Embed Size (px)
Citation preview
1286
just pedantic to comment that their plan, if correct,shows that such a reversal of flow is anatomically possible,but a plan does not, and cannot, show that it ever occurs infact. Our experimental evidence strongly suggests thatincreased centripetal flow occurs not through reversal offlow in centrifugal vessels but through increased flow inexisting centripetal vessels.
A. MCPHERSONN. E. SHAW.
Clinical Research Wing,Institute of Orthopaedics,
Stanmore, Middlesex.
1. Penrose, L. S., Delhanty, J. D. A. Lancet, June 10, 1961, p. 1261.2. Penrose, L. S., Ellis, J. R., Delhanty, J. D. A. ibid. 1960, ii, 409.3. Carter, C. O., Hamerton, J. L., Polani, P. E., Gunalp, A., Weller, S. D. V.
ibid. p. 678.4. Buckton, K. E., Harnden, D. G., Baikie, A. G., Woods, G. E. ibid.
Jan. 21, 1961, p. 171.
TRIPLOID CELLS IN A HUMAN EMBRYO
JOY D. A. DELHANTYJ. R. ELLISP. T. ROWLEY.
Galton Laboratory,University College London,
W.C.1.
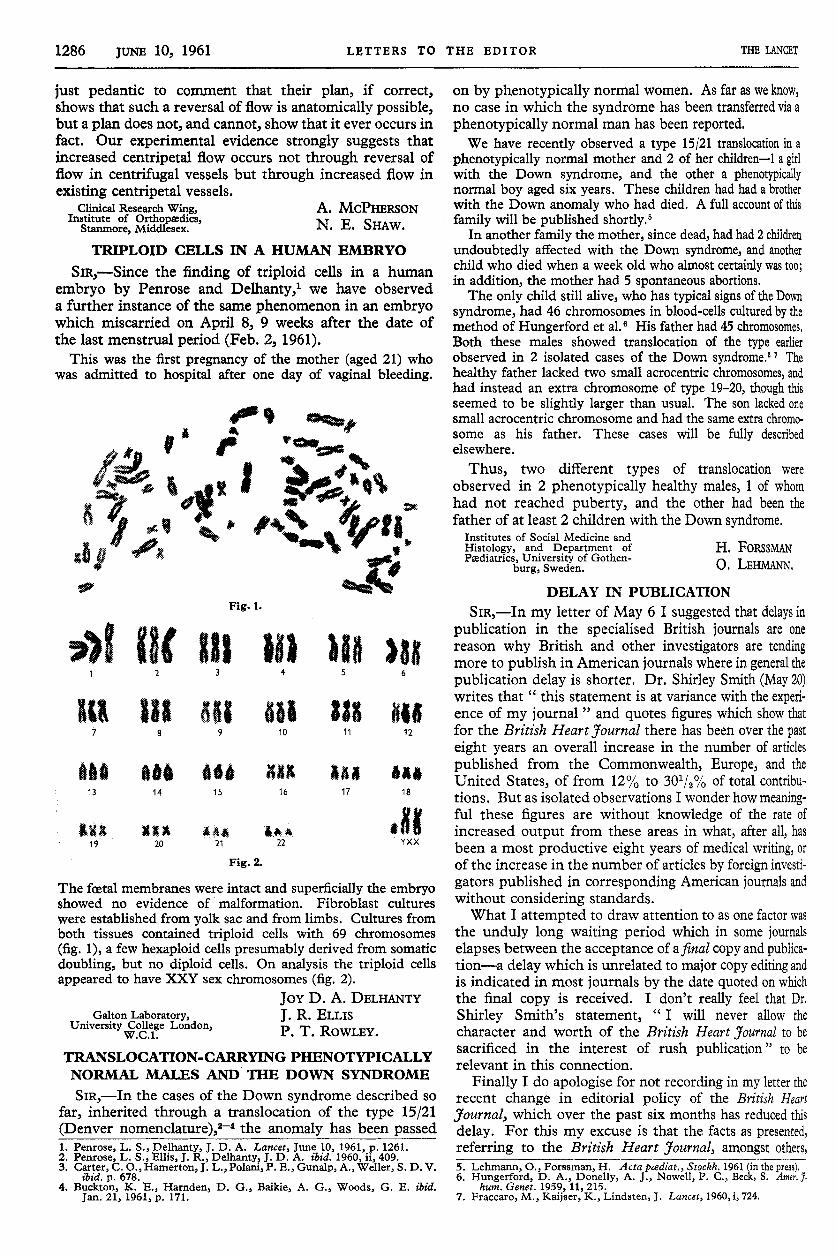
SiR,-Since the finding of triploid cells in a human
embryo by Penrose and Delhanty,l we have observeda further instance of the same phenomenon in an embryowhich miscarried on April 8, 9 weeks after the date ofthe last menstrual period (Feb. 2, 1961).
This was the first pregnancy of the mother (aged 21) whowas admitted to hospital after one day of vaginal bleeding.
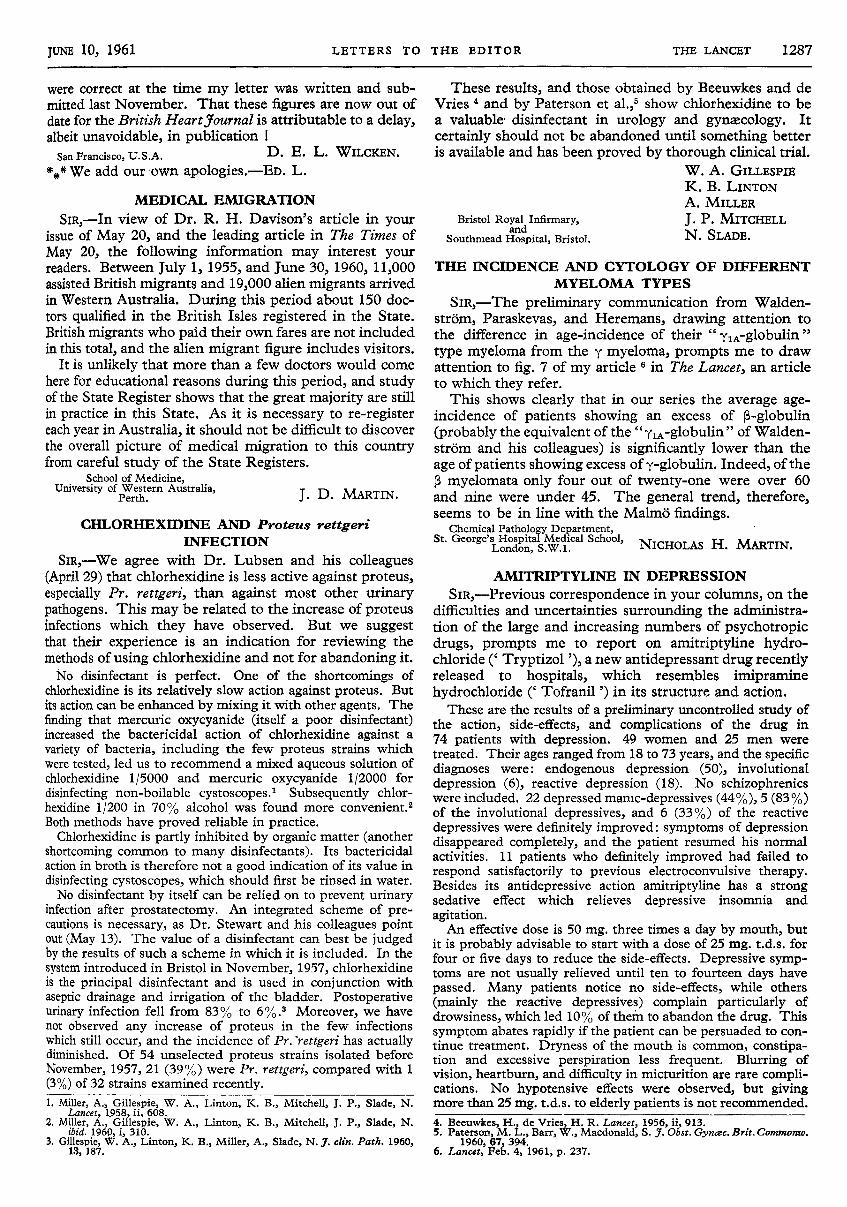
The foetal membranes were intact and superficially the embryoshowed no evidence of malformation. Fibroblast cultureswere established from yolk sac and from limbs. Cultures fromboth tissues contained triploid cells with 69 chromosomes
(fig. 1), a few hexaploid cells presumably derived from somaticdoubling, but no diploid cells. On analysis the triploid cellsappeared to have XXY sex chromosomes (fig. 2).
TRANSLOCATION-CARRYING PHENOTYPICALLYNORMAL MALES AND THE DOWN SYNDROME
H. FORSSMANO. LEHMANN.
Institutes of Social Medicine andHistology, and Department ofPædiatrics, University of Gothen-
burg, Sweden.
SIR,-In the cases of the Down syndrome described sofar, inherited through a translocation of the type 15/21(Denver nomenc1ature),2-4 the anomaly has been passed
on by phenotypically normal women. As far as we know,no case in which the syndrome has been transferred via aphenotypically normal man has been reported.We have recently observed a type 15/21 translocation in a
phenotypically normal mother and 2 of her children-1 a girlwith the Down syndrome, and the other a phenotypicallynormal boy aged six years. These children had had a brotherwith the Down anomaly who had died. A full account of thisfamily will be published shortly.5
In another family the mother, since dead, had had 2 childrenundoubtedly affected with the Down syndrome, and anotherchild who died when a week old who almost certainly was too;in addition, the mother had 5 spontaneous abortions.The only child still alive, who has typical signs of the Down
syndrome, had 46 chromosomes in blood-cells cultured by themethod of Hungerford et al. His father had 45 chromosomes.Both these males showed translocation of the type earlierobserved in 2 isolated cases of the Down syndrome,.2 Thehealthy father lacked two small acrocentric chromosomes, andhad instead an extra chromosome of type 19-20, though thisseemed to be slightly larger than usual. The son lacked onesmall acrocentric chromosome and had the same extra chromo-some as his father. These cases will be fully describedelsewhere.
Thus, two different types of translocation were
observed in 2 phenotypically healthy males, 1 of whomhad not reached puberty, and the other had been thefather of at least 2 children with the Down syndrome.
5. Lehmann, O., Forssman, H. Acta pœdiat., Stockh. 1961 (in the press).6. Hungerford, D. A., Donelly, A. J., Nowell, P. C., Beck, S. Amer. J.
hum. Genet. 1959, 11, 215.7. Fraccaro, M., Kaijser, K., Lindsten, J. Lancet, 1960, i, 724.
DELAY IN PUBLICATION
SIR,-In my letter of May 6 I suggested that delays inpublication in the specialised British journals are one
reason why British and other investigators are tendingmore to publish in American journals where in general thepublication delay is shorter. Dr. Shirley Smith (May 20)writes that " this statement is at variance with the experi-ence of my journal " and quotes figures which show thatfor the British Heart Journal there has been over the pasteight years an overall increase in the number of articlespublished from the Commonwealth, Europe, and theUnited States, of from 12% to 301/2% of total contribu-tions. But as isolated observations I wonder how meaning-ful these figures are without knowledge of the rate ofincreased output from these areas in what, after all, hasbeen a most productive eight years of medical writing, orof the increase in the number of articles by foreign investi-gators published in corresponding American journals andwithout considering standards.What I attempted to draw attention to as one factor was
the unduly long waiting period which in some journalselapses between the acceptance of a final copy and publica-tion-a delay which is unrelated to major copy editing andis indicated in most journals by the date quoted on whichthe final copy is received. I don’t really feel that Dr,Shirley Smith’s statement,
" I will never allow thecharacter and worth of the British Heart Journal to besacrificed in the interest of rush publication " to berelevant in this connection.
Finally I do apologise for not recording in my letter therecent change in editorial policy of the British Heart
yoMfMd7, which over the past six months has reduced thisdelay. For this my excuse is that the facts as presented,referring to the British Heart Journal, amongst others,
1287
were correct at the time my letter was written and sub-mitted last November. That these figures are now out ofdate for the British Heartyournal is attributable to a delay,albeit unavoidable, in publication !San Francisco, U.S.A. D. E. L. WILCKEN.
*** We add our own apologies.-ED. L.D. E. L. WILCKEN.
1. Miller, A., Gillespie, W. A., Linton, K. B., Mitchell, J. P., Slade, N.Lancet, 1958, ii, 608.
2. Miller, A., Gillespie, W. A., Linton, K. B., Mitchell, J. P., Slade, N.ibid. 1960, i, 310.
3. Gillespie, W. A., Linton, K. B., Miller, A., Slade, N. J. clin. Path. 1960,13, 187.
MEDICAL EMIGRATION
J. D. MARTIN.School of Medicine,
University of Western Australia,Perth.
SIR,-In view of Dr. R. H. Davison’s article in yourissue of May 20, and the leading article in The Times ofMay 20, the following information may interest yourreaders. Between July 1, 1955, and June 30, 1960, 11,000assisted British migrants and 19,000 alien migrants arrivedin Western Australia. During this period about 150 doc-tors qualified in the British Isles registered in the State.British migrants who paid their own fares are not includedin this total, and the alien migrant figure includes visitors.
It is unlikely that more than a few doctors would comehere for educational reasons during this period, and studyof the State Register shows that the great majority are stillin practice in this State. As it is necessary to re-registereach year in Australia, it should not be difficult to discoverthe overall picture of medical migration to this countryfrom careful studv of the State Registers.
CHLORHEXIDINE AND Proteus rettgeriINFECTION
W. A. GILLESPIEK. B. LINTONA. MILLER
J. P. MITCHELLN. SLADE.
Bristol Royal Infirmary,and
Southmead Hospital, Bristol.
SIR,-We agree with Dr. Lubsen and his colleagues(April 29) that chlorhexidine is less active against proteus,especially Pr. rettgeri, than against most other urinarypathogens. This may be related to the increase of proteusinfections which they have observed. But we suggestthat their experience is an indication for reviewing themethods of using chlorhexidine and not for abandoning it.No disinfectant is perfect. One of the shortcomings of
chlorhexidine is its relatively slow action against proteus. Butits action can be enhanced by mixing it with other agents. Thefinding that mercuric oxycyanide (itself a poor disinfectant)increased the bactericidal action of chlorhexidine against avariety of bacteria, including the few proteus strains whichwere tested, led us to recommend a mixed aqueous solution ofchlorhexidine 1/5000 and mercuric oxycyanide 1/2000 for
disinfecting non-boilable cystoscopes.1 Subsequently chlor-hexidine 1/200 in 70% alcohol was found more convenient.2Both methods have proved reliable in practice.Chlorhexidine is partly inhibited by organic matter (another
shortcoming common to many disinfectants). Its bactericidalaction in broth is therefore not a good indication of its value indisinfecting cystoscopes, which should first be rinsed in water.No disinfectant by itself can be relied on to prevent urinary
infection after prostatectomy. An integrated scheme of pre-cautions is necessary, as Dr. Stewart and his colleagues pointout (May 13). The value of a disinfectant can best be judgedby the results of such a scheme in which it is included. In the
system introduced in Bristol in November, 1957, chlorhexidineis the principal disinfectant and is used in conjunction withaseptic drainage and irrigation of the bladder. Postoperativeurinary infection fell from 83% to 6%.3 Moreover, we havenot observed any increase of proteus in the few infectionswhich still occur, and the incidence of Pr.rettgeri has actuallydiminished. Of 54 unselected proteus strains isolated beforeNovember, 1957, 21 (39%) were Pr. rettgeri, compared with 1(3%) of 32 strains examined recently.
These results, and those obtained by Beeuwkes and deVries 4 and by Paterson et a1.,5 show chlorhexidine to bea valuable disinfectant in urology and gynaecology. It
certainly should not be abandoned until something betteris available and has been proved by thorough clinical trial.
4. Beeuwkes, H., de Vries, H. R. Lancet, 1956, ii, 913.5. Paterson, M. L., Barr, W., Macdonald, S. J. Obst. Gynœc. Brit. Commonw.
1960, 67, 394.6. Lancet, Feb. 4, 1961, p. 237.
THE INCIDENCE AND CYTOLOGY OF DIFFERENTMYELOMA TYPES
NICHOLAS H. MARTIN.Chemical Pathology Department,
St. George’s Hospital Medical School,London, S.W.1.
SiR,—The preliminary communication from Walden-strom, Paraskevas, and Heremans, drawing attention tothe difference in age-incidence of their " ylA-globulin "type myeloma from the y myeloma, prompts me to drawattention to fig. 7 of my article 6 in The Lancet, an articleto which they refer.
This shows clearly that in our series the average age-incidence of patients showing an excess of P-globulin(probably the equivalent of the " YiA’glooulin " of Walden-strom and his colleagues) is significantly lower than theage of patients showing excess of y-globulin. Indeed, of theP myelomata only four out of twenty-one were over 60and nine were under 45. The general trend, therefore,seems to be in line with the Malmö findings.
AMITRIPTYLINE IN DEPRESSION
SIR,-Previous correspondence in your columns, on thedifficulties and uncertainties surrounding the administra-tion of the large and increasing numbers of psychotropicdrugs, prompts me to report on amitriptyline hydro-chloride (’ Tryptizol ’), a new antidepressant drug recentlyreleased to hospitals, which resembles imipraminehydrochloride (’ Tofranil ’) in its structure and action.These are the results of a preliminary uncontrolled study of
the action, side-effects, and complications of the drug in74 patients with depression. 49 women and 25 men weretreated. Their ages ranged from 18 to 73 years, and the specificdiagnoses were: endogenous depression (50), involutional
depression (6), reactive depression (18). No schizophrenicswere included. 22 depressed manic-depressives (44%), 5 (83%)of the involutional depressives, and 6 (33%) of the reactivedepressives were definitely improved: symptoms of depressiondisappeared completely, and the patient resumed his normalactivities. 11 patients who definitely improved had failed torespond satisfactorily to previous electroconvulsive therapy.Besides its antidepressive action amitriptyline has a strongsedative effect which relieves depressive insomnia and
agitation.An effective dose is 50 mg. three times a day by mouth, but
it is probably advisable to start with a dose of 25 mg. t.d.s. forfour or five days to reduce the side-effects. Depressive symp-toms are not usually relieved until ten to fourteen days havepassed. Many patients notice no side-effects, while others(mainly the reactive depressives) complain particularly ofdrowsiness, which led 10% of them to abandon the drug. Thissymptom abates rapidly if the patient can be persuaded to con-tinue treatment. Dryness of the mouth is common, constipa-tion and excessive perspiration less frequent. Blurring ofvision, heartburn, and difficulty in micturition are rare compli-cations. No hypotensive effects were observed, but givingmore than 25 mg. t.d.s. to elderly patients is not recommended.





























