Embed Size (px)
Citation preview

Current Best Practices in Prevention
July 20, 2011
James Emshoff, Ph.D.Georgia State University
EMSTAR Research, Inc.

July 20, 2011
We Will Be Starting Shortly
Welcome

WELCOME!
CAPT Southeast Resource Team
Shannon GreerIT Specialist Iris E. Smith
Coordinator
Charline McCordT/TA Coordinator
Penny DeaversT/TA Specialist, GRAA
Carol A. HagenEpidemiologist
Carlos PavaoT/TA Specialist
Deirdre DanaharT/TA Specialist
LaShawn Martin
Sr. Admin Assistant
Bertha GorhamEvaluator
Donna DentAssociate
Coordinator

Welcome to Connect Pro
• We will be using the following windows:– PowerPoint Window– Attendee List– Chat– Note
• We will also use the
“Raise your Hand” feature
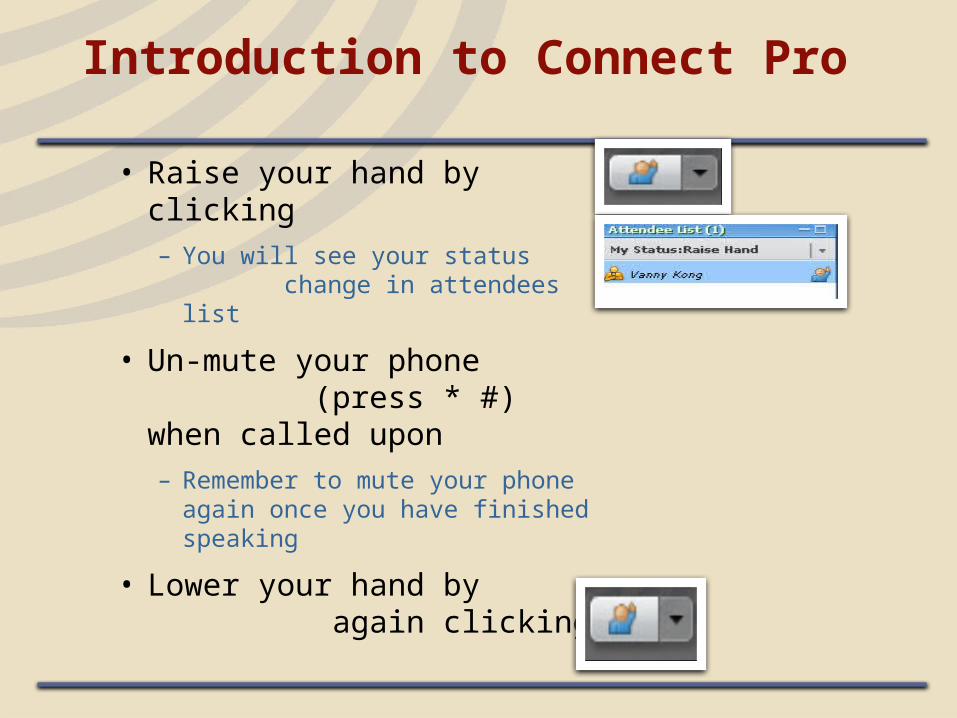
Introduction to Connect Pro
• Raise your hand by clicking– You will see your status
change in attendees list
• Un-mute your phone (press * #) when called upon– Remember to mute your phone
again once you have finished speaking
• Lower your hand by again clicking

Asking Questions in Connect Pro
• By Writing:
– Write question in Chat window
– Press enter
– Only the moderator will see the question

Learning Objectives
• By the end of this webinar, participants will be able to:– Describe current research and trends in
prevention science
– Describe processes, content, and principles to enhance the effectiveness of prevention programs.
– Discuss examples of evidence-based prevention programs and practices that employ these processes, content and principles.

Rationale for Prevention
• We believe in the logic – “a stitch in time…” “an ounce of prevention…”
• If early initiation can be prevented, it is likely that lifetime addiction can be prevented.
• The cost of alcohol and drug use in our society is $485 billion.

But It’s Still an Uphill Battle . . .
• You can’t see what doesn’t happen
• Costs now – benefits later
• Crisis mentality
• Political resistance

The Premise of Prevention Science
To prevent a problem before it happens, the factors that predict the problem must be changed.

Two Major Advancesin Prevention Science
• Identification of predictors of problem behaviors as targets for prevention
• Identification of tested and effective preventive policies and programs
Principles

Promotive and Protective Factors
• Individual CharacteristicsHigh IntelligenceResilient TemperamentCompetencies and Skills

Promotive and Protective Factors
• In social domains of family, school, peer group and neighborhood:Pro-social opportunitiesReinforcement for pro-social involvementBonding (connectedness, attachment)Clear and healthy standards for behavior

Promotive and Protective Factors (con’t.)
• In social domains of family, school, peer group and neighborhood:Opportunities for learning ChildcareGood schools (i.e., high spending, good
teachers, low student-teacher ratios, moderate size, supportive learning, small work units)
Health care• Most important when risk factors are high

16
Risk Factors forAdolescent Problem Behaviors
XExtreme Economic Deprivation
Low Neighborhood Attachment and
Community Disorganization
Transitions and Mobility
Media Portrayals of Violence
Community Laws and Norms Favorable Toward Drug Use, Firearms, and Crime
Availability of Firearms
axe
XAvailability of Drugs
Community
Dep
ressio
n &
A
nxie
ty
Vio
len
ce
Sch
ool D
rop
-O
ut
Teen
P
reg
nan
cy
Delin
qu
en
cy
Su
bsta
nce
Ab
use
Risk Factors

School Risk Factors
• Academic failure – beginning in late elementary school
• Lack of commitment to school• Exposure to violence and drug use

Family Risk Factors
• Family history• Family management problems• Family conflict – low family involvement• Favorable parental attitudes and low monitoring

Individual Risk Factors (Childhood)
• Difficult temperament• Poor self-regulation• Sensation-seeking• Impulsive• Low harm avoidance• Anxiety• Depression• ADHD• ANY adverse childhood experiences or trauma
(especially child maltreatment or family disruption)
Individual/Peer Risk Factors (Adolescence)
• Deviant peers• Rejection by peers• Low commitment to school • School failure• Access and availability• Perceived norms • Negative emotions• Conduct disorder• Anti-social behavior

Individual Risk Factors (Young Adulthood)
• College• Antisocial behavior• Lack of commitment to
traditional adult roles

Underage Drinking
• Risks start at ages 3-5, as children exposed to alcohol, norms, parental modeling, and associated positive expectancies
• Later, role of peers increases• Prevention strategies:
– Raising the drinking age– Raising prices– Limiting media and family exposure– Monitoring

One Risk Factor–Multiple Outcomes
• Most substance abuse risk factors also predict: – Delinquency– Violence– School drop-out– Teen pregnancy– Depression and anxiety (more family, less
community)

One Program – Multiple Outcomes
• Preventive interventions that address shared risk factors for different adolescent health risk behaviors have produced reductions in multiple outcomes, including school dropout, drug use and crime.
Hawkins et al, 1999; Botvin et al., 2002 ; Flay et al, 2004; Haggerty et al., 2007; Schweinhart et al, 1992; 2005

Risk and Protective Factor Models
• Main effects – cumulative and direct• Moderating (e.g., the presence of a protective
factor can moderate the effect of a risk factor; a genetic factor may exacerbate a risk factor)
• Mediating – chains of events (e.g., poverty leads to ineffective parenting and/or living in disorganized neighborhoods which leads to problem behaviors)

How to Reduce Risk Factor Effects
• Change the experience (e.g., teach coping)• Change exposure• Avert negative chain reactions• Increase protective factors• Change settings

Programs, Policies, and Practices
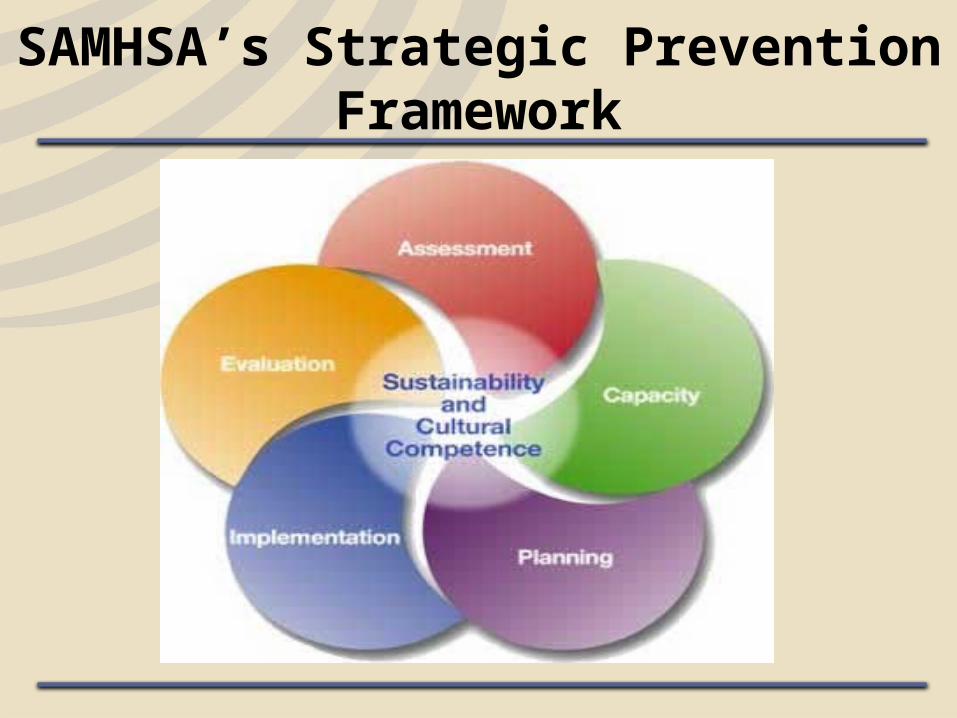
SAMHSA’s Strategic Prevention Framework

Preventive Intervention Opportunities
29

Prevention Programs
• Universal programs reach the general population (such as all students in a school).
• Selective programs target individuals or groups at elevated risk (such as children of drug users or poor school achievers).
• Indicated programs focus on people who exhibit some symptoms of a disorder but not a diagnosable “case”.
• Tiered programs incorporate two or more levels of intervention, with increasing intensity for individuals at greater risk.

School-Based Prevention
• Schools are the most widely used setting for prevention
• Schools provide access to children and adolescents
• Programming should be developmentally appropriate
• Effective programming has been identified at all grades

Effective School-Based Prevention
• Is interactive• Focuses on social influences• Emphasizes norms and social commitment• Has a community component• Uses peer leaders• Uses life skills

Strategies that Do Not Work
• Information only • Testimonials from recovered addicts• Scare tactics• Affective education (e.g., self-esteem building
only)• Alternative programming (e.g., recreation
programs without skills training)

Raising Healthy Children
• Teacher in-service training– Classroom management– Interactive teaching– Cooperative learning
• Parent workshops– Raising healthy children – behavioral principles– Supporting school success– Guiding good choices, refusal and decision-making
• Child social, cognitive and emotional skills training (e.g., problem solving, emotional regulation)
Core components

Outcomes
• By the start of fifth grade, students exposed to full intervention reported:
less initiation of alcohol less initiation of delinquency better family management better family communication
Outcomes (cont.)
• By the start of fifth grade, students exposed to full intervention reported:
improved family involvement higher attachment to family higher school rewards higher school bonding

Longer-Term OutcomesControls vs. Intervention Youth
• By age 18: Less heavy alcohol use (25% to 15%)Less lifetime violence (60% to 48%)Less grade repetition (23% to 14%)
• By age 21:– More high school graduates (81% vs. 91%)– More attending college (6% vs. 14%)– Fewer selling drugs (13% vs. 4%)– Fewer with a criminal record (53% to 42%)

38
0%
10%
20%
30%
40%
50%
60%
70%
11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
Age
Cum
ulati
ve O
nset
Tx
Sig. effect on STI Hazard rate, p < 0.019
Control
Full Tx
Effects on Sexually Transmitted Infection Onset through Age 30
38.8%
26.2%

Investment in Raising Healthy Children Reduces Costs of Later Problems
$1.00
$3.14
Aos et al. (2004)
Investment Return
Community and Environmental Change
• Mass media campaigns are a part of the solution (Derzon et al, 2002) Alcohol use reduced from 53% to 51%Tobacco use reduced from 37% to 35%Marijuana use reduced from 24% to 22%Videos work bestTarget parentsInclude supplementary activitiesMore effective for males
• Coalitions have promise

Community and Environmental Change
• Restriction of outlet density and zoning • Enhanced enforcement of sales to minors• Limiting marketing, especially youth-oriented
marketing

Community-Level Intervention
• Communities Mobilizing for Change Changed policies Focused on alcohol outlets selling to youth Reduced access from family and friends Changed norms Reduced access and teen DUIs

Community-Level Intervention
• Community Trials Community mobilization Responsible beverage service Increased enforcement of drunk driving laws Reduced underage access Changed zoning and outlet access EFFECTS: Reduced alcohol-related injuries
and deaths
Safe Schools/Healthy Students (SS/HS) Initiative
• Launched in 1999 as a comprehensive response to address the mental, emotional, and behavioral health of students and to make sure kids felt safe in their schools.
• Represents an unprecedented collaboration between the U.S. Departments of Health and Human Services, Education, and Justice
• Has served more than 365 grantees comprising schools and communities across the nation

SS/HS Goals
• Requires school districts to partner with their local mental health, juvenile justice, and law enforcement agencies
• Harnesses the power of schools, local agencies, and community partners to ensure that students:Feel safe in schools, free from violence and
bullying Avoid drugs, alcohol, and violence Have increased access to mental health servicesDon’t feel isolated, because they can connect with
their schools and communities

Findings
• Schools and communities became safer and fewer students were exposed to violence
• A large number of school staff said they were better able to detect mental health issues in their students and also saw reductions in students’ alcohol and drug use
• Longstanding “silos” were broken down as schools began working closely with community agencies

The SBIRT Concept
• SBIRT uses a public health approach to universal screening for substance use problems.
• SBIRT provides:Immediate rule out of non-problem users;Identification of levels of risk;Identification of patients who would benefit
from brief advise, and;Identification of patients who would benefit
from higher levels of care.

The Problem

Primary Goal
• The primary goal of SBIRT is not to identify those who are dependent and need higher levels of care.
• The primary goal of SBIRT is to identify those who are at moderate or high risk for psycho-social or health care problems related to their substance use choices.


Learning from Health Care
The health care system routinely screens for potential medical problems (cancer, diabetes, hypertension), provides preventative services prior to the onset of acute symptoms, and delays or precludes the development of chronic conditions.

SBriefInterventionRT
• Low Risk: Brief Advice• Moderate risk: Brief Intervention based on Motivational
Interviewing• High risk: BI + on site brief therapy
SBIReferralTreatment• Possible dependance: BI plus referral to treatment

Alcohol and Drug Use DecreasedSix Months After Receiving at Least a Brief Intervention
8.0
4.7
6.2
4.2
1.7
3.2
0.0
2.0
4.0
6.0
8.0
10.0
Alcohol Use* Binge Drinking* Drug Use*
Before BeforeBeforeAfter After After
*p < .05
Day
s of
Use
in L
ast
30 D
ays
Multi-level, Multi-modal Intervention
• Midwestern Prevention Program (Pentz et al)Classroom curriculumParent trainingDevelopment of a community task forceMedia campaignReduced tobacco and marijuana – effects
expand over time

Multi-level, Multi-modal Intervention
• Project NorthlandCommunity organizingYouth action teamsMedia campaignParent training School curriculumPrevented 8th grade drinking, tobacco,
marijuana

“Interventions designed to prevent mental, emotional and behavioral disorders and problems and those designed to promote mental, emotional and behavioral health both frequently involve directly strengthening children’s competencies and positive mental health or strengthening families, schools or communities. However, improved knowledge pertaining to the conceptualization and assessment of developmental competencies is needed to better inform interventions.”
National Research Council & Institute of Medicine (2009). Preventing Mental, Emotional, and Behavioral Disorders Among Young People. Pg. 110


Prevention of Substance Abuse and Mental Illness
• Goal 1.1: Build emotional health, prevent or delay onset of, and mitigate symptoms and complications from substance abuse and mental illness.
• Goal 1.2: Prevent or reduce consequences of underage drinking and adult problem drinking.
• Goal 1.3: Prevent suicides and attempted suicides among populations at high risk, especially military families, youth, and American Indians and Alaska Natives.
• Goal 1.4: Reduce prescription drug misuse and abuse.

Trauma and Justice
• Goal 2.1: Develop a comprehensive public health approach to trauma.
• Goal 2.2: Make screening for trauma and early intervention and treatment common practice.
• Goal 2.3: Reduce the impact of trauma and violence on children, youth, and families.
• Goal 2.4: Address the needs of people with mental and substance use disorders and with histories of trauma within the criminal and juvenile justice systems.
• Goal 2.5: Reduce the impact of disasters on the behavioral health of individuals, families, and communities.

Military Families
• Goal 3.1: Improve Military Families’ access to community-based behavioral health care through coordination with TRICARE, Department of Defense, or Veterans Health Administration services.
• Goal 3.2: Improve quality of behavioral health prevention, treatment, and recovery support services by helping providers respond to the needs and culture of Military Families.
• Goal 3.3: Promote the behavioral health of Military Families with programs and evidence-based practices that support their resilience and emotional health.
• Goal 3.4: Develop an effective and seamless behavioral health service system for Military Families through coordination of policies and resources across Federal, national, State, Territorial, local, and Tribal organizations.

Health Care Reform Implementation
• Goal 4.1: Assure behavioral health is included in all aspects of Health Care Reform (HCR) implementation.
• Goal 4.2: Support Federal, State, and Territorial efforts to develop and implement new provisions under Medicaid/Medicare.
• Goal 4.3: Finalize and implement the parity provisions in Mental Health Parity and Addictions Equity Act and the Affordable Care Act.
• Goal 4.4: Develop changes in SAMHSA Block Grants to support recovery and resilience.
• Goal 4.5: Foster the integration of primary and behavioral health care.

Housing and Homelessness
• Goal 5.1: Prevent homelessness among individuals with mental and substance use disorders.
• Goal 5.2: Create permanent stable housing for behavioral health populations.
• Goal 5.3: Implement supportive housing services.

Health Information Technology
• Goal 6.1: Foster provider adoption and implementation of Electronic Health Records (EHR).
• Goal 6.2: Promote behavioral health EHR standards.
• Goal 6.3: Address issues of behavioral health privacy/confidentiality in EHR.
• Goal 6.4: Engage State and Territorial HIT leaders to develop and disseminate behavioral health functionality within provider EHR systems.

Data, Outcomes, and Quality
• Goal 7.1: Implement an integrated approach for SAMHSA’s collection, analysis, and use of data.
• Goal 7.2: Create common standards for measurement and data collection to better meet stakeholder needs.
• Goal 7.3: Improve the quality of SAMHSA’s program evaluations and services research.
• Goal 7.4: Improve quality and accessibility of surveillance, outcome/performance, and evaluation information for SAMHSA staff, stakeholders, funders, and policymakers.

Public Awareness and Support
• Goal 8.1: Increase capacity for Americans to understand and to access treatment and recovery supports for behavioral health conditions.
• Goal 8.2: Create a cohesive SAMHSA identity and media presence.
• Goal 8.3: Lead the field through communication around SAMHSA’s Strategic Initiatives and HHS Priorities
• Goal 8.4: Get information to the workforce.
• Goal 8.5: Increase social inclusion and reduce discrimination.

Dissemination and Implementation
• Large gap between what we know and what we do
• Research often not fully translated into widespread practice
• Need to learn more about marketing and adoption decisions
• Dissemination and adoption without effective implementation does not lead to outcomes
Conclusion
• Treatment is 7 times more cost effective than domestic law enforcement, 10 times more effective than interdiction, and 23 times more effective than the "source control" method. (RAND, 1994)
• If treatment is this cost-effective, what if we can prevent the need for treatment?
• http://www.wsipp.wa.gov/rptfiles/04-07-3901.pdf - cost benefit analysis

Other Resources and Lists of Drug Abuse Prevention Programs and Policies
• NREPP http://nrepp.samhsa.gov/AdvancedSearch.aspx
• NIDA’s town hall -http://www.nida.nih.gov/drugpages/prevention.html
• Blueprints for Violence Prevention www.colorado.edu/cspv/blueprints/
• Safe Schools Healthy Students http://www.sshs.samhsa.gov/initiative/commercial.aspx
Preventing Mental, Emotional and Behavioral Disorders Among Young People:
Progress and Possibilities
O’Connell, M.E., Boat, T. & Warner, K.E. (2009). Washington D.C. National Academies Press.

Thank You for Participating!
CAPT Southeast Service Area Resource Team
Shannon GreerIT Specialist
Iris E. SmithCoordinator
Charline McCordT/TA Coordinator
Penny DeaversT/TA Specialist
Carol HagenEpidemiologist
Carlos PavaoT/TA Specialist
Deirdre DanaharT/TA Specialist
LaShawn MartinSenior Administrative
Assistant
Bertha GorhamEvaluator
Donna DentAssociate Coordinator
Contact Information
LaShawn Martin
Senior Administrative Assistant, Southeast Resource Team
Center for the Application of Prevention Technologies
678-954-5824