Embed Size (px)
Citation preview

Dealing with weight regain after Roux-en-Y gastric bypass: surgical approach
Robin Blackstone, MD, FACS
Masters of Minimally Invasive Bariatric Surgery
April 5, 2013 Orlando, Florida

Disclosures
• PI Enteromedics VBLOC and Recharge Trials
• Consulting Johnson and Johnson/Ethicon Surgical

Changing Semantics
• Remission of weight
• Partial Remission of weight
• Weight regain
• ELIMINATE THE WORD FAILURE….

Weight Loss after RYGB is Widely
and Normally Distributed
10
0%
5 65 140
% Excess Body Weight Loss at 1 year
Nu
mb
er
of P
atie
nts
5
75
150
n=682
50
%
Hatoum IJ et al. Obesity 2009; 17(1):98-9.
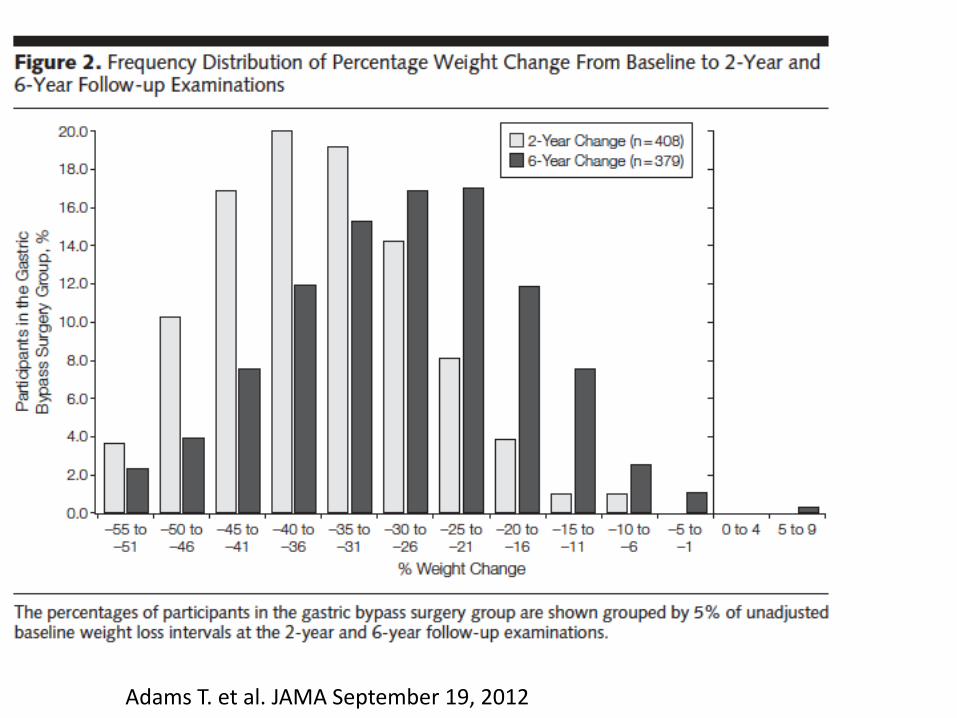
Adams T. et al. JAMA September 19, 2012

Bariatric Surgery
Evidence for Physiological Mechanisms
1. Dramatic effects on hunger and satiety
2. Few patients become underweight after surgery
3. Transient weight gain during pregnancy
4. Little or no weight loss in thin patients or animals
5. Changes in GI endocrine markers – ghrelin, PYY, GLP-1, amylin
6. Increased energy expenditure (bypass procedures)
7. Ability to reverse effects of surgery with drugs and genetic
manipulation

Anatomic Dissection of RYGB

Gastric Bypass: Five Operations
5. Partial vagotomy

Gastric Bypass: Five Operations
1. Isolation of gastric cardia

Gastric Bypass: Five Operations
2. Exclusion of distal stomach
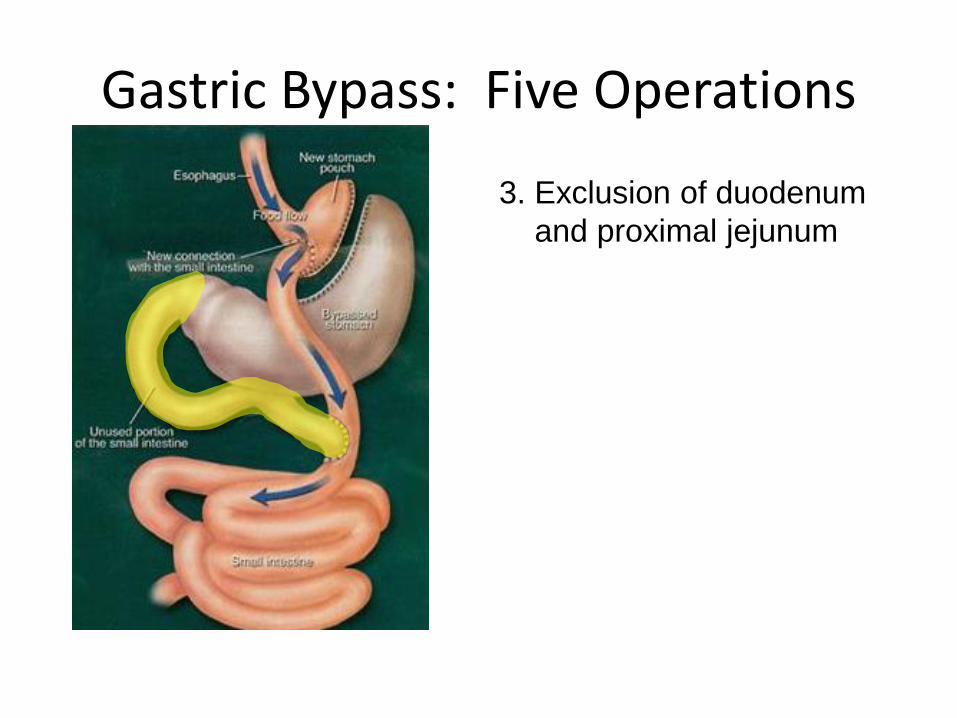
Gastric Bypass: Five Operations
3. Exclusion of duodenum
and proximal jejunum
4
3
ELS
10 cm

Gastric Bypass: Five Operations
4. Exposure of distal intestine
to undigested nutrients

Altering the “Set Point” with Gastric
Surgery
30 35 40 45
Body Mass Index (kg/m2)
kcal / 24
ho
urs
2000
2500
3000
Baseline
Energy
Expenditure
Baseline
Energy
Intake
Post-op
Energy
Intake
Post-op
Energy
Expenditure

RYGB: Resolution of the “Overfed”
State
30 35 40 45
Body Mass Index (kg/m2)
kcal / 24
ho
urs
2000
2500
3000 Post-op
Energy
Intake
Post-op
Energy
Expenditure
Overfed state

RYGB Mimics the Overfed State
0 25 50 75 100 125 150 175 200200
250
300
350Overfed
Control
Food Restricted
Days
Bo
dy W
eig
ht
(g)
Resolution of the overfed state

RYGB Mimics the Overfed State
0 25 50 75 100 125 150 175 200200
250
300
350Overfed
Control
Food Restricted
Days
Bo
dy W
eig
ht
(g)
Resolution of the overfed state
OLD model
of RYGB
CURRENT model
of RYGB

Set Point and Weight Regain F
at M
ass S
et P
oin
t
Time (years)
Aging and environmental influences (no intervention)
Surgery Environmental influences
and aging

RYGB Induces Weight Loss in Mice
40
60
80
100
120
0 1 2 3 4 5 6 7 8 9 10 11
Time after Surgery (Weeks)
% P
reo
pera
tive B
od
y W
eig
ht
Sham
RYGB
Stylopoulos N et al. Obesity 2009; 17(10):1839-1847.

0
2000
4000
6000
8000
10000
12000
14000
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
Time (Weeks)
RYGB
Sham
RYGB Reduces Nutrient Intake
Cu
mu
lati
ve F
oo
d I
nta
ke
(kcal)
Stylopoulos N et al. Obesity 2009; 17(10):1839-1847.
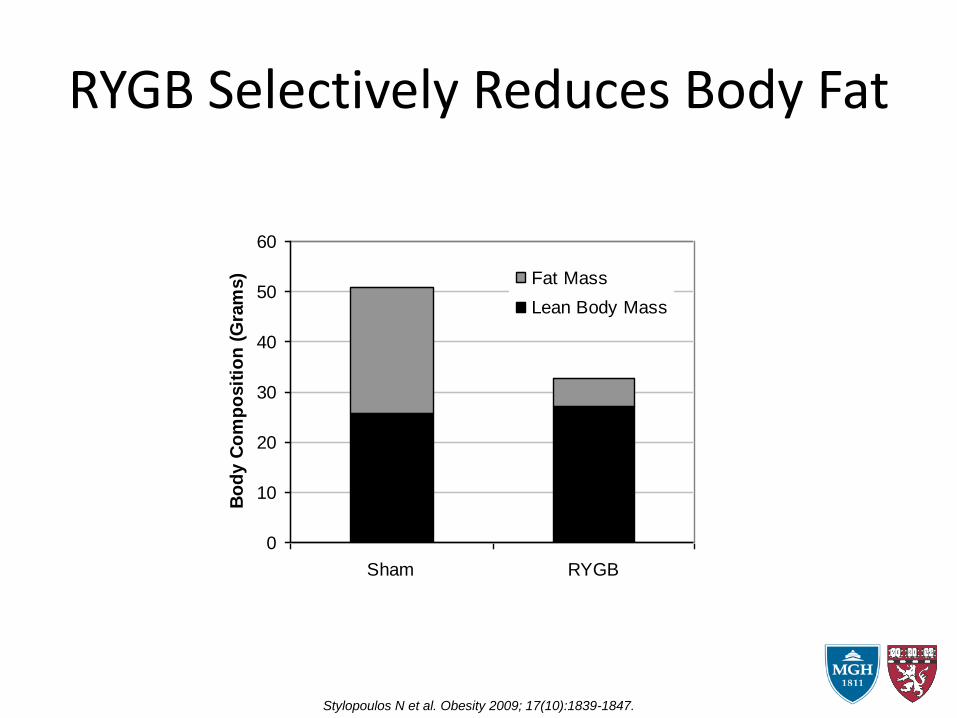
RYGB Selectively Reduces Body Fat
0
10
20
30
40
50
60
Sham RYGB
Bo
dy C
om
po
sit
ion
(G
ram
s) Fat Mass
Lean Body Mass
Stylopoulos N et al. Obesity 2009; 17(10):1839-1847.

Nutr
ient A
bsorp
tion
(%)
Before
RYGB
After
RYGB
Stool Calorimetry
RYGB Does Not Alter Caloric
Absorption
Stylopoulos N et al. Obesity 2009; 17(10):1839-1847.

RYGB Increases Energy Expenditure
400
500
600
700
800
900
1000
1100
1200
400
450
500
550
600
650
700
750
800
850
900
TE
E -
VO
2 (
ml/hr/
kg
.75)
RE
E -
VO
2 (
ml/hr/
kg
.75)
Sham RYGB Weight-matched * p<0.05
** p<0.001
** ** *
** ** *
Stylopoulos N et al. Obesity 2009; 17(10):1839-1847.

GI Endocrine Responses to RYGB
Time after start of meal (min)
0 20 40 60 80 100
Active G
LP
-1 (
pg/m
l)
0
50
100
150
200
250
300RYGB
Sham
Lean
5 min mixed meal
-10
*
#
*
**
Time after start of meal (min)
0 20 40 60 80 100P
YY
(p
g/m
l)
0
50
100
150
200
250
300RYGB
Sham
Lean
5 min mixed meal
-10
*
**
**
**
Time after start of meal (min)
0 20 40 60 80 100P
YY
(p
g/m
l)
0
50
100
150
200
250
300RYGB
Sham
Lean
5 min mixed meal
-10
*
**
**
**
Time after start of meal (min)
0 20 40 60 80 100
GIP
(p
g/m
l)
0
100
200
300
400
500
600
5 min mixed meal
-10
Time after start of meal (min)
0 20 40 60 80 100
Active
Am
ylin
(p
g/m
l)
0
50
100
150
200
250
5 min mixed meal
-10
*
*
Time after start of meal (min)
0 20 40 60 80 100
Acyl
ate
d G
hre
lin (
pg
/ml)
0
50
100
150
200
250
300 RYGB
Sham
Lean
5 min mixed meal
-10
**
GLP-1 PYY Amylin
Ghrelin GIP
Shin AC et al. Endocrinology 2010; 151(4):1588-1597.

GLP-1 levels in human after RYGB
Peterli R et al. Ann Surg 2009; 250(2):234-41.
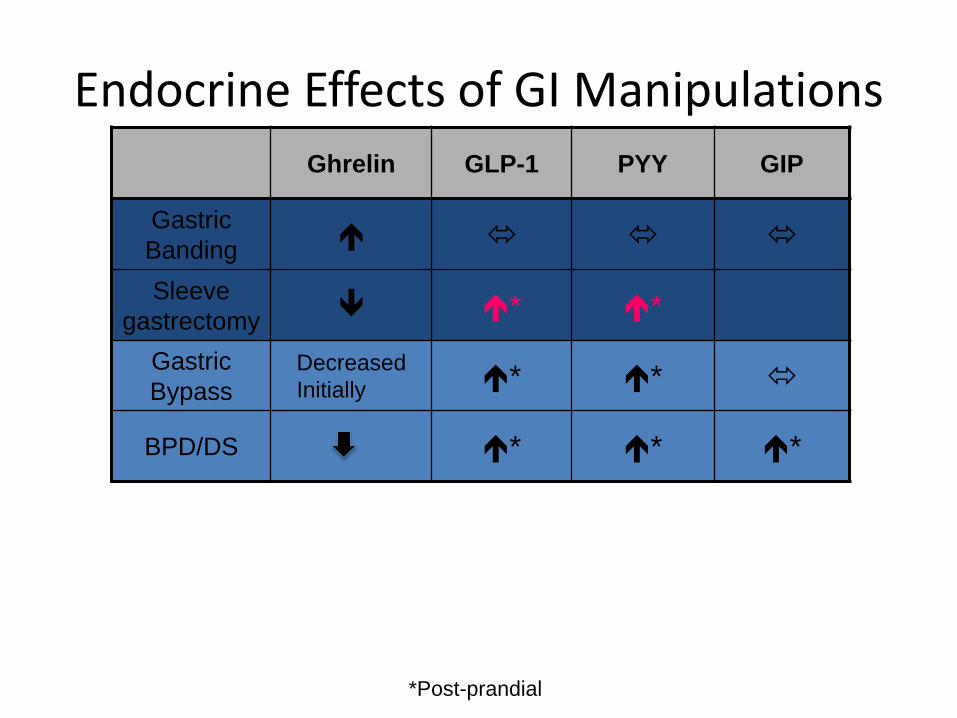
Endocrine Effects of GI Manipulations Ghrelin GLP-1 PYY GIP
Gastric
Banding
Sleeve
gastrectomy * *
Gastric
Bypass
Decreased
Initially * *
BPD/DS * * *
*Post-prandial

Clinical Predictors of RYGB Weight
Loss
• Increased preoperative BMI
• Presence of T2DM
– Duration of T2DM
– ? Relationship with b-cell failure
• Lack of physical activity
• Increased patient age
• Inadequate surgical “restriction”
– Pouch size
– Diameter of gastro-jejunal anastomosis
• Lack of patient follow-up / compliance
• None of these predictors is sufficiently
powerful to determine clinical practice
Associations with more modest weight loss

Carbohydrate eating leads to weight regain
• When a post GBP patient eats any simple sugar (carbohydrates: rice, pasta, bread, potatoes) then evoke a very strong GLP1 response
• The GLP1 drives the release of insulin which outlasts the simple sugar in the blood causing a relative low blood sugar which drives eating
• This occurs over and over all day with subsequent weight regain

Intensive Medical/Behavioral Therapy
• STOP eating any carbs except in green vegetables
• Need to increase energy expenditure and drive body fat percent below 30% in order to reengage the LEPTIN coupling with metabolism (good evidence for Leptin resistance at Body Fat >30%)
• Get the original set of parameters to work for the patient

So what is there to revise?
• Possible options:
– Revise the gastrojejunostomy
– Take out the distal remnant (decrease ghrelin)
– Lengthen the Roux limb
– Convert to Sleeve/ Duodenal switch

THANK YOU





























