-
ORIGINAL ARTICLE
Three-dimensional computed tomographicanalysis of changes to the
external featuresof the nose after surgically assisted
rapidmaxillary expansion and orthodontictreatment: A prospective
longitudinal study
Anders Magnusson,a Krister Bjerklin,b Hyungmin Kim,c Peter
Nilsson,d and Agneta Marcussone
J€onk€oping and Link€oping, Sweden, and Boston, Mass
aSenioDentabAssoDentacPostdHospidAssoPostgeAssoUnit,All
auPotenSuppoand tReprinfor Poe-maiSubm0889-Copyrhttp:/
404
Introduction: The aim of this prospective, longitudinal study
was to evaluate changes to the external shape andform of the nose
after surgically assisted rapid maxillary expansion and orthodontic
treatment. The changeswere registered using a 3-dimensional
computer tomography technique, based on superimposition onthe
anterior base of the skull. Methods: The subjects comprised 35
patients (mean age, 19.7 years; range,16.1-43.9 years). Low-dose,
helical computerized tomography images were taken at treatment
start and afterorthodontic treatment, about 18 months postsurgery.
The 3-dimensional models were registered andsuperimposed on the
anterior cranial base. Results: There were in general significant
widening and overallanterior and inferior displacement of the nasal
soft tissues. The changes varied in size and direction.
Nocorrelation was found between the initial and final widths of the
nose, or between the initial and final widths ofthe nostrils.
Conclusions: After surgically assisted rapid maxillary expansion,
the most obvious changes tothe external features of the nose were
at the most lateral alar bases. The difference in lateral
displacementprofoundly influenced the perception of a more rounded
nose. Patients with narrow and constrained nostrilscan benefit from
these changes. The 3-dimensional superimposition applied in this
study is a reliable method,circumventing projection and measurement
errors. (Am J Orthod Dentofacial Orthop 2013;144:404-13)
Transverse maxillary hypoplasia is associated pri-marily with
functional impairments, such asposterior crossbite, dental
crowding, reducednasal respiratory function, or anteroposterior
skeletal
r consultant, Department of Orthodontics, Institute for
Postgraduatel Education, J€onk€oping, Sweden.ciate professor,
Department of Orthodontics, Institute for Postgraduatel Education,
J€onk€oping, Sweden.octoral research fellow, Department of
Radiology, Brigham and Women'stal, Harvard Medical School, Boston,
Mass.ciate professor, Department of Oral and Maxillofacial Surgery,
Institute forraduate Dental Education, J€onk€oping, Sweden.ciate
Professor, Department of Dentofacial Orthopaedics,
MaxillofacialUniversity Hospital, Link€oping, Sweden.thors have
completed and submitted the ICMJE Form for Disclosure oftial
Conflicts of Interest, and none were reported.rted by Futurum, the
Academy for Healthcare, County Council, J€onk€oping,he Medical
Research Council of Southeast Sweden.t requests to: Anders
Magnusson, Department of Orthodontics, Institutestgraduate Dental
Education, Box 1030, SE-551 11 J€onk€oping, Sweden;l,
[email protected], January 2013; revised and accepted,
April 2013.5406/$36.00ight � 2013 by the American Association of
Orthodontists./dx.doi.org/10.1016/j.ajodo.2013.04.013
anomalies, and less with facial esthetics.1-5 A widelyrecognized
treatment modality for this condition iscorrection of the
underlying skeletal anomaliesby surgically assisted rapid maxillary
expansion(SARME).6-8
Although the skeletal and dental effects of SARMEhave been
evaluated in several clinical and radiographicstudies, little is
known about its effect on the shape andform of the nose.9-11 The
soft-tissue changes can bequite obvious, and most clinicians have
observedpatients in whom SARME has been associated withpronounced
changes to the nose. In some patients,this might be regarded as an
untoward side effect; inothers, it could improve facial
esthetics.
Soft-tissue changes after corrective orthognathicsurgery have
been described in a number ofstudies.12-15 Consistent findings
after maxillaryadvancement and maxillary impaction are
labialchanges and widening of the nose.16 Most surgeonsare aware of
these phenomena and use differenttechniques to reduce these
effects.17,18
Delta:1_given nameDelta:1_surnameDelta:1_given
nameDelta:1_surnameDelta:1_given
namemailto:[email protected]://dx.doi.org/10.1016/j.ajodo.2013.04.013
-
Magnusson et al 405
The size and shape of the nostrils and the width ofthe alar base
are considered to play important rolesin respiration. It is
suggested that the site responsiblefor sensing airflow and
stuffiness is in the nasalvestibule.19,20 Guenthner et al21
associated modifica-tions in the shape of the external nares with
changedairway patency. This finding was supported by Cole,22
who found significant associations between minoralterations in
this region and improvement or deteriora-tion in respiratory
function. Moreover, Magnusson et al4
concluded that even small changes to the soft tissues inthe most
anterior part of a narrow nose can be critical tothe subject's
perception of nasal obstruction.
However, with reference to SARME, little is knownabout
associated soft-tissue changes and the effectson facial esthetics
and respiration.
SARME is often followed by second-stage surgerythat can have a
further impact on the soft tissues andrespiration. Thus, it is
essential to identify soft-tissuechanges associated with SARME to
predict or preventthese effects.
Previous studies on SARME and its effects on softtissues have
been limited by the methods available atthe time for quantifying
soft-tissue changes. Nganet al23 and Filho et al24 used traditional
2-dimensional(2D) lateral cephalograms. When applied to
assesschanges in the soft-tissue profile, 2D cephalometricshave
major disadvantages. It is difficult to quantifysoft-tissue
alterations adequately from a frontalperspective. Berger et al25
used serial frontal photo-graphs to measure soft-tissue changes,
and Ramieriet al26,27 used laser scanning and 3-dimensional
(3D)morphometry. In the 3D analysis, the superimpositionmethod is
crucial. The major disadvantage of thesemethods is the potential
error associated with uncertainsuperimposition, which is related to
approximations oraveraged data.
Recently, there have been impressive advancesin computed
tomography and imaging techniques,offering new, precise, and
accurate approaches to super-imposition.
The purpose of this prospective study was to evaluatechanges to
the external features of the nose after SARMEand orthodontic
treatment, using a 3D imagingtechnique and registration based on
superimpositionon the anterior cranial base.
MATERIAL AND METHODS
Our prospective sample comprised patients sched-uled to undergo
SARME. The inclusion criterion forSARME was a real transverse
discrepancy according toJacobs et al.28 The magnitude of the
skeletal discrepancy(.5 mm) was primarily assessed clinically and
on study
American Journal of Orthodontics and Dentofacial Orthoped
models in Class I relationships.1 Transverse assessmentswere
also done on computed tomography models.29
This sample was previously evaluated by Magnussonet al4 with
reference to skeletal changes after SARME.The same orthodontic,
surgical, and radiographicprocedures were applied in both
studies.
According to power and size calculations, a priori, theminimum
sample size was set at 34 patients, a 5 0.05,and power of 80%. To
ensure that the sample size metthese requirements, 40 patients were
recruited consecu-tively at the Department of Orthodontics,
Institute forPostgraduate Dental Education, J€onk€oping, Sweden,and
at the Department of Dentofacial Orthopaedics,Maxillofacial Unit,
University Hospital, in Link€oping,Sweden. Participation in the
study was voluntary:3 patients declined to participate, and 2
patients wereexcluded because their computed tomography recordswere
incomplete. The sample thus comprised 35 patients(14 male, 21
female). The mean age at treatment startwas 19.7 years (range,
16.1-43.9 years).
The study was approved by the ethics committee ofthe Faculty of
Health Sciences, Link€oping University, inSweden (reference:
M746-04).
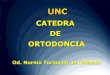
The presurgical orthodontic preparation included thefollowing.
The maxillary expansion appliance compriseda tooth-borne device
activated by means of aconventional hyrax expander (hyrax II;
Dentaurum,Ispringen, Germany) with a soldered framework
andorthodontic bands (Fig 1). The degree of expansionwas calculated
for each patient, including a generalbilateral overexpansion of
half a molar-cusp width.The patients were instructed to activate
the jackscrew1 turn (approximately 0.225-0.250 mm) twice a dayafter
a postoperative latency period of 5 days. Postoper-ative control
was scheduled for 12 days postsurgery andincluded a periapical
radiograph to ensure clinicallysymmetrical interdental separation
and a medialdiastema.30 In patients with a “bad
separation”—ie,intra-alveolar separation and risk for
periodontalinjuries—prophylactic treatment was initiated. Atthat
time, the amount of additional expansion wascalculated.
Surgical treatment was undertaken by 2 experiencedsenior oral
and maxillofacial surgeons (P.N. and another)at the Department of
Oral and Maxillofacial Surgery,Institute for Postgraduate Dental
Education, J€onk€oping,Sweden, and at the Department of
DentofacialOrthopaedics, Maxillofacial Unit, University
Hospital,Link€oping, Sweden, with a technique similar to
thatdescribed by Glassman et al.31
The surgery was carried out under general anesthesiaand
nasotracheal intubation. The mucoperiostealincision in the
maxillary vestibule extended from the
ics September 2013 � Vol 144 � Issue 3
-
Fig 1. Skeletal maxillary transverse discrepancyexceeding 5 mm.
Tooth-borne maxillary expansionappliance, activated by a
conventional hyrax expander(Hyrax II; Dentaurum, Ispingen,
Germany).
406 Magnusson et al
right to the left second premolar. Osteotomies wereperformed on
the maxillary lateral walls, from thepiriform aperture to the
pterygoid plates. The pterygo-maxillary sutures were kept intact.
The linings of thefloor and lateral walls of the nasal passage
werereflected. A vertical osteotomy at the anterior nasal spineand
the median palatal suture was carried out to ensureseparation of
the maxillary halves. The hyrax expanderwas activated by 12 turns
to verify the success of theosteotomy and to ensure visible
symmetrical separation;it was then deactivated by the same
amount.
Depending on their physical condition, the patientswere
discharged from the hospital on the same day orthe day after
surgery.
The postsurgical orthodontic procedures includedthe following.
After a mean active expansion period of15 days (range, 11-17 days),
the appliance was used asa passive retainer for 90 days. At that
time, the hyraxexpander was replaced by a modified transpalatal
arch,and fixed appliance treatment began.
On completion of the active treatment phase, thetranspalatal
arch was removed, and fixed appliancetreatment continued with stiff
rectangular archwires toadjust the transverse width and to control
and correctthe buccal root torque of the molars.
All transverse discrepancies were corrected by the endof
treatment (mean, 18 months postoperatively), and theorthodontic
treatment period was then concluded. Atthis point, 26 patients were
referred for second-stageorthognathic surgery. In the remaining 9
patients, thefixed appliance was debonded, and a Hawley plate
wasprovided as a retainer.
The computed tomography examinations were un-dertaken at the
Center for Medical Image Science andVisualization at University
Hospital, Link€oping, Sweden,
September 2013 � Vol 144 � Issue 3 American
and at the Department of Radiology, Ryhov CountyHospital,
J€onk€oping, Sweden, 1 week before surgeryand at the end of the
active orthodontic treatment phase(mean, 18 months
postoperatively).
A helical computed tomography machine (SomatomeSensation 64
CT-scanner; Siemens Medical Solutions,Erlangen, Germany) with a
low-dose protocol(CARE dose 4D; Siemens Medical Solutions) was
usedat 120 kV and 55 mA. The rotation time was 1 second,and the
pitch factor was 0.9, with a collimation of0.6 mm. The increment
was 0.3 mm. According to themanufacturer, the isotopic resolution
or voxel size was0.33 mm. The patient's head was positioned so
thatthe Frankfort horizontal plane was vertical.
The scanned area comprised the anterior cranial baseto the
mandibular base. After examination, the imageswere processed at a
radiologic workstation (SectraImtec AB, Link€oping, Sweden) with a
slice thicknessof 0.75 mm and slice increments of 0.3 mm inKernel H
60s sharp FR, to allow further segmentationand registration.
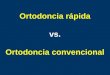
The data were processed to visualize and measuresoft-tissue
changes caused by SARME, using a modifiedversion of a technique
described by Cervidanes et al.32,33
This process involves image segmentation, registration,and
visualization (Fig 2).
The image registration and superimposition of thepreoperative
and postoperative 3D models were donebefore segmentation with a
volumetric registrationmethod: specifically, normalized mutual
information,based on the anterior cranial base. The cranial
fossaeand the ethmoid bone surfaces are regarded as stableareas,
with growth completed before puberty.34,35
Once the preoperative and postoperative volumes areregistered,
they share the same coordinate system,which compensates for any
discrepancies betweenbefore and after volumes, and diminishes the
risks ofprojection and measurement errors.
Segmentation is the process of outlining the shape ofa
structure—in this case, anterior cranial base, and theouter
surfaces of the nasal and midface soft tissues.The segmentation was
performed semiautomatically inAMIRA (Mercury Computer System,
Berlin, Germany)by an author (H.K.). In the semiautomatic
segmentationtechnique, the region of interest is outlined with
mouseclicks in the cross-sections of a data set, and
algorithms(simple thresholding and region growing) are applied,
sothat the path that best fits the edge of the image isshown. With
simple thresholding, is it possible to selecta range of gray values
(in Hounsfield units, HU). In thisstudy, the lower threshold in
bony structures was setto 300 HU, and values above this level were
automati-cally selected. The threshold value was interactively
Journal of Orthodontics and Dentofacial Orthopedics
-
Fig 2. Helical computed tomography images were taken for each
patient before and after treatment.Visualization and segmentation
involve creation of a 3D model and delineation of the
anatomicstructures of interest. The 3D models were superimposed on
the anterior cranial base by means ofa volumetric registration
method. A graphical user interface-based application (Di2Mesh) was
usedfor 3D analysis and measurements.
Magnusson et al 407
adjusted to achieve better contours. Semiautomatictools in AMIRA
were effectively used to accelerate theprocess.
A landmark-based, nonrigid mapping technique,thin-plate spline,
was used to determine the correspond-ing soft-tissue points between
the presurgery andpostsurgery 3D models.36 This was done by a
pipelineprocedure according to the method of Kim et al.37
Di2Mesh software (Institute for Surgical Technology&
Biomechanics, University of Bern, Bern, Switzerland) isa graphical
user interface-based application allowing theuser to compute
surface-to-surface distances in anyspecified direction and
visualize them with a colormap.37
Fifteen validated landmarks were used for themeasurements (Fig
3).12,38,39 The landmarks wereidentified and digitized by the first
author (A.M.). Thenonrigid transformation model, thin-plate
splinedeformation, and closest-point matching were used toshow
displacements.37 The software (Di2Mesh)computed the closest-point
relationship between thepresurgical and postsurgical landmarks in a
3DEuclidean space coordinate system.
American Journal of Orthodontics and Dentofacial Orthoped
The displacement vectors were normalized with theFrankfort
horizontal plane coordinate system accordingto the method of Xia et
al.40 The transversal plane isdefined by right and left porion, and
the averagedcoordinates of right and left orbitale. The frontal
planeis perpendicular to the transversal plane, through rightand
left porion. The sagittal plane is perpendicular tothe transversal
and frontal planes, through nasion.This means that the zero point
of the Frankforthorizontal plane will be the center of left and
rightporion. As shown in Figure 4, lateral displacement onthe
x-axis, superior displacement on the y-axis, andanterior
displacement on the z-axis were recorded aspositive values.
The transverse displacements of corresponding land-marks on the
x-axis were also summarized. TheEuclidean distances—ie, the
shortest distances between2 landmarks—were measured to evaluate the
heightand width of the nose and nostrils (Fig 5).
Ten computed tomography volumes were randomlyselected. The
anatomic landmarks were located anddigitized in each 3D model. The
same observer(A.M.) repeated the procedure 4 weeks later, and
the
ics September 2013 � Vol 144 � Issue 3
-
Fig 3. Landmarks:1, pronasale, the most anteriormidpoint of the
nasal tip; 2 and 3, alar right and left, themost lateral point on
each alar contour; 4 and 5, alarcurvature right and left, the point
located at the facialinsertion of each alar base; 6, columella, the
midpointon columella at the level of the superior
nostrils(landmarks 8 and 9); 7, subnasale, the midpoint onthe
nasolabial soft-tissue contour between thecolumella crest and the
upper lip; 8 and 9: nostril superiorright and left, the most
superior points of the nostril;10 and 11, nostril inferior right
and left, the most inferiorpoints of the nostril; 12 and 13,
nostril lateral rightand left, the most lateral points of the
nostril; 14 and 15,alar base right and left, the most lateral
points of thealar base.
Fig 4. The displacement vectors were normalized withthe
Frankfort horizontal plane coordinate system andrecorded as
positive values laterally in the x-axis, superi-orly in the y-axis,
and anteriorly in the z-axis.
408 Magnusson et al
displacements of the landmarks were calculated. Theerror of the
measurements was calculated by intraclasscorrelation coefficient
(ICC) for single measurements;this is an expression of
intraobserver reliability. An ICCabove 0.75 indicates excellent
reliability. The ICC valueswere between 0.851 and 0.992. Landmarks
1, 6, and 7 inthe midline showed the weakest ICC values.
Statistical analysis
Statistical analyses were undertaken using theStatistical
Package for the Social Sciences III (version20.0; SPSS, Chicago,
Ill). The distribution of data wastested with the 1-sample
Kolmogorov-Smirnov test.The results showed normal distribution of
the data,but because of the sample size, nonparametric testswere
also warranted. Median values and percentileswere used to describe
the changes and distributions.The Wilcoxon signed rank
nonparametric test was usedto evaluate pretreatment and
posttreatment differences.The level of significance was set at P
\0.05. TheSpearman rho was applied to assess the
correlationsbetween the changes at the nose.
September 2013 � Vol 144 � Issue 3 American
RESULTS
There were in general significant widening andoverall anterior
and inferior displacement at the nose.
For the x-axis (lateral displacement, left and right),
alllandmarks at the alar wings showed lateral displacement(Table
I). The displacements on the left and right sideswere symmetrical
and most obvious at the lateral alarbases (Fig 3; landmarks 14 and
15). The amount ofdisplacement of the lateral alar bases
decreasedgradually toward pronasale and toward the facialinsertion
of the nostrils.
The most pronounced lateral change to the nostrilswas at the
utmost lateral point of the inner contour ofthe nostrils, which
decreased in the anterior and inferiordirections of the x-axis.
Landmarks 1, 6, and 7 in the midline (Fig 3) showedno
significant lateral displacements; neither did land-marks 10 and 11
at the most inferior point of the nostrils(Fig 3). There were
significant correlations (P \0.001)between the lateral
displacements at the alar wingsand between the lateral
displacements in the nostrils.
For the y-axis (superior and inferior displacement),most
landmarks showed moderate inferior displacement(Table I). The most
significant displacements, albeitminor, were found at pronasale and
subnasale (Fig 3;landmarks 1 and 7). The amounts of displacement
atpronasale and subnasale decreased gradually in theposterior and
lateral directions on the y-axis.
For the z-axis (anterior and posterior displacement),the most
significant and obvious displacement occurred
Journal of Orthodontics and Dentofacial Orthopedics
-
Fig 5. A, The shortest distances without orientation in space
were measured for nose height(landmarks 1 and 7), nose width I
(landmarks 2 and 3), nose width II (landmarks 4 and 5), and
nosewidth III (landmarks 14 and 15); B, and for nostril length
(landmarks 8 and 10, and 9 and 11), nostrilwidth I (landmarks 12
and 13), and nostril width II (landmarks 10 and 11).
Table I. Median displacements and changes at the nose measured
at 15 landmarks (in mm) (Fig 3)
Landmark
X-axis Y-axis Z-axis
Medianchange p10 p90
Wilcoxontest
Medianchange p10 p90
Wilcoxontest
Medianchange p10 p90
Wilcoxontest
1 0.11 �0.64 0.86 NS �0.26 �1.40 0.28 z 0.03 �0.14 0.80 y2 1.10
0.06 1.89 z �0.25 �1.34 1.23 NS 0.46 �1.23 2.28 *3 0.70 �0.13 1.91
z �0.04 �1.85 1.04 NS 0.63 �0.72 2.39 z4 0.59 �0.62 2.16 y �0.27
�1.84 1.06 NS 1.14 �0.17 2.82 z5 0.58 �1.22 1.85 * �0.48 �1.91 1.11
* 1.18 �0.40 3.45 z6 0.10 �0.54 1.38 NS �0.11 �1.20 0.61 NS 0.41
�0.59 2.04 y7 0.09 �1.22 1.20 NS �0.51 �2.28 0.59 y 0.07 �1.32 1.41
NS8 0.42 �0.47 1.67 NS �0.20 �1.52 1.00 NS 0.26 �0.36 1.57 y9 �0.10
�1.44 1.00 NS �0.35 �1.29 0.62 * 0.22 �0.50 1.31 *
10 0.35 �1.32 2.26 NS �0.19 �1.49 1.23 NS 0.85 �0.85 1.94 z11
0.29 �1.04 1.87 NS �0.12 �1.47 0.76 NS 1.07 �0.23 2.37 z12 0.81
�0.42 2.40 z 0.48 �1.79 0.71 y 0.18 �2.06 1.44 NS13 0.67 �0.33 1.76
z 0.47 �1.43 1.10 * 0.43 �0.94 2.12 y14 1.47 0.30 2.90 z 0.10 �1.12
1.66 NS 1.36 0.05 2.76 z15 1.41 0.46 2.60 z �0.04 �1.62 1.03 NS
1.98 0.37 3.25 z
Displacements were recorded as positive values laterally in the
x-axis, superiorly in the y-axis, and anteriorly in the z-axis.p10,
10th percentile; p90, 90th percentile; NS, nonsignificant.*P\0.05;
yP\0.01; zP\0.001.
Magnusson et al 409
anteriorly (Table I), particularly at landmarks near thefacial
insertion (Fig 3; landmarks 4, 5, 10, 11, 14, and15). This anterior
displacement was, however, notevident at subnasale (Fig 3; landmark
7), which showeda contrasting, posterior displacement.
The Euclidean distance (the shortest distancebetween 2
landmarks) was analyzed and calculated forheight and width of the
nose and nostrils (Fig 5; TableII). Nose height, measured between
pronasale andsubnasale (Fig 5, A), remained unchanged, but a
American Journal of Orthodontics and Dentofacial Orthoped
significant and evident widening was apparent at thealar wings
and alar base (Fig 5, A; nose width I, nosewidth III). The nose
width at the facial insertion persistedunchanged (Fig 5, A; nose
width II). A significantwidening of the nostrils was obvious at the
lateral alarwings (Fig 5, B; nostril width I) but not at the
lowestpoint (Fig 5, B; nostril width II). The nostril
lengthremained unchanged. No correlation was foundbetween the
initial and final widths of the nose, orbetween the initial and
final widths of the nostrils.
ics September 2013 � Vol 144 � Issue 3
-
Table II. Median changes between landmarks withoutorientation in
space (in mm) (Fig 5)
Medianchange p10 p90
Wilcoxontest
Nose height(landmarks 1 and 7)
0.18 �1.38 2.15 NS
Nose width I(landmarks 2 and 3)
1.66 0.27 3.13 *
Nose width II(landmarks 4 and 5)
1.01 �0.65 2.72 NS
Nose width III(landmarks 14 and 15)
3.09 1.56 4.70 y
Nostril height(landmarks 8 and 10,9 and 11)
�0.47 �1.12 0.83 NS
Nostril width I(landmarks 12 and 13)
1.47 �0.08 3.19 y
Nostril width II(landmarks 10 and 11)
0.68 �1.51 2.29 NS
p10, 10th percentile; p90, 90th percentile; NS,
nonsignificant.*P\0.01; yP\0.001.
410 Magnusson et al
DISCUSSION
The results show that after SARME there is a true 3Dchange in
the nose: not only widening of the nose, butalso anterior and
inferior displacement of the wholenasomaxillary complex. The
displacements vary in sizeand direction, and the complexity of the
changes isdifficult to assess without a valid and reliable
method.
The computed tomography models and the refined3D methodology
used in this study, with volumetricregistration based on the
anterior cranial base, offerprecise and accurate superimpositions,
which areessential for quantifying and determining
spatialdisplacements. The vectors were normalized with theFrankfort
horizontal plane coordinate system, whichallows analysis of changes
in each direction. The 3Dbreakdown of the changes facilitates
greater under-standing of the variations and might offer
someindication of possible causes. Displacements withoutorientation
in space were used to estimate and correlatethe magnitude of
changes.
A crucial factor for correct analysis is the validity
andreliability of the measurements: ie, the accuracy of theselected
landmarks and the error of the measurements.Landmarks for
measurement were selected to show thedisplacements in different
areas with good reliability. TheICC value was high (.0.977) for
extreme landmarks atthe inner andouter contours of the alarwings.
TheweakestICC scores, although still above 0.851, were for
landmarksin the midline (pronasale, columella, and subnasale).
A source of bias in measuring soft tissues is theirsoftness and
adaptability. The immediate postoperative
September 2013 � Vol 144 � Issue 3 American
swelling after SARME will subside within a few weeks,but
residual swelling will persist.41 To prevent this sourceof error,
the soft-tissue registration was done at the endof treatment, at a
mean of 18 months postoperatively.
The most obvious amount of widening was found atthe most lateral
alar base (Fig 5, A; nose width III), amean of 2.88 mm,
representing a mean increase of 9%of the initial width. Berger et
al25 reported an increasein the nasal base width of up to 2 mm, and
Ramieriet al27 found a mean widening of 1.4 mm. The wideningin our
study was more pronounced than the values inprevious studies. This
discrepancy cannot be readilyexplained but might be attributable to
such factors asvariations in surgical techniques or differences in
theaccuracy and reliability of the measuring methodsapplied in the
studies.
Because candidates for SARME are patients withtransverse
skeletal discrepancies, it would be logical toexpect most changes
to occur in a transverse direction.The results showed lateral
displacements, but thesewere accompanied by anterior and inferior
displace-ments. A possible and rational explanation is
theoccurrence of corresponding displacements in the softand hard
tissues. According to Chung et al42 and Bretoset al,43 the anterior
displacement in our study could berelated to the anterior
displacement of the underlyingskeletal structures. However,
Lagrav�ere et al44 foundno evidence for either anterior or inferior
skeletaldisplacement after SARME. To resolve such contradic-tory
findings, further studies are warranted, applyingappropriate modern
measuring techniques to documentmaxillary displacement after SARME
and correlationswith soft-tissue changes.
The soft-tissue changes not only are thus related tothe extent
or direction of the skeletal displacements,but also are more likely
multifactorial consequences ofdifferent elements, such as the
surgical technique, theamount of soft tissues, the facial type, or
a gain or lossin weight. It is nevertheless important for the
clinicianto be aware of soft-tissue changes associated withSARME.
Ideally, it should be possible to predict thetreatment outcome to
prevent unwanted side effects.
On the x-axis, the most significant displacementswere found at
the lateral parts of the nose, primarily atthe alar base (Fig 3;
landmarks 14 and 15), secondarilyat the lateral alar wings (Fig 3;
landmarks 2 and 3),and less significantly, at the insertions of the
alar wings(Fig 3; landmarks 4 and 5). No significant lateral
changeswere found in the midsagittal plane.
The difference in lateral displacements between thelateral
landmarks played an essential role in theperception of a more
rounded shape and an increasedsize of the nose. This, combined with
more circular
Journal of Orthodontics and Dentofacial Orthopedics
-
Magnusson et al 411
nostrils, made the nostrils more visible in the frontal viewand
gave a sense of an increased nasolabial angle, eventhough an
overall anterior and inferior displacement ofthe nasomaxillary
complex was evident. This outcomemight be attributable to the
surgical technique used.The osteotomies were performed on the
maxillary lateralwalls, from the piriform aperture to the pterygoid
plates,including detachment of the mucosa and soft tissue onthe
nasal floor and lateral walls. The detachment ofsoft tissues at the
insertion of the alar wings (Fig 3; land-marks 4 and 5) might
explain why this displacement wasmuch less pronounced than that in
the attached softtissues at the lateral alar bases (Fig 3;
landmarks 14and 15).
Whether this widening and the overall anterior andinferior
displacement of the nose are beneficial to thepatient is a clinical
judgment. The main purpose of thesurgical techniques available for
controlling the widthof the nose is to diminish the width at the
anterior inser-tions of the alar wings and nostrils. These
techniques donot take into account the widening at the
attachedlateral alar base.45 Such a procedure should be usedwith
caution after SARME when there is a risk of anunesthetic
accentuated rounding of the anterior nose.
The most statistically significant changes were foundin the
anterior direction (z-axis). The changes were inmost cases quite
minor, but the uniformity in directionand the significance
nevertheless demonstrate anteriormovement of the nose. The
magnitude of the anteriordisplacements varied but, in accordance
with the lateraldisplacement on the x-axis, was most obvious at
themost lateral alar base (Fig 3; landmarks 14 and 15).
The displacements on the y-axis were less significant,small, and
varied in direction and can perhaps be relatedto factors other than
the effects of SARME. The mostsignificant displacements on the
y-axis were found atsubnasale and pronasale. We found no
correlationbetween the initial and final nostril widths, or
betweenthe initial and final nose widths. This lack of
correlationhighlights the complexity of all affected
components.There is, however, a clear tendency toward overall
lateral,anterior, and inferior displacement of the nose;
theclinician should take these into account in
treatmentplanning.
Some measurements were of particular note. Theheight of the nose
measured from subnasale topronasale as well as the length of the
nostrils remainedunchanged. These findings indicate increased
nostrilarea associated with widening of the nostrils. Thechange in
nostril shape from a narrow slit to a moreovoid or circular form
postoperatively was obvious andsignificant. In this context, it is
of interest that narrownostrils are associated with nasal
obstruction,46 and
American Journal of Orthodontics and Dentofacial Orthoped
widening is associated with a subjective perception ofimproved
nasal function.4 Consequently, patients withnarrow and constrained
nostrils benefit from thesoft-tissue changes.
These data consisted of measurements of displace-ments at
specific digitized landmarks at the nose. TheDi2Mesh software
application can, without landmarks,also analyze any specified
displacement and visualizethe displacements using a color map. The
colorvisualization of the displacements in this softwareshowed
major changes in the paranasal region. Thesechanges were not
analyzed because of the lack ofreliable and valid landmarks in this
area, but they willhave an indirect impact on the appearance of the
noseand the midface. Furthermore, at the time of registra-tion,
uncertain lip posture precluded evaluation ofchanges to the upper
lip.
With respect to radiation exposure, it is importantthat ethical
aspects are addressed, not only in thecontext of clinical studies,
but also in routine practice.Radiation exposure should always
follow the “as lowas reasonably achievable” principle.47 In this
study, theassessed risk of radiation exposure was weighed
againstachieving the required information: a 3D assessment
ofchanges to the external shape and form of the nose. Thesample
comprised nongrowing patients scheduled toundergo SARME; additional
2D images would haveincreased their radiation dose but provided
only limitedor partial diagnostic information.
To secure a high diagnostic advantage in treatmentplanning, a
low-dose helical computed tomographymachine was used, with a
low-dose protocol. Cone-beam computed tomography scans would have
beenan acceptable alternative but were not available at thetime.
The submission to the board of ethics for approvalof the study
included a discussion of radiation exposure.
CONCLUSIONS
There were in general significant widening andoverall anterior
and inferior displacement of allnasomaxillary soft tissues.
The changes were most obvious laterally andanteriorly on the
x-axis and y-axis.
There was variety in the size of the displacements thatrounded
the shape of the nose in the frontal view.
Therewas significantwideningof thenostrils andan in-crease in
nostril area. Patients with narrow and constrainednostrils can
benefit from the soft-tissue changes.
There were no correlations between the initial andfinal widths
of the nostrils, or the initial and final widthsof the nose.
It is questionable whether an alar cinch suture willprevent
widening at the alar base.
ics September 2013 � Vol 144 � Issue 3
-
412 Magnusson et al
ACKNOWLEDGMENTS
We thank Gunvor Johansson for her excellentassistance; Mauricio
Reyes, head of the Medical ImageAnalysis group at the Institute for
Surgical Technologyand Biomechanics at the University of Bern,
Bern,Switzerland; Birgit Ljungquist, our statistician; andRune
Lindsten, head of the orthodontic department ofThe Institute for
Postgraduate Dental Education,J€onk€oping, Sweden.
REFERENCES
1. Northway WM, Meade JB Jr. Surgically assisted rapid
maxillaryexpansion: a comparison of technique, response, and
stability.Angle Orthod 1997;67:309-20.
2. Byloff FK, Mossaz CF. Skeletal and dental changes
followingsurgically assisted rapid palatal expansion. Eur J Orthod
2004;26:403-9.
3. Lehman JA Jr, Haas AJ, Haas DG. Surgical orthodontic
correctionof transverse maxillary deficiency: a simplified
approach. PlastReconstr Surg 1984;73:62-8.
4. Magnusson A, Bjerklin K, Nilsson P, Jonsson F, Marcusson A.
Nasalcavity size, airway resistance, and subjective sensation
aftersurgically assisted rapid maxillary expansion: a
prospectivelongitudinal study. Am J Orthod Dentofacial Orthop
2011;140:641-51.
5. Bishara SE, Staley RN. Maxillary expansion: clinical
implications.Am J Orthod Dentofacial Orthop 1987;91:3-14.
6. Brown GVI. The surgery of oral and facial diseases and
malforma-tions, their diagnosis and treatment, including plastic
surgicalreconstruction, 4th ed. Philadelphia: Lea & Febiger;
1938.
7. Betts NJ, Vanarsdall RL, Barber HD, Higgins-Barber K, Fonseca
RJ.Diagnosis and treatment of transverse maxillary deficiency.Int J
Adult Orthod Orthognath Surg 1995;10:75-96.
8. Bays RA, Greco JM. Surgically assisted rapid palatal
expansion: anoutpatient technique with long-term stability. J Oral
MaxillofacSurg 1992;50:110-3.
9. Matteini C, Mommaerts MY. Posterior transpalatal distraction
withpterygoid disjunction: a short-term model study. Am J
OrthodDentofacial Orthop 2001;120:498-502.
10. Koudstaal MJ, Poort LJ, van der Wal KG, Wolvius EB,
Prahl-Andersen B, Schulten AJ. Surgically assisted rapid
maxillaryexpansion (SARME): a review of the literature. Int J Oral
MaxillofacSurg 2005;34:709-14.
11. Magnusson A, Bjerklin K, Nilsson P, Marcusson A.
Surgicallyassisted rapid maxillary expansion: long-term
stability.Eur J Orthod 2009;31:142-9.
12. Baik HS, Kim SY. Facial soft-tissue changes in skeletal
Class IIIorthognathic surgery patients analyzed with 3-dimensional
laserscanning. Am J Orthod Dentofacial Orthop 2010;138:167-78.
13. Day CJ, Robert T. Three-dimensional assessment of the facial
softtissue changes that occur postoperatively in orthognathic
patients.World J Orthod 2006;7:15-26.
14. Rauso R, Tartaro G, Tozzi U, Colella G, Santagata M.
Nasolabialchanges after maxillary advancement. J Craniofac Surg
2011;22:809-12.
15. Ryckman MS, Harrison S, Oliver D, Sander C, Boryor
AA,Hohmann AA, et al. Soft-tissue changes after
maxillomandibularadvancement surgery assessed with cone-beam
computed
September 2013 � Vol 144 � Issue 3 American
tomography. Am J Orthod Dentofacial Orthop
2010;137(Supp):S86-93.
16. O'Ryan F, Schendel S. Nasal anatomy and maxillary surgery.
II.Unfavorable nasolabial esthetics following the Le Fort I
osteotomy.Int J Adult Orthod Orthognath Surg 1989;4:75-84.
17. Muradin MS, Seubring K, Stoelinga PJ, vd Bilt A, Koole
R,Rosenberg AJ. A prospective study on the effect of modified
alarcinch sutures and V-Y closure versus simple closing sutures
onnasolabial changes after Le Fort I intrusion and
advancementosteotomies. J Oral Maxillofac Surg 2011;69:870-6.
18. Westermark AH, Bystedt H, Von Konow L, Sallstrom KO.
Nasolabialmorphology after Le Fort I osteotomies. Effect of alar
base suture.Int J Oral Maxillofac Surg 1991;20:25-30.
19. Aldren C, Tolley NS. Further studies on nasal sensation of
airflow.Rhinology 1991;29:49-55.
20. Clarke RW, Jones AS. The distribution of nasal airflow
sensitivity innormal subjects. J Laryngol Otol 1994;108:1045-7.
21. Guenthner TA, Sather AH, Kern EB. The effect of Le Fort I
maxillaryimpaction on nasal airway resistance. Am J Orthod
1984;85:308-15.
22. Cole P. Nasal and oral airflow resistors. Site, function,
andassessment. Arch Otolaryngol Head Neck Surg 1992;118:790-3.
23. Ngan P, H€agg U, Yiu C, Merwin D, Wei SH. Soft tissue
anddentoskeletal profile changes associated with maxillary
expansionand protraction headgear treatment. Am J Orthod
DentofacialOrthop 1996;109:38-49.
24. Filho HN, Gonçales ES, Berrentin-Felix G, de Souza C�esar
U,Acĥja GL. Evaluation of the facial soft tissues following
surgicallyassistedmaxillary expansion associated with the simple
V-Y suture.Int J Adult Orthod Orthognath Surg 2002;17:89-97.
25. Berger JL, Pangrazio-Kulbersh V, Thomas BW, Kaczynski
R.Photographic analysis of facial changes associated with
maxillaryexpansion. Am J Orthod Dentofacial Orthop
1999;116:563-71.
26. Ramieri GA, Spada MC, Nasi A, Tavolaccini A, Vezzetti
E,Tornincasa S, et al. Reconstruction of facial morphology from
laserscanned data. Part I: reliability of the technique.
DentomaxillofacRadiol 2006;35:158-64.
27. Ramieri GA, Nasi A, Dell'acqua A, Verze L. Facial soft
tissuechanges after transverse palatal distraction in adult
patients. IntJ Oral Maxillofac Surg 2008;37:810-8.
28. Jacobs JD, Bell WH, Williams CE, Kennedy JW 3rd. Control of
thetransverse dimension with surgery and orthodontics. Am J
Orthod1980;77:284-306.
29. Podesser B, Williams S, Bantleon HP, Imhof H. Quantitation
oftransverse maxillary dimensions using computed tomography:
amethodological and reproducibility study. Eur J Orthod
2004;26:209-15.
30. Cureton SL, Cuenin M. Surgically assisted rapid palatal
expansion:orthodontic preparation for clinical success. Am J
OrthodDentofacial Orthop 1999;116:46-59.
31. Glassman AS, Nahigian SJ, Medway JM, Aronowitz HI.
Conserva-tive surgical orthodontic adult rapid palatal expansion:
sixteencases. Am J Orthod 1984;86:207-13.
32. Cevidanes LH, Styner MA, Proffit WR. Image analysis
andsuperimposition of 3-dimensional cone-beam computed tomog-raphy
models. Am J Orthod Dentofacial Orthop 2006;129:611-8.
33. Cevidanes LH, Motta A, Proffit WR, Ackerman JL, Styner M.
Cranialbase superimposition for 3-dimensional evaluation of
soft-tissuechanges. Am J Orthod Dentofacial Orthop
2010;137(Supp):S120-9.
34. Belden CJ. The skull base and calvaria. Adult and
pediatric.Neuroimaging Clin N Am 1998;8:1-20.
Journal of Orthodontics and Dentofacial Orthopedics
http://refhub.elsevier.com/S0889-5406(13)00562-3/sref1http://refhub.elsevier.com/S0889-5406(13)00562-3/sref1http://refhub.elsevier.com/S0889-5406(13)00562-3/sref1http://refhub.elsevier.com/S0889-5406(13)00562-3/sref2http://refhub.elsevier.com/S0889-5406(13)00562-3/sref2http://refhub.elsevier.com/S0889-5406(13)00562-3/sref2http://refhub.elsevier.com/S0889-5406(13)00562-3/sref3http://refhub.elsevier.com/S0889-5406(13)00562-3/sref3http://refhub.elsevier.com/S0889-5406(13)00562-3/sref3http://refhub.elsevier.com/S0889-5406(13)00562-3/sref4http://refhub.elsevier.com/S0889-5406(13)00562-3/sref4http://refhub.elsevier.com/S0889-5406(13)00562-3/sref4http://refhub.elsevier.com/S0889-5406(13)00562-3/sref4http://refhub.elsevier.com/S0889-5406(13)00562-3/sref4http://refhub.elsevier.com/S0889-5406(13)00562-3/sref5http://refhub.elsevier.com/S0889-5406(13)00562-3/sref5http://refhub.elsevier.com/S0889-5406(13)00562-3/sref6http://refhub.elsevier.com/S0889-5406(13)00562-3/sref6http://refhub.elsevier.com/S0889-5406(13)00562-3/sref6http://refhub.elsevier.com/S0889-5406(13)00562-3/sref7http://refhub.elsevier.com/S0889-5406(13)00562-3/sref7http://refhub.elsevier.com/S0889-5406(13)00562-3/sref7http://refhub.elsevier.com/S0889-5406(13)00562-3/sref8http://refhub.elsevier.com/S0889-5406(13)00562-3/sref8http://refhub.elsevier.com/S0889-5406(13)00562-3/sref8http://refhub.elsevier.com/S0889-5406(13)00562-3/sref9http://refhub.elsevier.com/S0889-5406(13)00562-3/sref9http://refhub.elsevier.com/S0889-5406(13)00562-3/sref9http://refhub.elsevier.com/S0889-5406(13)00562-3/sref10http://refhub.elsevier.com/S0889-5406(13)00562-3/sref10http://refhub.elsevier.com/S0889-5406(13)00562-3/sref10http://refhub.elsevier.com/S0889-5406(13)00562-3/sref10http://refhub.elsevier.com/S0889-5406(13)00562-3/sref11http://refhub.elsevier.com/S0889-5406(13)00562-3/sref11http://refhub.elsevier.com/S0889-5406(13)00562-3/sref11http://refhub.elsevier.com/S0889-5406(13)00562-3/sref12http://refhub.elsevier.com/S0889-5406(13)00562-3/sref12http://refhub.elsevier.com/S0889-5406(13)00562-3/sref12http://refhub.elsevier.com/S0889-5406(13)00562-3/sref13http://refhub.elsevier.com/S0889-5406(13)00562-3/sref13http://refhub.elsevier.com/S0889-5406(13)00562-3/sref13http://refhub.elsevier.com/S0889-5406(13)00562-3/sref14http://refhub.elsevier.com/S0889-5406(13)00562-3/sref14http://refhub.elsevier.com/S0889-5406(13)00562-3/sref14http://refhub.elsevier.com/S0889-5406(13)00562-3/sref15http://refhub.elsevier.com/S0889-5406(13)00562-3/sref15http://refhub.elsevier.com/S0889-5406(13)00562-3/sref15http://refhub.elsevier.com/S0889-5406(13)00562-3/sref15http://refhub.elsevier.com/S0889-5406(13)00562-3/sref15http://refhub.elsevier.com/S0889-5406(13)00562-3/sref16http://refhub.elsevier.com/S0889-5406(13)00562-3/sref16http://refhub.elsevier.com/S0889-5406(13)00562-3/sref16http://refhub.elsevier.com/S0889-5406(13)00562-3/sref17http://refhub.elsevier.com/S0889-5406(13)00562-3/sref17http://refhub.elsevier.com/S0889-5406(13)00562-3/sref17http://refhub.elsevier.com/S0889-5406(13)00562-3/sref17http://refhub.elsevier.com/S0889-5406(13)00562-3/sref17http://refhub.elsevier.com/S0889-5406(13)00562-3/sref18http://refhub.elsevier.com/S0889-5406(13)00562-3/sref18http://refhub.elsevier.com/S0889-5406(13)00562-3/sref18http://refhub.elsevier.com/S0889-5406(13)00562-3/sref19http://refhub.elsevier.com/S0889-5406(13)00562-3/sref19http://refhub.elsevier.com/S0889-5406(13)00562-3/sref20http://refhub.elsevier.com/S0889-5406(13)00562-3/sref20http://refhub.elsevier.com/S0889-5406(13)00562-3/sref21http://refhub.elsevier.com/S0889-5406(13)00562-3/sref21http://refhub.elsevier.com/S0889-5406(13)00562-3/sref21http://refhub.elsevier.com/S0889-5406(13)00562-3/sref22http://refhub.elsevier.com/S0889-5406(13)00562-3/sref22http://refhub.elsevier.com/S0889-5406(13)00562-3/sref23http://refhub.elsevier.com/S0889-5406(13)00562-3/sref23http://refhub.elsevier.com/S0889-5406(13)00562-3/sref23http://refhub.elsevier.com/S0889-5406(13)00562-3/sref23http://refhub.elsevier.com/S0889-5406(13)00562-3/sref23http://refhub.elsevier.com/S0889-5406(13)00562-3/sref24http://refhub.elsevier.com/S0889-5406(13)00562-3/sref24http://refhub.elsevier.com/S0889-5406(13)00562-3/sref24http://refhub.elsevier.com/S0889-5406(13)00562-3/sref24http://refhub.elsevier.com/S0889-5406(13)00562-3/sref24http://refhub.elsevier.com/S0889-5406(13)00562-3/sref24http://refhub.elsevier.com/S0889-5406(13)00562-3/sref24http://refhub.elsevier.com/S0889-5406(13)00562-3/sref25http://refhub.elsevier.com/S0889-5406(13)00562-3/sref25http://refhub.elsevier.com/S0889-5406(13)00562-3/sref25http://refhub.elsevier.com/S0889-5406(13)00562-3/sref26http://refhub.elsevier.com/S0889-5406(13)00562-3/sref26http://refhub.elsevier.com/S0889-5406(13)00562-3/sref26http://refhub.elsevier.com/S0889-5406(13)00562-3/sref26http://refhub.elsevier.com/S0889-5406(13)00562-3/sref27http://refhub.elsevier.com/S0889-5406(13)00562-3/sref27http://refhub.elsevier.com/S0889-5406(13)00562-3/sref27http://refhub.elsevier.com/S0889-5406(13)00562-3/sref28http://refhub.elsevier.com/S0889-5406(13)00562-3/sref28http://refhub.elsevier.com/S0889-5406(13)00562-3/sref28http://refhub.elsevier.com/S0889-5406(13)00562-3/sref29http://refhub.elsevier.com/S0889-5406(13)00562-3/sref29http://refhub.elsevier.com/S0889-5406(13)00562-3/sref29http://refhub.elsevier.com/S0889-5406(13)00562-3/sref29http://refhub.elsevier.com/S0889-5406(13)00562-3/sref30http://refhub.elsevier.com/S0889-5406(13)00562-3/sref30http://refhub.elsevier.com/S0889-5406(13)00562-3/sref30http://refhub.elsevier.com/S0889-5406(13)00562-3/sref31http://refhub.elsevier.com/S0889-5406(13)00562-3/sref31http://refhub.elsevier.com/S0889-5406(13)00562-3/sref31http://refhub.elsevier.com/S0889-5406(13)00562-3/sref32http://refhub.elsevier.com/S0889-5406(13)00562-3/sref32http://refhub.elsevier.com/S0889-5406(13)00562-3/sref32http://refhub.elsevier.com/S0889-5406(13)00562-3/sref33http://refhub.elsevier.com/S0889-5406(13)00562-3/sref33http://refhub.elsevier.com/S0889-5406(13)00562-3/sref33http://refhub.elsevier.com/S0889-5406(13)00562-3/sref33http://refhub.elsevier.com/S0889-5406(13)00562-3/sref34http://refhub.elsevier.com/S0889-5406(13)00562-3/sref34
-
Magnusson et al 413
35. Melsen B. Time of closure of the spheno-occipital
synchondrosisdetermined on dry skulls. A radiographic craniometric
study.Acta Odontol Scand 1969;27:73-90.
36. Bookstein FL. Principle warps: thin-plate splines and
thedecomposition of deformations. IEEE Trans Pattern Anal
MachIntell 1989;11:567-85.
37. Kim H, Jurgens P, Weber S, Nolte LP, Reyes M. A new
soft-tissuesimulation strategy for cranio-maxillofacial surgery
usingfacial muscle template model. Prog Biophys Mol Biol
2010;103:284-91.
38. Swennen GRJ. 3-D cephalometric soft tissue landmarks.
In:Swennen GRJ, Schutyser F, Hausamen JE, editors.
Three-dimensional cephalometry. Berlin, Germany:
Springer-Verlag;2006. p. 183-226.
39. Yamada T, Mori Y, Minami K, Mishima K, Sugahara T, Sakuda
M.Computer aided three-dimensional analysis of nostril
forms:application in normal and operated cleft lip patients. J
Cranioma-xillofac Surg 1999;27:345-53.
40. Xia J, Wang D, Samman N, Yeung RW, Tideman H.
Computer-assisted three-dimensional surgical planning and
simulation: 3Dcolor facial model generation. Int J Oral Maxillofac
Surg 2000;29:2-10.
American Journal of Orthodontics and Dentofacial Orthoped
41. Nooreyazdan M, Trotman CA, Faraway JJ. Modeling
facialmovement: II. A dynamic analysis of differences caused
byorthognathic surgery. J Oral Maxillofac Surg 2004;62:1380-6.
42. Chung CH, Woo A, Zagarinsky J, Vanarsdall RL, Fonseca
RJ.Maxillary sagittal and vertical displacement induced by
surgicallyassisted rapid palatal expansion. Am J Orthod Dentofacial
Orthop2001;120:144-8.
43. Bretos JL, Pereira MD, Gomes HC, Toyama Hino C, Ferreira
LM.Sagittal and vertical maxillary effects after surgically
assisted rapidmaxillary expansion (SARME) using Haas and hyrax
expanders.J Craniofac Surg 2007;18:1322-6.
44. Lagrav�ere MO, Major PW, Flores-Mir C. Dental and
skeletalchanges following surgically assisted rapid maxillary
expansion.Int J Oral Maxillofac Surg 2006;35:481-7.
45. Millard DR Jr. The alar cinch in the flat, flaring nose.
Plast ReconstrSurg 1980;65:669-72.
46. Hinton VA, Warren DW, Hairfield WM, Seaton D. The
relationshipbetween nasal cross-sectional area and nasal air volume
in normaland nasally impaired adults. Am J Orthod Dentofacial
Orthop1987;92:294-8.
47. Radiation and your patient: a guide for medical
practitioners. AnnICRP 2001;31:5-31.
ics September 2013 � Vol 144 � Issue 3
http://refhub.elsevier.com/S0889-5406(13)00562-3/sref35http://refhub.elsevier.com/S0889-5406(13)00562-3/sref35http://refhub.elsevier.com/S0889-5406(13)00562-3/sref35http://refhub.elsevier.com/S0889-5406(13)00562-3/sref36http://refhub.elsevier.com/S0889-5406(13)00562-3/sref36http://refhub.elsevier.com/S0889-5406(13)00562-3/sref36http://refhub.elsevier.com/S0889-5406(13)00562-3/sref37http://refhub.elsevier.com/S0889-5406(13)00562-3/sref37http://refhub.elsevier.com/S0889-5406(13)00562-3/sref37http://refhub.elsevier.com/S0889-5406(13)00562-3/sref37http://refhub.elsevier.com/S0889-5406(13)00562-3/sref38http://refhub.elsevier.com/S0889-5406(13)00562-3/sref38http://refhub.elsevier.com/S0889-5406(13)00562-3/sref38http://refhub.elsevier.com/S0889-5406(13)00562-3/sref38http://refhub.elsevier.com/S0889-5406(13)00562-3/sref39http://refhub.elsevier.com/S0889-5406(13)00562-3/sref39http://refhub.elsevier.com/S0889-5406(13)00562-3/sref39http://refhub.elsevier.com/S0889-5406(13)00562-3/sref39http://refhub.elsevier.com/S0889-5406(13)00562-3/sref40http://refhub.elsevier.com/S0889-5406(13)00562-3/sref40http://refhub.elsevier.com/S0889-5406(13)00562-3/sref40http://refhub.elsevier.com/S0889-5406(13)00562-3/sref40http://refhub.elsevier.com/S0889-5406(13)00562-3/sref41http://refhub.elsevier.com/S0889-5406(13)00562-3/sref41http://refhub.elsevier.com/S0889-5406(13)00562-3/sref41http://refhub.elsevier.com/S0889-5406(13)00562-3/sref42http://refhub.elsevier.com/S0889-5406(13)00562-3/sref42http://refhub.elsevier.com/S0889-5406(13)00562-3/sref42http://refhub.elsevier.com/S0889-5406(13)00562-3/sref42http://refhub.elsevier.com/S0889-5406(13)00562-3/sref43http://refhub.elsevier.com/S0889-5406(13)00562-3/sref43http://refhub.elsevier.com/S0889-5406(13)00562-3/sref43http://refhub.elsevier.com/S0889-5406(13)00562-3/sref43http://refhub.elsevier.com/S0889-5406(13)00562-3/sref44http://refhub.elsevier.com/S0889-5406(13)00562-3/sref44http://refhub.elsevier.com/S0889-5406(13)00562-3/sref44http://refhub.elsevier.com/S0889-5406(13)00562-3/sref44http://refhub.elsevier.com/S0889-5406(13)00562-3/sref45http://refhub.elsevier.com/S0889-5406(13)00562-3/sref45http://refhub.elsevier.com/S0889-5406(13)00562-3/sref46http://refhub.elsevier.com/S0889-5406(13)00562-3/sref46http://refhub.elsevier.com/S0889-5406(13)00562-3/sref46http://refhub.elsevier.com/S0889-5406(13)00562-3/sref46http://refhub.elsevier.com/S0889-5406(13)00562-3/sref47http://refhub.elsevier.com/S0889-5406(13)00562-3/sref47
Three-dimensional computed tomographic analysis of changes to
the external features of the nose after surgically assisted r
...Material and methodsStatistical analysis
ResultsDiscussionConclusionsAcknowledgmentsReferences