Embed Size (px)
Citation preview

© 2015
Wou
nd C
are P
eople
Ltd
SKIN CARE
JCN 2015, Vol 29, No 6 53
Skin cancer can affect people at any age, however the majority of skin cancers develop in
older people (Farage et al, 2008; Johnson and Taylor, 2012), with the incidence of malignant melanoma being 10 times that of younger people (Lasithiotakis et al, 2010). It can be difficult for community nurses to identify dangerous skin lesions as many people have a certain amount of benign lesions that make identification difficult (Lasithiotakis et al, 2010).
The higher risk in older adults is partly due to immunosenescence (the gradual deterioration of the immune system over time) (Sachs et al, 2001), as well as risk factors that accumulate throughout a lifetime, such as exposure to the sun and ultraviolet (UV) radiation that damages cells. It is also harder to identify malignant skin lesions in older people as their skin in general is changing through age and chronic disease, such as diabetes, heart failure, chronic obstructive pulmonary disease (COPD) etc, which all have a detrimental effect on the skin’s integrity (Lasithiotakis et al, 2010).
Dealing with common skin lesions in older people
Annette Aldridge
CAUSES
Long-term cell damage and mutations from ultraviolet (UV) radiation increase the likelihood of pigment changes in the skin as well as skin cancers such as malignant melanoma, basal cell carcinoma, squamous cell carcinoma, and actinic keratoses (see below for explanations of different skin cancers) (Baldry et al, 2006).
There are various types of skin cancer, but the two most common types are basal cell carcinoma and squamous cell carcinoma (known as non-melanoma skin cancer). Malignant melanoma is rarer but needs to be treated as early as possible because it can grow quickly and metastasise (spread to other tissues), making it the most dangerous form of skin cancer.
Working outdoors, sunbathing (including tanning beds), severe burns and smoking all increase skin cancer risk (Johnson and Taylor, 2012).
In some people with conditions that affect the immune system (such as human immunodeficiency virus [HIV], human papilloma virus [HPV]; organ transplantation), skin cancer risk is even greater.
COMMON SKIN LESIONS
Some of the most common skin lesions include: Seborrhoeic keratosis: very
common and harmless skin lesions or ‘warts’ with an unknown aetiology (Balin, 2015). Seborrhoeic keratoses are the most common benign tumours in older people and have a varying degree of pigmentation. They rarely become malignant
Actinic keratoses: cell damage from UV rays causes keratoses or ‘scaly’, crusty elevated lesions that are rough in texture and resemble warts. Affects areas of the body that are commonly exposed to the sun such as the face, scalp, back of the hands
Basal cell carcinoma: cancer that develops in the basal cell layer of the epidermis (outer layer of the skin). Again, due to exposure to UV light, is commonly located on the face and neck. Basal cell carcinoma results in open sores, red patches, pink growths, shiny bumps, or scars. There are many sub-types including nodular basal cell carcinoma, superficial basal cell carcinoma and mor-phoeic basal cell carcinoma, all of which have different presentations
Bowen’s disease: also known as squamous cell carcinoma in situ and is an easily curable early form of skin cancer that develops in the squamous cells (‘flat’ cells forming outer layers of the epidermis). The main sign is a red, scaly patch on the skin
Squamous cell carcinoma: common type of keratinocytic or non-melanoma skin cancer that develops in the squamous cells. Squamous cell carcinoma can invade the deeper layers of the skin and in rare cases can
Annette Aldridge, lead nurse, dermatology, Royal Free London NHS Foundation Trust
This article will highlight some common skin lesions present in the older population. Skin lesions of this type may be frequently seen by community nurses and can be categorised as benign lesions, non-melanoma and melanoma skin cancers. The article contains a description of the lesions along with a guide to the correct terminology used to establish an accurate diagnosis. The prevalence and causes of these lesions along with an explanation of varying treatment options is also included.
KEYWORDS:Basal cell carcinoma Squamous cell carcinoma Malignant melanoma

© 2015
Wou
nd C
are P
eople
Ltd
54 JCN 2015, Vol 29, No 6
SKIN CARE
metastasise and prove fatal Malignant melanoma: develops
from the pigment-containing cells known as melanocytes. The most common sign is the appearance of a new naevus (more commonly known as moles) or a change in an existing one. Malignant melanomas are often irregular in shape and may itch or bleed.
ASSESSMENT
Community nurses should always consider referring larger lesions (over 6mm), those that have indistinct outlines, or those that occur
form and structure of organisms) characteristics are key and there are two important elements for the community nurse: Careful tactile and visual
examination of the lesion Correct use of dermatological
terminology.
A full description should identify the following six features: Size Colour and pigmentation Texture (rough; smooth) Shape and symmetry Location (extensor surfaces;
flexor surfaces) Type (palpability indicated
by shadow).
The type of skin lesion can be subdivided into primary and secondary. The primary lesion (Table 1) is due to damage by disease or trauma and the secondary lesion (Table 2) arises as a consequence of the primary lesion. For example, a burst bulla or blister — the primary lesion — will form a crust or scab — the secondary lesion. The shape, configuration and distribution (Tables 3 and 4) will all help to achieve a full picture of the lesion.
PRESENTATION OF SKIN LESIONS
Seborrhoeic keratosis (basal cell papilloma)Seborrhoeic keratosis lesions (Figure 1
repeatedly, to a dermatology or skin cancer specialist. A dermatology specialist may recommend a biopsy, which is the best way to determine the type of lesion the patient has as well as its extent (Johnson and Taylor, 2012). An excisional biopsy should always be performed if a melanoma is suspected.
IDENTIFYING SKIN LESIONS
Using the correct terminology to describe a skin lesion is crucial to accurate diagnosis. The morphologic (morphology is a branch of biology dealing with the study of the
Table 1: Primary lesions
Macule A flat non-palpable lesion, with an area of colour change that measures less than 5mm. They can be well- or ill-defined
Patch A flat non-palpable lesion, with an area of colour change that measures over 5mm. They may have some subtle surface changes such as wrinkling or fine scale but the surface is unchanged
Papule A circumscribed palpable lesion caused by a proliferation of cells in the epidermis or superficial dermis that measures less than 5mm
Plaque A palpable lesion caused by proliferation of cells in the epidermis or superficial dermis that measures over 5mm
Vesicle A circumscribed fluid-filled lesion with a diameter less than 5mm
Bulla A fluid-filled lesion containing serous or seropurulent fluid with a diameter over 5mm
Nodule A palpable lesion caused by a proliferation of cells into the mid-deep dermis with a diameter over 5mm
Cyst An epithelial-lined cavity containing liquid, semi-solid or sold material
Wheal A rounded or flat-topped swelling in the upper dermis that has a red halo or flare and disappears within 24–48 hours
PurpuraRed/purple lesions caused by extravasation of blood into the skin or mucous membrane that may be palpable or non-palpable. Small lesions (less than 3mm) are called petechiae. Lesions over 5mm are called ecchymoses
Table 2: Secondary lesions
Scales Produced by abnormal keratinisation of the epidermal cells that have died and shed
Lichenification The thickening of the epidermis commonly caused by scratching
Pustule A small elevated fluid-filled lesion containing neutrophils — can be red or white
Crust A dried collection of serum and cellular exudate
Fissure A linear discontinuation of epithelial lining with a sharply demarcated margin that can extend into the dermis
Erosion The incomplete loss of the epidermis. The lesion is moist, circumscribed and usually depressed
Ulcer The complete loss of the epidermis in addition to part of the dermis and even some subcutaneous fat
Scar
Contains fibrous tissue and results from the biological process of wound healing. Hypertrophic scars take the form of a red raised lesion on the skin within the confines of the original wound area. Keloid scars are a form of excessive scarring and can grow indefinitely into large tumourous neoplasms. Striae scarring is caused when the skin is stretched rapidly, such as in significant weight gain
AtrophyLoss of tissue, which can be epidermal, dermal or subcutaneous. With epidermal atrophy the skin appears thin, translucent and wrinkled. Dermal or subcutaneous atrophy results in depression of the skin
Table 3: Distribution
Generalised All over
Symmetric One side mirrors the other
Flexural Inside of joints
Extensor Outside of joints
Intertriginous In an area where two skin areas touch or rub together
Morbilliform Resembling measles
Palmoplantar On the palm or sole
Periorificial Around an orifice
Periungual Under a finger or toenail
Blaschkoid
Following the path of Blaschko’s lines (lines of normal cell development in the skin)
Photo-distributed Areas exposed to sunlight
Dermatomal Associated with a particular nerve

© 2015
Wou
nd C
are P
eople
Ltd
Solutions with you in mind
Warnings and precautions: For topical use only. Do not use on broken or infl amed skin. Caution should be exercised with concomitant treatment with other medicated topical products. If the condition becomes worse or if patients experience side effects/adverse incidents, discontinue treatment with Balneum Cream and seek medical advice.
Adverse incidents: Although very few adverse incidents have been reported, the most frequent are local skin reactions.
Special precautions for storage: Do not store above 25°C. Use within 6 months of fi rst opening.
Pack sizes: Available in 50g (£2.85) and 500g (£9.97) pump dispensers.
CE marking held by: Almirall Hermal GmbH, Scholtzstraße 3, 21465 Reinbek, Germany.
Distributed in the UK by: Almirall Ltd, 1 The Square, Stockley Park, Uxbridge, UB11 1TD.
Date information last revised: 02/2015.
Item code: UKSOY3039.
Adverse incidents should be reported. Online reporting forms and information can be found at
www.mhra.gov.uk/yellowcard. Adverse incidents should also be reported to Almirall Ltd.
PRODUCT INFORMATION
Name of the Class I Medical Device: Balneum Cream
Ingredients: Urea 5 %, Ceramide NP, Aqua, Glycine Soya Oil, Propylene Glycol, Cetearyl Alcohol, Liquid Paraffi n, Isohexadecane, Sodium Lactate, Lactic Acid, PEG-20 Stearate, Polysorbate 60, Squalane, Stearic Acid, Disodium EDTA, Lecithin, Tocopherol, Ascorbyl Palmitate, Hydrogenated Palm Glycerides Citrate. Balneum Cream is free of fragrances, colourants and preservatives.
Pharmaceutical form: White cream.
Indications: Balneum Cream is formulated to protect the skin, to maintain skin moisture and to restore the impaired skin barrier in conditions giving rise to dry skin. It contains urea, ceramide NP and physiological lipids. Urea is known to increase the skins ability to retain water and maintain skin hydration. Ceramide NP is known to help restore the barrier function of skin. Balneum Cream is designed for daily use to relieve dry and very dry skin conditions including eczema, psoriasis and other dermatological conditions.
Method of administration: Using clean hands, apply the cream to the skin once or twice daily.
Contraindications: Patients with known hypersensitivity to any of the ingredients, soya or peanut.
REHYDRATES AND RESTORES AGED SKIN
References1. Brown K, et al. The effect of an emollient cream containing 5% urea on the biophysical properties of aged skin. Poster presented at 11th meeting: European Epidermal Barrier Research Network and COST Action BM 0903 Skin Barrier in Atopic Disease Scotland. May 8th 2013. 2. Almirall Data on File BAL01.
Date of preparation: A
ugust 2015 Item num
ber: U
KSO
Y3305
There are easier things to...
Urea 5% and ceramide NP
ONCE-DAILY USE CAN PROVIDE 24 HOURS SKIN HYDRATION.1,2
I M P R OV E S S K I N B A R R I E R FUNCTION & SKIN INTEGRITY.1
ONCE-DAILY HAS THE POTENTIAL TO REDUCE THE BURDEN ON RESOURCES.

© 2015
Wou
nd C
are P
eople
Ltd
SKIN CARE
56 JCN 2015, Vol 29, No 6
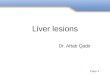
a–c) are very common harmless skin lesions that are most common on the face and trunk, with the sexes equally affected (Balin, 2015). Seborrhoeic keratosis usually develops after the age of 50, but flat inconspicuous lesions are often visible earlier. The exact cause of seborrhoeic keratosis is not known, however the name is misleading as the lesions do not follow a seborrhoeic distribution (scalp, face, chest and upper back), nor do they originate from the sebaceous glands.
Seborrhoeic keratosis lesions have a distinctive ‘stuck-on’ appearance (Figure 1) as they grow ‘outwards’ (epidermal
proliferation), rather than infiltrating down into the epidermis. They may be flat, raised or pedunculated (attached by a peduncle, or small ‘stalk’). The colour varies from yellow to dark brown and colour variation between multiple lesions is common as is ‘speckling’ within a single lesion — this is due to incidental melanocytic activity within the lesion.
The surface of seborrhoeic keratosis lesions may have greasy scaling and scattered keratin plugs. The margin is usually fairly sharply defined and often ovoid in shape.
These lesions are more common in white skin and can vary in size from a few millimetres in diameter to 2–3cm. They can be itchy and become inflamed when irritated or scratched (Schofield and Kneebone, 2006). They are particularly problematic under the elastic bands of trousers and underwear, for example. As these benign lesions are common and asymptomatic, no treatment is required. However, for those people who would like them removed, they can be treated with either cryotherapy (local or general use of low temperatures) or curette and cautery (electrosurgery).
Actinic keratosisActinic keratosis is a global
condition and its prevalence rates are highest in countries that have high sun exposure and a large fair-skinned population. In the UK, 19–24% of individuals over 60 years have at least one actinic keratosis (de Berker et al, 2007). Actinic keratosis is a premalignant, keratinocytic neoplasm (new and abnormal growth of tissue) induced by cumulative exposure to solar radiation (Figure 2 a–c). The lesions present as scaly, crusting erythematous lesions seen most often on the photo-distributed skin of light-skinned individuals who have an outdoor occupation or an excess of recreational sun exposure.
The lesions usually measure 2–30mm and come in a variety of colours (from yellow, pink, and white to red), comprising rough papules that are sometimes more noticeable through palpation than visualisation. They may appear as solitary lesions or in a cluster.
In patients with severe photodamage, actinic keratosis lesions tend to flow together to create what is known as ‘field change’ (see Figure 2c), which involves a whole area of skin — such as the scalp in balding men or the shins in women who have historically worn skirts — developing multiple actinic keratoses with a background of erythema (redness). Due to these lesions being caused by cumulative photodamage, actinic keratosis is rarely seen in individuals under 30 years of age (Spencer, 2015).
Treatment options include cryotherapy, curette and cautery, 5-fluorouracil (a strong topical medication) or photodynamic therapy (uses a drug, called a
Table 4: Configuration
Agminate In clusters
Annular Ring-shaped
Arciform Bow-shaped
Digitate With finger-like projections
Discoid Round or disc-shaped
Figurate Having a definite or particular shape or figure
Guttate Drop-like
Gyrate Spiral-shaped
Herpetiform Resembling herpes
Invagination Turned inward
Linear In a line
Mamillated Rounded, breast-like projections
Peduncle Elongated ‘stalk’ of tissue
Pedunculated Supported by a peduncle
Reticular Resembling a net
Serpignous With a wavy border
Stellate Star-shaped
Targetoid Resembling a darts bullseye
Verrucous Wart-like
Figure 1 a–c.Examples of different presentations of seborrhoeic keratosis lesions.
a: Keratin plugs b: Greasy, ‘stuck on’ c: Irritated
Figure 2 a–c.Examples of different presentations of actinic keratosis.
a: Mild scale b: Hyperkeratotic c: Field change

© 2015
Wou
nd C
are P
eople
Ltd
JCN 2015, Vol 29, No 6 57
SKIN CARE
Premalignant fibroepithelioma (tumour that mostly occurs on the lower trunk of older people).
Noduloulcerative basal cell carcinoma is the most common form of basal cell carcinoma and presents as solitary lesions that have been non-healing for several months. Although the majority are asymptomatic, they have a tendency to bleed and pruritus (severe itching) is not uncommon. Noduloulcerative lesions begin as translucent papules that have a ‘pearly’ appearance and have telangiectasia (dilated capillaries) running through them. These features are more easily visualised if the skin is stretched. Left untreated, the noduloulcerative basal cell carcinoma will enlarge and ulcerate, exhibiting a central crater. Crusting may occur and the lesion will develop into an erosion or ulcer with a pearly rolled margin.
Treatment options for noduloulcerative basal cell carcinomas include excision, Mohs surgery (microscopically controlled surgery) in difficult or recurrent cases, and radiotherapy for larger lesions or those in an awkward area.
Squamous cell carcinomaThese are the second most common UK skin cancer (BAD, 2012b) (Figure 5 a–c). Unlike basal cell carcinomas, squamous cell carcinomas can metastasise. Squamous cell carcinomas arise from the stratified epithelium and can be located anywhere on the skin, as well as the mucous membranes where there is a higher potential for metastasis (Veness, 2001).
This type of skin cancer often develops from a preceding actinic
while they attack the skin and other tissues such as cartilage (most commonly in the nose and ears) and bone (most commonly on the scalp), they do not spread to internal organs (Figure 4 a–c). Basal cell carcinomas are slow-growing, locally destructive tumours, thought to arise from a subset of the basal cells in the epidermis (Mackie, 2003).
The most common presentation is on photo-distributed areas such as the face, head, neck and — in men who work outside — the trunk. However, any area of the body can be involved.
Basal cell carcinomas are the most common form of cancer, accounting for 80% of all skin cancers in the UK (British Association of Dermatologists [BAD], 2012a). There are six clinical variants of basal cell carcinomas (Arndt et al, 1997): Noduloulcerative (nodular
in appearance) Superficial (resemble a scaly red
flat mark) Pigmented (black and
brown lesions) Morpheaform (insidious
tumour with innocuous surface characteristics masking potential for widespread extension)
Metatypical (has the capacity to spread and develop metastasis)
photosensitiser or photosensitising agent, and a particular type of light to destroy cells), especially if there is field change (see ‘treatments’ section, below).
Bowen’s diseaseBowen’s disease (also known as squamous cell carcinoma in situ) is an early form of skin cancer, which is easily curable (Figure 3 a–c). It usually affects middle-aged and older people, occurring commonly on the limbs and trunk. The associated lesions demonstrate full-thickness dysplasia (enlargement of an organ through proliferation of abnormal cells) of the epidermis without invasion of the deeper dermis. They are usually slowly enlarging well-defined erythematous macules associated with minimal induration (increase in the fibrous elements in tissue) and slight scaling and can be easily misdiagnosed as psoriasis, eczema or fungal infection (Kaldas, 2014). However, unlike eczema and psoriasis, Bowen’s disease usually presents as a solitary lesion.
Bowen’s disease was reported to follow exposure to sheep dip or the ingestion of arsenic that was found in certain tonics and foods up until the mid-20th century (Reed, 1998).
Treatment includes photodynamic therapy, cryotherapy, and curette and cautery, however caution should be taken when administering either cryotherapy or curette and cautery to the lower legs, as this area is slow to heal in the elderly and may precipitate a leg ulcer (Ahmed et al, 2000).
Basal cell carcinomas By definition, basal cell carcinomas (sometimes known as ‘rodent ulcers’)are malignant tumours, however
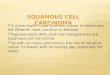
Figure 3 a–c.Examples of different presentations of Bowen’s disease.
a: Erythematous b: Scaling c: Prepared for photodynamic therapy
Figure 4 a–c.Different presentations of noduloulcerative basal cell carcinoma.
a: Overlying telangiectasia (dilated capillaries)
b: Rolled margin, central crater
c: Ulcerated

© 2015
Wou
nd C
are P
eople
Ltd
SKIN CARE
58 JCN 2015, Vol 29, No 6
keratosis or an area of Bowen’s disease. Those arising from actinic keratosis rarely metastasise, but those arising from scars, ulcers, sinus tracks, irradiated skin and mucous membranes often do.
The most common sites are on photo-distributed areas while patients often report that the lesion appeared after they were scratched while gardening. Squamous cell carcinomas may also complicate chronic vascular leg ulcers that are in a state of stasis — something to consider if a venous ulcer under compression bandaging is not showing signs of improvement after six weeks (Poyner, 2005).
Squamous cell carcinomas can vary in their appearance but usually the first noticeable change is a thickening of the skin with scaling or hyperkeratosis (thickening of the skin’s surface). More differentiated tumours often have a ‘warty’, keratotic crust, whereas others may be nodular. The edges of the lesion will be poorly defined and there may be dilated telangiectatic blood vessels. Eventually, the original hard, nodular discoid lesion will become ulcerated with a ‘juicy’ appearance.
Treatment options include excision, curette and cautery for very
small, thin tumours; Mohs surgery for difficult or recurring lesions; and radiotherapy if the lesion is large or in an awkward place. Chemotherapy is used only if the lesion has spread to other organs.
Malignant melanomaMelanoma is considered the most serious type of skin cancer as it involves an invasive malignant tumour (Figure 6 a–c). In the UK, there is a staging system used to indicate the most likely outcome and the best treatment options. There are four stages, with stage 1 having the best prognosis and stage 4 the poorest (BAD, 2012c).
Melanomas can arise from a pre-existing naevus as well as presenting at a completely new site. There are four main types of melanoma: Superficial spreading: the most
common variety, predominately developing on men’s backs and women’s legs
Lentigo maligna melanoma: classically develops in photo-distributed areas of the body in older people
Acral lentiginous melanoma: occurs on the palmoplantar aspects (soles of the feet and palms of the hands) and also near or under the nails
Nodular melanoma: this has a poor prognosis because of the vertical invasive growth and is more common in men than women, usually occurring in those over 50 years old.
The sign of a healthy naevus is a symmetrical lesion with a well-defined border, which is the same colour throughout, has a diameter that is smaller than 7mm and has not changed. As naevi usually present as a different colour to the surrounding skin, the acronym ABCDE is used to assess pigmented lesions. Should one of these markers not meet the definition of a healthy naevus, referral to a dermatologist should be sought: Asymmetry: is the pigmented
lesion asymmetrical? If a mirror is placed through the centre of the lesion do both sides mirror each other? If not, this is an asymmetrical lesion
Border: is the border of the lesion well-defined? Can the edge of the lesion be marked with a pen? If there are ‘feathered’ or ‘jagged’ edges the border is affected
Colour: is the colour of the lesion uniform or multicoloured? Colours vary from brown, blue, grey, black, red with possibly a white veil through the centre
Diameter: is the pigmented lesion less than 7mm in diameter? Can a rubber from the end of a pencil be placed over the lesion? Does the lesion protrude from the side of the rubber?
Evolving/enlarging: does the lesion have a history of changing? Does it itch? Has it bled? Has it grown?
Excision is the main treatment option for malignant melanoma, although depending on the stage, additional treatment/management may include sentinel lymph node biopsy, radiotherapy or chemotherapy.
TREATMENTS
As part of informed consent, patients need to have the treatment and side-effects explained to them before any procedures are undertaken.
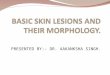
Figure 5 a–c.Different presentations of squamous cell carcinoma.
a: Hard, nodular b: Ulcerating c: ‘Juicy’
Figure 6 a–c.Examples of different presentations of malignant melanoma.
a: Superficial spreading: stage 1
b: Melanoma c: Nodular: stage 4

© 2015
Wou
nd C
are P
eople
Ltd
JOURNAL OF COMMUNITY NURSING
Welcome to JCN’s learning zone...
JCN’s online resource, which, together with the learning zone in the Journal of Community Nursing, helps you to develop your knowledge in vital areas of care, to keep up to date with clinical practice.
Read the article
Reflect on what you have learnt
Review your knowledge with the online test
... Then, download your certificate to show that you have completed this e-learning unit and gained competency in this area of clinical practice.
JCN’s learning zone — an essential educational resource for all busy nurses working in the community.

© 2015
Wou
nd C
are P
eople
Ltd
SKIN CARE
60 JCN 2015, Vol 29, No 6
CryotherapyCryotherapy involves liquid nitrogen being delivered through a spray nozzle directly onto the lesion. Short treatment times are used to treat minor lesions. Longer treatment times are required for more resistant lesions such as skin cancers, but the advantages of cryotherapy are that it can be performed in a primary care setting — it is also quick and generally leaves a good cosmetic result (Thai and Sinclair, 1999).
Early, fairly flat, scaly lesions often respond well to cryotherapy, as do smaller lesions. Thicker lesions do not respond well, however and may need further treatment. There can also be some pain, swelling, blister formation, vascular necrosis, infection, bleeding and hypertrophic scars among other side-effects (Thai and Sinclair, 1999).
Topical 5-fluorouracilTopical 5-fluorouracil is a cream that is absorbed only by diseased cells and represents a topical form of chemotherapy. It can be used to treat large areas, is simple to apply at home and can be repeated numerous times over a period of years, as well as being able to treat subclinical lesions. However, it can be painful if the treated area becomes inflamed and cannot penetrate through thick lesions, although it can penetrate to the base of hair follicles (Electric Medicines Compendium, 2014).
Photodynamic therapyPhotodynamic therapy involves the application of a photosensitising cream that is only absorbed by diseased cells. The patient waits for three hours for the drug to be absorbed before a red light source activates the photosensitizer.
Photodynamic therapy can be used as an outpatient procedure for several lesions at one time. It can also be utilised for areas of field change. It is often successful in areas of poor healing and provides excellent cosmetic outcomes. However, it is not suitable for thick nodular lesions and can be painful during irradiation. The patient is reviewed three months after treatment and if there are any signs of
residual disease, then a repeat session is prescribed (Electric Medicines Compendium, 2015). However, the equipment and drugs are not widely available and treatment has to be performed by trained nurses who are competent in recognising skin lesion.
Curette and cauteryCurette and cautery can be used in both benign and malignant skin lesions. This technique can be used when the material being removed is softer than the surrounding skin or there is a natural plane to separate diseased tissue from normal tissue. It leaves the skin with a graze-like injury, although in skin cancers this may be a little deeper than a graze. It is also common practice to cauterise any small blood vessels during the procedure and this may leave a blackened appearance.
One of the benefits of this treatment is that diagnosis can be confirmed histologically, it usually has excellent cosmetic results and a single treatment is often curative. However, healing can be slow in areas of friction such as under ‘bra’ straps or waist bands and on the lower limbs. There may also be depressed or ‘lumpy’ scarring, altered pigmentation, infection of the wound surface and bleeding (Cunliffe and Chou, 2007).
ExcisionExcision involves the surgical removal of lesions under local anaesthetic. The advantage of this technique is its ability to confirm diagnosis histologically as well as providing a cure for some lesions. However, it is not without risks, including dehiscence, bleeding, haematoma, scarring and, in some cases, poor healing (Cunliffe and Chou, 2007).
Mohs surgeryUsed for skin cancers, particularly those in awkward areas. The tissue is removed layer by layer and examined microscopically until all margins are clear of disease. Advantages of this technique include a cure rate for basal cell carcinoma of 97–99.8% (Snow and Mikhail, 2004); the ability to preserve tissue in awkward or anatomically important areas; and good cosmetic results.
Disadvantages include the length of the procedure; the risk of misreading the slides (it can be difficult to distinguish between hair follicles and carcinoma); wound infection; dehiscence, bleeding and unexplained poor healing.
RadiotherapyRadiotherapy involves radiation from a high-energy electron beam (particulate) or superficial x-rays (photons). The electron beam causes less damage to underlying cartilage and bone but is more complex to deliver. Advantages include the painless nature of the technique, which does not require anaesthetic; its use in patients unsuitable for surgery; and the fact that it is less destructive than surgery.
Disadvantages include a lack of margin control; the need for tertiary referral and multiple visits; and occasional ulceration. Radiotherapy cannot be repeated if treatment fails and there is a long-term risk of inducing secondary malignancy in the treatment field (Rigel et al, 2011).
ChemotherapyIntravenous chemotherapy targets the cancer cells and while it can provide hope for the patient, it is not necessarily a cure. The advantage
Answer the following questions about this topic, either to test the
new knowledge you have gained or to form part of your ongoing practice
development portfolio.
1 – What are the causes of skin cancer?
2 – What are the main types of skin cancer?
3 – Name the most common features of skin cancer
4 – Are you familiar with the types of lesions that develop?
5 – Would you know the main treatments for skin cancer?
Five-minute test

© 2015
Wou
nd C
are P
eople
Ltd
SKIN CARE
JCN 2015, Vol 29, No 6 61
is that it can address symptoms, however the disadvantages include the fact that it is still experimental and requires a prolonged course of treatment involving multiple visits (Marsden et al, 2010).
CONCLUSION
There are thousands of different skin diseases and skin lesions are just a small area of dermatology. With limited space, only a brief overview of six types have been provided in this article. With each lesion discussed comes varying presentations. A comprehensive history is essential to accurately formulate a diagnosis. By studying the lesions discussed within this article and learning the correct terminology, nurses have the opportunity to make a tangible impact on the wellbeing of patients.
At some stage in their life everyone, will have something uncommon or ‘strange’ on their skin. The author does not expect community nurses to become experts overnight, but by using the ABCDE acronym they will be able to notice when a lesion does not fit into the ‘normal’ range and refer appropriately. JCN
REFERENCES
Ahmed I, Berth-Jones J, Charles-Holmes S, O’Callaghan CJ, Ilchyshyn A (2000) Comparison of cryotherapy with curettage in the treatment of Bowen’s disease: a prospective study. Br J Dermatol 143(4): 759–66
Arndt KA, Wintroub BU, Robinson JK, LeBoit PE (1997) Primary Care Dermatology. WB Saunders Company, London
BAD (2012a) Basal cell carcinoma. Available online: www.bad.org.uk (accessed 10 October, 2015)
BAD (2012b) Squamous cell carcinoma. Available online: www.bad.org.uk (accessed 10 October, 2015)
BAD (2012c) Melanoma. Available online: www.bad.org.uk (accessed 10 October, 2015)
Baldry RJ, Harries MJ, Nayeemuddin F, Rhodes LE (2006) Disorders of aging skin. Rev Clin Gerontol 16(3): 165–77
Balin AK (2015) Seborrhoeic keratosis. Available online: http://emedicine.medscape.com/article/1059477-overview (accessed 10 October, 2015)
CunliffeTP, Chou C (2007) Primary Care Dermatology Society — Skin Surgery Guidelines. Available online: www.pcds.org.uk/images/downloads/skin_surgery_guidelines.pdf (accessed 10 October, 2015)
de Berker D, McGregor JM, Hughes BR (2007) Guidelines for the management of actinic keratoses. Br J Dermatol 156: 222–30
Electronic Medicines Compendium (2014) Efudix cream. Available online: www.medicines.org.uk/emc/medicine/6219/SPC/Efudix+Cream (accessed 10 October, 2015)
Electronic Medicines Compendium (2015) Metvix 160mg/g cream. Available online: www.medicines.org.uk/emc/medicine/11913 (accessed 10 October, 2015)
Farage MA, Miller KW, Berardesca E, Maibach HI (2008) Neoplastic skin lesions in the elderly patient. Cutaneous and Ocular Toxicology 27(3): 213–29
Johnson SR, Taylor MA (2012) Identification and management of malignant skin lesions among older adults. J Nurse Pract 8(8): 610–16
Kaldas MV (2014) Bowen Disease Clinical Presentation. Available online: http://emedicine.medscape.com/article/1100113-clinical (accessed 10 October, 2015)
Lasithiotakis KG, Petrakis IE, Garbe C (2010) Cutaneous melanoma in the elderly: epidemiology, prognosis and treatment. Melanoma Res 20(3): 163–70
MacKie RM (2003) Clinical Dermatology. Oxford University Press, Oxford
Marsden JR, Newton-Bishop JA, Burrows L, et al (2010) Revised UK guidelines for the management of cutaneous melanoma 2010. Br J Dermatol 163: 238–56
Poyner TF (2005) Dermatology made easy: How to make a diagnosis. Nuffield Press, Oxford
Reed CM (1998) Parrish’s chemical food never contained arsenic. Br Med J 317(7152): 212
Rigel DS, Robinson JK, Ross, et al (2011) Cancer of the Skin. Second edition. Elsevier Health Sciences, Philadelphia
Sachs DL, Marghoob AA, Halpern A (2001) Skin cancer in the elderly. Clin Geriatr Med 17(4): 715–38
Schofield J, Kneebone R (2006) Skin Lesions: A practical guide to diagnosis, management and minor surgery. Second edition. Metro Commercial Printing Limited, He rtfordshire
Snow SN, Mikhail GR (2004) Mohs Micrographic Surgery. Second edition.University of Wisconsin Press, Wisconsin
Spencer JM (2015) Actinic Keratosis. Available online: http://emedicine.medscape.com/article/1099775-overview (accessed 10 October, 2015)
Thai KE, Sinclair RD (1999) Cryosurgery of benign skin lesions. Aus J Dermatol 40: 175–86
Veness M (2001) Lip cancer: important management issues. Aus J Dermatol 42: 30–2
With over 13,000 cases of melanoma diagnosed in 2012, and 74% of these
presenting in the over 50s, the author presents a timely reminder that community nurses are ideally placed to identify and instigate action for the treatment of these potentially fatal lesions.
Skin cancers of the non-melanoma and melanoma types can be overlooked or mistaken for the more common benign cutaneous growths found in the older population. A clear and concise description of each of the six common types of skin lesion
Expert commentary David A Haigh, clinical nurse specialist, Guy’s and St. Thomas’ NHS Foundation Trust, London
is given by the author, which should help community nurses to distinguish between them and decide upon the appropriate intervention.
The author has also helpfully used the correct terminology to describe the lesions accurately — this is not only appropriate for these particular lesions, but for all dermatology conditions irrespective of age. As the author points out, the piece is not aimed at experts but does provide relevant information to help community nurses begin to identify and distinguish between harmful and non-harmful skin growths.