Embed Size (px)
Citation preview

Current and Future Assessment, Identification,
and Intervention: Going from the Model T to the Tesla
(Part 2)
Paul Beljan, PsyD, ABPdN, ABNJustin Gardner, PsyDDustin Howard, PsyD

Acknowledgements & DeclarationsCenter for Clinical Systems Biology, Rochester General HospitalGordon Broderick, PhD
Cole Lyman, MS
Beljan Psychological ServicesPaul Beljan, PsyD, ABPdN, ABN
Midwestern University, GlendaleJessica Powell, PsyDThomas Virden, III, PhD
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The authors have no business affiliations and are not using this presentation to promote any products.
The opinions and assertions contained herein are the private views of the author and are not to be construed as official or as reflecting the views of Beljan Psychological Services, Midwestern University, Glendale, or Rochester Regional Health 2

Flow of Material
3
TreatmentComputational ModelingAutismNeuropsychology

Pediatric Neuropsychologythe state of the field1

Working with the Model T
5
Diagnosis
Using normative data and clinical judgment to identify a disorder
TreatmentProviding a list of potential treatment recommendations
02
01

Bringing out the Tesla
6
DiagnosisUsing normative data, clinical judgment, and
process analysis to identify a disorder
TreatmentProviding tailoredtreatment recommendations for maximal outcomes
Predictive ModelingMaximizing diagnostic accuracy and refining individualized neuropsychological dynamics
03
01 02

MultidisciplinaryDrawing on knowledge from different disciplines, each staying within their own boundaries
Integrating Specialties
TransdisciplinaryIntegrating the disciplines in a context that transcends each one’s traditional boundaries
7Choi & Pak, 2006

Autism Spectrum Disordercomputational modeling in context2

1/59Children in the US are diagnosed with ASD
$11.5 trillionLifetime social cost by 2029 given exponential increase in incidence
$3.6 millionLifetime social cost per person
9Baoi et al., 2018

Autism Throughout History
10
1 3 5
42
Leo Kanner (1943)
Hans Asperger (1944)
DSM-IVAutism
Asperger’s
Childhood Disintegrative D/O
PDD-NOS
Transdisciplinary
Approaches
Childhood
Psychopathy
DSM-5
Spectrum (Continuum)

ASD & the DSM-5⬢ Persistent deficits in
social communication and social interaction⬡ Social-emotional
reciprocity⬡ Non-verbal
communication⬡ Developing relationships
⬢ Restricted, repetitive patterns of behavior, interests, or activities⬡ Stereotypy⬡ Insistence on sameness⬡ Restricted and fixated
interests⬡ Hyper- or hypo-
reactivity to sensory input
11APA, 2013

Severity⬢ Level 1:
RequiringSupport
⬢ Level 2: RequiringSubstantial Support
⬢ Level 3: Requiring Very Substantial Support
12APA, 2013
“Neurotypical” vs “Neurodivergent”Call it what it is – a disorder

But Wait, There’s More!DSM-5 nosology of ASD is a good place to start, but it is not the end-all be-all
Clinicians must utilize expertise and deductive reasoning (and maybe
some math) to fill in the rest
13

Diagnostic MethodsObservationGARS-3
Poor SensitivityFair Specificity
ADI-RHigh SensitivityPoor Specificity
ADOS-2Adequate AccuracyDecent inter-Rater Reliability
NeuropsychologyNEPSY-II
Low Theory of Mind scoreLow Affect Recognition score
<WISC-V><Low FSIQ score?><Higher PIQ than VIQ?>Bx Observations and Process
MedicineGenetics
NRXNNLGNSHANK
NeuroanatomyDLPFCCerebellumLocalized overconnectivity
14Carlson et al., 2017
Zander et al., 2015
McCrimmon et al., 2014
Woodbury-Smith & Sherer, 2018)
Floris et al., 2018
Dawson et al., 2007
Brooks et al., 2010

Treatment ModalitiesMedicationAtypical Antipsychotics (irritability)
Stimulants (inattention)
Alpha2A-Adrenergics (inattention)
Serotonergics (emotional/behavioral)
*Used only to manage secondary symptoms of ASD
TherapyApplied Behavior Analysis (ABA) to shape adaptive and social behaviors
Psychotherapy to treat social/emotional sequelae
Social Skills Training to emulate non-ASD social skills
*The most research-backed treatment modalities to remediate ASD-like
behaviors
15

“Early intervention is only half
the battle
16

Issues with the Model T⬢ Vaguely defined
constructs⬡ i.e., “Reciprocity”?
⬡ Low focus on the process of how constructs are produced in the brain
⬢ Disjointed measures⬡ GARS/ADI-R/ADOS
⬢ Poor disciplinary overlap⬡ SLP
⬡ Psychology
⬡ Medicine
⬢ Variable diagnostic accuracies⬡ AUC
⬡ Reliability
⬢ Poorly defined quanta⬡ “Spectrum” = Dartboard!
⬢ Generalized treatment recommendations⬡ “See a psychiatrist”
⬡ “See a therapist”
⬢ Non-time dependent course of treatment⬡ “Do these whenever
and however”
17

Computational Modelingthe Tesla3

“There are likely to be new advances in assessment
technology, but not assessment philosophy
19
Harvey, 2012

Bridging the GapPsychologists should integrate advanced mathematics, graph theory, and data visualization in research and clinical practice
⬡ More accurate diagnostics⬡ More individualized treatment recommendations⬡ Greater ability to track treatment progress
20Parsons & Duffield, 2020

Computational Modeling MethodsBlack Box Models
Probabilistic outcomes are based solely on the nature of inputs (i.e., machine learning)
*High Interpolation*Sensitive to data used
White Box ModelsHow the internal structure of systems affect the identification of an output, based on 1st principles
*High extrapolation*Good with sparse data
21
First Principles Models
A basic proposition that starts directly at the level
of established laws*Deductive Reasoning*
22

Mechanistic Modeling and ASD: The AimsTo develop a mechanistic model of neuropsychological
regulation with the capacity for identifying and explaining the neuropsychological impairment of individuals with ASD, informing clinical diagnostics, and predicting dynamic
treatment recommendations tailored for maximal restoration of neuropsychological functioning
23

LET’S REVIEW SOME CONCEPTSMechanicsA system in which a function exists that transforms inputs into outputs through deterministic methods
DynamicsA mechansitic system in which a function describes the time dependence of variables
RegulationThe mechanistic interaction that explains dynamical shifts in the homeostasis of a network
24
Maximal OutcomesThe most efficient path of attaining the best possible treatment outcomes given the initial condition and available treatments

Principles of Regulatory ModelingA. System processes occur as part of a highly integrated closed-loop network of elements which interact in specific logical manners to produce complex behaviors
B. Network models are robust and have built-in redundancies and complementary functions to compensate for disturbances
C. Human mechanistic regulatory network models can describe illness dynamics with varying levels of granularity
25Broderick & Craddock, 2013

26

27
Healthy Resting
Chronic illness
Healthy Resting
Chronic illness
Chronic illness
Healthy Resting
Non-Illness PerturbationGenetics
EnvironmentTeratogens
Illness
Homeostatics

28
Closed loop systems are adherent to a relatively stable homeostatic fluctuation unless perturbed by a significant outside force
Healthy Resting
Chronic illness
Healthy Resting
Chronic illness
Chronic illness
Healthy Resting
Non-ASD Perturbation ASD
Autism Homeostatics

How to Get There
29
Network Model
CreationAttractor
LandscapeNetwork
Model Validation
Develop a circuit diagram of neuropsychological regulation using text-mining and domain expertise with specified constraints
Ground model & compare it against sample data to determine fidelity of hypothesis-driven network
Assess the resultant attractor landscape to determine allowable homeostatic states

30
Nodes:
A
B
C
D
Edges:
A upregulates BA upregulates CB upregulates DB downregulates CC downregulates DD downregulates A
A B C D
GAD 0 1 -1 1
MDD 1 -1 0 -1
Parameterization
1 = up-regulated (high)
0 = nominal (average)
-1 = down-regulated (low)
Hypothetical Network CreationNote: Such formalism
allows you to approximate
dynamics without detailed
kinetic information

31
HPG Axis Network Creation
Nodes:Hypothalamus
GnRH
LH
FSH
Testosterone
Edges:Hypothalamus → GnRHGnRH → LHGnRH → FSHLH → TestosteroneFSH → TestosteroneTestosterone → FSHTestosterone → LHTestosterone → Hypothalamus
Hypothalamus
GnRH
FSH
Testosterone
LH
Hypo GnRH LH FSH Test
GAD 0 1 -1 1 -1
MDD 1 -1 0 -1 1
Parameterization
1 = up-regulated (high)
0 = nominal (average)
-1 = down-regulated (low)

32Gardner et al., 2021
Psychoneuroimmunology of PTSD
Sleep
Neurotransmitters
Brain Regions
Cytokines
Psych
Physiology
Neuropsych
Neuropsychological Functioning for Symptoms of ASD?
33

AIMS
34
TREATMENT
STRUCTURE
DIAGNOSTICS
DYNAMICS
AUTISM
Is there a model of neuropsychological regulation?Can the model explain dynamic relaxation trajectories?Can the model predict a stable attractor space coinciding with ASD?

Network Model Creation⬢ Neuropsychological Nodes⬢ Neuropsychological Regulations⬢ Prior Knowledge Support
35

36
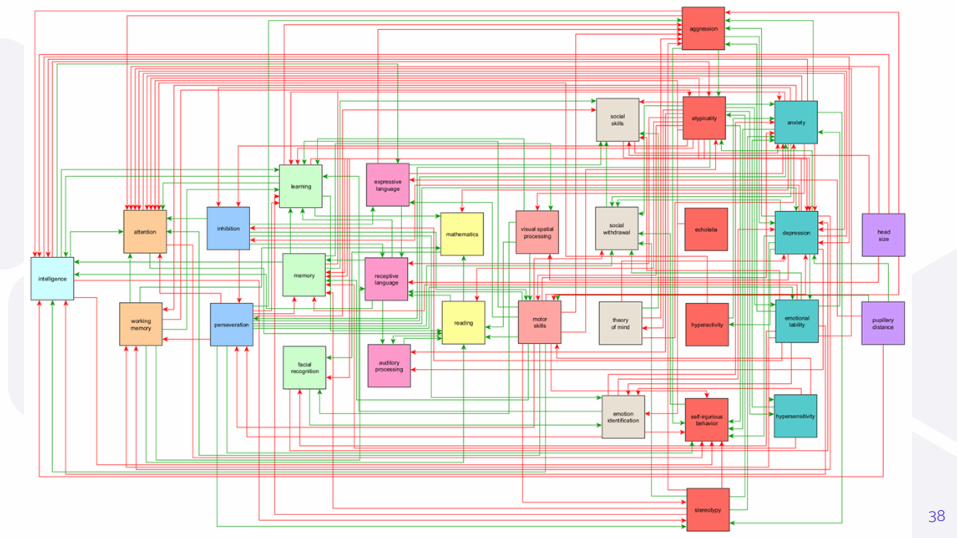
Neuropsychological Domains Model Nodes
Intelligence Intelligence Quotient
Attention Attention
Working Memory
Executive Functioning Inhibition
Perseveration
Learning/Memory Learning
Memory
Facial Recognition
Language Expressive Language
Receptive Language
Auditory Processing
Academics Mathematics
Reading
Visual-Motor Visual-Spatial Processing
Motor Skills
Social Social Skills
Social Withdrawal
Theory of Mind
Emotion Identification
Behavioral Aggression
Atypicality
Echolalia
Hyperactivity
Self-Injurious Behavior
Stereotypy
Psychological Anxiety
Depression
Emotional Lability
Hypersensitivity
Biological Head Size
Pupillary Distance
Neuropsychological Nodes
31 total variables (“nodes”)
Text Mining
37Retrieved from https://www.Elsevier.com
38
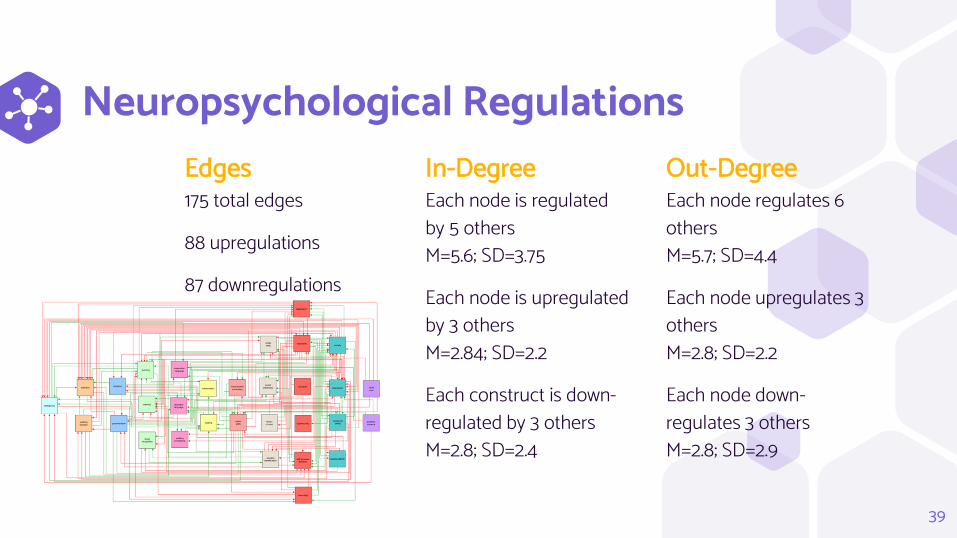
Neuropsychological RegulationsEdges175 total edges
88 upregulations
87 downregulations
In-DegreeEach node is regulated by 5 othersM=5.6; SD=3.75
Each node is upregulated by 3 others M=2.84; SD=2.2
Each construct is down-regulated by 3 others M=2.8; SD=2.4
Out-DegreeEach node regulates 6 others M=5.7; SD=4.4
Each node upregulates 3 othersM=2.8; SD=2.2
Each node down-regulates 3 othersM=2.8; SD=2.9
39
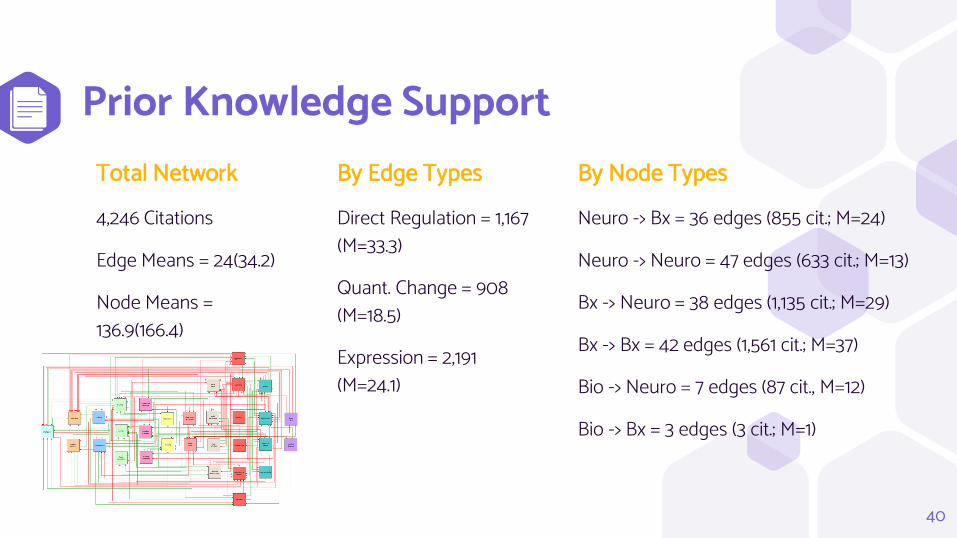
Prior Knowledge SupportTotal Network4,246 Citations
Edge Means = 24(34.2)
Node Means = 136.9(166.4)
By Edge TypesDirect Regulation = 1,167 (M=33.3)
Quant. Change = 908 (M=18.5)
Expression = 2,191 (M=24.1)
By Node TypesNeuro -> Bx = 36 edges (855 cit.; M=24)
Neuro -> Neuro = 47 edges (633 cit.; M=13)
Bx -> Neuro = 38 edges (1,135 cit.; M=29)
Bx -> Bx = 42 edges (1,561 cit.; M=37)
Bio -> Neuro = 7 edges (87 cit., M=12)
Bio -> Bx = 3 edges (3 cit.; M=1)
40

Network StructureFindings
Network Diameter: shortest distance between two most distant nodes = 5
Average Number of Neighboring Nodes: average number of nodes within one “jump” = 10.9
Connection Density: the ratio between the total number of edges compared to total possible number of edges = 0.19
InterpretationThe model is relatively dense with a high number of interactions
Constructs in neuropsychology are highly affected by changes in other domains
Changes in one neuropsychological domain cause rapid and widespreadchanges across all neuropsychological domains
41
Network MechanicsFindings
Closeness: how quickly information spreads from a given node to all other nodesBetweenness: the relative control a node has over the interaction of others (“bridge”)Authorities: those with high in-degreesHubs: those with high out-degrees
InterpretationAnxiety, Atypicality, and Depression cause the largest network-wide regulatory impactDepression, Anxiety, Attention, and Atypicality are the most common intermediaries (“bridges”)Attention, Self-Injurious Behavior, and Learning are highly dependent on changes in othersMotor Skills, Atypicality, and Perseveration cause the largest changes in others
42

Key Mechanistic Finding Results suggest the most important measures to assess when determining overall neuropsychological functioning in ASD are:
Attention Motor SkillsLearning AtypicalityPerseveration Self-Injurious Behavior
43

AIMS
44
TREATMENT
STRUCTURE
DIAGNOSTICS
DYNAMICS
AUTISM
Is there a model of neuropsychological regulation?Can the model explain dynamic relaxation trajectories?Can the model predict a stable attractor space coinciding with ASD?

Network Validation⬢ How well does the model explain clinical cases?
45

46
Node Level DesignationsAggression 0 = average; 1 = highAnxiety 0 = average; 1 = highAttention 0 = very low; 1 = low; 2 = averageAtypicality 0 = average; 1 = highAuditory Processing 0 = very low; 1 = averageDepression 0 = average; 1 = highEcholalia 0 = absent; 1 = presentEmotion Identification 0 = very low; 1 = low; 2 = averageEmotional Lability 0 = average; 1 = highExpressive Language 0 = low; 1 = averageFacial Recognition 0 = low; 1 = averageHead Size 0 = average; 1= largeHyperactivity 0 = average; 1 = highHypersensitivity 0 = average; 1 = highInhibition 0 = very low; 1 = low; 2 = averageIntelligence 0 = low; 1 = averageLearning 0 = low; 1 = averageMathematics 0 = very low; 1 = low; 2 = averageMemory 0 = low; 1 = averageMotor Skills 0 = low; 1 = averagePerseveration 0 = average; 1 = high; 2 = very highPupillary Distance 0 = average; 1 = wideReading 0 = very low; 1 = low; 2 = averageReceptive Language 0 = low; 1 = averageSelf-Injurious Behavior 0 = absent; 1 = presentSocial Skills 0 = very low; 1 = low; 2 = averageSocial Withdrawal 0 = average; 1 = highStereotypy 0 = absent; 1 = presentTheory of Mind 0 = very low; 1 = low; 2 = averageVisual Spatial Processing 0 = low; 1 = averageWorking Memory 0 = low; 1 = average
Logic
al Pa
ram
eter
s

Node LFE HFE Health Level Designations
Aggression 1 0 0 0 = average; 1 = highAnxiety 1 1 0 0 = average; 1 = highAttention 0 1 2 0 = very low; 1 = low; 2 = averageAtypicality 1 1 0 0 = average; 1 = highAuditory Processing 0 0 1 0 = very low; 1 = averageDepression 1 0 0 0 = average; 1 = highEcholalia 1 0 0 0 = absent; 1 = presentEmotion Identification 0 1 2 0 = very low; 1 = low; 2 = averageEmotional Lability 1 1 0 0 = average; 1 = highExpressive Language 0 1 1 0 = low; 1 = averageFacial Recognition 0 0 1 0 = low; 1 = averageHead Size 1 1 0 0 = average; 1= largeHyperactivity 1 0 0 0 = average; 1 = highHypersensitivity 1 1 0 0 = average; 1 = highInhibition 0 1 2 0 = very low; 1 = low; 2 = averageIntelligence 0 1 1 0 = low; 1 = averageLearning 0 1 1 0 = low; 1 = averageMathematics 0 1 2 0 = very low; 1 = low; 2 = averageMemory 0 1 1 0 = low; 1 = averageMotor Skills 0 0 1 0 = low; 1 = averagePerseveration 2 1 0 0 = average; 1 = high; 2 = very highPupillary Distance 1 1 0 0 = average; 1 = wideReading 0 1 2 0 = very low; 1 = low; 2 = averageReceptive Language 0 1 1 0 = low; 1 = averageSelf-Injurious Behavior 1 0 0 0 = absent; 1 = presentSocial Skills 0 1 2 0 = very low; 1 = low; 2 = averageSocial Withdrawal 1 1 0 0 = average; 1 = highStereotypy 1 1 0 0 = absent; 1 = presentTheory of Mind 0 1 2 0 = very low; 1 = low; 2 = averageVisual Spatial Processing 0 1 1 0 = low; 1 = averageWorking Memory 0 1 1 0 = low; 1 = average
Mode
l Con
strain
ts

Source of Validation Sets
48
Node Published
Pseudonym
Source
LF1 Case 2 Kanner, 1943; 1971
LF2 Case 3 Kanner, 1943; 1971
LF3 Case 4 Kanner, 1943; 1971
LF4 Case 5 Kanner, 1943; 1971
LF5 Case 7 Kanner, 1943; 1971
LF6 Case 9 Kanner, 1943; 1971
LF7 Case 11 Kanner, 1943; 1971
LF8 Hellmuth Asperger, 1944
HF1 Case 1 Kanner, 1943; 1971
HF2 Case 6 Kanner, 1943; 1971
HF3 Case 8 Kanner, 1943; 1971
HF4 Case 10 Kanner, 1943; 1971
HF5 Fritz Asperger, 1944
HF6 Harro Asperger, 1944
HF7 Ernst Asperger, 1944
Note:The model needs to be constrained by clinical cases of given disease states so it will adhere to observed pathological topologies

Validation Set Findings⬢ Low-Functioning ASD N=8⬢ High-Functioning ASD N=7
49
Note – The model is not
built on the 15 cases,
only validated on them. It
was built on the samples
used in over 4,000
research articles!
50
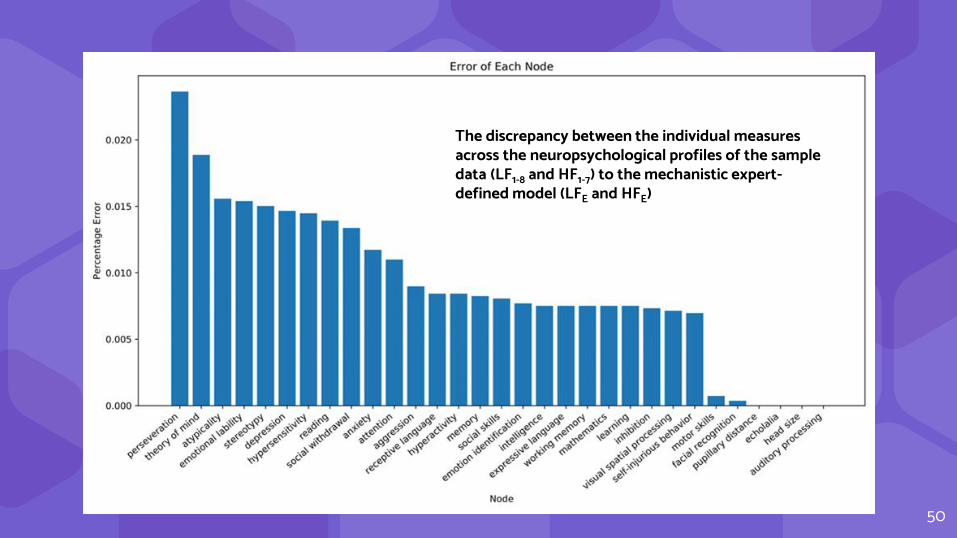
The discrepancy between the individual measures across the neuropsychological profiles of the sample data (LF1-8 and HF1-7) to the mechanistic expert-defined model (LFE and HFE)
51
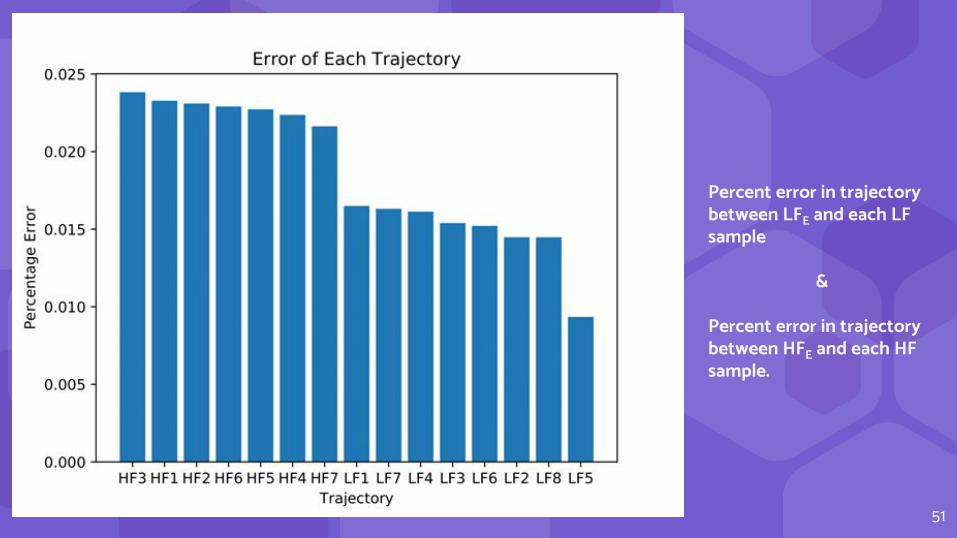
Percent error in trajectory between LFE and each LF sample
&
Percent error in trajectory between HFE and each HF sample.
ValidationFindings
⬢ Highest nodal error = perseveration (2.5%) and ToM(1.9%)
⬢ Most nodal errors were below 0.75%
⬢ Classification accuracy was 72.2%⬡ Not just of diagnosis, but
neuropsychological profiles of scores across all domains
Interpretation⬢ The model explains the
clinically observed fluctuations of functioning across time and environments
⬢ The model is highly reliable
⬢ The model has a high degree of sensitivity and specificity, and is much better with LF
52

AIMS
53
TREATMENT
STRUCTURE
DIAGNOSTICS
DYNAMICS
AUTISM
Is there a model of neuropsychological regulation?Can the model explain dynamic relaxation trajectories?Can the model predict a stable attractor space coinciding with ASD?

Attractor Landscaping⬢ How discrepant is the neuropsychological
functioning of ASD from non-ASD?
54

55
Attractor Spaces.Think: Einstein

56

57
Healthy Resting
Chronic illness
Healthy Resting
Chronic illness
Chronic illness
Healthy Resting
Non-ASD ASD
Autism Landscaping

Manhattan Distances
58
DA1 DA2 DA3 LFE HFE Health
DA1 0 26 5 17 26 26
DA2 26 0 12 39 18 0
DA3 5 21 0 20 23 21
LFE 17 39 20 0 21 39
HFE 26 18 23 21 0 18
Health 26 0 21 39 18 0
Note: the
maximum MD
is 40 bits
Attractor LandscapingFindings
⬢ Attractor search returned 3 undefined stable discovered attractors (DA1, DA2, DA3)
⬢ The most proximal to DA1 was LF (MD = 17)
⬢ The most proximal to DA2 was Health (MD = 0)
⬢ DA3 was too distant from HF
Interpretation⬢ The model can predict a set of
neuropsychological attractors proximal to health and low-functioning ASD
⬢ The model perfectly explains healthy neuropsychological functioning
⬢ The model explains a condition very similar to low-functioning ASD
59

Treatmentproviding the most efficient recommendations4

FUTURE AIMS
61
TREATMENT
STRUCTURE
DIAGNOSTICS
DYNAMICS
AUTISM
Is there a model of neuropsychological regulation?Can the model explain dynamic relaxation trajectories?Can the model predict a stable attractor space coinciding with ASD?Is there a mechanistic network model of ASD?Can the model inform individualized treatment recommendations?

Iterative Edge Cutting
62
Nodes:A
B
C
D
Edges:
A upregulates B
A upregulates C
B upregulates D
B downregulates C
C downregulates D
D downregulates A
Rice et al., 2016

Which to Cut/Re-Polarize?
63
DA1 LFE
DA1 0 0
LFE 0 0
DA3 HFE
DA3 0 0
HFE 0 0
LF ASD
HF ASD
64
Neuropsychological Emulation

FUTURE AIMS
65
TREATMENT
STRUCTURE
DIAGNOSTICS
DYNAMICS
AUTISM
Is there a model of neuropsychological regulation?
Can the model explain dynamic relaxation trajectories?
Can the model predict a stable attractor space coinciding with ASD?
Is there a mechanistic network model of ASD?
Can the model inform individualized treatment recommendations?

66
Healthy Resting
Chronic injury
Healthy Resting
Chronic injury
Chronic injury
Healthy Resting
Healthy Resting
Chronic injury
Healthy Resting
Chronic injury
Chronic injury
Healthy Resting
Therapeutic remodeling
Think: “Post-Traumatic Growth”

Monte Carlo Simulations⬢ The use of combinatory optimization
schemes to identify individualized treatments and their time course for maximal remittance of symptoms
67Craddock et al., 2015

Standard Treatment for ASD
68
Social
SkillsAnxiety ToM Motor Skills Attention
What’s a better way?

Most Effective Treatment Aims for ASD
69
Social
SkillsAnxiety ToM Motor Skills Attention
Anxiety ToM Motor Skills Attention
What’s an even better way?

Treatment Time Course
70
Attention Anxiety Motor Skills ToM
Anxiety ToM Motor Skills Attention
What’s an EVEN better way?

Compounding Complexity
71
Attention
TxRx
Rx 1 Rx 2 Tx 1 Tx 2
Anxiety Motor Skills ToM

The Benefit of Computational Modeling⬢ Merging clinical expertise with simple
deductive reasoning to enhance diagnostics and take treatment to the next level
⬢ All you need is the right tools! (and a bit of math)
72

Key Take-Awayslet’s sum it all up5

Key Take-Aways⬢ There is much untapped text-based clinical data in
published research, and text-mining can allow clinicians to synthesize a large amount of useful information
⬢ Most of what we know about the neuropsychological profile of ASD is within behavioral correlations (anxiety, depression, social skills, etc.), with little emphasis placed on neuropsychological or biological causatives
74

Key Take-Aways 2⬢ The proposed mechanistic model of neuropsychological
functioning demonstrated a 72% diagnostic accuracy⬢ The model perfectly explains healthy neuropsychological
functioning
75

Key Take-Aways 3⬢ The same “unbroken” neuropsychological circuitry explains
low-functioning ASD with a high degree of fidelity⬢ The underlying neuropsychological circuitry in ASD is not as
impaired as we think!⬢ Next step is to iteratively cut wires to ascertain a model that
perfectly explains ASD, thereby knowing which nodes and edges are unalterably affected
76

Key Take-Aways 4⬢ It may be possible to computationally derive treatment
methods for maximal emulation of typical neuropsychological functioning in children with ASD
⬢ There is a coming shift in which clinicians will begin moving away from traditional statistics into process-based predictive modeling
⬢ Such methods offer greater diagnostic efficiency and the ability to identify individualized treatment recommendations for maximal treatment outcomes
77

Final ConsiderationsStrengths
Quick
Comprehensive
Highly granular
Individualized
Efficient
LimitationsLimited extant neuropsychological & biological research support for ASD functioning (much more for behavioral observations)
Unavoidable noise (differing working definitions across fields)
Methodology is grounded in the DSM-5, but it extends beyond strict DSM-5 parameters
78

ReferencesAmerican Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing
Baoi, J., Wiggins, L., Christensen, D., … & Dowling, M. (2018). Prevalence of autism spectrum disorder among children aged 8 years: Autism and developmental disabilities monitoring network. Surveillance Summary, 67(6), 1-23. Retrieved from https://www.cdc.gov
Broderick, G., & Craddock, T.J. (2013). Systems biology of complex symptom profiles: Capturing interactivity across behavior, brain and immune regulation. Brain, Behavior, and Immunity, 29, 1-8. doi: 10.1016/j.bbi.2012.09.008
Broderick, G., Katz, B. Z., Fernandez, H., et al. (2012). Cytokine expression profiles of immune imbalance in post-mononucleosis chronic fatigue. Journal of Translational Medicine, 10(1). 191.
Brooks, B., Sherman, E., & Strauss, E. (2010). NEPSY-II: A Developmental Neuropsychological Assessment, 2nd Edition. Child Neuropsychology, 16, 80-81. doi: 10.1080/09297040903146966
Carlson, J., Geisinger, K., & Johnson, J. (2017). The Gilliam Autism Rating Scale, Third Edition (GARS-3). The Twentieth Mental Measurements Yearbook
Choi, B., & Pak, A. (2006). Multidisciplinary, interdisciplinary and transdisciplinary in health research, services, education and policy: Definitions, objectives, and evidence of effectiveness. Clinical and Investigative Medicine, 29(6), 351-364.
Craddock, T., Del Rosario, R., Rice, M., … & Broderick, G. (2015). Achieving remission in Gulf War illness: A simulation-based approach to treatment design. PLOSone. doi:10.1371/journal.pone.0132774
Craddock, T.J., Fritsch, P., Rice, M., Del Rosario, R., … & Broderick, G. (2014). A role for homeostatic drive in the perpetuation of chronic illness: Gulf war illness and chronic fatigue syndrome. PLOS One, 9(1). doi: 10.1371/journal.pone.0084839
Dawson, M., Soulieres, I, … & Mottron, L. (2007). The level and nature of autistic intelligence. Psychological Science, 18(8), 657-662. doi: 10.1111/j.1467-9280.2007.01954.x
Floris, D., & Howells, H. (2018). Atypical structural and functional motor networks in autism. Progress in Brain Research, 238, 207-248. doi: 10.1016/bs.pbr.2018.06.010
Folcik, V., Broderick, G., Mohan, S., …& Marsh, C. B. (2011). Using an agent-based model to analyze the mechanistic communication network of the immune response. Theoretical Biology and Medical Modelling, 8(1). http://www.tbiomed.com/content/8/1/1
79

References (cont.)Gardner, J., Toole, J. T., Kalia, H., Spink, G., & Broderick, G. (2021). Knowing what we know: Leveraging community knowledge through automated text-mining. Advances in Clinical Medical Research and Healthcare Delivery, 1(1). Retrieved from https://scholar.rochesterregional.org/advances/vol1/iss1/2
Harvey, P. (2012). Clinical applications of neuropsychological assessment. Dialogues in Clinical Neuroscience, 14(1), 91-99. doi: 10.31887/DCNS.2012.14.1/pharvey
Koziol, L.F., Beljan, P., Bree, K., et al. (2016). Large-Scale Brain Systems and Neuropsychological Testing: An Effort to Move Forward. Switzerland: Springer International Publishing
Koziol, L.F., Barker, L.A., Joyce, A.W., & Hrin, S. (2014). Large-scale brain systems and subcortical relationships: The vertically organized brain. Applied Neuropsychology Child, 3(4), 253-263. doi: 10.1080/2122965.2014.946804
McCrimmon, A. & Rostad, K. (2014). Test Review, Autism Diagnostic Observation Schedule, Second Edition (ADOS-2). Psychoeducational Assessment, 32(1), 88-92. Retrieved from https://journal-sagepub-com
Parsons, T., & Duffield, T. (2020). Paradigm shift toward digital neuropsychology and high-dimensional neuropsychological assessments: Review. Journal of Medical Internet Research, 22(12). Doi: 10.2196/23777
Toole, J.T., et al. (2018). Increasing resilience to traumatic stress: Understanding the protective role of well-being. In: Yan Q. (Eds). Psychoneuroimmunology: Methods in Molecular Biology, 1781. New York, NY: Humana Press
Webb, J., Beljan, P., et al. (2004). Misdiagnosis and Dual Diagnosis of Gifted Children and Adults: ADHD, Bipolar, OCD, Asperger’s, Depression, and Other Disorders, 2nd Ed. Tucson, AZ: Great Potential Press
Wechsler, D. (2014). WISC-V Administration and Scoring Manual. Bloomington, MN. NCS Pearson, Inc.
Weiss, L., Munoz, M., & Prifitera, A. (2016). Testing Hispanics with the WISC-V and WISC-IV. WISC-V Assessment and Interpretation Scientist-Practitioner Perspectives, 215-236
Woodbury-Smith, & Sherer, S. (2018). Progress in the genetics of autism spectrum disorder. Developmental Medicine & Child Neurology, 60, 445-451. doi: 10.1111/dmcn.13717
Zander, E., & Bolte, S. (2015). The added value of the combined use of the Autism Diagnostic Interview-Revised and the Autism Diagnostic Observation Schedule: Diagnostic validity in a clinical Swedish sample of toddlers and young preschoolers. Autism, 19(2), 187-199. doi: 10.1177/1362361313516199
80

Panel Discussion
81
Paul BeljanPsyD, ABPdN, ABN
Pediatric Neuropsychologist
Dustin HowardPsyD
Licensed Clinical Psychologist
Justin GardnerPsyD
Postdoctoral Fellow
1. Identify two subtle nuances in interpreting WISC V data2. Describe at least one way the WISC V is an appropriate measure
for Spanish-speaking bilingual children whose secondary language is English
3. Name a neuropsychologically based behavioral management method
4. List two principles components of a psychological evaluation that research suggests are most predictive in diagnosing Autism Spectrum Disorder (ASD)
5. Identify integrative and individualized treatment interventions in Autism Spectrum Disorder for maximal therapeutic outcomes
6. Identify two key benefits and limitations to utilizing novel computational approaches to the diagnostic and treatment process of complex pervasive psychological disorders

Feel Free to Contact Us!Paul Beljan, PsyD, ABPdN, ABNBeljan Psychological Services9835 E. Bell Rd., Ste. 140Scottsdale, AZ 85260(602) [email protected]
Dustin Howard, PsyDDesierto Psychological, PLLC(480) [email protected]
Justin Gardner, PsyDBeljan Psychological Services(602) [email protected]
82