectional
710
Reprod
uctiveaged
wom
enwho
hadat
leaston
ebirthin
thefiveyearspriorto
thestud
y
Interviewer
administered
questio
nnaire
-Utilizationof
ANC
(uptake)
-Tim
ingof
firstANC
visit
Entryin
tocare
after12
weeks
ofge
station
Placeof
reside
nce(living
inruralarea)
3Abu
kaet
al.2014
[35]
Facilitybased
stud
yCross
sectional
406
Preg
nant
wom
enattend
ing
health
facility
Interviewer
administered
questio
nnaire
-Timingof
firstANC
booking
Entryin
tocare
after12
weeks
ofge
station
Age
(≥20
year),no
n-attend
ance
ofform
aled
ucation,
high
parity,
perceivedthat
timelyANCisno
tim
portant,no
thaving
inform
ation,
previous
non-useof
ANC
4Bayouet
al.2016
[36]
Com
mun
itybasedstud
yCross
sectional
814
Reprod
uctiveaged
wom
enwho
hadat
leaston
ebirthin
the
threeyearspriorto
thestud
y
Interviewer
administered
questio
nnaire
-Earlyinitiationof
ANC
-Atleastfour
ANC
visit
-Ade
quacyof
ANC
Entryin
tocare
after12
weeks
ofge
station
Uninten
dedpreg
nancyand
non-attend
ance
ofform
aled
ucation
5Belayneh
etal.2014
[34]
Facilitybased
stud
yCross
sectional
369
Preg
nant
wom
enattend
ing
ANCservicein
health
facility
Face-to-face
interview
techniqu
e-Tim
ingof
firstANC
booking
Entryin
tocare
after12
weeks
ofge
station
Non
-atten
danceof
form
aled
ucation,
olde
rage[30–49],previous
early
ANCvisit,pe
rceivedsufficien
tnu
mbe
rof
ANC(4+)
6Gud
ayu2015
[37]
Facilitybased
stud
yCross
sectional
390
Preg
nant
wom
enattend
ing
ANCservicein
health
facilities
Face-to-face
exitinterview
techniqu
e-LateANCbo
oking
Entryin
tocare
after12
weeks
ofge
station
Not
obtaininginform
ationon
right
timeto
initiate,pe
rceivedrig
httim
eto
book
ANC(12+
weeks),
non-autono
my,anduseof
urine
testto
iden
tifypreg
nancy
7Gud
ayuet
al.2014
[30]
Facilitybased
stud
yCross
sectional
407
Preg
nant
wom
enattend
ing
health
facility
Face-to-face
exitinterview
techniqu
e-Tim
ingof
firstANC
booking
Entryin
tocare
after12
weeks
ofge
station
Age
(>25),youn
gerageat
marriage
,preg
nancychecking
bymeans
othe
rthan
urinetest,p
erceived
right
time
tostartANC(12+
weeks),and
non-autono
my
8YilalaandSinishaw
2015
[33]
Facilitybased
stud
yCross
sectional
407
Preg
nant
wom
enattend
ing
antenatalcareclinicin
health
facility
Face-to-face
exitinterview
techniqu
e-Lateinitiationof
ANC
Entryin
tocare
after12
weeks
ofge
station
Non
-atten
danceof
form
aled
ucation,
poor
know
ledg
eof
ANC,n
otreceivingadvice
from
HEW
,not
gettingadvice
onANCbo
oking,
perceivedrig
httim
eof
ANC(12+
weeks)
9Ze
geye
etal.2013
[65]
Facilitybased
stud
yCross
sectional
446
Preg
nant
wom
enattend
ing
health
facility
Face-to-face
exitinterview
techniqu
e-EarlyANCvisit
Entryin
tocare
after12
weeks
ofge
station
Highparity,lack
ofknow
ledg
eof
ANC,
unintend
edpreg
nancy
10Tarikuet
al.2010
Facilitybased
stud
yCross
sectional
612
Preg
nant
wom
enattend
ing
health
facility
Face
toface
exitinterview
-Tim
ingof
firstANC
booking
Entryin
tocare
after12
weeks
ofge
station
Highparity,un
intend
edpreg
nancy,
obtainingadvice
onwhe
nto
book
firstANC
11CSA
2014
[20]
Com
mun
itybasedstud
yCross
sectional
(DHSdata)
1571
Reprod
uctiveaged
wom
enwho
hadat
leaston
ebirth
inthefiveyearspriorto
thesurvey
Interviewer
administered
questio
nnaire
-Tim
ingof
ANC
initiation
-Atleaston
eANC
visit
Entryin
tocare
after16
weeks
ofge
station
Placeof
reside
nce(living
inruralarea)
Tesfaye et al. Reproductive Health (2017) 14:150 Page 7 of 17
Table
1Descriptio
nof
thestud
ycharacteristicsfortheinclud
edstud
iesin
thereview
(Con
tinued)
No
Autho
randyear
Settingof
thestud
yDesignof
thestud
ySample
size
Stud
ysubjects
Datacollectionmetho
dPrim
aryOutcomeof
Interest
Delayed
ANC
(definition
)Stud
yspecificpred
ictin
gfactorsfor
delayedup
take
ofANC
12Dam
meet
al.2015
[28]
Facilitybased
stud
yCross
sectional
379
Preg
nant
wom
enattend
ing
ANCservicein
health
facilities
Face-to-face
exitinterview
techniqu
e-Tim
ingof
firstANC
booking
Entryin
tocare
after16
weeks
ofge
station
Non
-atten
danceof
form
aled
ucation,
ruralresiden
ce,low
income,having
noaw
aren
esson
timingof
ANC
13Ew
enetuet
al.2015
[29]
Facilitybased
stud
yCross
sectional
178
Preg
nant
wom
enattend
ing
ANCservicein
health
facility
Interviewer
administered
structured
questio
nnaire
Late
ANCinitiation
Entryin
tocare
after16
weeks
ofge
station
Non
-atten
danceof
education,
rural
reside
nce,no
historyof
prem
ature
birth,
late
recogn
ition
ofpreg
nancy,
andun
intend
edpreg
nancy
14Fisseh
aet
al.2015
[66]
Facilitybased
stud
yCross
sectional
410
Preg
nant
wom
enattend
ing
ANCservicein
health
facilities
Interviewer
administered
structured
questio
nnaire
Timingof
FirstANC
Booking
Entryin
tocare
after16
weeks
ofge
station
Nohistoryof
stillbirth,
nopreg
nancy
complications,lackof
know
ledg
eof
timeto
initiateANC,n
opartne
rinvolvem
enton
ANC
15Geb
remeskeletal.
2015
[40]
Facilitybased
stud
yCross
sectional
409
Preg
nant
wom
enattend
ing
ANCservicein
health
facility
Interviewer
administered
structured
questio
nnaire
Timingof
FirstANC
Atten
dance
Entryin
tocare
after16
weeks
ofge
station
Low
income,no
treceivingadvice
onwhe
nto
startANC,h
ouseho
ldfood
insecurity,un
intend
edpreg
nancy
16Giru
m2016
[38]
Facilitybased
stud
yCross
sectional
362
Preg
nant
wom
enattend
ing
ANCservicein
health
facilities
Face
toface
exitinterview
Timingof
FirstANC
Visit
Entryin
tocare
after16
weeks
ofge
station
Ruralresiden
ce,low
income,
non-attend
ance
ofed
ucation,
not
receivingadvice
ontim
ingof
visit
andun
intend
edpreg
nancy
17Gulem
aand
Berhane2017
[67]
Facilitybased
stud
yCross
sectional
960
Preg
nant
wom
envisitin
ghe
alth
facilitiesforthe
firsttim
e
Interviewer
administered
structured
questio
nnaire
Timingof
FirstANC
Visit
Entryin
tocare
after16
weeks
ofge
station
Une
mploymen
t,low
income,pe
rceived
ANCinitiationtim
e(16weeks
+),
unintend
edpreg
nancy,having
preg
nancycomplications
18Hailesilasieand
Enqu
selasie2010
[41]
Facilitybased
stud
yCross
sectional
419
Preg
nant
wom
enattend
ing
ANCat
governmen
the
alth
facilities
Face-to-face
interview
ofpreg
nant
wom
enLate
Initiationof
ANC
ServiceUtilization
Entryin
tocare
after16
weeks
ofge
station
Youn
gerage,no
n-attend
ance
ofform
aled
ucation,
low
perceivedbe
nefit
ofANC,uninten
dedpreg
nancy,pe
rceived
ANCinitiationtim
e(4-6
mon
ths)
19Hussenet
al.2016
[42]
Facilitybased
stud
yCross
sectional
255
Preg
nant
wom
enattend
ing
ANCat
governmen
the
alth
facilities
Interviewer
administered
structured
questio
nnaire
TimelyInitiationof
FirstANCVisit
Entryin
tocare
after16
weeks
ofge
station
Non
-atten
danceof
form
aled
ucation,
lack
ofknow
ledg
eof
ANC,late
recogn
ition
ofpreg
nancy,high
parity
20Lerebo
etal.2015
[31]
Facilitybased
stud
yCross
sectional
415
Preg
nant
wom
enattend
ing
ANCat
governmen
the
alth
facilities
Face
toface
interview
ofpreg
nant
wom
enLate
BookingforANC
Entryin
tocare
after16
weeks
ofge
station
Highparity,un
intend
edpreg
nancy,
perceivedrig
httim
eto
book
ANC
(16weeks
+),no
historyof
abortio
n
21Moh
ammed
and
Berhane2014
[68]
Facilitybased
stud
yCross
sectional
383
Preg
nant
wom
enattend
ing
ANCat
selected
publiche
alth
centres
Face
toface
interview
ofpreg
nant
wom
enTimingof
firstANC
initiation
Entryin
tocare
after16
weeks
ofge
station
Youn
gerage,no
n-attend
ance
ofform
aled
ucation,
incorrectpe
rcep
tionof
timingof
ANC,b
eing
busy
22Tekelaband
Berhanu2014
[32]
Facilitybased
stud
yCross
sectional
401
Preg
nant
wom
enattend
ing
ANCserviceat
governmen
tal
health
centres
Interviewer
administered
structured
questio
nnaire
Late
initiationof
ANC
Entryin
tocare
after16
weeks
ofge
station
Age
(≥25
year),no
n-attend
ance
ofform
aled
ucation,
low
mon
thlyincome,
high
parity,previous
non-useof
ANC,
unintend
edpreg
nancy
From
allthe
iden
tifiedstud
ies,10
06wereexclud
eddu
ringscreen
ingfordu
plication,
and29
53du
ringtitle,abstractan
dfulltext
assessmen
tOne
stud
ywas
exclud
eddu
eto
poor
metho
dologicalq
ualityan
dtherest
21stud
ieswereinclud
edin
themeta-an
alysis
Tesfaye et al. Reproductive Health (2017) 14:150 Page 8 of 17
Employed women were less likely to delay their ANC ascompared to their counterparts. However, the subgroup(delayed ANC initiation ≥12 weeks) (OR, 0.76; 95% CI:0.53, 1.09) showed no association between maternal oc-cupation and delayed booking of ANC. But the overallassociation was not altered. The heterogeneity test
showed an I2 value of 74%, and therefore random effectmodel was considered for the analysis.
Husband’s educationAssociation between husband’s education and delayed initi-ation of ANC was carried out in one group of studies that
Fig. 2 Pooled estimation of delayed initiation of ANC in Ethiopia, 2002–2017. NB (◊: Overall combined pooled proportion, and ■: Originalstudies proportion)
Table 2 Overview of factors associated with delayed initiation of ANC according to the three delay model in Ethiopia, 2002–2017
Category of thefactors
Significantly associated with delayed ANC (COR at 95% CI)
Yes No
Delay one Maternal ageMaternal educationHusband’s educationPregnancy intentionWomen’s autonomyPartner involvementKnowledge on ANCPresence of pregnancy complicationParity
History of abortionMarital status
Delay two Place of residenceMaternal occupationMonthly income
Delay three Means of checking pregnancy Previous ANC utilization
Tesfaye et al. Reproductive Health (2017) 14:150 Page 9 of 17
defined the outcome variable with (≥ 16 weeks), as thisvariable was not reported in the other group of stud-ies. The analysis showed that women having a hus-band who attended formal education were less likelyto delay their first antenatal visit as compared tothose women whose husband had never attended for-mal education (OR, 0.44; 95% CI: 0.23, 0.85). Randomeffect model was implemented for the analysis sincethe I2 value was greater than 50%.
Women’s autonomyWe conducted analysis of a single group of studiesthat defined the outcome variable with (≥12 weeks)due to the unavailability of corresponding data aboutwomen’s autonomy in the other group of studies. Ac-cordingly, the analysis result revealed that women’sautonomy has a significant association with delayedinitiation of ANC (OR, 0.38; 95% CI: 0.15, 0.94). Au-tonomous women were less likely to initiate their firstANC later than non-autonomous women. Randomeffect model was used for the analysis as the I2 testresult is 89%.
Previous use of ANCThe finding revealed that there was no significant associ-ation between previous utilization of ANC and delayedinitiation of ANC (OR, 0.62; 95% CI: 0.34, 1.11). Thiswas the case in both subgroups of the studies, and theoverall analysis result. We assumed a random effectmodel for the analysis as the I2 value 85% showed sub-stantial heterogeneity between the studies.
ParityParity was another predicting factor that affected delayedinitiation of ANC. In this regard, women with no parity(nulliparous) were less likely to have delayed their ANCinitiation as compared to women who were primiparaand above. This was demonstrated in the overall OddsRatio, 0.46 at 95% CI: 0.36, 0.58. There was no differencein the association between parity and delayed initiationof ANC in the subgroup analysis. Since the I2 valuewas 67%, indicating considerable heterogeneity of theincluded studies, we assumed a random effect modelfor the analysis.
Fig. 3 Subgroup and overall association between maternal age (reference category: age 31–49) and delayed initiation of ANC in Ethiopia, 2002–2017
Tesfaye et al. Reproductive Health (2017) 14:150 Page 10 of 17
Partner involvementWe conducted the analysis using studies from both sub-groups and it was found that partner involvement has asignificant association with delayed initiation of ANC.Women who had a partner who was involved in ANCwere less likely to delay thier first ANC initiation com-pared with women with no partner involvement in ANC(OR, 0.24; 95% CI: 0.07, 0.75). We considered a randomeffect model for the analysis because the I2 value was 85%.
Knowledge of ANCThe overall analysis of both groups of studies showedthat knowledge of ANC has association with delayedinitiation of ANC. Knowledgeable women were lesslikely to delay their ANC booking as compared to non-knowledgeable women (OR, 0.40; 95% CI: 0.32, 0.51).Fixed effect model was assumed for the analysis as theChi square test (7.08) with the p-value (0.21) showed
statistically insignificant heterogeneity among the in-cluded studies for this factor analysis.
History of abortionWe found no significant association between history ofabortion and delayed initiation of ANC (OR, 1.16; 95%CI: 0.79, 1.69), and this was true in the analysis result ofboth subgroups of studies. We assumed a random effectmodel since the I2 statistics (77%) showed substantialheterogeneity.
Pregnancy complicationsThere was significant association between the presenceof complications during pregnancy and delayed initiationof ANC on a single group analysis (delayed initiation ofANC ≥ 16 weeks). Women who experienced complica-tions during pregnancy were less likely to delay theirfirst ANC attendance compared to women who did not
Fig. 4 Subgroup and overall association between maternal education (reference category: never attended formal education) and delayedinitiation of ANC in Ethiopia, 2002–2017
Tesfaye et al. Reproductive Health (2017) 14:150 Page 11 of 17
experience complications during pregnancy (OR, 0.23;95% CI: 0.06, 0.95). Random effect model was used forthe analysis since the I2 value was greater than 50%.
Means of identifying pregnancyNo sub-group analysis was performed due to lack of rele-vant statistics with regards to means of identifying preg-nancy in one group (delayed initiation of ANC ≥ 16 weeks).Single group (delayed initiation of ANC ≥ 12 weeks) ana-lysis however showed a significant association betweenmeans of identifying pregnancy with delayed initiation ofANC. Women who identified their pregnancy with aurine test were less likely to delay their first ANC visit ascompared to women who identified their pregnancy usingother means (OR, 0.50; 95% CI: 0.36, 0.69). We consideredrandom effect model for the analysis since the I2 valuewas greater than 50%.
DiscussionMaternal age, maternal education, husband’s education,maternal occupation, place of residence, parity, knowledgeof ANC, women’s autonomy, partner involvement, preg-nancy intention, presence of pregnancy complications,and means of identifying pregnancy were significantly as-sociated factors for delayed initiation of ANC inEthiopia. We found out that nearly two thirds of thewomen in Ethiopia initiated their first ANC late after12th week of pregnancy. Marital status, history ofabortion and previous use of ANC showed no signifi-cant association with delayed initiation of ANC.Timely initiation and continuous attendance of ANC is
believed to improve maternal health outcomes [23, 55].This is the case particularly in developing countries wherethe health status of women is very poor. It is imperative tounderstand the overall level of delayed initiation of ANCand the contributing factors at the country level to inform
Fig. 5 Subgroup and overall association between place of residence (reference category: rural) and delayed initiation of ANC in Ethiopia, 2002–2017
Tesfaye et al. Reproductive Health (2017) 14:150 Page 12 of 17
current efforts to improve maternal outcomes throughadequate utilization of ANC in Ethiopia. The current sys-tematic review supplied a summary of available evidenceon the level of delayed initiation of ANC and associatedfactors in Ethiopia. The importance of systematic reviewsto provide relevant information to transform health caredelivery system and policy modification or ratification waswell documented [56]. This systematic review summarizedup-to-date empirical evidence and fleshed out key areas ofaction regarding delayed initiation of ANC in Ethiopia.This is an important step-forward to ensure maternalhealth program planners and policy makers in the countrymake informed decisions regarding where the correctivemeasures should be instituted and maximized.Even though the WHO [10, 11] recommended initi-
ation of ANC attendance not later than the first trimes-ter of pregnancy, the reviewed evidence showed that themagnitude of delayed initiation of ANC is very high, at64% in Ethiopia. This figure was almost in line with acomparative report of demographic and health survey dataof twenty one sub-Saharan African countries [21] where,on average, more than two-thirds of the reproductive aged
women initiated their first ANC after the first trimester ofpregnancy. This might be due to several socio-cultural,economic and contextual factors including women’s poordecision making power at a household level due to deeplyrooted gender inequality, poor educational status, andpoverty, which in turn could limit the women’s abilityto seek care earlier. The decision to early seek careand assistance during pregnancy among Ethiopianwomen especially in rural areas are linked with many cul-tural practices [57, 58], which were barrier to accessingservices throughout a woman’s pregnancy. Delayed initi-ation of ANC was a significant risk factor for maternaldeath, particularly among the disadvantaged women [22].Hence countries need to prioritise efforts to improve theinitiation of ANC.According to this review, maternal age and education,
husband’s education, parity, knowledge of ANC andwomen’s autonomy were influencing factors for delayedfirst ANC attendance in Ethiopia. The result of the currentreview was in agreement with the systematic review ofstudies [43, 44, 59] conducted in other settings where ma-ternal age, maternal education, husband’s education, and
Fig. 6 Subgroup and overall association between pregnancy intention (reference category: unintended) and delayed initiation of ANC inEthiopia, 2002–2017
Tesfaye et al. Reproductive Health (2017) 14:150 Page 13 of 17
parity were the influencing factors for delayed initiation ofANC. The possible reason for older women aged 31 to 49delaying their first ANC might be that they most likely areuneducated, have poor knowledge of ANC, have experi-enced pregnancies without complications previously, areless fearful unlike younger women and may be more likelyto be multiparous. Education of the mother and husbandcould play a great role in improving awareness of healthmatters in general, and the importance of ANC in particu-lar. Having a better awareness may enable women to seekANC and utilize the service early in pregnancy. This wasparticularly reflected in the systematic review of studiesamong non-western women in industrialized countries[45] where women’s low level of educational status was as-sociated with late entry into ANC.Furthermore, a lack of knowledge about ANC is posi-
tively associated with delayed initiation of ANC. Womenwho had been provided with information regarding ANC,pregnancy risks and danger signs were more likely to initi-ate ANC early compared to women who did not haveknowledge of these issues. This could motivate the womento initiate ANC early to better avoid the risks associatedwith pregnancy. It is anticipated that well informedwomen were more likely to make judicious choices aboutthe proper utilization of ANC. It was also found that
women’s autonomy was a significant predictor of delayedinitiation of ANC where non-autonomous women weremore likely to postpone ANC, which could be due to thefact that they were under the influence of their partner orfamily (especially in male headed households), restrictedto comply with family norms, had lack of family or so-cial support, and a partner who was not available orwho refused to accompany them. This was demon-strated in a systematic review of studies in the develop-ing countries [44], where social support from familymembers, extent of ties within social networks, andobtaining health information from these sources highlyinfluence timely utilization of ANC.Additionally, the meta-analysis revealed that place of
residence, maternal occupation, monthly income, andpartner involvement were significantly associated withdelayed ANC initiation. Rural women were more likelyto delay their first ANC attendance than urban women.This could be explained by the fact that urban womenwould most likely have easy access to health care facilities,have a good awareness of health matters, and have betterexposure to media. Moreover, unemployed women weremore likely to delay initiation of ANC as compared toemployed women. A similar finding was reported in othersystematic reviews [43, 45] where not being in employment
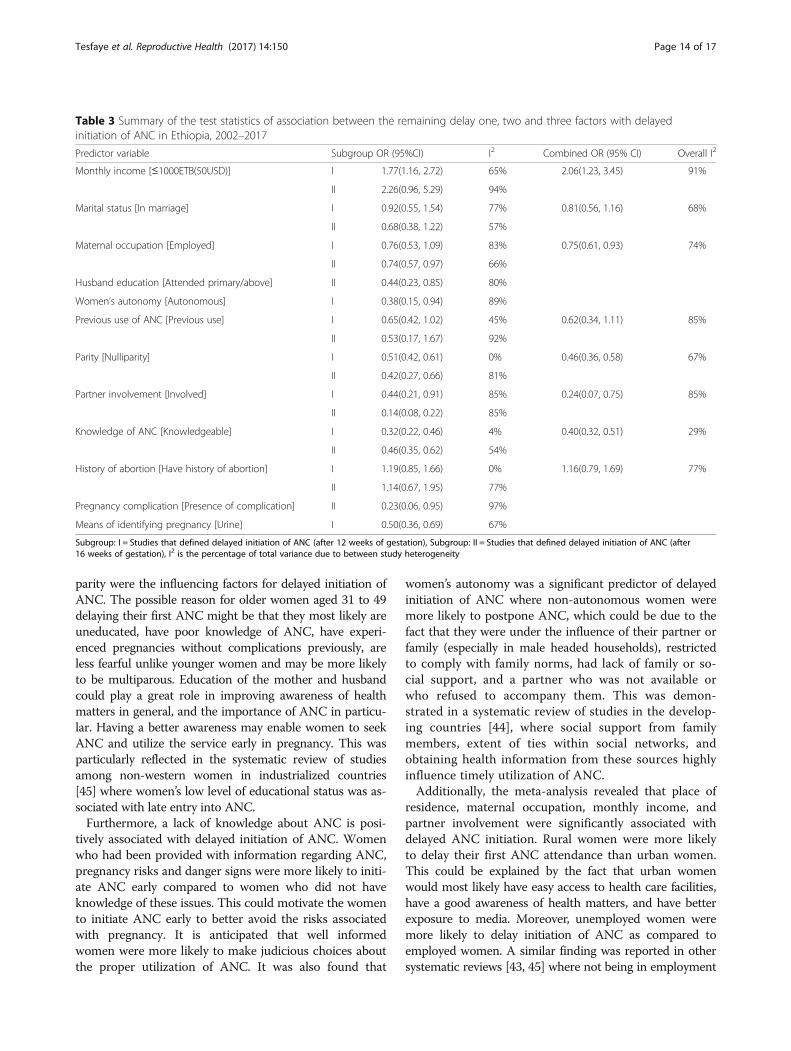
Table 3 Summary of the test statistics of association between the remaining delay one, two and three factors with delayedinitiation of ANC in Ethiopia, 2002–2017
Predictor variable Subgroup OR (95%CI) I2 Combined OR (95% CI) Overall I2
Monthly income [≤1000ETB(50USD)] I 1.77(1.16, 2.72) 65% 2.06(1.23, 3.45) 91%
II 2.26(0.96, 5.29) 94%
Marital status [In marriage] I 0.92(0.55, 1.54) 77% 0.81(0.56, 1.16) 68%
II 0.68(0.38, 1.22) 57%
Maternal occupation [Employed] I 0.76(0.53, 1.09) 83% 0.75(0.61, 0.93) 74%
II 0.74(0.57, 0.97) 66%
Husband education [Attended primary/above] II 0.44(0.23, 0.85) 80%
Women’s autonomy [Autonomous] I 0.38(0.15, 0.94) 89%
Previous use of ANC [Previous use] I 0.65(0.42, 1.02) 45% 0.62(0.34, 1.11) 85%
II 0.53(0.17, 1.67) 92%
Parity [Nulliparity] I 0.51(0.42, 0.61) 0% 0.46(0.36, 0.58) 67%
II 0.42(0.27, 0.66) 81%
Partner involvement [Involved] I 0.44(0.21, 0.91) 85% 0.24(0.07, 0.75) 85%
II 0.14(0.08, 0.22) 85%
Knowledge of ANC [Knowledgeable] I 0.32(0.22, 0.46) 4% 0.40(0.32, 0.51) 29%
II 0.46(0.35, 0.62) 54%
History of abortion [Have history of abortion] I 1.19(0.85, 1.66) 0% 1.16(0.79, 1.69) 77%
II 1.14(0.67, 1.95) 77%
Pregnancy complication [Presence of complication] II 0.23(0.06, 0.95) 97%
Means of identifying pregnancy [Urine] I 0.50(0.36, 0.69) 67%
Subgroup: I = Studies that defined delayed initiation of ANC (after 12 weeks of gestation), Subgroup: II = Studies that defined delayed initiation of ANC (after16 weeks of gestation), I2 is the percentage of total variance due to between study heterogeneity
Tesfaye et al. Reproductive Health (2017) 14:150 Page 14 of 17

explained women’s delayed entry into the care. It was alsoevidenced that women with high economic status weremore likely to receive ANC earlier than those with a lowereconomic status [43, 44]. These financial constraints are inturn related to other barriers to seeking help, includingtransportation costs, the cost of obtaining care, or labora-tory tests [60, 61].Moreover, our finding suggests that women whose
partner was involved in ANC were less likely to delaytheir first ANC attendance than women whose partnerwas not involved in ANC. Partner involvement in termsof initiating and/or supporting the idea to utilize ANCearly, or by accompanying the pregnant mother to thehealth facility may have an important impact on theearly attendance of ANC. In many traditions, the in-volvement of men in reproductive health has not beenconsidered an important issue. In general male partnersdid not accompany their wives to attend ANC and othermaternal health services [43]. The husband’s lack of in-volvement in ANC may immensely affect the women’scapability to initiate ANC early. It was found in a sys-tematic review [62] that the involvement of men in ANChas a positive influence on the overall uptake of the ser-vice and its early attendance.Furthermore, the meta-analysis identified factors such
as pregnancy intention, presence of pregnancy complica-tions and means of identifying pregnancy as an import-ant factors that affect delayed initiation of ANC. Thisfinding is consistent with a systematic review of smallscale studies conducted in both developed and develop-ing countries [63] on the relationship between preg-nancy intention and timely initiation as well as obtainingadequate ANC. It was revealed that unintended preg-nancy has a strong association with delayed initiation offirst ANC services. Another systematic review [44] con-firmed that women whose pregnancy was unintendedtended to initiate ANC later than the first trimester ofpregnancy. With regards to complications during preg-nancy, the findings of this study is similar to a systematicreview of literature [43] conducted in developing coun-tries where pregnant women who did not experience ob-stetric complications were more likely to delay their firstANC compared to their counterparts.In the current systematic review and meta-analysis, we
observed some discrepancies in the included studies indefining the outcome variable “delayed initiation ofANC”. Half of the included studies defined delayed initi-ation of ANC based on the cut-off point of 12 weeks ofgestation, whereas the rest of the studies defined it basedon 16 weeks. However the WHO [10, 11] defined lateANC initiation as entry into care after 12th week of preg-nancy. Conversely, in this review we noticed a contrast-ing type of definition across several studies [27–42] aswell as ANC practice in health facilities [53], implying
that there was poor compliance of the WHO recom-mendation on the timing of first ANC initiation inEthiopia. Countries might prefer to adapt or contextual-ise the original clinical practice guidelines with somechanges, depending on their setting, to effectively imple-ment the recommendations. Even if recommendationsfrom the parent clinical practice guidelines can beadapted, how they are implemented needs to addresslocal issues. Thus countries may need to contextualiseguideline by addressing those implementation issues sothat care becomes more relevant to the local environ-ments [64]. However, at least there should not be incon-sistencies between the implemented specific healthrecommendation within the country’s health care deliv-ery system and the health research arena. Hence, we rec-ommend to concerned parties in the health sector inEthiopia, particularly the health research scholars, thatthere is a need to adhere to the WHO recommendedguideline on the timing of ANC initiation. Moreover,any further adapted or contextualised guideline on thetiming of ANC initiation needs to be followed or imple-mented consistently in a standardized way.The current systematic review and meta-analysis was not
without limitations. The first limitation was the exclusionof qualitative studies from the review, which might revealother important factors affecting women’s behaviour todelay ANC attendance or might otherwise corroborate thequantitative findings. Secondly, since our meta-analysisused Crude Odds Ratios, it might be difficult to fully ascer-tain the effect of the exposure factors on the outcome ofinterest. Thirdly, as all the included studies were cross-sectional by design, it is difficult to establish temporal rela-tionship between the outcome and exposure variables.Lastly, conducting meta-analysis despite the inherentheterogeneity between the included studies might have af-fected the quantitative findings. Our systematic review andmeta-analysis also has some strengths. In this regard, weconsidered selection and inclusion of both published andunpublished literature which has the potential to minimizepublication bias. Moreover, our search strategy was exten-sive using a number of major medical databases andother search engines. Lastly, we conducted a sub-groupanalysis of studies that employed different definitions ofdelayed initiation of ANC to appreciate the independ-ent subgroup findings.
ConclusionThe current review revealed that nearly two thirds ofwomen were delaying their first ANC visit in Ethiopia.The review pointed out various factors attributed to highlevel of delayed initiation of ANC in Ethiopia. Amongthese maternal age, place of residence, maternal educa-tion, husband’s education, maternal occupation, familymonthly income, pregnancy intention, parity, knowledge
Tesfaye et al. Reproductive Health (2017) 14:150 Page 15 of 17

of ANC, women’s autonomy, partner involvement, prob-lem during pregnancy, and means of identifying pregnancyshowed significant association with delayed initiation ofANC. Therefore, intervention efforts to improve ANCutilization in Ethiopia require targeting these impedingfactors. Moreover, strategies should be designed to inten-sify advocacy of female education, women’s empowermentactivities need to be continued through economic re-forms, family planning programs should be strength-ened to reduce unintended pregnancies, and partnerinvolvement in ANC should be promoted through dif-ferent means of communication. Further qualitativestudies are recommended to gain further insight intothe societal and health system barriers that contributeto delayed initiation of ANC in Ethiopia.
Additional files
Additional file 1: PRISMA-P (Preferred Reporting Items for Systematicreview and Meta-Analysis Protocols) 2015 checklist: recommended itemsto address in a systematic review protocol*. (DOC 85 kb)
Additional file 2: Search Strategy. (DOCX 28 kb)
AbbreviationsANC: Antenatal care; CI: Confidence interval; DHS: Demographic and HealthSurvey; ETB: Ethiopian birr; JBI: Joanna Briggs Institute; MAStARI: Meta-Analysisof Statistics Assessment and Review Instrument; M-H: Mantel–Haenszel;NSW: New South Wales; OR: Odds ratio; PRISMA: Preferred Reporting Items forSystematic Reviews and Meta-Analyses Protocols; USD: United States Dollar;WHO: World Health Organization
AcknowledgmentsWe are very grateful to the University of Newcastle, Australia for providing afull scholarship for the corresponding author, and free access to the digitalonline library to search the electronic databases that were considered forthis review. We also would like to acknowledge Haramaya University forproviding free internet access and an office.
Ethical approval and consent to participateNot applicable.
FundingNot applicable.
Availability of data and materialsThe data that support the review findings of this study are available uponsubmitting a reasonable request to the corresponding author.
Authors’ contributionsGT, DL, CC, RS conceptualized the design of the systematic review. GTdrafted the manuscript and is the guarantor of the review. All authorscontributed to the development of the article search strategy, setting studyselection criteria, the strategy for assessment of risk of bias, and dataabstraction form. GT and AS involved in the screening, assessment ofeligibility, selection of studies and critical appraisal as well as data extraction.DL, CC, AS and RS have participated in critically revising the manuscript forimportant intellectual contents. All authors read, provided feedback andapproved the final manuscript.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims in publishedmaps and institutional affiliations.
Author details1Research Centre for Generational Health and Ageing, Faculty of Health andMedicine, University of Newcastle, Newcastle, Australia. 2School of PublicHealth, College of Health and Medical Sciences, Haramaya University, Harar,Ethiopia. 3Mothers and Babies Research Centre, Faculty of Health andMedicine, University of Newcastle, Newcastle, Australia.
Received: 18 July 2017 Accepted: 8 November 2017
References1. Prata N, Passano P, Sreenivas A, Gerdts C. Maternal mortality in developing
countries: challenges in scaling-up priority interventions. Women's Health.2010;6(2):311–27.
2. WHO. Maternal mortality Fact sheet. 2016.3. WHO. Trends in Maternal Mortality: 1990 to 2015 estimates by WHO,
UNICEF, UNFPA, World Bank Group and the United Nations PopulationDivision Excutive summary. 2015.
4. WHO. Trends in Maternal Mortality: 1990 to 2013. 2014.5. Birmeta K, Dibaba Y, Woldeyohannes D. Determinants of maternal health care
utilization in Holeta town, central Ethiopia. BMC Health Serv Res. 2013;13(256):10.6. Ronsmans C, Graham W. Maternal mortality: who, when, where, and why.
Lancet. 2006;368(9542):1189–200.7. Tey N, Lai S. Correlates of and barriers to the utilization of health Services
for Delivery in South Asia and sub-Saharan Africa. ScientificWorldJournal.2013;2013
8. Godefay H, Byass P, Kinsman J, Mulugeta A. Understanding maternalmortality from top-down and bottom-up perspectives: case of Tigrayregion, Ethiopia. J Glob Health. 2015;5(1)
9. FMOH. HSTP Health Sector Transformation Plan. 2015.10. Villar J, P B. WHO antenatal care randomized trial: Manual for the
implementation for the new model. 2002.11. WHO. WHO recommendations on antenatal care for a positive pregnancy
experience. 2016.12. CSA. Ethiopia Demographic and Health Survey 2011 Demographic
surveillance Addis Ababa, Ethiopia and Calverton,Maryland. USA: CSA; 2011.13. CSA. Ethiopian Demographci and Health Survey 2016.14. CSA. Ethiopia Demographic and Health Survey. 2005.15. Ayele D, Belayihun B, Teji K, Ayana D. Factors affecting utilization of
maternal health Care Services in Kombolcha District, eastern Hararghe zone,Oromia regional state, eastern Ethiopia. Int Sch Res Notices. 2014;2014:7.
16. Abosse Z, Woldie M, Ololo S. Factors influencing antenatal care serviceutilization in Hadiya zone. Ethiop J Health Sci. 2010;20(2):75–82.
17. Dutamo Z, Assefa N, Egata G. Maternal health care use among marriedwomen in Hossaina, Ethiopia. BMC Health Serv Res. 2015;15(365):1–9.
18. CSA. Population Projection of Ethiopia for All Regions At Wereda Level from2014–2017. 2014.
19. Melaku Y, Weldearegawi B, Tesfay F, Abera S, Abraham L, Aregay A, et al.Poor linkages in maternal health care services? Evidence on antenatal careand institutional delivery from a community-based longitudinal study inTigray region, Ethiopia. BMC Pregnancy and Childbirth. 2014;14(418)
20. CSA. The Ethiopian mini health and demographic survey. Addis Ababa,Ethiopia, Calverton, Maryland, USA: Central statistical agency of Ethiopia; 2014.
21. Wang W, Alva S, Wang S, Fort A. Level and trends in the use of maternalhealth services in developing countries: DHS comparative reports 26: USAID.2011.
22. Cantwell R, Clutton-Brock T, Cooper G. Saving mothers’ lives: reviewingmaternal deaths to make motherhood safer: 2006-2008. The eighth reportof the confidential enquiries into maternal deaths in the United Kingdom.BJOG. 2011;118(1):149-57.
23. Ziyo F, Matly F, Mehemd G, Dofany E. Relation between prenatal care andpregnancy outcome at Benghazi. Sudanese Journal of public health. 2012;4(4):403–10.
24. Thaddeus S, Maine D. Too far to walk: maternal mortality in context. Soc SciMed. 1994;38(8):1091–110.
25. Berhane Y, Gossaye Y, Emmelinb M, Hogberg U. Women’s health in a ruralsetting in societal transition in Ethiopia. Soc Sci Med. 2001;2001(53):1525–39.
Tesfaye et al. Reproductive Health (2017) 14:150 Page 16 of 17

26. Mekonnen Y, Mekonnen A. Utilization of maternal health Care Services inEthiopia. Calverton: Maryland, USA; 2002.
27. Abosse Z, Woldie M, Ololo S. Factors influencing antenatal care serviceutilization in hadiya zone. Ethiop J Health Sci. 2010;20(2):75–82.
28. Damme T, Workineh D, Gmariam A. Time of Antenatal Care Booking andAssociated Factors Among Pregnant Women Attending Ambo Town HealthFacilities, Central Ethiopia. 2015.
29. Ewnetu W, Assegid S, Wondafrash W, Ewnetu H. Factors associated with lateantenatal care initiation in an Ethiopian clinic. Research. 2015.
30. Gudayu T, Woldeyohannes S, Abdo A. Timing and factors associated withfirst antenatal care booking among pregnant mothers in Gondar town;north West Ethiopia. BMC Pregnancy Childbirth. 2014;14(1):287.
31. Lerebo W, Kidanu A, Tsadik M. Magnitude and associated factors of latebooking for antenatal Care in Public Health Centers of Adigrat town, Tigray.Ethiopia Clinics Mother Child Health. 2015;12(171):2.
32. Tekelab T, Berhanu B. Factors associated with late initiation of antenatal careamong pregnant women attending antenatal Clinic at Public HealthCenters in Kembata Tembaro zone, southern Ethiopia. Science, Technologyand Arts Research Journal. 2014;3(1):108–15.
33. Yilala Y. Assesment of late initiation of antenatal care and associated factorsamong antenatal care attendees in selected health centers of Addis Ababa,Ethiopia (Master Thesis): AAU; 2015.
34. Belayneh T, Adefris M, Andargie G. Previous Early Antenatal ServiceUtilization Improves Timely Booking: Cross-Sectional Study at University ofGondar Hospital, Northwest Ethiopia. 2014.
35. Abuka T, Alemu A, Birhanu B. Assessment Of Timing Of First Antenatal CareBooking And Associated Factors Among Pregnant Women Who AttendAntenatal Care At Health Facilities In Dilla Town, Gedeo Zone, SouthernNations, Nationalities, And Peoples Region, Ethiopia, 2014: AAU; 2014.
36. Bayou Y, Mashalla Y, Tshweneagae G. The adequacy of antenatal careservices among slum residents in Addis Ababa, Ethiopia. BMC PregnancyChildbirth. 2016;16(1):142.
37. Gudayu T. Proportion and factors associated with late antenatal carebooking among pregnant mothers in Gondar town, north West Ethiopia.Afr J Reprod Health. 2015;19(2):93–9.
38. Girum T. Assessment of timing of first antenatal care visit and associatedfactors among pregnant women attending antenatal Care in Dilla TownGovernmental Health Institutions, southern Ethiopia. Alternative &Integrative Medicine. 2016;5(3)
39. Amentie M, Abera M, Abdulahi M. Utilization of antenatal care services andinfluencing factors among women of child bearing age in Assosa District,Benishangul Gumuz regional state, West Ethiopia. Global Journal of MedicalResearch. 2015;15(2)
40. Gebremeskel F, Dibaba Y, Admassu B. Timing of first antenatal careattendance and associated factors among pregnant women in Arba Minchtown and Arba Minch District, Gamo Gofa Zone, South Ethiopia. 2015.
41. Haileselassie D. Magnitude and factors affecting late initiation of antenatalcare service utilization among pregnant women in government healthinstitutions, Mekelle Town, Ethiopia (Master Thesis): AAU; 2010.
42. Hussen S, Melese E, Dembelu M. Timely Initiation of First Antenatal CareVisit of Pregnant Women Attending Antenatal Care Service. 2016.
43. Simkhada B, Teijlingen E, Porter M, Simkhada P. Factors affecting theutilization of antenatal care in developing countries: systematic review ofthe literature. J Adv Nurs. 2007;61(3):244–60.
44. Hajizadeh S, Tehrani F, Simbar M, Farzadfar F. Factors influencing the use ofprenatal care: a systematic review. J midwifery. Reprod Health. 2016;4(1):544–57.
45. Boerleider A, Wiegers T, Manniën J, Francke A, Devillé W. Factors affectingthe use of prenatal care by non-western women in industrialized westerncountries: a systematic review. BMC Pregnancy Childbirth. 2013;13(81)
46. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al.Preferred reporting items for systematic review and meta-analysis protocols(PRISMA-P) 2015 statement. Systematic Reviews. 2015;4(1)
47. Moher D, Liberati A, Tetzlaff J, Altman D. Preferred reporting items for systematicreviews and meta-analyses: the PRISMA statement. PLoS Med. 2009;6(7)
48. Reuters T, inventorEndNote X 7.3.1 (BId 8614), Cite While You Write TMPatented technology U.S patent number 8,092,24119888–2015.
49. Institute TJB. Joanna Briggs institute Reviewers' manual 2014 edition.Adelaide: Adelaide University; 2014.
50. Cochrane C, inventorReview Manager (RevMan) [Computer program].Version 5.3. Copenhagen: The Nordic Cochrane Centre, The CochraneCollaboration 2014.
51. Higgins J, Hompson S. Quantifying heterogeneity in a meta-analysis. 2002.52. StatsDirect Ltd. StatsDirect statistical software. England: StatsDirect Ltd.;
2013. http://www.statsdirect.com.53. FMOH. Antenatal Care Module: 13. In: Providing focused antenatal care; 2010.54. Beller E, Glasziou P, Altman D, Hopewell S, Bastian H, Chalmers I, et al.
PRISMA for abstracts: reporting systematic reviews in journal andconference abstracts. PLoS Med. 2013;10(4)
55. Vintzileos A, Ananth C, Smulian J, Scorza W, Knuppel R. The impact of prenatalcare on neonatal deaths in the presence and absence of antenatal high-riskconditions. Am J Obstet Gynecol. 2002;186(5):1011–6.
56. Moat K, Lavis J, Wilson M, Røttingen J, Barnighausen T. Twelve myths aboutsystematic reviews for health system policymaking rebutted. J Health ServRes Policy. 2013;18(1):44–50.
57. USAID/MCHIP. Cultural Barriers to Seeking Maternal Health Care in Ethiopia:A Review of the Literature. 2012.
58. Warren C. Care seeking for maternal health: challenges remain for poorwomen. Ethiopian Journal of Health Development. 2010;24(Special 1):100–4.
59. Jong E, Jansen D, Baarveld F, Schans C, Schellevis F, Reijneveld S.Determinants of late and/or inadequate use of prenatal healthcare in high-income countries: a systematic review. Eur J Pub Health. 2011;22(6):904–13.
60. Yang Y, Yoshitoku Y, Harun R, Junichi S. Factors Affecting the utilization ofantenatal care services among women in Kham district, Xiengkhouangprovince, Lao PDR. Nagoya J Med Sci. 2010;72:23–33.
61. Anyait A, Mukanga D, Oundo G, Nuwaha F. Predictors for health facilitydelivery in Busia district of Uganda: a cross sectional study. BMC PregnancyChildbirth. 2012;12(132)
62. Ayebare E, Mwebaza E, Mwizerwa J, Namutebi E, Kinengyere A, Smyth R.Interventions for male involvement in pregnancy and labour: a systematicreview. 2006.
63. Dibaba Y, Fantahun M, Hindin M. The effects of pregnancy intention on theuse of antenatal care services: systematic review and meta-analysis. ReprodHealth. 2014;10(50)
64. Dizon J, Machingaidze S, Grimmer K. To adopt, to adapt, or tocontextualise? The big question in clinical practice guideline development.BMC Res Notes. 2016;9(442)
65. Zegeye A, Bitew B, Koye D. Prevalence and determinants of early antenatalcare visit among pregnant women attending antenatal Care in Debre BerhanHealth Institutions, Central Ethiopia. Afr J Reprod Health. 2013;17(4):130–6.
66. Fisseha G, Miruts G, Tekie M, W/Michael A, Yemane D, Gerezigiher T.Predictors of timing of first antenatal care booking at public health centersin Mekelle City, northern Ethiopia. J Gynecol Obst. 2015;3(3):55–60.
67. Gulema H, Berhane Y. Timing of first antenatal care visit and its associatedfactors among pregnant women attending public health facilities in AddisAbaba, Ethiopia. Ethiopian Journal of Health Sciences. 2017;27(2):139–46.
68. Mohammed Z, Berhane E. Assessment of timing of first antenatal care (ANC)initiation and associated factors among pregnant women in selected publichealth centres in Addis Ababa, Ethiopia, 2014: AAU; 2014.
• We accept pre-submission inquiries
• Our selector tool helps you to find the most relevant journal
• We provide round the clock customer support
• Convenient online submission
• Thorough peer review
• Inclusion in PubMed and all major indexing services
• Maximum visibility for your research
Submit your manuscript atwww.biomedcentral.com/submit
Submit your next manuscript to BioMed Central and we will help you at every step:
Tesfaye et al. Reproductive Health (2017) 14:150 Page 17 of 17




![Early Initiation of Antenatal Care and Factors Associated ...downloads.hindawi.com/journals/aph/2017/1624245.pdf · 6 AdvancesinPublicHealth [21].Andotherslikeeducationallevelofmothersandtheir](https://img.dokumen.tips/doc/110x75/5cd8c8d688c9938f428c4efd/early-initiation-of-antenatal-care-and-factors-associated-6-advancesinpublichealth.jpg)