Embed Size (px)
Citation preview
DEFINING EMOTIONAL AND BEHAVIORAL DISORDERS
Even though no definition of emotional behavioral disorders proposed so far has provided a consistent, universally agreed-on standard for identification, diagnosis, communication, and research, they all agree that a child's behavior, to be considered disordered, must meet three criteria:
severity the child’s behavior must differ markedly from current social or cultural norms
difficulty in school the child’s behavior problem(s) adversely affects educational performance
chronicity the child’s behavior problem(s) has existed over a long periodof time or been unresponsive to direct intervention in general education
T 8.1W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved.
CHARACTERISTICS OF CHILDREN WITHEMOTIONAL AND BEHAVIORAL DISORDERS
Externalizing Behaviors The most common pattern of behavior by children with emotional and behavior disorders consists of antisocial, or externalizing behaviors.
Antisocial behavior and aggression often occur with little or no provocation and take many forms—noncompliance, verbal abuse toward adults and other children, destructiveness and vandalism, physical attackson others.
A pattern of antisocial behavior early in a child's school career is the best single predictor of delinquency in adolescence.
Many believe that most children who exhibit deviant behavior patterns will grow out of them with time and become normally functioning adults. Research indicates that it is not so for children who display consistent patterns of aggressive, coercive, antisocial, and/or delinquent behavior.
Internalizing Behaviors Some children engage in too little social interaction with others; they are said to have internalizing behavior disorders.
Although children who consistently act immature and withdrawn do not present a threat to others, their behavior creates a serious impediment to their development.
These children seldom play with others their own age, they usually do not have the necessary social skills to make friends and have fun, and they often retreat into daydreams and fantasies.
Some are fearful of things without reason, frequently complain of being sick or hurt, and go into deep bouts of depression. Because children who manifest internalizing behaviors may be less disturbing to others, there is the danger of their not
being identified.
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.2
CHARACTERISTICS OF CHILDREN WITHEMOTIONAL AND BEHAVIORAL DISORDERS (con’t)
School Achievement and Intelligence The disruptive and defiant behavior of students with emotional and behavior disorders almost always leads to academic difficulties.
Many more children with emotional and behavior disorders score in the slow learner or mildly retarded rangeon IQ tests than do normal children.
Even when IQ scores are taken into account, children with emotional and behavior disorders achieve below the levelssuggested by their scores.
It is estimated that only 30% of students with behavior disorders are performing at or above grade level (Knister et al., 1990).
Two nationwide studies reported the following academic outcomes for students with emotional and behavioral disorders:
two thirds could not pass competency exams for their grade level
they had the lowest grade-point average of any group of students with disabilities
they had the highest absenteeism rate of any group of students
48% drop out of high school, compared with 30% of all students with disabilities
Social Skills and Interpersonal Relationships Many students with emotional and behavioral disorders experience great difficulty in making and keeping friends.
Compared to their same-age peers without behavioral disorders, adolescents with behavior disorders report lower levels of empathy toward others, participation in fewer curricular activities, less frequent contacts with friends, and lower-quality relationships.
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.3
CAUSES OF EMOTIONAL AND BEHAVIORAL DISORDERS
Biological Factors For the vast majority of children with emotional and behavior disorders, there is no evidence of organic injury or disease.
Some experts believe that all children are born with a biologically determined temperament. Although a child's inborn temperament may not in itself cause a behavior problem, it may predispose the child to problems.
Even when a clear biological impairment exists, however, no one has been able to say with certainty whether the physiological abnormality actually causes the behavior problem or is just associated with it insome unknown way.
Environmental Factors Events in the child's life that affect the way she acts.
Considered important in the development of emotional and behavior disorders in all conceptual models. What events are important and how they are analyzed, however, are viewed differently by professionals
with different approaches. Dodge (1993) has identified three primary causal factors that contribute to the development of conduct
disorder and antisocial behavior: (1) an adverse early rearing environment, (2) an aggressive pattern of behavior displayed upon entering school, and (3) social rejection by peers.
Considerable research evidence supports Dodge's contention that these causal factors operate in temporal sequence.
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.4
CAUSES OF EMOTIONAL AND BEHAVIORAL DISORDERS (con’t)
Influence of Home The relationship children have with their parents, particularly during the early years, is critical to the way they learn to act.
Parents who treat their children with love, are sensitive to their children's needs, and provide praise and attention for desired behaviors tend to have normal children with positive behavioral characteristics.
Antisocial children often come from homes in which parents are inconsistent disciplinarians, use harsh and excessive punishment, spend little time engaged in prosocial activities with their children, do not monitor the whereabouts and activities of their children, and show little love and affection for good behavior.
The relationship between parent and child is dynamic and reciprocal: the behavior of the child affects the behavior of the parents just as much as the parents' actions affect the child's actions.
Influence of the Community When students associate with peers who exhibit antisocial behavior, they are more likely to experience additional trouble in the community and at school.
Influence of School Because most children with emotional and behavior disorders are not identified until they are in school, it is reasonable to question whether the school actually contributes to the incidence of behavior disorders.
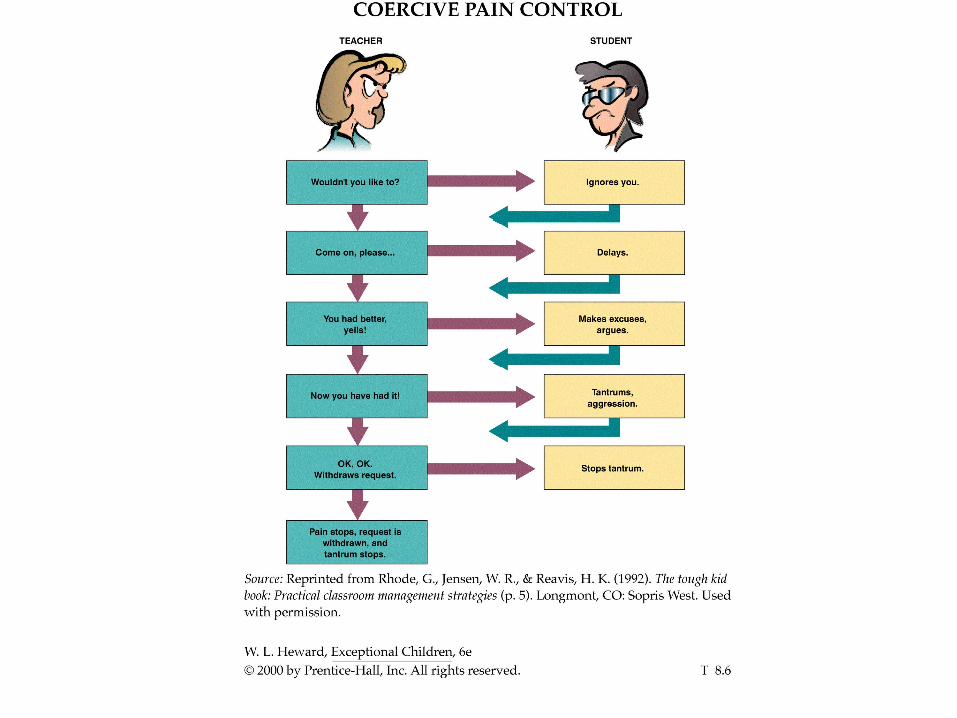
Several studies have demonstrated that what takes place in the classroom can maintain and actually strengthen deviant behavior patterns, even though the teacher is trying to help the child (e.g., coercive pain control shown by Transparency 8.6).
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.5
IDENTIFICATION AND ASSESSMENT
Screening Tests Most screening devices for emotional and behavioral disorders consist of behavior rating scales or checklists that are completed by teachers, parents, peers, and/or children themselves. Children identified via a screening process then undergo more thorough assessment to determine their eligibility for special education and their specific educational needs.
Examples: Behavior Rating Profile (BRP-2), Child Behavior Checklist (CBCL), Systematic Screening forBehavioral Disorders (SSBD)
Projective Tests A project test consists of ambiguous stimuli (e.g., "What does this inkblot look like to you?") or open-ended tasks (e.g., "Complete this sentence for me: 'Most girls ... '"). It is assumed that responses to items that have no right or wrong answer will reveal a person's true personality characteristics.
Examples: Rorschach Test, Thematic Apperception Test, Draw a Person: Screening Procedure for Emotional Disturbance
The results of projective tests have proven to be of minimal value in prescribing appropriate intervention,
because (1) children often do not respond in a testing or interview situation in the same way they do in the
classroom or at home, (2) the tests sample an indirect and extremely limited sample of a child's behavioral
repertoire, and (3) the tests do not assess how the child typically acts over a period of time.W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.7
IDENTIFICATION AND ASSESSMENT (con’t.)
Direct Observation and Measurement of Behavior the actual behaviors that cause concern about a child are clearly specified and observed in the settings where they normally occur (e.g., in the classroom, on the playground).
behavior can be measured objectively along several dimensions: rate (or frequency), duration, latency, topography, and magnitude
leads to a direct focus on the child's problem—the inappropriate behavior—and ways of dealing with it, as
opposed to concentrating on some presumed (and unreachable) problem within the child
Functional Assessment purpose is to obtain information about when, where, and why problem behaviors occur as well as when, where, and why they do not occur
involves interviews with significant others and direct observation to determine the environmental events that typically occur before and after the behavior(s) of concern
may also involve experimental manipulation of one or more antecedent or consequent events surroundingthe target behavior in an attempt to verify the function of the behavior for the child
this information can then be used to improve the effectiveness and efficiency of behavioral intervention
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.8
FIVE MEASURABLE DIMENSIONS OF BEHAVIOR
Rate (or frequency) how often a particular behavior is performed. The frequency, or rate, of behavior may be too high (e.g., crying, hitting others) or too low (e.g., playing with others).
Duration how long a child engages in a given activity. Behaviors can be maladaptive because the duration is too long (e.g., a tantrum of an hour or more) or too short (e.g., paying attention or working independently for no more than several seconds at a time).
Topography the physical shape or form of behavior. Many behaviors must be performed with precise topography in order to be functional (e.g., speech, handwriting, self-care). The topography of other behaviors may be maladaptive, bizarre, or dangerous to the child or others (e.g., twirling a small object close to one’s eyes).
Latency the time that elapses between the opportunity to respond and the beginning of the behavior. The latency of a child's behavior may be too long (e.g., several minutes elapse before beginning to comply with the teacher's request) or too short (e.g., at the slightest provocation or frustration the child immediately begins screaming and tantruming, thus having no time to consider more appropriate alternative behaviors).
Magnitude The strength or intensity of behavior. The magnitude of a child's responses may be too little (e.g., talking in a volume so low that you cannot be heard) or too much (e.g., slamming the door).
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.9
SELF-MANAGEMENT
Many children with emotional and behavior disorders think they have little control over their lives. Things just seem to happen to them, and being disruptive is their means of reacting to a world that is inconsistent and frustrating.
Numerous studies have demonstrated that students with behavior problems can effectively use various self-management strategies to help regulate their behavior.
Self-monitoring is a relatively simple procedure in which the student observes and records the occurrence (and sometimes the nonoccurrence) of his or her own behavior.
Self-evaluation involves comparing one's behavior against a standard or goal.
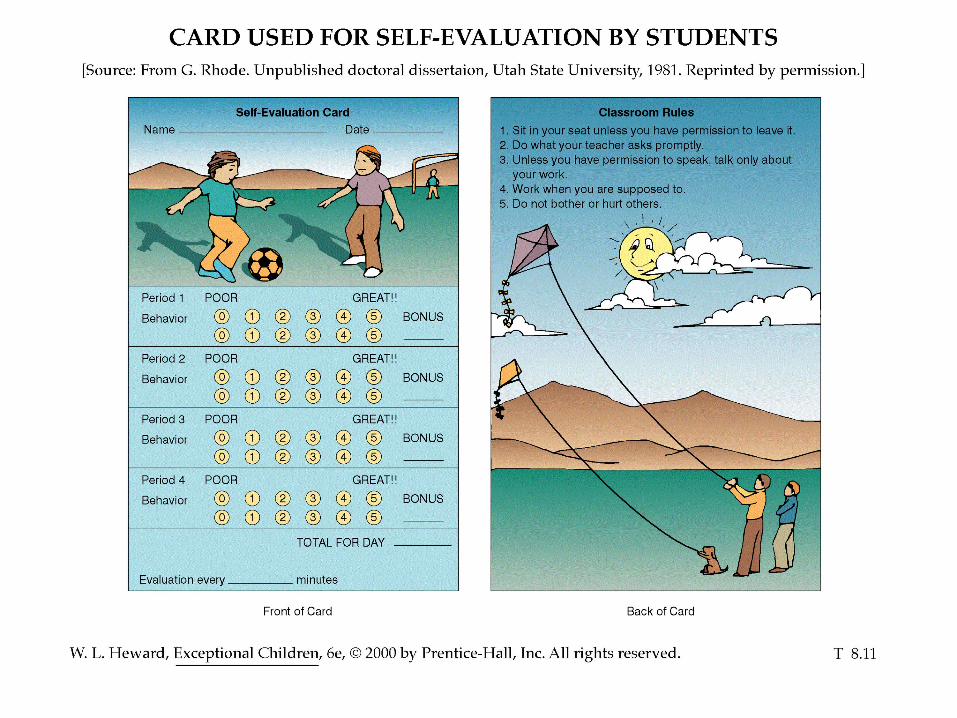
Example: Rhode, Morgan, and Young (1983) helped six students with emotional and behavioral disorders learn to bring their highly disruptive and off-task behaviors under control in a resource room with a combination of techniques that featured self-monitoring and self-evaluation. Initially, the teacher rated each student and awarded points at 15-minute intervals on a scale from 5 (great) to 0 (poor) for classroom behavior and academic work. Then the students began to evaluate their own behavior with the same rating system and were rewarded when their self-ratings were within one point of the teacher's rating (see Transparency 8.11).
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.10
TWO IMPORTANT AFFECTIVE SKILLS FOR TEACHERS OFSTUDENTS WITH EMOTIONAL AND BEHAVIORAL DISORDERS
differential acceptance being able to receive and witness frequent and often extreme acts of anger, hate, and aggression from children without responding similarly
the teacher must view disruptive behavior for what it isbehavior that reflects thestudent's past frustrations and conflict with himself and those around himand tryto help the child learn better ways of behaving
should not be confused with approving or condoning antisocial behavior; the child
must learn that he is responding inappropriately calls for understanding without condemning
empathetic relationship the ability to recognize and understand the many nonverbal cues that often are the keys to understanding the individual needs of emotionally disturbed children
W. L. Heward, Exceptional Children, 6e, 2000 by Prentice-Hall, Inc. All rights reserved. T 8.12