Embed Size (px)
Citation preview

1
Not to be reproduced or copied without permission from Kidney Health Australia
Decision making and symptom control
in kidney failure
Primary Care Education WorkshopThis module was conceived and developed by PEAK*
Presented by: Dr Stephen May
V0621
2
Not to be reproduced or copied without permission from Kidney Health Australia
Housekeeping
Housekeeping

3
Not to be reproduced or copied without permission from Kidney Health Australia
Acknowledgements:
Thanks to the ‘Primary Care Education Advisory
Committee for Kidney Health Australia’ (PEAK) who
has developed and reviewed this education.
Thanks to our volunteer presenters!
Thanks to our webinar sponsors
4
Not to be reproduced or copied without permission from Kidney Health Australia
Learning outcomes
1. Describe comprehensive conservative care as a treatment option for Kidney Failure
2. Recognise and manage common symptoms and complications in Kidney Failure
3. Discuss end-of-life in the setting of Kidney Failure
Learning aim
Provide the tools for management of all stages of Chronic Kidney disease (CKD) in a primary care setting.
5
Not to be reproduced or copied without permission from Kidney Health Australia

6
Not to be reproduced or copied without permission from Kidney Health Australia
What is CKD?
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p7
CKD is defined as…

7
Not to be reproduced or copied without permission from Kidney Health Australia
How prevalent is CKD in
Australian adults?
a) 1 in 5
b) 1 in 10
c) 1 in 20
d) 1 in 100
Question:
8
Not to be reproduced or copied without permission from Kidney Health Australia
How prevalent is CKD in
Australian adults?
a) 1 in 5
b) 1 in 10
c) 1 in 20
d) 1 in 100
Answer:

9
Not to be reproduced or copied without permission from Kidney Health Australia
CKD is a major public health problem
1.Australia Bureau of Statistics. Australian Health Survey: Biomedical Results for Chronic Diseases,2011‐12. ABS, Canberra; 2013
2. Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020
1 in 10 Australian adults has
CKD1
Less than 10% of people with
CKD are aware they have the
condition2 2
Major independent risk factor for cardiovascular
disease2
common, harmful & treatable
10
Not to be reproduced or copied without permission from Kidney Health Australia
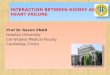
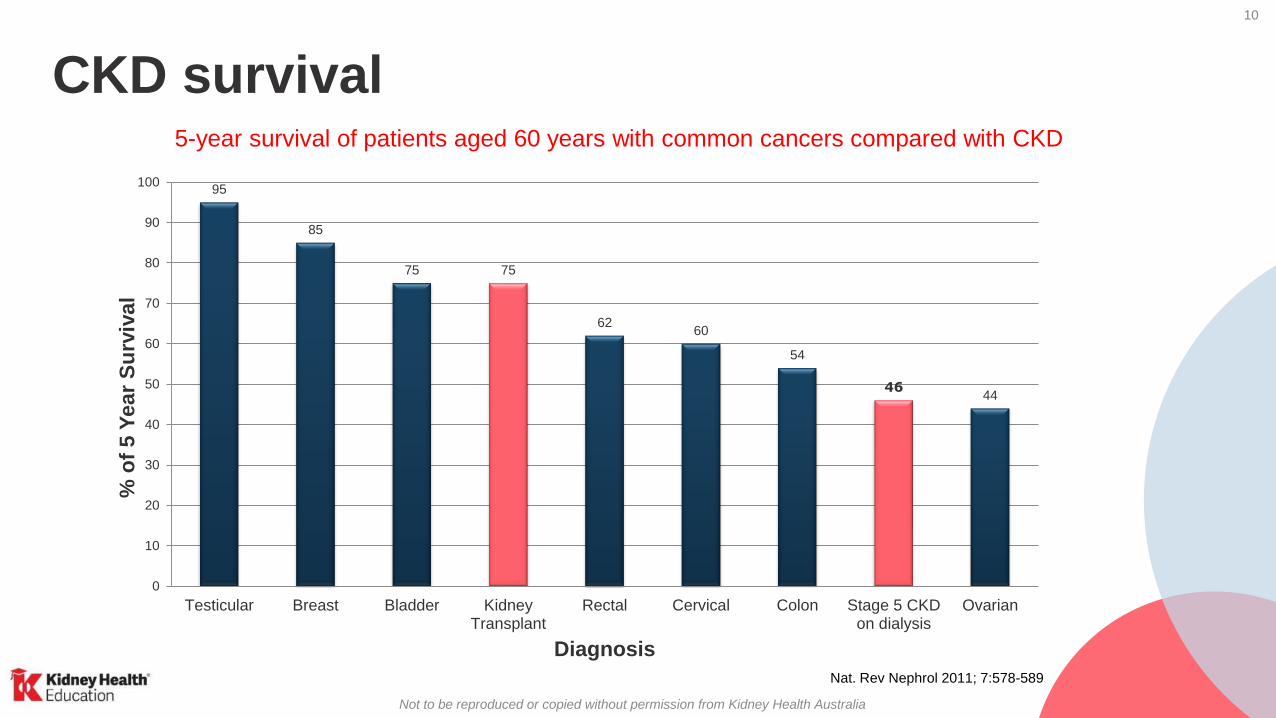
Nat. Rev Nephrol 2011; 7:578-589
95
85
75 75
6260
54
4644
0
10
20
30
40
50
60
70
80
90
100
Testicular Breast Bladder KidneyTransplant
Rectal Cervical Colon Stage 5 CKDon dialysis
Ovarian
% o
f 5 Y
ear
Su
rviv
al
Diagnosis
CKD survival5-year survival of patients aged 60 years with common cancers compared with CKD
11
Not to be reproduced or copied without permission from Kidney Health Australia
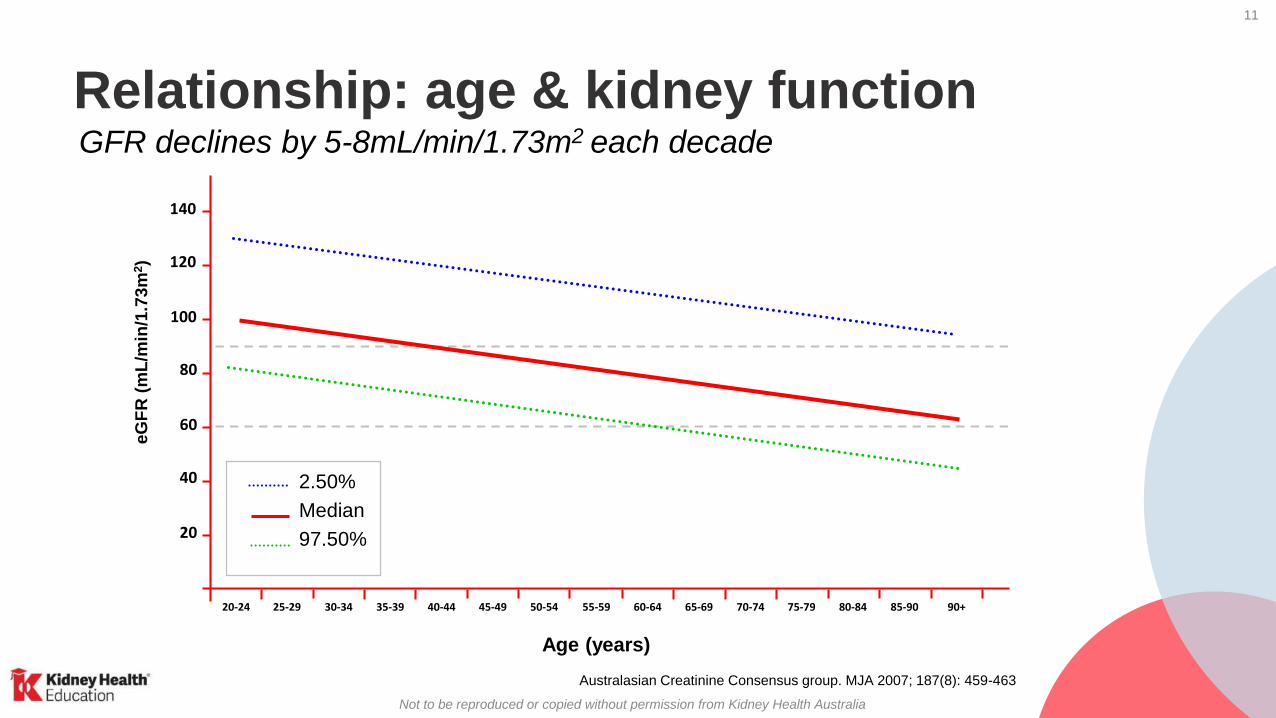
20-24
Age (years)
20
40
60
80
100
120
140
25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-90 90+
eG
FR
(mL
/min
/1.7
3m
2)
2.50%
Median
97.50%
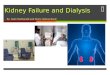
Australasian Creatinine Consensus group. MJA 2007; 187(8): 459-463
Relationship: age & kidney functionGFR declines by 5-8mL/min/1.73m2 each decade
12
Not to be reproduced or copied without permission from Kidney Health Australia
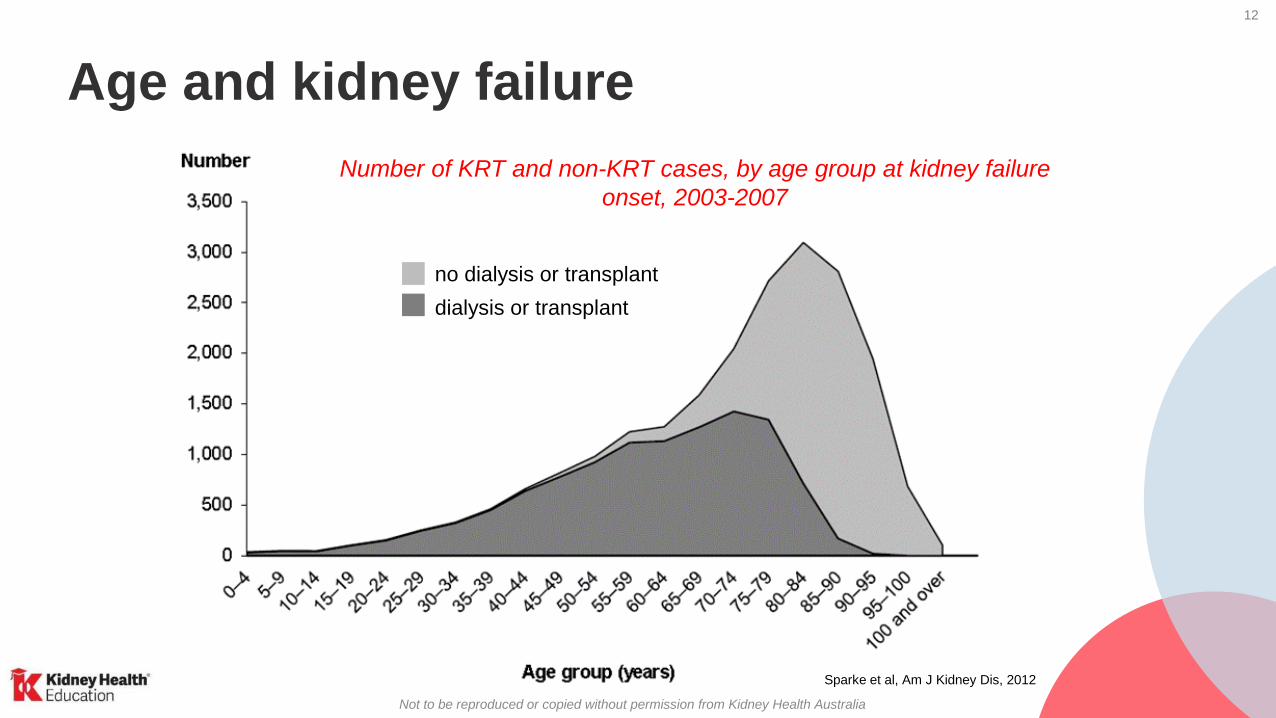
Age and kidney failure
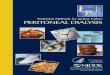
Number of KRT and non-KRT cases, by age group at kidney failure
onset, 2003-2007
Sparke et al, Am J Kidney Dis, 2012
no dialysis or transplant
dialysis or transplant

13
Not to be reproduced or copied without permission from Kidney Health Australia
Who cares for kidney failure patients?
• For elderly individuals with kidney failure –
who cares for them?
– General practitioner
– Geriatrician
– Nephrologist
• In practice only a small percentage will be
referred to a nephrologist

14
Not to be reproduced or copied without permission from Kidney Health Australia
Case study - Jim
Background
• 74 years old
• Retired farmer
• Lives at home in a small rural
town with his wife of 26 years

15
Not to be reproduced or copied without permission from Kidney Health Australia
Case study - Jim
Medical history
Type 2 diabetes Insulin-dependent 5 years
Neuropathy, retinopathy, previous
osteomyelitis & foot ulcers
Hypertension 15 years
Hypercholesterolaemia 15 years
Ischaemic heart disease 10 years
L Nephrectomy In 2006 for kidney cancer
eGFR 18 mL/min/1.73 m2
(20 mL/min/1.73m2 4 months ago)
Albumin/ creatinine ratio 28 mg/mmol
Pulmonary fibrosis Needs oxygen at night
Medications Diltiazem, perindopril, aspirin, simvastatin,
atenolol

16
Not to be reproduced or copied without permission from Kidney Health Australia
Staging CKDCombine eGFR stage, albuminuria stage and underlying diagnosis to specify CKD stage
e.g. stage 3b CKD with microalbuminuria secondary to diabetic kidney disease
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020
Jim is hereJim is here

17
Not to be reproduced or copied without permission from Kidney Health AustraliaChronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p31-33
Managing CKD in primary care
Follow the corresponding
colour-coded action plan
found in the handbook

18
Not to be reproduced or copied without permission from Kidney Health Australia
At this stage in Jim’s CKD, what are your main management goals?
Options:
a) Continue to monitor Jim
b) Refer to Nephrologist
c) Discuss treatment options for kidney failure
d) Discuss an Advance Care Directive with Jim
Question:
Case study

19
Not to be reproduced or copied without permission from Kidney Health Australia
c) It’s important to discuss the future and ALL the options, in full,
with patients and their family members 3-6 months BEFORE
treatment is required and/or urgent
d) Advance Care Directive
b) Referral to a Nephrologist is recommended when eGFR
<30 mL/min/1.73m2. Appropriate referral not only allows for
appropriate management but provides time to discuss treatment
options.
Answer
20
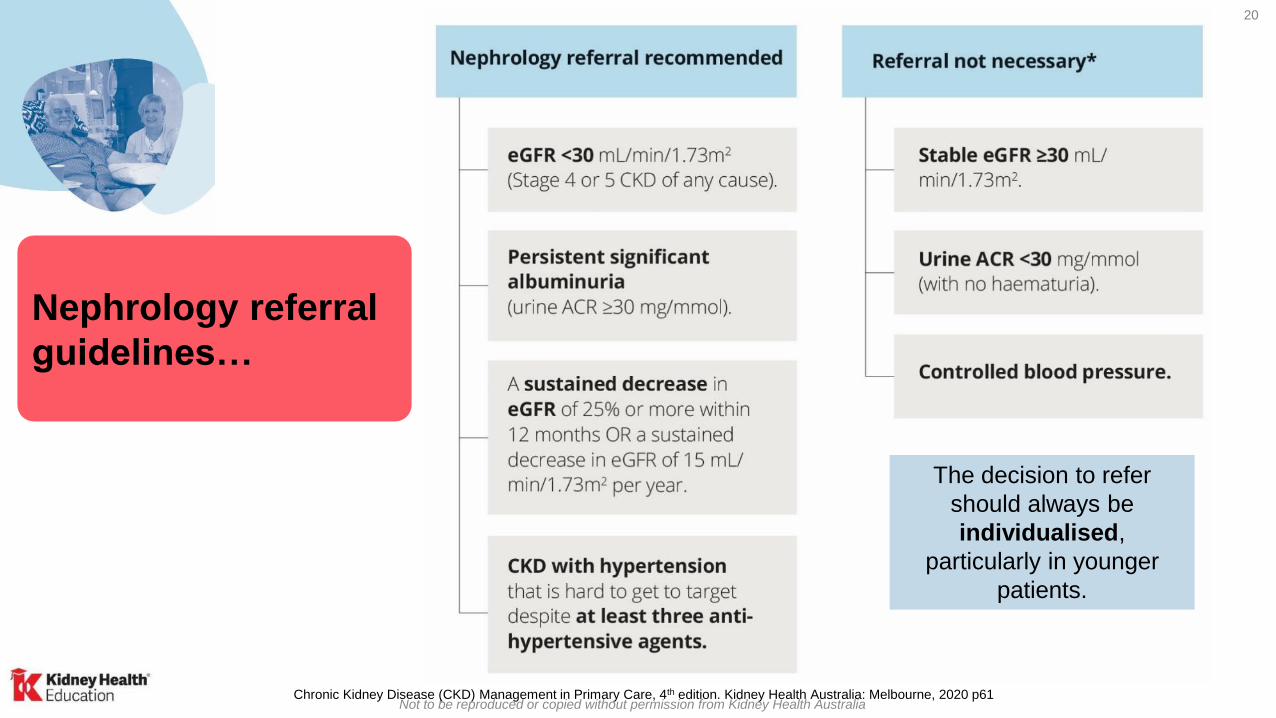
Not to be reproduced or copied without permission from Kidney Health AustraliaChronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p61
Nephrology referral
guidelines…
The decision to refer
should always be
individualised,
particularly in younger
patients.

21
Not to be reproduced or copied without permission from Kidney Health Australia
Preserve Kidney Function

22
Not to be reproduced or copied without permission from Kidney Health Australia

23
Not to be reproduced or copied without permission from Kidney Health Australia
Preserve Kidney Function

24
Not to be reproduced or copied without permission from Kidney Health Australia
Treatment options - Dialysis
Haemodialysis is connecting to a
haemodialysis machine at home
or hospital, ~3x /week lasting 5
hours each.
Peritoneal Dialysis is a
tube permanently inserted into the
abdomen. Fluids are then introduced
regularly to draw waste from the body.

25
Not to be reproduced or copied without permission from Kidney Health Australia
• 4-7 years ave. wait time for a
deceased donor organ
• Living donor transplants- before
dialysis is started- is called pre-
emptive transplantation
– make up 11% of all transplant
operations in Australia.
Treatment options - Transplantation
26
Not to be reproduced or copied without permission from Kidney Health Australia
Treatment options - Comprehensive
Conservative Care
• Dialysis or kidney transplantation is not suited to
everyone
• Comprehensive Conservative Care (CCC) aims to
preserve kidney function through dietary management
and medications
• CCC cannot stop the decline in kidney function
Further information on treatment options available at www.kidney.org.au
or by calling Kidney Helpline on 1800 454 363
27
Not to be reproduced or copied without permission from Kidney Health Australia
Treatment options for kidney failure
Comprehensive Conservative Care
• A treatment for kidney failure that does not involve dialysis or transplant.
• Aimed at minimising symptoms and complications with medication and maximising quality of life
• Progression to end of life will occur
• Lifestyle and Quality Of Life are important considerations in choosing the right treatment

28
Not to be reproduced or copied without permission from Kidney Health Australia
CKD 3/4
Diagnosis & treatment, treat
comorbidities & slow progression
Renal Unit CKD Management
CKD 3/4
Estimate progression, treat complications,
educate patient & family about all treatment
options
CKD 5
Treatment = Dialysis, transplantation or
CCC, control symptoms, address
complications, QOL
Manage complications of CKD
Palliative
care (end of
life)
Palliative Care
CKD risk factor reduction, CKD management
Screen patients for CKD risk factors
Primary Care CKD Management
CKD
diagnosis /
progression
Referral to NephrologistCKD progression
CKD pathway

29
Not to be reproduced or copied without permission from Kidney Health Australia
It is not a static
process and is
not limited to a
single point in
time
Decision making
Peritoneal dialysis
Transplant
Nocturnal dialysis
Haemodialysis
CCC
Home dialysis

30
Not to be reproduced or copied without permission from Kidney Health Australia
Case study
Imagine that you have recently learned that you
have stage 4 CKD and are likely to progress to
Kidney Failure within the next 3 months.
What factors in your own situation
might change your management
choice?
Submit your suggestions in the
public chat box.
Question:

31
Not to be reproduced or copied without permission from Kidney Health Australia
Treatment options: what is important for patients?
• Lifestyle and QOL issues are very important for patients:
- Time of day dialysis is available
- Number of visits to hospital/centre for dialysis per week
- Difficulty and cost of transport to dialysis
- Travel and holiday options
• Patients approaching Kidney Failure may be willing to trade
considerable life expectancy to reduce the burden and restrictions
imposed by dialysis
Morton RL et al. CMAJ 2012
Relocation

32
Not to be reproduced or copied without permission from Kidney Health Australia
Case study - Jim
What could you do if Jim was
struggling with the decision about
treatment?
Submit your suggestions in the
public chat box.
Question:
You discuss each treatment option with Jim and his wife.
You feel that Jim has a good understanding of the options
available.

33
Not to be reproduced or copied without permission from Kidney Health Australia
Renal Replacement
Pathway
Conservative Care Pathway
Undecided PathwayAll Options
legitimate

34
Not to be reproduced or copied without permission from Kidney Health Australia
Legal issues
Where do things stand legally when a patient refuses dialysis
treatment or chooses to stop dialysis treatment.
• Jim makes an appointment to see you without his wife present.
• He makes it clear that he “does not want to be hooked up to
machines; he wants to be at home.”
• He has told his wife and children, but they are not happy with this
decision.
Declines
35
Not to be reproduced or copied without permission from Kidney Health Australia
Legal issues Unless incompetent, patients have an absolute legal &
moral right to consent to, withdraw or refuse treatment
without any obligation to explain.
• Doctors have a responsibility to:– fully inform
– discuss options and reasons
– support
• If a doctor has concerns about competence, or legal
implications, then they should:– seek another opinion
– discuss with colleagues & the patient's nephrologist), and/or
– obtain advice from their medical indemnity provider
Decline

36
Not to be reproduced or copied without permission from Kidney Health Australia
Case study
How would you help Jim’s family
understand Jim’s decision for
non-dialysis care?
Question: Submit your suggestions in the
public chat box.

37
Not to be reproduced or copied without permission from Kidney Health Australia
CARI recommendation for
dialysis
is an expectation of
survival with a quality of
life acceptable to the
patient
38
Not to be reproduced or copied without permission from Kidney Health Australia
SurvivalDialysis versus a non-dialysis pathway
An Australasian study showed that elderly patients with kidney failure who commence dialysis have high mortality.
• 1-year survival of 77%, 2-year survival of 59% and 3-year survival of 45%
• Survival of elderly patients with Kidney Failure on a non-dialysis pathway is difficult to estimate because of lack of data
• Survival without dialysis may be between 9 - 22 months
• More comorbidities = worse outcomes
Foote C, Ninomiya T, Gallagher M et al. NDT 2012
39
Not to be reproduced or copied without permission from Kidney Health Australia
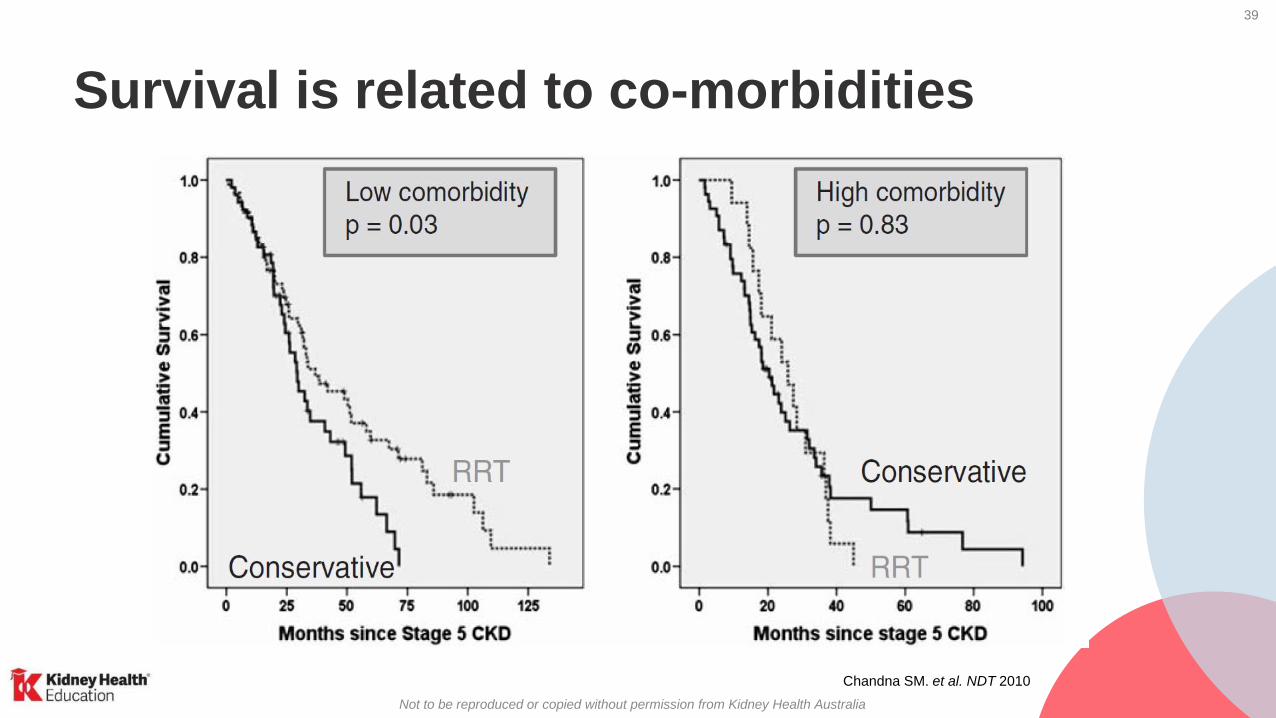
Survival is related to co-morbidities
Chandna SM. et al. NDT 2010

40
Not to be reproduced or copied without permission from Kidney Health Australia
Factors in Survival
• Age
• Comorbidities
• Frailty
• Social Determinants
41
Not to be reproduced or copied without permission from Kidney Health Australia
Case study – Jim
• Jim and his family visit the local dialysis centre and meet
with the renal team and community palliative care team.
• After a series of conferences Jim and his family agree the
best pathway is comprehensive conservative care at
home, with involvement of the local GP and palliative
care team
• What to expect now…

42
Not to be reproduced or copied without permission from Kidney Health Australia
Jim is seen a month later and is complaining of the
following issues
• Surges of neuropathic pain in his feet
• Severe itch
• A sensation of being unable to keep his legs still
• Ongoing breathlessness and nausea
• Difficulty sleeping
Jim’s family believe that Jim would not be
experiencing these symptoms if he was on dialysis.
Is this true or false?
Question:
Case study - Jim
a) True
b) False

43
Not to be reproduced or copied without permission from Kidney Health Australia
b) False....Symptoms in Kidney Failure managed with and without dialysis
Murtagh F et al, J Pall Med 2007; Adv Chr Kidney Dis 2007
Dialysis Non-dialysis
Fatigue/tiredness 71% 75%
Pruritus 55% 74%
Constipation 53%
Anorexia 49% 47%
Pain 47% 53%
Sleep disturbance 44% 42%
Anxiety 38%
Dyspnoea 35% 61%
Nausea 33%
Restless legs 30% 48%
Depression 27% 40%
44
Not to be reproduced or copied without permission from Kidney Health Australia
Symptom assessment
• Several symptom inventory tools validated for Kidney Failure
• Allow patients and clinicians to focus on symptoms causing
most difficulty
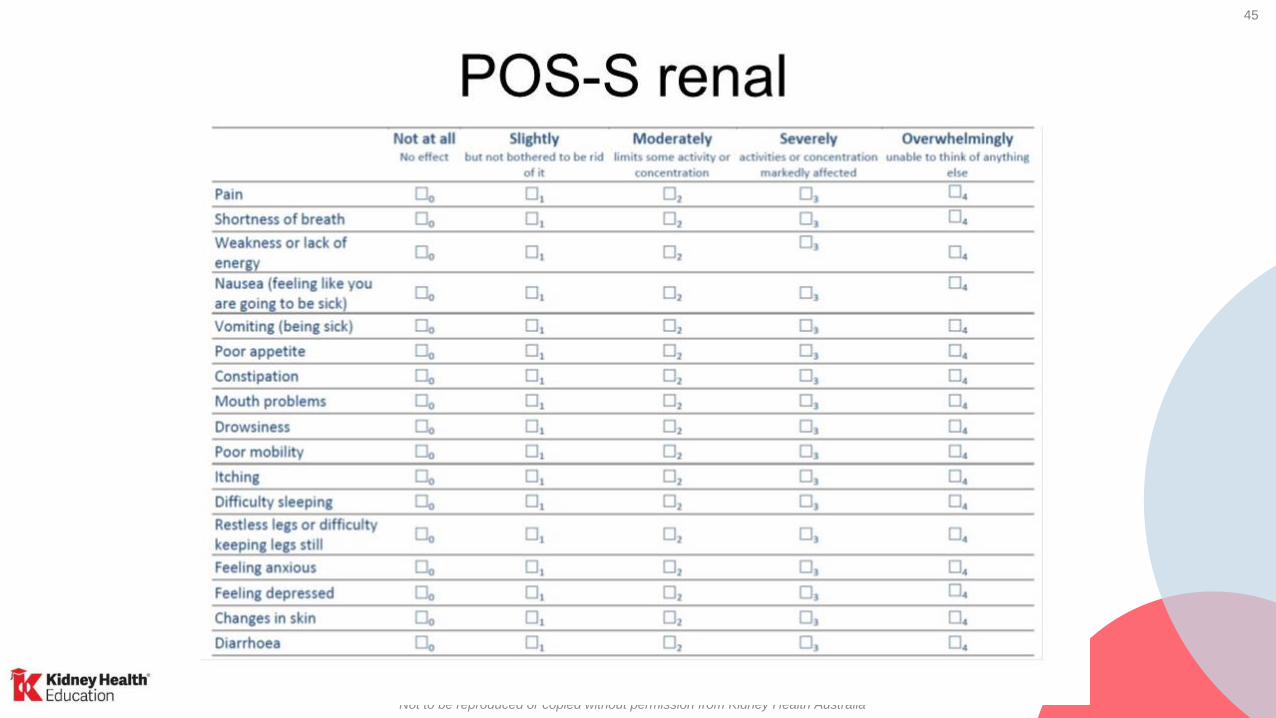
• Simple example is the Palliative care Outcome Scale –
Symptoms (POS-S) Renal instrument
- Validated for renal patients
- Symptom scores nil → overwhelming
- www.pos-pal.org
45
Not to be reproduced or copied without permission from Kidney Health Australia

46
Not to be reproduced or copied without permission from Kidney Health Australia
Case study – Jim’s Symptoms
You see Jim for his 6-monthly review
• His eGFR has decreased to 10 mL/min/1.73m2 (previously
18 mL/min/1.73m2)
• Jim has Stage 5 CKD with macroalbuminuria.
• Using the POS-S Renal tool you identify that Jim is having
the most difficulty with pain control.

47
Not to be reproduced or copied without permission from Kidney Health Australia
You see Jim for his six-monthly review. His eGFR has decreased to
10 mL/min/1.73m2 (previously 18 mL/min/1.73m2) Jim has Stage 5 CKD with macroalbuminuria
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p9
Case study- Jim
Jim is here

48
Not to be reproduced or copied without permission from Kidney Health Australia
Case study
What are the recommended steps for
managing pain for patients undergoing
comprehensive conservative care for
kidney failure?
a) Determine cause & severity
b) Develop pain management plan
c) Refer to pain clinic
d) I honestly have no idea
Question
49
Not to be reproduced or copied without permission from Kidney Health Australia
Pain in kidney failure
• Common in kidney failure with & without dialysis
• Variety of etiologies
- Musculoskeletal
- Neuropathic (diabetic neuropathy)
- Ischaemic (causes nociceptive, visceral, and neuropathic pains)
• Multidisciplinary approach consisting of nephrology, pain medicine,
palliative care, general practice, nursing and other relevant
disciplines is advised

50
Not to be reproduced or copied without permission from Kidney Health Australia
Pain management
It is important to determine a cause for the pain
Mild – moderate pain Moderate – severe pain
• Paracetamol or tramadol
• Analgesics not as effective for
neuropathic pain
• Avoid NSAIDS and COX-2
inhibitors: can adversely affect
kidney function
• Many opioids are renally excreted
• Opioid choice and dose/interval
individualised to each patient
o Fentanyl safest as its renally excreted
metabolites are inactive
o Morphine and oxycodone have active
metabolites which accumulate and can be
toxic
o Hydromorphone use is controversial as its
metabolite can accumulate → but evidence
in humans in lacking

51
Not to be reproduced or copied without permission from Kidney Health Australia
Common symptoms in kidney failure
• Acidosis
• Anaemia
• Cognitive decline
• Depression
• Haematuria
• Hyperkalaemia
• Malnutrition
• Muscle & bone disorder
• Muscle cramps
• Oedema
• Pruritus
• Restless legs
• Sleep apnoea
• Uraemia
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p68

52
Not to be reproduced or copied without permission from Kidney Health Australia
Anaemia in CKD
• Symptoms usually develop when eGFR
<60mL/min/1.73m2
• Prevalence increases as eGFR
declines
• Can contribute to symptoms of fatigue,
depression and sleep disturbances
• >70% of people with kidney failure
have anaemia1
1. Int. J. Mol. Sci. 2020, 21, 725; The Influence of Inflammation on Anemia in CKD Patients. Ann Gluba-Brzozka
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p70

53
Not to be reproduced or copied without permission from Kidney Health Australia
Cognitive decline
• CKD affects global cognition, attention,
memory & executive functions
• CKD is a risk factor or accelerated aging
• Cognitive impairment is common, & severity
increases with CKD stage
Things to consider in assessment:
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p71
o Screen for cognition in CKD – Mini-Mental
State Examination (MMSE)
o Safety
o Medication adherence / Medication review
o Falls
o Risk of delirium
o Self-care issues and engagement with care

54
Not to be reproduced or copied without permission from Kidney Health Australia
Psychosocial issues
• Depression and/or anxiety is common throughout CKD
& can affect:
1/5 people with CKD
&
1/3 people on dialysis
• Depression & CKD effect mortality, hospitalisation,
medication & treatment adherence, nutrition & quality
of life
• Screen regularly, maintain clinical awareness of
depression – DAS-21 or Kessler K10
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 pp71-72
55
Not to be reproduced or copied without permission from Kidney Health Australia
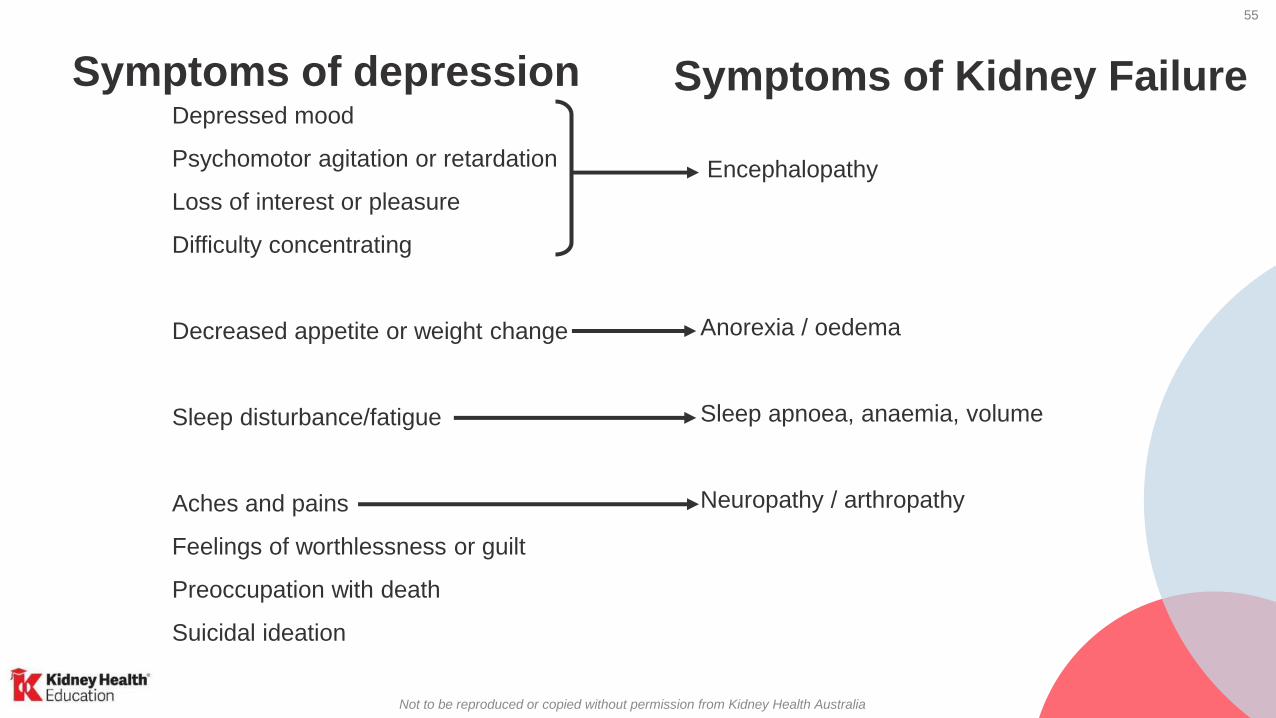
Symptoms of depression Symptoms of Kidney FailureDepressed mood
Psychomotor agitation or retardation
Loss of interest or pleasure
Difficulty concentrating
Decreased appetite or weight change
Sleep disturbance/fatigue
Aches and pains
Feelings of worthlessness or guilt
Preoccupation with death
Suicidal ideation
Encephalopathy
Anorexia / oedema
Sleep apnoea, anaemia, volume
Neuropathy / arthropathy
56
Not to be reproduced or copied without permission from Kidney Health Australia
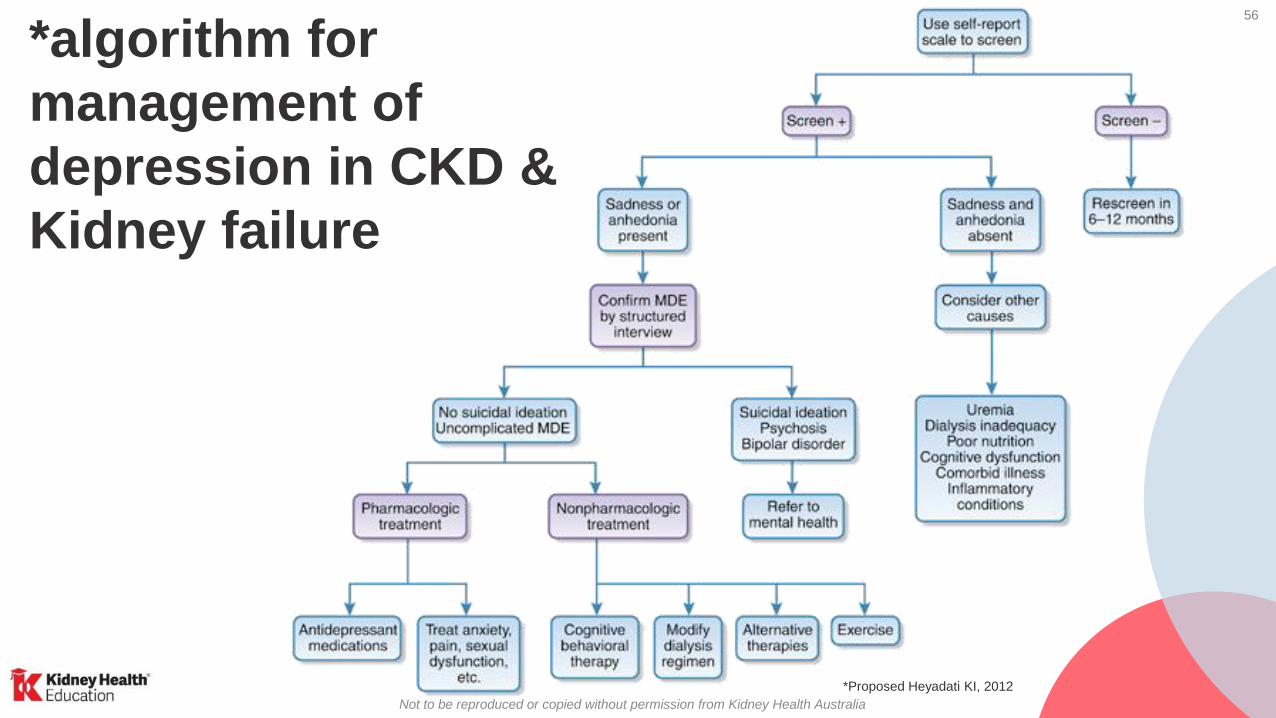
*algorithm for
management of
depression in CKD &
Kidney failure
*Proposed Heyadati KI, 2012
57
Not to be reproduced or copied without permission from Kidney Health Australia
Pruritus
• Itchy skin is a common and debilitating side
effect of CKD – affects up to 70% of people with
stage 4-5 CKD.
• Multifactorial causes:
– calcium & phosphate imbalance,
– inadequate dialysis,
– overactive parathyroid glad,
– magnesium and Vit A levels,
– nerve changes in the skin
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p78

58
Not to be reproduced or copied without permission from Kidney Health Australia
Restless legs syndrome
• Common in kidney failure with & without dialysis
with eGFR <15mL/min/1.73m2
• May increase in severity as death approaches
• Affects quality of life through sleep disturbance
• Home therapies such as massage, warm baths,
warm/cool compresses, relaxation techniques may
be beneficial
Chronic Kidney Disease (CKD) Management in Primary Care, 4th edition. Kidney Health Australia: Melbourne, 2020 p78
If the patient
is troubled by
both uraemic
pruritus and
restless legs
syndrome
commence
Gabapentin
as it has been
shown to
have efficacy
in both
symptoms.
*Gabapentin is PBS indicated for refractory neuropathic pain
59
Not to be reproduced or copied without permission from Kidney Health Australia
Case study Jim
For Jim’s neuropathic pain, pruritus and restless leg syndrome…
• Gabapentin for (may also help with sleep?)
→Titrate up by 100mg increments according to tolerability and response
- If eGFR >50 commence 100mg tds
- If eGFR 30-49 commence 100mg nocte – 100mg bd and titrate up
- If eGFR 15-29 commence 100mg nocte and titrate
- If eGFR <15 commence 100mg every second night and titrate up
For Jim, the following treatment and dosing was considered in his
comprehensive conservative care plan…

60
Not to be reproduced or copied without permission from Kidney Health Australia
Case study - Jim
For Jim’s nausea…
• Metoclopramide HCl – 10mg half hour before meals
• Also helps early satiety and gastroparesis related to diabetes
• Haloperidol
- Elimination is via bile, faeces and urine; If eGFR < 10 or dialysis begin with low end of
dose range; In elderly use low doses to avoid extrapyramidal reactions; Increased risk of
sedation in renal failure and 50% of normal dose is recommended
- Minimal commencing dose - 0.5 mg.
- Typical commencing doses for:
* Nausea - 0.5 mg bd * Delirium - 1mg bd
• Ondansetron not recommended due to it being expensive & constipating

61
Not to be reproduced or copied without permission from Kidney Health Australia
Nausea
• Common and often multifactorial in origin
• Significantly affects quality of life & nutritional intake
• Metoclopramide hydrochloride as first line
• Haloperidol recommended (start with dose at lower end of
effective range e.g. 0.5mg bd)
• Levomepromazine can be used if symptoms persist, but it is
more sedating
• Cyclizine not recommended as may cause hypotension or
arrhythmia in patients with cardiac comorbidities; use only
under palliative specialist supervision
62
Not to be reproduced or copied without permission from Kidney Health Australia
Case study - Jim
For Jim’s breathlessness and possibly sleep…
Lorazepam was used
- Elimination is renal (88%) and faecal (7%)
- If eGFR <10ml/min/1.73m2 or dialysis begin with low end of dose range and titrate
according to response
- CNS adverse effects more pronounced in patients with renal impairment
- Minimal commencing dose - 0.5 mg-1mg bd (sublingual or oral)
- Alternatives small dose of hydromorphone 0.25-0.5mg qid
Note: For terminal secretions Glycopyrrolate 0.4mg-0.8mg SL Q 1-2 hourly

63
Not to be reproduced or copied without permission from Kidney Health Australia
Dyspnoea• Approaches 80% in final days
• Effectively controlled in <50% in cases
• Multifactorial – may include cardiac disease, respiratory disease, fluid overload, anaemia
• Pneumonia is a common final event
• Treatment requires urgency:
- often rapid progression
- severe distress
- often only hours before dying

64
Not to be reproduced or copied without permission from Kidney Health Australia
Management of dyspnoea
Non-
pharmacological
Pharmacological Pharmacological detail
• Calm
reassurance
• Fan
• Sitting upright
• Open window
• Oxygen
• Sedatives
• Opioids
• Antisecretory
agents
• Conscious (lorazepam 0.5mg
SL bd)
• Unconscious (midazolam)
• Commence with small doses
of hydromorphone 0.25-
0.5mg qid & carefully titrate to
response
• Scopolamine, glycopyrrolate

65
Not to be reproduced or copied without permission from Kidney Health Australia
Case study - Jim
The rate at which Jim’s kidney function has declined allows a
rough prediction kidney function is likely not to survive longer
than a year.
15
20
10
5
30
0 1 3 542
Predicted decline of GFReGFR
Months

66
Not to be reproduced or copied without permission from Kidney Health Australia
Jim’s chosen treatment pathway
requires end of life planning.
For Jim’s follow up
appointments, what are your
next considerations?
a) Advance care planning
b) End of life planning
c) Kidney function preservation
d) Symptom management
e) Quality of life
Question:

67
Not to be reproduced or copied without permission from Kidney Health Australia
Advance care planning
Advance care planning should be already in place for…
i. all competent patients aged 65 years and above, and
ii. all competent patients, irrespective of age, who fulfil one or more of
the following criteria:
• The Nephrologist would not be surprised if the patient were to die in the next 12
months
• Two or more significant co-morbidities
• Poor functional status
• Chronic malnutrition
• Poor quality of life
68
Not to be reproduced or copied without permission from Kidney Health Australia
Recommendations
1. Discussions should include the patient’s family
2. Content of discussion and documentation should include:
• Nature of Kidney Failure, prognosis and quality of life
• Selecting a substitute decision maker
• Exploring expectations, goals of care and values
• An indication as to what circumstances the patient would wish that dialysis & all other active
treatment cease & a purely palliative approach commence. This process may continue over many
conversations
3. Should be documented and universally available to relevant parties
It is both advisable and appropriate to initiate ACP with a Kidney Failure patient

69
Not to be reproduced or copied without permission from Kidney Health Australia
Dying with dignity: What patients want
Meanings of dying with dignity from perspective of patients, families & health professionals
Guo & Jacelon Palliative Medicine 2014
Themes Patients Health Professionals Families
A human right ✓ ✓
Autonomy and independence ✓ ✓ ✓
Relieved symptom distress ✓ ✓ ✓
Respect ✓ ✓ ✓
Being human and being self ✓ ✓ ✓
Meaningful relationships ✓ ✓ ✓
Dignified treatment and care ✓ ✓ ✓
Existential and spiritual satisfaction ✓ ✓
Privacy ✓ ✓
Safe and calm environment ✓
70
Not to be reproduced or copied without permission from Kidney Health Australia
Terminal phase care: how to ensure comfort
• Communication
• Anticipating symptoms, proactive response
- Pain (generally only if a pre-existing problem)
- Nausea
- Restlessness, confusion
- Dyspnoea – fluid balance, pneumonia
- Pruritus
- Myoclonus, twitching
• Communication
• Anticipating need for non-oral medication routes
• Communication

71
Not to be reproduced or copied without permission from Kidney Health Australia
Delirium in terminal phase care
• Common: 80 – 90% in last few weeks
• Almost always multifactorial; illness, medications
• May rapidly worsen, with paranoia and agitation
• Very distressing for all involved
• Not likely to be reversible in last few days of life, such as after withdrawing from dialysis (this is d/t uraemic encephalopathy)
• Main intervention is effective sedation
• If conscious – haloperidol – 1mg bd sci and 1-2mg prn
• If unconscious - midazolam – Subcutaneous route 2.5 mg - 5 mg q 4 hours ; about 1/3 as potent as IV route but IV is complicated and impractical in reality

72
Not to be reproduced or copied without permission from Kidney Health Australia
Communication in terminal phase care:issues regarding sedation for delirium
• Delirium not reversible; ongoing physiologic decline
• Once effectively sedated, will not likely awaken again
• Medications not hastening process, but ensuring
comfort
• Encourage ongoing communication by family, including
private time alone with patient
• Be cautious in presenting “non-choices” as choices…
there are no other realistic options but sedation in trying
to settle a restless, agitated, delirious person who is
imminently dying

73
Not to be reproduced or copied without permission from Kidney Health Australia
Key points
• Treatment decision making process is ongoing
• Need to respect individual “informed” decisions
• Tools are available to help decision-making process
• Well managed comprehensive conservative care is an attractive
option particularly when co-morbidities present
• GPs play an important role in symptom management
• Communication critical to ensuring comfort in terminal phase

74
Not to be reproduced or copied without permission from Kidney Health Australia
Patient resources
Kidney HelplineFree call information service
Contact 1800 454 363
Kidney Health Australia Resource Hub
Kidney.org.auFactsheets, books & videos

75
Not to be reproduced or copied without permission from Kidney Health Australia
Kidney failure patient resources
An introduction to series of books includes:Kidney Disease Treatment Options
Peritoneal Dialysis
Haemodialysis
Home Dialysis
Kidney Transplantation
Live Kidney Donation
Living with Kidney
FailurePatient information
booklets, fact sheets,
App, Kidney Helpline,
and more
www.kidney.org.au/resources
My Kidneys, My ChoiceContains a check list of issues to consider
kidney.org.au/your-kidneys/treatment/my-kidneys-my-choice

76
Not to be reproduced or copied without permission from Kidney Health Australia
How can I get the 4th edition handbook?
Download a free digital copy at
www.kidney.org.au/health-
professionals
Buy a hardcopy ($15) from
www.kidney.org.au/shop
CKD-GO! App
can be downloaded for FREE on the
iPhone & Android app stores

77
Not to be reproduced or copied without permission from Kidney Health Australia
Want to learn more about CKD?
1. Go to kidney.org.au/health-professionals/webinars
for interactive webinars & recordings
2. Complete our free online
learning available at
www.thinkgp.com.au/KHA