Embed Size (px)
Citation preview

Dallas, TX • November 2–4, 2012
Reducing Contrast Extravasation
Linda McDonald, MSN, RN, CRN
Radiology Advanced Practice Nurse
Children’s Hospital of Pittsburgh of UPMC

Dallas, TX • November 2–4, 2012
Objectives
• Discuss how contrast delivery is different from most other medications and how this impacts extravasation
• List three actions to reduce extravasation potential during contrast delivery
Dallas, TX • November 2–4, 2012
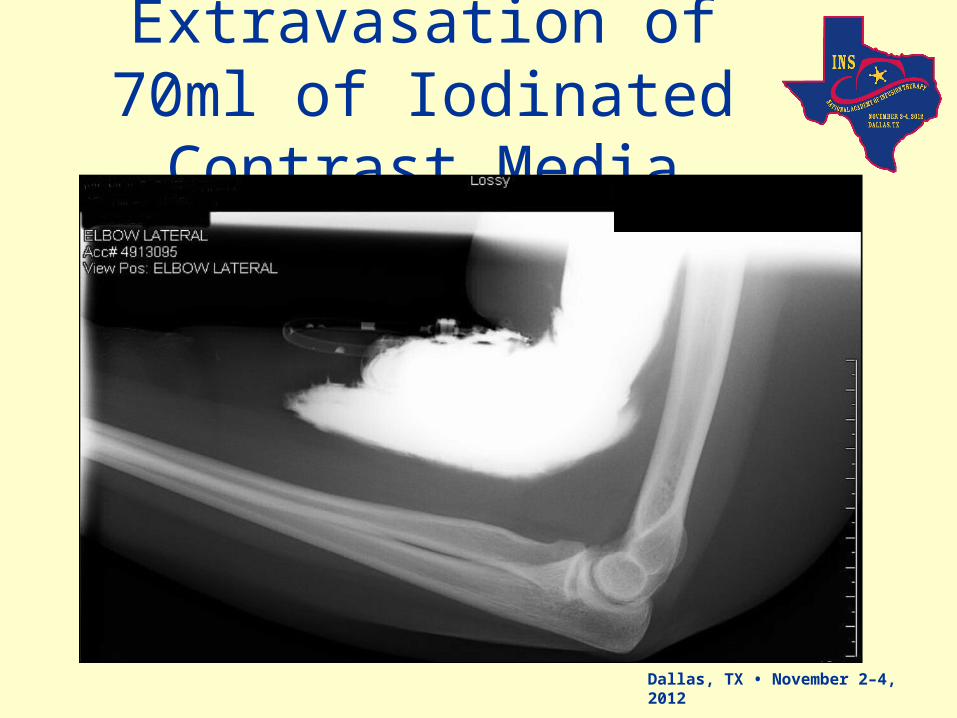
Extravasation of 70ml of Iodinated Contrast
Media

Dallas, TX • November 2–4, 2012
This took 17.5 seconds to happen

Dallas, TX • November 2–4, 2012
What is an extravasation ?
• “the inadvertent infiltration of vesicant solution or medication into surrounding tissue”1
• Vesicant – “an agent capable of causing blistering, tissue sloughing, or necrosis when it escapes from the intended vascular pathway into surrounding tissues”1

Dallas, TX • November 2–4, 2012
What Does The Patient Feel?
• Most feel a sensation of swelling or tightness, Wang,et al reported 79% experienced this5
• Most also feel stinging or burning pain at the site, Wang, et al reported 24% experienced this5
• Some feel nothing at all2, Wang, et al reported 8% experienced no symptoms5

Dallas, TX • November 2–4, 2012
Incidence of Contrast Extravasation
• American College of Radiology (ACR) reports a 0.1% to 0.9% rate of extravasation from power injection of contrast media for a CT scan
• Equates to 1/1000 to 1/106 patients
• Frequency not related to injection flow rate

Dallas, TX • November 2–4, 2012
What is IV contrast ?
• diagnostic material that alters x-ray absorption by body tissues or organs
• can discriminate between disease and normal tissue
• Many diseases would go undetected if contrast media was not used 3
Dallas, TX • November 2–4, 2012
Where is it used ?
• Computed Tomography (CT)
• Magnetic Resonance Imaging (MRI)
• Positron Emitting Imaging with CT (PET/CT)
• Fluoroscopy
• Angiography

Dallas, TX • November 2–4, 2012
Types of IV Contrast
• Iodine-based contrast – used in CT, Angiography, Fluoroscopy- Ionic – 1st generation
- Non-ionic – 2nd generation
- Iso-osmolar – 3rd generation
• Gadolinium-based contrast – used in MRI
Dallas, TX • November 2–4, 2012
Contrast Characteristics That
Are Problematic
• Osmolality
• Viscosity
• pH
Dallas, TX • November 2–4, 2012
Osmolality of Contrast Media
• Osmolality – “number of milliosmoles per kilogram of solvent”, measure of the total number of particles (solutes) in a solution1
• Normal serum osmolality is 280-295 mOsm/kg H2O
• IV Contrast medias range from 290 - 1970 mOsm/kg H2O2

Dallas, TX • November 2–4, 2012
Viscosity of Contrast Media
• describes a fluid's internal resistance to flow - a measure of fluid friction4
water is “thin” with low viscosity
honey is “thick” with high viscosity
• Range from 2 - 26.6 cP
Dallas, TX • November 2–4, 2012
pH of Contrast Media
• The acidity or alkalinity of a substance1
• Blood has a pH of 7.35-7.45
• Range from 5.5 – 8.0

Dallas, TX • November 2–4, 2012
Comparison of Iodinated IV Contrasts
• Ionic – HOCM (high osmolar contrast media) - osmolality 1000-1551 mOsm/kgH2O
- viscosity 6-16.4 cps at 25°C, 4-10.5 cps at 37°C
• Non-ionic – LOCM (low osmolar contrast media) - osmolality 744-874 mOsm/kgH2O
- viscosity 14.3-22 cps at 25°C, 9-10.4 cps at 37°C
• Iso-osmolar – IOCM - osmolality 290-769 mOsm/kgH2O
- viscosity 20.9-26.6 cps at 25°C, 9.4-26.6 cps at 37°C

Dallas, TX • November 2–4, 2012
Comparison of Gadolinium Contrast
Media• Gadolinium
- osmolality 688 - 1970 mOsm/kgH2O
- viscosity 2 - 9.2 cps at 25°C
1.4 - 5.3cps at 37°C

Dallas, TX • November 2–4, 2012
How is IV Contrast Injected ?
• Hand injected by a syringe
• Mechanically injected by a power injector

Dallas, TX • November 2–4, 2012
Why Use Power Injectors ?
• Best enhancement seen in 15 – 120 seconds after injection7
• Small volumes can be quickly injected by hand
• Larger volumes can not be injected fast enough by hand
• Today there are CT scanners that can scan a whole body in 5 seconds
Dallas, TX • November 2–4, 2012
How Fast Does it Inject ?
• Rates ranging from 1-10ml per second
• Adult for CT of abdomen and pelvis with contrast commonly receives 60ml of contrast at 4ml per second
• 60ml is injected in 15 seconds

Dallas, TX • November 2–4, 2012
How Much Pressure is Used ?
• Most injectors are set at a default of a maximum pressure setting of 300-325 psi
• Injectors only exert the psi necessary to deliver the contrast at the rate programmed

Dallas, TX • November 2–4, 2012
What Steps Are Taken To Prevent
Extravasation ?• Inspect the site
• Verify blood return
• Verify ability to flush easily with NSS
• Verify patient has no discomfort with NSS flush
• Verify that the catheter and accessory products are power injectable
• Verify flow rate is appropriate for the catheter size

Dallas, TX • November 2–4, 2012
What Steps Are Taken to Detect
Extravasation ?• Patient instructions – get cooperation to
immediately tell RT if any pain or sensation of swelling
• Palpation of site during first 15 seconds of injection, then RT exits scan room
• Maintain communication with the patient via intercom and/or video monitor

Dallas, TX • November 2–4, 2012
Equipment That May Help Reduce Extravasation
• Extravasation detectors – sensors placed on skin - designed to prevent moderate to severe contrast extravasations
• Dual head injectors that inject saline prior to the contrast
Dallas, TX • November 2–4, 2012
ACR Recommendations
• ACR recommends use of the antecubital or forearm vein – if smaller hand or wrist vein is used then injection rate should be decreased to 1.5ml/sec2
• Metal needles should be avoided and flexible plastic cannula used2

Dallas, TX • November 2–4, 2012
What IV Access Device is Used?
• Central Venous Access Devices– Power injectable catheters and ports– Preferable because they are located in larger
central veins and power injection requires less psi to deliver the desired rate
• Peripheral Venous Catheters– Catheters must be power injectable– Gauge of catheter must be large enough to
accommodate the required rate of flow– Accessory devices must be power injectable

Dallas, TX • November 2–4, 2012
Short Peripheral IV Devices
• Infusion Nursing Standards of Practice have stated these catheters are not appropriate for “infusates with osmolality >600mOsm/L.”1
• Risk – Benefit assessment of the patient to determine appropriateness of central venous access vs. short peripheral IV catheter access

Dallas, TX • November 2–4, 2012
What Patients Are Most At Risk of Extravasation
• Those unable to communicate
• Abnormal circulation in the limb to be injected
• Altered circulation such as in PVD, diabetic vascular disease, Reynaud’s Disease
• Venous thrombosis or insufficiency

Dallas, TX • November 2–4, 2012
What Patients Are Most At Risk of
Extravasation cont.• Multiple punctures in to the same vein
• Prior radiation or extensive surgery in the limb to be injected
• Peripheral IV catheters that have been in place more than 24 hours
• Catheters in sites such as the hand, wrist, foot or ankle are at higher risk

Dallas, TX • November 2–4, 2012
When Extravasation Does Occur What
Happens ?• Toxic to the surrounding tissues especially the skin
• Acute local inflammatory response that make peak in 24-48 hours
• Most will resolve without further problems
• Rare occurrence of severe symptoms – most common is Compartment Syndrome
Dallas, TX • November 2–4, 2012
How Do We Reduce The Incidence of
Contrast Extravasations?• Collaboration of all disciplines
involved in the patient’s vascular access– ED and inpatient physicians & nurses– IV Team– Radiology– Oncology– Pharmacy

Dallas, TX • November 2–4, 2012
Case Study
• Contrast extravasation rate was 0.6%
• Volume of contrast extravasated was commonly over 50ml
• 75% of contrast extravasations occurred in pre-existing IV on ED or inpatients
• Non-power injectable accessory devices were in use

Dallas, TX • November 2–4, 2012
Actions• Education on contrast media, vein
selection, assessment of venous access, assessment for use of power injectable devices, & treatment of extravasations for radiology RNs and RTs
• Education expanded to include radiologists and radiology residents
• Each extravasation was investigated & patient was followed until resolved

Dallas, TX • November 2–4, 2012
Results
• Slightly improved outcomes– Extravasation rate slightly decreased– Volume of contrast extravasated was lower– Use of only power injectable accessory
devices became the standard– Still saw inpatients and ED patients
experiencing most of the extravasations

Dallas, TX • November 2–4, 2012
What Next ?• Hospital Extravasation Task Force was
created – was a subcommittee of the Patient Safety Committee– Radiology– IV Team– Oncology– Patient Safety– Emergency Department– Inpatient Nursing– Plastic Surgery– Pharmacy

Dallas, TX • November 2–4, 2012
What Was Found ?
• Discovered that many pre-hospital IV catheters were involved in extravasation
• Found that education for nurses, paramedics and technologists varied greatly
• Staff had no involvement with IV product selection
• Extravasation treatment was inconsistent

Dallas, TX • November 2–4, 2012
Next Steps
• Standardized mandatory IV education housewide for all RNs and all IV starters/injectors
• Changed hospital policy requiring IV catheter removal within 24 hours for those started outside the hospital
• Developed hospital extravasation policy that defined vesicants and treatment, standardized documentation of extravs
Dallas, TX • November 2–4, 2012
Collaborations
• ED and Radiology worked together– ED RN or Paramedic would immediately
start a new IV with power injectable accessories on all trauma and stroke patients, this IV was indicated for use to inject IV contrast
– Trauma Team changed brand of triple lumen catheter to a power injectable one

Dallas, TX • November 2–4, 2012
Collaborations
• IV Team and Radiology worked together– Education done for IV Team RNs about
contrast media and need for certain gauge catheters for certain studies
– PICC nurses included possible need for CT and MRI contrast injection in their decision algorithm for catheter selection which resulted in more power injectable PICCs inserted

Dallas, TX • November 2–4, 2012
Collaborations
• Oncology and Radiology worked together– Power Ports were only to be accessed with
a power injectable huber needle– Education for the oncology staff regarding
contrast media injection focusing on assessment of solutions that have been administered through that catheter & possible need of new site prior to CT
– Hospital port now power injectable

Dallas, TX • November 2–4, 2012
Results
FISCAL YEAR EXTRAVASATION RATES
0.60%0.52%
0.39%0.34%
0.30%
0.00%
0.10%
0.20%
0.30%
0.40%
0.50%
0.60%
0.70%
FY 2007 FY 2008 FY2009 FY 2010 FY 2011
FISCAL YEAR EXTRAVASATION RATES

Dallas, TX • November 2–4, 2012
Lessons Learned
• Collaboration is the key to successfully reducing contrast extravasations
• Communication between all disciplines involved in the patient’s care is imperative
• We can improve patient safety and satisfaction when we work together

Dallas, TX • November 2–4, 2012
References
1. Infusion Nurse Society. (2011, January/February). Infusion Nursing Standards of Practice. Journal of Infusion Nursing, ppS5-108.
2. American College of Radiology (2012). Retrieved August 30, 2012 from ACR Manual on Contrast Media Version 8. http://www.acr.org/~/media/ACR/Documents/PDF/QualitySafety/Resources/Contrast%20Manual/FullManual.pdf.
3. Gross, K., & Costa, N. (2008). Core Curriculum for Radiologic and Imaging Nursing, 2nd Edition (pp1-83). Pensacola: American Radiological Nurses Association.
4. MEDRAD XDS® Extravasation Detector. (2012), Bayer HealthCare Radiology & Interventional. Retrieved August 30, 2012 from http://www.medrad.com/en-us/info/products/Pages/XDS-details.aspx.
5. Wang, C., Cohan, R., Ellis, J., Adusumilli, S., & Dunnick, N.(2007, April). Frequency, Management, and Outcome of Extravasation of Nonionic Iodinated Contrast Medium in 69,657 Intravenous Injections. Radiology, pp 80-87.






























