Embed Size (px)
Citation preview
Abstracts / Pancreatology 13 (2013) S1–S80 S21
were excluded. The median time interval between the onset of AP andadmission was 24 (09:48) hours. According to KDIGO AKI criteria, patientswere divided into four groups: without AKI (n¼80) 53%, 1st stage (n¼35)23%, 2nd stage (n¼22) 14%, 3rd stage (n¼15) 10%.
Results: Significant differences (p<0.05) in severity condition (APACHEII, Ranson, SOFA scores) were found among all groups except for data be-tween groups with 2nd and 3rd stages (Table).
The 60-day Kaplan-Meier survival plot (Figure) shows a diversion ofthe survival rates among the groups (p¼0.000). There was no significantdifference between the groups without AKI and 1st stage (hospital mor-tality rates were 23% and 34% respectively, (p¼0.415)) compared to a largeincrease in mortality (early phase of disease) in groups with 2nd and 3rdstages (hospital mortality rates 64% and 60% respectively, (p¼0.727)).
Conclusions: The development of AKI (47% of the ICU patients with AP)is associated with worse clinical outcome. Timely recognition of severedisease and applying appropriate therapy (1st stage of AKI and earlier) areextremely important in management of patients with OF.
Keywords: Acute kidney injury and acute pancreatitis
[P-019].
CT findings reflecting Grey-Turner sign as predictors of outcomein acute pancreatitis
Yakubbay Abdullaev, Shamil Galeev, Michael Rubtsov,Oleg Skryabin, Shamil Galeev
General Surgery, Saint Luke Clinical Hospital, Saint Petersburg,Russian Federation
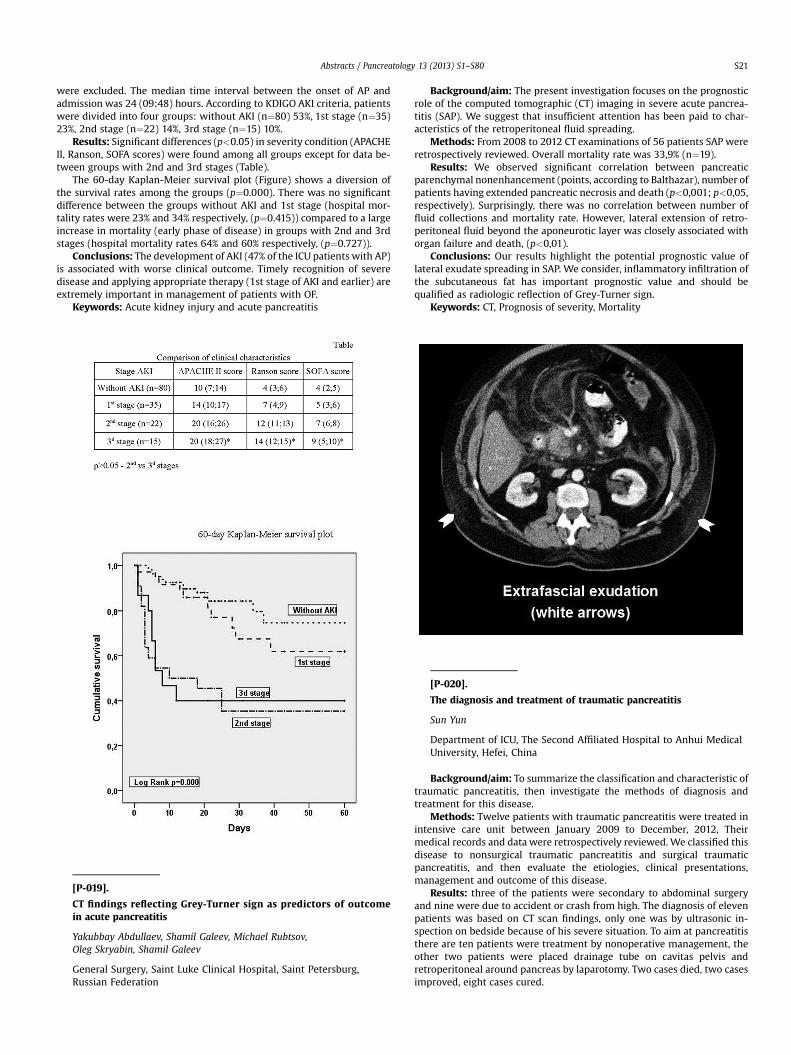
Background/aim: The present investigation focuses on the prognosticrole of the computed tomographic (CT) imaging in severe acute pancrea-titis (SAP). We suggest that insufficient attention has been paid to char-acteristics of the retroperitoneal fluid spreading.
Methods: From 2008 to 2012 CT examinations of 56 patients SAP wereretrospectively reviewed. Overall mortality rate was 33,9% (n¼19).
Results: We observed significant correlation between pancreaticparenchymal nonenhancement (points, according to Balthazar), number ofpatients having extended pancreatic necrosis and death (p<0,001; p<0,05,respectively). Surprisingly, there was no correlation between number offluid collections and mortality rate. However, lateral extension of retro-peritoneal fluid beyond the aponeurotic layer was closely associated withorgan failure and death, (p<0,01).
Conclusions: Our results highlight the potential prognostic value oflateral exudate spreading in SAP. We consider, inflammatory infiltration ofthe subcutaneous fat has important prognostic value and should bequalified as radiologic reflection of Grey-Turner sign.
Keywords: CT, Prognosis of severity, Mortality
[P-020].
The diagnosis and treatment of traumatic pancreatitis
Sun Yun
Department of ICU, The Second Affiliated Hospital to Anhui MedicalUniversity, Hefei, China
Background/aim: To summarize the classification and characteristic oftraumatic pancreatitis, then investigate the methods of diagnosis andtreatment for this disease.
Methods: Twelve patients with traumatic pancreatitis were treated inintensive care unit between January 2009 to December, 2012, Theirmedical records and data were retrospectively reviewed. We classified thisdisease to nonsurgical traumatic pancreatitis and surgical traumaticpancreatitis, and then evaluate the etiologies, clinical presentations,management and outcome of this disease.
Results: three of the patients were secondary to abdominal surgeryand nine were due to accident or crash from high. The diagnosis of elevenpatients was based on CT scan findings, only one was by ultrasonic in-spection on bedside because of his severe situation. To aim at pancreatitisthere are ten patients were treatment by nonoperative management, theother two patients were placed drainage tube on cavitas pelvis andretroperitoneal around pancreas by laparotomy. Two cases died, two casesimproved, eight cases cured.





























