Embed Size (px)
DESCRIPTION
Cushing Syndrome 2013
Citation preview

04/05/2013
1
Cushing Syndrome(Hypercortisolism)
Titis Kurniawan, MNS
Scope
� Physiology of Cortex Adrenal
� Overview Cushing’s syndrome (CS)
� Etiology CS
� Diagnostic test
� Sign & Symptom CS
� Patophysiology CS
� CS Management

04/05/2013
2
Anatomy Fisiology Adrenal Gland
Cortex
Medulla
Aldosterone
(mineralocorticoid)Cortisol
(glucocorticoid)Androgen
Catecholamines; epi &
norepinephrin
Zona glomerulosa Zona fasciculata Zona reticularis
� Katabolik thd protein� Glukoneogenesis & inhibit insulin� Immunosupressive� Suppress parasympatis syst �
Increase Hcl
Fungsi Sistem Reproduksi (pria), ciri sex pria
� Organ target � ginjal (tubule distal & ductus colectivus)
� Bagian dari renin-angiotensin� >> retensi Na dan sekresi K� >> retensi cairan� >> tekanan darah
Sympathetic Nervous System �
increases in heart rate, blood pressure, blood glucose levels, and a general reaction of the

04/05/2013
3
Normal Range of Cortisol
Reference ranges for blood plasma content of free cortisol
Time Lower limit Upper limit Unit
09:00 am140 700 nmol/L
5 25 µg/dL
Midnight80 350 nmol/L
2.9 13 µg/dL
Reference ranges for urinalysis of free cortisol
Lower limit Upper limit Unit
28 or 30 280 or 490 nmol/24h
10 or 11 100 or 176 µg/24 h
Cushing Syndrome
� Is: group of symptoms resulted from any conditions that increase of blood glukokortikoid level (Maitra, A & Kumar, V., 2007; Schteingart, 2006)
� Can spontaneously occured follow high dose glukokortikoid prescription
� Insidence: 5 – 25 cases/1 million people/year
� Risk: 25 – 45 years old, women,uncontrolled diabetes, & obesity
� Type;� Iatrogenic; long-term glucocorticoid prescription� Spontan; Dependen & Independen ACTH

04/05/2013
4
Etiology� Iatrogenic ; Long term glukokortikoid prescription
(astma, artritis rheumatoid, limfoma & integument problem who receive glucocorticoid/steroid as anti inflamation agent
� Spontan; hypersecretion cortisol resulted from impairment of hipotalamus-hippofisis-adrenal axis (spontan)�Dependen ACTH
� ACTH secretion from ipofisis gland� Adenoma � sintesis & release ACTH ectopic
� Independen ACTH� Adenoma sintesis & release peptida = ACTH� Carsinoma sel paru/karsinoid bronkus, & sel pankreas release
CRH ectopic� Hiperplasia cortex adrenal nodular bilateral � >> cortisol
PathophysiologyIatrogenic Spontan
>> Glucocorticoid/Cortisol>> Katabolisme Protein
OtotIntegumen
Tulang
<< matrik tulang
Osteoporosis
Mudah cidera/ Perub. Postur/
Vertebra
Rapuh
Mudah luka
Luka sukar
sembuh
Kerusakan jaringan elastis
Striae
Risiko Ggn. Body Image
Ggn Integritas kulit
Vaskuler
Tipis & rapuh
Ptechiae
Atropi & lemah
Intoleransi aktivitas
Imun
Ggn pembentukan antibodi &
proliferasi limfoid
Risiko Infeksi
Jaringan Adiposa
Distribusi di sentral tubuh
CushingoidBuffalo hump,
moonface Obesity
>> Katabolisme karbohidrat
>> glukosa darah
<< Respon imunitas
>> sekresi lambung
Respon psikologis
>> HCLRisk Ulkus peptikum
Ggn Mood, euforia, depresi Risk. Koping tidak eektif/perilaku destruktif
<< GnRHGgn Sist
Reproduksi
>> aktivasi jantung

04/05/2013
5
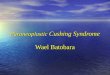
Signs & Symptoms
Diagnostic Test
� Riwayat kesehatan
� Pemeriksaan fisik (sign & symptoms)
� Urinary free cortisol (UFC) test (220 –330nmol/24h)
� Plasma cortisol test
� Low doses dexamethasone test
� Cortisol circadian rhythm assessment
� MRI
� Dll

04/05/2013
6
Suspected CS Screening
– 24 hour urine free cortisol - Reflects cortisolproduction. Always measure urinary creatinineto insure completeness of collection
– Overnight dexamethasone suppression test– Both tests detect uncontrolled cortisol
production but do not distinguish etiology– Be careful with Pseudo cushing;
– Related to depression & alcoholism
– Periodic hormonogenesis
– When in doubt, wait 6-12 weeks and re-evaluate!
Dexamethason suppression test� Dexamethason exogenous steroid that provides negative
feedback to the pituitary to suppress the secretion of ACTH
� The test is given at low (usually 1–2 mg) and high (8 mg) doses of dexamethasone and the levels of cortisol are measured to obtain the results
� Low & high dose � no change cortisol � other causes (ectopic ACTH syndrome)
� Low dose � not change, but change with High dose �Cushing diseases � MRI of Pituitary considered
...........Diagnostic Test

04/05/2013
7
Nursing Process
Assessment� History; asthma, rheumatoid artritis, konsumsi obat steroid
� Psikologis; insomnia, euforia, depresi singkat, mood alteration
� General; Obesitas, moon face, buffalo hump
� Opthamic; Cataract, glaukoma, keluhan pandangan kabur
� Cardiovascular: HT, CHF, ptechie, echymosis
� Integumen: luka memar, luka tidak sembuh, striae, acne
� Muskuloskeletal: muscle weakness, atropi, myopathy
osteoporosis
� Gastrontestinal; peptic ulcer
� Pemeriksaan lab; hiperglikemia, hypernatremia, hypokalemia
Nursing Diagnoses
� Resiko injury b.d weakness, osteoporosis,
� Resiko infeksi b.d immunosupresi
� Self care deficit b.d muscle weakness, fatigue, altered sleeppatern
� Ggn integritas kulit b.d edema, gangguan penyembuhan luka, kulit yg tipis dan mudah pecah
� Ggn Body image b.d perubahan penampilan fisik
� Perub proses fikir b.d. perubahan mood, irritabilitas, depresi
� Risiko kping tdk efektif b.d. mood, irritabilitas, depresi
......Nursing Process

04/05/2013
8
Nursing Intervention�Pengendalian resiko injury
�Pengendalian resiko infeksi
�Anjurk istirahat dan aktivitas yg tepat
�Promote integritas kulit→mobilisasi u/ mcegah breakdown skin
� Improve body image
�Relationship with other
�BB dpt dikendalikan dg Diet low KH, Low sodium
� Improve proses berfikir
� Improve mekanisme koping
......Nursing Process