Embed Size (px)
Citation preview
Decreased Intravesical Adenosine Triphosphate in Patients with
Refractory Detrusor Overactivity and Bacteriuria
Colin A. Walsh, Ying Cheng, Kylie J. Mansfield,* Katrina Parkin, Chinmoy Mukerjeeand Kate H. Moore†
From the Departments of Urogynaecology (CAW, YC, KP, KHM) and Microbiology (CM), St. George Hospital, University of New SouthWales, Sydney, and Graduate School of Medicine, University of Wollongong, Wollongong, New South Wales (KJM), Australia
Purpose: Although several studies have examined the relationship betweenadenosine triphosphate release from the urothelium and bladder sensationsincluding painful filling and urgency, the association between bacteriuria andurothelial adenosine triphosphate release has not been well studied. Weevaluated women with refractory detrusor overactivity who were experiencingan acute exacerbation of detrusor overactivity symptoms including frequency,urgency and nocturia (and/or urge incontinence). We measured changes inintravesical adenosine triphosphate levels in these women with and withoutbacteriuria.Materials and Methods: In this prospective cohort study women with refractorydetrusor overactivity were invited to our unit during acute symptomatic exacer-bation. On presentation a catheter urine specimen was collected and 50 mlnormal saline instilled into the bladder to evoke gentle stretch, with removalafter 5 minutes. Adenosine triphosphate concentrations were determined onfresh washings using a bioluminescence assay.Results: The incidence of bacteriuria 103 cfu/ml or greater was 27% (15 of 56specimens) during the 16-month study period. Adenosine triphosphate concentra-tions were lower during episodes of bacteriuria in the overall cohort (p � 0.0013) andpaired samples from individual patients (p � 0.031) compared to episodes of sterileurine.Conclusions: In the first study on the subject to our knowledge, we demonstrateda striking difference between adenosine triphosphate levels measured in thepresence and absence of bacteriuria in this patient group.
Abbreviations
and Acronyms
ATP � adenosine triphosphate
CSU � catheter specimen ofurine
DO � detrusor overactivity
OAB � overactive bladder
UTI � urinary tract infection
Accepted for publication October 1, 2012.Study received human research and ethics
committee approval.Supported by the Pfizer OAB-LUTS OAB-LUTS
Competitive Grants Program (WS428347) and a2010 International Urogynecological AssociationResearch Grant.
* Correspondence: Graduate School of Medi-cine, University of Wollongong, Wollongong,NSW, 2522, Australia (telephone: �61 2 42215851; FAX: �61 2 4221 4341; e-mail: [email protected]).
† Financial interest and/or other relationshipwith Hospira.
For another article on a related
topic see page 1567.
Key Words: adenosine triphosphate; bacteriuria; urinary bladder, overactive
INVESTIGATION into the mechanisms in-volved in the sensation of urinary ur-gency has revealed the importance ofa bladder purinergic system involvingnonadrenergic, noncholinergic neu-rotransmission.1 In the healthy blad-der, stretch of the bladder wall stim-ulates the release of ATP from theurothelium,2 which interacts with pu-rinergic P2X2/3 receptors located on
the suburothelial afferent nerves, giv-0022-5347/13/1894-1383/0THE JOURNAL OF UROLOGY®
© 2013 by AMERICAN UROLOGICAL ASSOCIATION EDUCATION AND RES
ing rise to a normal sensation of blad-der fullness.3 However, in bladder dis-ease states this mechanism is alteredand enhanced purinergic neurotrans-mission is believed to contribute to anabnormal sensation of urgency.4
To date, most studies on ATP releasein bladder dysfunction have focused onwomen with bladder dysfunction char-acterized by painful filling, for example
patients with interstitial cystitis5–7 andhttp://dx.doi.org/10.1016/j.juro.2012.10.003Vol. 189, 1383-1387, April 2013
EARCH, INC. Printed in U.S.A.www.jurology.com 1383

DECREASED ADENOSINE TRIPHOSPHATE AND BACTERIURIA1384
painful bladder syndrome.8 Purinergic dysfunction indiseases such as detrusor overactivity characterizedby urinary urgency in the absence of pain has beenexamined to a lesser extent.9,10 Despite the fact thatUTI is one of the most common causes of urinaryurgency in women, the relationship between ATP con-centrations and bacteriuria has not been well studied.
The purinergic system is well-known to triggerinflammatory responses via activation of purinergicreceptors located on cells of the innate immune sys-tem.11 In addition, cyclophosphamide induced cysti-tis is associated with hypersensitivity of bladderafferent nerves to ATP in rat bladders.12 Severalstudies have confirmed high rates of bacteriuria(25% to 40%) in women with urodynamic refractoryDO13 and a wider group with clinical overactivebladder syndrome.14,15 A significant proportion ofwomen with detrusor overactivity are refractory toconventional treatment modalities.16 In this studywe examine the levels of intravesical ATP in pa-tients with refractory DO who are experiencing anacute exacerbation of DO symptoms. IntravesicalATP levels were correlated with the presence orabsence of bacteriuria.
MATERIALS AND METHODS
A 16-month prospective cohort study was performed at atertiary urogynecology unit. Women with urodynamicallyproven detrusor overactivity refractory to the standardtherapeutic strategies of behavioral modification and an-ticholinergic agents were considered eligible for study in-clusion. We defined refractory DO as failure to respond to2 or more anticholinergic agents coupled with outpatientbladder training for 1 year or more, with persistent dis-abling symptoms on frequency-volume chart.17
In December 2009 our departmental database wassearched for eligible women. A total of 68 women withrefractory DO were identified and were mailed a personalletter inviting them to participate in the study. Womenwere invited to attend our unit whenever their OAB symp-toms were acutely worsened, ie frequency, urgency, noc-turia (with or without urge incontinence). On presenta-tion, participants completed a validated 4-point (0, 1, 2, 3)urgency score (see table).18 All patients signed writtenconsent upon recruitment, and the study was approved bythe South Eastern Sydney Human Research and EthicsCommittee (reference 09/STG/72).
After recruitment, patients were catheterized by anexperienced study nurse using standard aseptic technique
Table
Urge Score Definition
0 None—no urgency1 Mild—awareness of urgency but is easily tolerated2 Moderate—enough urgency discomfort that it interferes with or s
3 Severe—extreme urgency discomfort that abruptly stops all activitiesand a standard 14Fr Nelaton catheter. A catheter speci-men of urine was retrieved, and forwarded immediately tothe microbiology laboratory for formal culture and sensi-tivity. After emptying the bladder, 50 ml sterile 0.9% NaClwas instilled to evoke gentle bladder stretch and the cath-eter clamped. After 5 minutes in situ, the saline wascollected for ATP analysis and the catheter was removed.The decision to prescribe empirical antibiotic treatmenton the day of specimen collection was made on an individ-ual basis according to patient symptoms. All womenwhose CSU specimens cultured bacteriuria 103 cfu/ml orgreater at 48 hours were treated with a 1-week course ofappropriate antibiotic therapy according to sensitivitytesting. All study participants were invited to return onany subsequent occasions whenever OAB symptoms wereacutely worsened.
CSU specimens from study participants were culturedusing horse blood agar incubated at 35C in 7% CO2 andMacConkey’s agar incubated at 35C in air. These culturemedia grow all known pathogens and contaminants.Pyuria was determined using hemocytometer counts onuncentrifuged urine specimens with counts of more than10 white blood cells per �l considered significant. Anybacteriuria 103 cfu/ml or greater was considered a positiveurine culture, in accordance with recent guidelines.19
Specimens with bacteriuria less than 103 cfu/ml were con-sidered sterile.
Saline samples were immediately stored at 4C andthen assayed for ATP within 30 minutes. ATP analysiswas performed immediately on 100 �l specimens takenfrom the top of the 50 ml saline bladder wash using aroutine luciferin/luciferase bioluminescence assay (Sigma)and a GloMax® 20/20 Luminometer.9 A standard ATPcalibration curve was constructed before and after per-forming the study assay using serial dilutions of ATPcreated from stock solution to allow correction for back-ground reagent values.
Median ATP concentrations were compared using theMann-Whitney test for nonparametric data. Paired anal-yses were performed using the Wilcoxon sign rank test.Two-tailed p values are reported throughout and the 5%level was considered significant. Statistical analysis wasperformed using Statsdirect 2.7.2.
RESULTS
Between January 1, 2010 and March 31, 2011, 33women with refractory DO were recruited and theysupplied 56 study specimens. The median (IQR) ageof women recruited was 70 (60–74) years. Studyparticipants were a severely affected group with amedian duration of OAB symptoms of 20 (8–24)
No. Sterile (%) No. Bacteriuric (%) Median nM ATP (IQR)
1 (2) 02 (5) 4 (27) 49.8 (9.3–64.4)
usual activities 13 (33) 5 (33) 39.1 (27.3–56.5)
hortens 24 (60) 6 (40) 37.0 (9.5–60.8)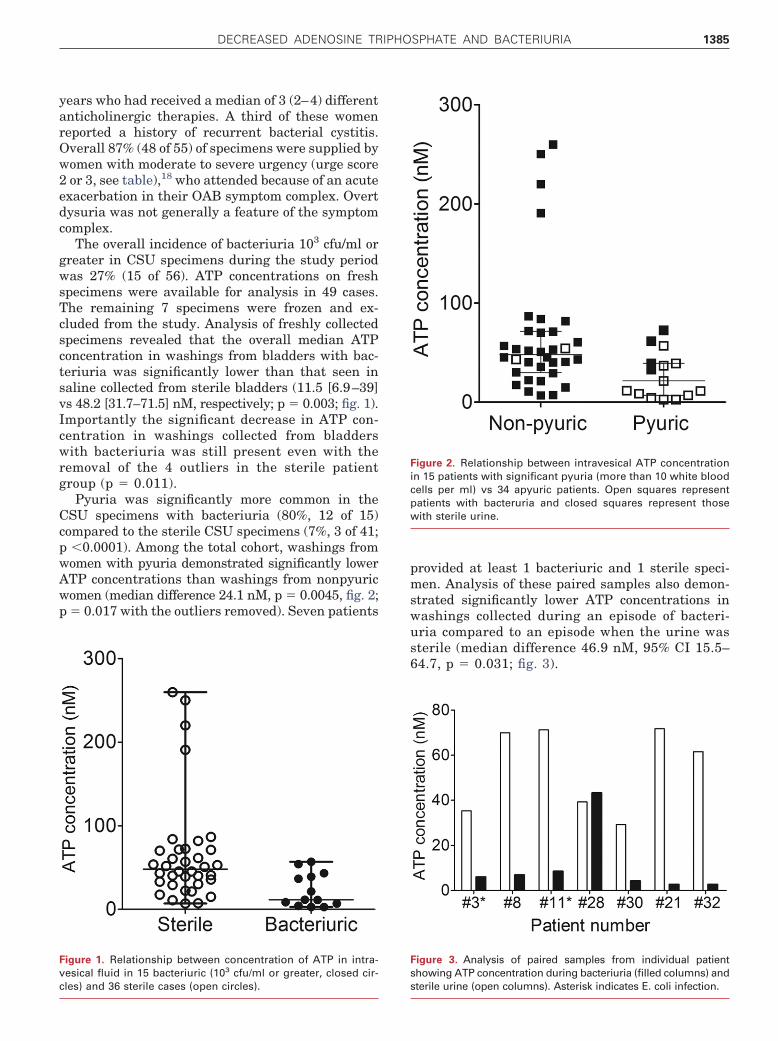
DECREASED ADENOSINE TRIPHOSPHATE AND BACTERIURIA 1385
years who had received a median of 3 (2–4) differentanticholinergic therapies. A third of these womenreported a history of recurrent bacterial cystitis.Overall 87% (48 of 55) of specimens were supplied bywomen with moderate to severe urgency (urge score2 or 3, see table),18 who attended because of an acuteexacerbation in their OAB symptom complex. Overtdysuria was not generally a feature of the symptomcomplex.
The overall incidence of bacteriuria 103 cfu/ml orgreater in CSU specimens during the study periodwas 27% (15 of 56). ATP concentrations on freshspecimens were available for analysis in 49 cases.The remaining 7 specimens were frozen and ex-cluded from the study. Analysis of freshly collectedspecimens revealed that the overall median ATPconcentration in washings from bladders with bac-teriuria was significantly lower than that seen insaline collected from sterile bladders (11.5 [6.9–39]vs 48.2 [31.7–71.5] nM, respectively; p � 0.003; fig. 1).Importantly the significant decrease in ATP con-centration in washings collected from bladderswith bacteriuria was still present even with theremoval of the 4 outliers in the sterile patientgroup (p � 0.011).
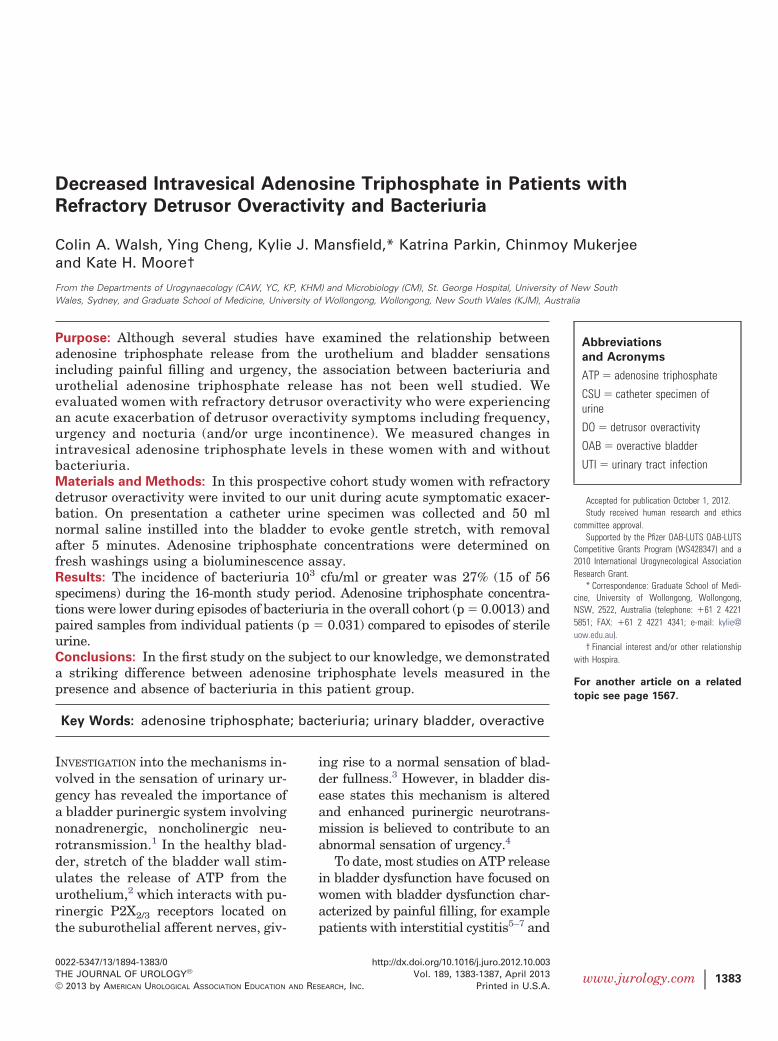
Pyuria was significantly more common in theCSU specimens with bacteriuria (80%, 12 of 15)compared to the sterile CSU specimens (7%, 3 of 41;p �0.0001). Among the total cohort, washings fromwomen with pyuria demonstrated significantly lowerATP concentrations than washings from nonpyuricwomen (median difference 24.1 nM, p � 0.0045, fig. 2;p � 0.017 with the outliers removed). Seven patients
Figure 1. Relationship between concentration of ATP in intra-vesical fluid in 15 bacteriuric (103 cfu/ml or greater, closed cir-
cles) and 36 sterile cases (open circles).provided at least 1 bacteriuric and 1 sterile speci-men. Analysis of these paired samples also demon-strated significantly lower ATP concentrations inwashings collected during an episode of bacteri-uria compared to an episode when the urine wassterile (median difference 46.9 nM, 95% CI 15.5–64.7, p � 0.031; fig. 3).
Figure 2. Relationship between intravesical ATP concentrationin 15 patients with significant pyuria (more than 10 white bloodcells per ml) vs 34 apyuric patients. Open squares representpatients with bacteruria and closed squares represent thosewith sterile urine.
Figure 3. Analysis of paired samples from individual patientshowing ATP concentration during bacteriuria (filled columns) and
sterile urine (open columns). Asterisk indicates E. coli infection.
DECREASED ADENOSINE TRIPHOSPHATE AND BACTERIURIA1386
There was no difference in ATP concentrations inwashings from Escherichia coli infected bladders (8)compared to those from nonE. coli infected bladders(7, p � 0.276) comprising Klebsiella (2), Streptococ-cus (2), Pseudomonas (1) and Enterococcus (1).There was no correlation between ATP concentra-tion and urge score (1-way ANOVA p � 0.862, seetable).
DISCUSSION
To our knowledge, an in vivo study of the effect ofbacteriuria on intravesical ATP release has not beenreported. One previous in vitro study examined theeffect of uropathogenic E. coli (more than 108 cfu/ml)on ATP release from a human urothelial cell line(UROtsa).20 This study demonstrated increasedATP release after a 1-hour treatment with uropatho-genic E. coli.20 In the present study more than aquarter of the women (27%) presenting with acuteexacerbation of DO symptoms characterized byworsening urgency had microbiological evidence ofbacteriuria. This is consistent with recent work.13–15
Based on the results of Säve and Persson in culturedUROtsa cells,20 we expected to see an increase inintravesical ATP concentrations in patients withbacteriuria. Thus, we were surprised to find thatbacteriuria was associated with significantly lowerATP concentrations in our study. This finding wasconsistent for the overall cohort of women (fig. 1) andin paired samples from individual study partici-pants (fig. 3).
This result is counterintuitive as patients withbacteriuria are known to experience symptoms offrequency and urinary urgency, although the urgescores were not significantly different in the sterilecompared to the bacteriuric cases (p � 0.064, seetable). Furthermore, the patients in the presentstudy were invited to present to our unit when theywere experiencing an acute exacerbation of OABsymptoms. Based on the in vitro experiments previ-ously described20 and the known role of ATP inafferent signaling,3,4 we predicted that we would seean increase in the ATP concentration in women withbacteriuria. Increased ATP release in bladder dys-function has previously been described in womenwith disorders characterized by painful bladder fill-ing.6–8 Our previous study in patients with DO alsodid not demonstrate increased ATP concentrations(compared to control women).9
It is not immediately apparent why women withrefractory DO should have lower ATP concentra-tions during episodes of bacteriuria. A simple expla-nation for the decreased intravesical ATP concentra-tion in women with bacteriuria could be that there isreduced ATP release from infected urothelial cells.
Evidence for inhibition of urothelial ATP release bybacterial products is available. Studies have shownthat some serotypes of E. coli lipopolysaccharide (egO55) are able to inhibit stretch induced ATP release,while other serotypes (eg O111) have no effect onurothelial ATP release.21 In addition, pyocyanin, avirulence factor of Pseudomonas aeruginosa, hasbeen shown to decrease ATP release from a urothe-lial cancer cell line in culture.22
Another factor that could influence the release ofATP in patients with bacteriuria is the viability ofthe urothelial cells. Women with bacterial cystitishave evidence of intracellular bacterial colonizationof urothelial cells, which is not demonstrated inasymptomatic control specimens.23 A smaller studyhas since found evidence of urothelial bacterial col-onization in women with the overactive bladder syn-drome.24 This intracellular colonization may lead toexfoliation of urothelial cells.23 Therefore, UTI mayresult in fewer viable urothelial cells. In addition,bacterial colonization may trigger apoptosis ofurothelial cells. These studies lend credence to theconcept that bacterial colonization may impair theendogenous release of ATP from the urothelium.
It is also possible that the lower ATP concentra-tions observed in patients with bacteriuria are re-lated to an increased breakdown of ATP (rather thanreduced ATP release). Ecto-ATPases are enzymeswhich break down extracellular ATP.25 Harvey et alconcluded that reduced activity of ecto-ATPases con-tributes to the higher ATP levels observed in somebladder disorders such as idiopathic detrusor insta-bility.26 Several different ecto-ATPases are knownto be localized to the bladder urothelium.27 The ac-tivity of endothelial ecto-ATPase can be altered bybacterial lipopolysaccharide.28 Therefore, infectionmay increase the enzymatic digestion of ATP, thusdecreasing ATP levels.
Digestion of ATP produces adenosine, which isknown to activate the immune response by stimu-lating chemotaxis of neutrophils.29 Such an inflam-matory response predisposes mice to recurrent cys-titis,30 an insidious problem in women and onedescribed by many of the patients with refractoryDO included in this study. However, the potentialeffect of UTI on ecto-ATPase activity and bladderATP concentrations in the human has not been in-vestigated.
In the present study more than a quarter of thewomen (27%) who presented with worsening ur-gency had microbiological evidence of bacteriuria inkeeping with other recent work.13–15 This reinforcesthe notion that women with refractory DO and anacute worsening of urinary urgency may have anincreased incidence of bacteriuria that may alter thenormal purinergic functioning of the afferent system
in these patients.
DECREASED ADENOSINE TRIPHOSPHATE AND BACTERIURIA 1387
CONCLUSIONSWomen with refractory detrusor overactivity whopresent with an acute worsening of urgency symp-toms have a high rate (27%) of bacteriuria. We dem-onstrated a decrease in ATP levels measured in thepresence of bacteriuria. This unexpected findinghighlights the need for greater understanding of the
effects of bacteriuria on the purinergic system andREFERENCES
2010; 57: 1087. receptor activation induce a
how this relates to the sensation of urinary urgencyin patients with refractory DO.
ACKNOWLEDGMENTS
Wendy Allen assisted with patient recruitment,
sample collection and study coordination.1. Burnstock G: Purine and pyrimidine receptors.Cell Mol Life Sci 2007; 64: 1471.
2. Ferguson DR, Kennedy I and Burton TJ: ATP isreleased from rabbit urinary bladder epithelialcells by hydrostatic pressure changes–a possiblesensory mechanism? J Physiol 1997; 505: 503.
3. Vlaskovska M, Kasakov L, Rong W et al: P2X3knock-out mice reveal a major sensory role forurothelially released ATP. J Neurosci 2001; 21:5670.
4. Burnstock G: Therapeutic potential of purinergicsignalling for diseases of the urinary tract. BJUInt 2011; 107: 192.
5. Palea S, Artibani W, Ostardo E et al: Evidence forpurinergic neurotransmission in human urinarybladder affected by interstitial cystitis. J Urol1993; 150: 2007.
6. Sun Y, Keay S, De Deyne PG et al: Augmentedstretch activated adenosine triphosphate releasefrom bladder uroepithelial cells in patients withinterstitial cystitis. J Urol 2001; 166: 1951.
7. Sun Y, Keay S, DeDeyne P et al: Stretch-activatedrelease of adenosine triphosphate by bladderuroepithelia is augmented in interstitial cystitis.Urology 2001; 57: 131.
8. Kumar V, Chapple CR, Surprenant AM et al:Enhanced adenosine triphosphate release fromthe urothelium of patients with painful bladdersyndrome: a possible pathophysiological explana-tion. J Urol 2007; 178: 1533.
9. Cheng Y, Mansfield KJ, Allen W et al: Doesadenosine triphosphate released into voided uro-dynamic fluid contribute to urgency signaling inwomen with bladder dysfunction? J Urol 2010;183: 1082.
10. Kumar V, Chapple CR, Rosario D et al: In vitrorelease of adenosine triphosphate from theurothelium of human bladders with detrusor over-activity both neurogenic and idiopathic. Eur Urol
11. Bours MJ, Swennen EL, Di Virgilio F et al: Aden-osine 5=-triphosphate and adenosine as endoge-nous signaling molecules in immunity and inflam-mation. Pharmacol Ther 2006; 112: 358.
12. Yu Y and de Groat WC: Sensitization of pelvicafferent nerves in the in vitro rat urinary bladder-pelvic nerve preparation by purinergic agonistsand cyclophosphamide pretreatment. Am JPhysiol Renal Physiol 2008; 294: F1146.
13. Walsh CA, Allen W, Parkin K et al: Low-countbacteriuria in refractory idiopathic detrusor over-activity versus controls. Urogynaecologia 2011;25: e4.
14. Khasriya R, Khan S, Lunawat R et al: The inade-quacy of urinary dipstick and microscopy as sur-rogate markers of urinary tract infection in uro-logical outpatients with lower urinary tractsymptoms without acute frequency and dysuria.J Urol 2010; 183: 1843.
15. Hessdoerfer E, Jundt K and Peschers U: Is adipstick test sufficient to exclude urinary tractinfection in women with overactive bladder? IntUrogynecol J Pelvic Floor Dysfunct 2011; 22: 229.
16. Morris AR, Westbrook JI and Moore KH: A lon-gitudinal study over 5 to 10 years of clinicaloutcomes in women with idiopathic detrusoroveractivity. BJOG 2008; 115: 239.
17. Moore KH, Nickson P, Richmond DH et al: Detru-sor mast cells in refractory idiopathic instability.Br J Urol 1992; 70: 17.
18. Nixon A, Colman S, Sabounjian L et al: A vali-dated patient reported measure of urinary ur-gency severity in overactive bladder for use inclinical trials. J Urol 2005; 174: 604.
19. Grabe M, Bishop MC, Bjerklund-Johansen TE etal: Guidelines on urological infections. Euro-pean Association of Urology 2009. Available atwww.uroweb.org/guidelines/onlineguidelines.Accessed November 7, 2011.
20. Säve S and Persson K: Extracellular ATP and P2Y
proinflammatory hostresponse in the human urinary tract. Infect Immun2010; 78: 3609.
21. Mansfield K, Cheng Y and Moore K: Treatment ofurothelial cells with lipopolysaccharide from en-teropathogenic E. coli reduces stretch inducedATP release. J Urol, suppl., 2012; 187: e368,abstract 904.
22. McDermott C, Chess-Williams R, Grant GD et al:Effects of Pseudomonas aeruginosa virulence fac-tor pyocyanin on human urothelial cell functionand viability. J Urol 2012; 187: 1087.
23. Rosen DA, Hooton TM, Stamm WE et al: Detec-tion of intracellular bacterial communities in hu-man urinary tract infection. PLoS Med 2007; 4:1949.
24. Khasriya RK, Ismail S, Wilson M et al: A newaetiology for OAB: intracellular bacterial coloni-sation of urothelial cells. Presented at 36th an-nual meeting of the International Urogynecologi-cal Association, Lisbon, Portugal, June 28-July 2,2011.
25. Plesner L: Ecto-ATPases: identities and functions.Int Rev Cytol 1995; 158: 141.
26. Harvey RA, Skennerton DE, Newgreen D et al:The contractile potency of adenosine triphos-phate and ecto-adenosine triphosphatase activityin guinea pig detrusor and detrusor from patientswith a stable, unstable or obstructed bladder.J Urol 2002; 168: 1235.
27. Yu W, Robson SC and Hill WG: Expression anddistribution of ectonucleotidases in mouse uri-nary bladder. PLoS One 2011; 6: e18704.
28. Kittel A: Lipopolysaccharide treatment modifiespH- and cation-dependent ecto-ATPase activity ofendothelial cells. J Histochem Cytochem 1999;47: 393.
29. Junger WG: Purinergic regulation of neutrophilchemotaxis. Cell Mol Life Sci 2008; 65: 2528.
30. Hannan TJ, Mysorekar IU, Hung CS et al: Earlysevere inflammatory responses to uropathogenicE. coli predispose to chronic and recurrent urinary
tract infection. PLoS Pathog 2010; 6: e1001042.




























