Embed Size (px)
DESCRIPTION
Â
Citation preview

Crunch Time for Health in SandwellPublic Health Annual Report 2007/08
SandwellPrimary Care Trust
NHS

ContentsForeword 3
Crunch Time for Health in Sandwell 4
60 Years of the NHS 18
Healthy People and Towns 22
Working Towards Better Health and Wellbeing 27
Town Profiles 32
Achievements and Awards 44
Acknowledgements 46
Support CD 47
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell

Foreword Welcome to the 19th Public Health Annual Report for Sandwell. This gives anoverview of the state of Sandwell’s public health in 2007/08 and the work that isbeing carried out to improve the health and wellbeing of those who live and work inthe Borough.
A more detailed version of the different sections that have informed this AnnualReport is contained on a CD at the back of this document and includes a full set ofthe Public Health Archive data sets for reference.
This year has seen a real milestone in healthcare with the 60th anniversary of theNHS. This has given me an opportunity to look back on how things have changed inthat time for the health of all who live in the six towns that make up Sandwell. Therehave been some dramatic changes over six decades, noticeably in the way we arenow protected against diseases and illnesses that once killed us.
Although things have improved, some things remain the same. Sandwell’s biggestkiller today – heart disease and stroke – is the same as it was 60 years ago. There areareas of real deprivation which have a major impact upon people’s ability to behealthy and live healthier lifestyles. That is the challenge that my colleagues and I faceevery day.
But it is the global ‘credit crunch’ that is really affecting us all right now. MyIntroduction to this Annual Report considers Crunch Time for Health in Sandwell and addressesthe effects of this economic downturn on our own health, wealth and wellbeing – and what wecan do about it. Health-wise, just like economically, we are all living beyond our means: stackingup a burden of health ‘debt’ in obesity, inactivity, unhappiness and dependence.
The health service itself has been funded at record levels on the back of the economic boom ofrecent years and has seen much improvement in care standards, waiting times, access and so on.But with the economy sinking, the ‘banker’ for our health that we rely on for our care and cures– the NHS – cannot bail us out for long. It cannot offer cures for everything and can barely copewith the burden of care.
The years of boom are about to be replaced with years of tightened belts in health servicespending as well as everywhere else – and we have to learn to adapt our own lifestyles tocontribute to aid our own recovery. We must learn to live within our health means by:
l Consuming what we need to live, not what supports our lifestyles.
l Growing as much of our own food as we can locally, to reduce our reliance on transported food and world harvests and world markets.
l Walking and cycling where we can, to reduce our reliance on petrol and to keep our bodies and minds fitter, leaner, and more alert.
l Equipping ourselves with health knowledge, so we can be self-reliant and independent and notat the mercy of health professionals and the health market.
l Developing our local alternative economy for health and self-reliance by building social enterprises, co-ops and community economic systems – such as the Credit Union and Time Banks – to prevent us being at the mercy of speculators and world finance markets.
My Public Health colleagues and I, together with our partners, are committed to helping andsupporting the people of Sandwell achieve all these things. By working together, and by reducingour debt burden of unhealthy lifestyles, ill health, dependency and over reliance on expensive andineffective medical treatments, we can all help to contribute towardsa more cost effective, affordable health service throughmaintaining and protecting health.
Dr John Middleton
Director of Public Health
3

Crunch Time for Health inSandwellFollowing the theme of Crunch Time For Health, it is appropriate and timely that we lookat work, skills and economic development – and the contribution that health and healthservices can make to improve economic security and independence as well as the healthand wellbeing of Sandwell people.
In this Introduction I have outlined the major challenges and areas of work being carriedout in Sandwell – and my recommendations for what we should be doing to improve thelives of everyone who lives and works in the Borough. More detail is available on the CDat the back of this report and this document highlights specific areas of work from thelast year that are worthy of note in their own sections.
Working in PartnershipSandwell Partnership – the body that pulls together all of the organisations that want tosee Sandwell thrive and flourish – has had a successful year. It has consulted widely onproposals for the revised Sandwell Plan – a 20-year plan for transforming the Borough –and the new Local Area Agreement (LAA). This is a kind of flexible ‘contract’ between theCouncil, its partners and the national Government which agrees how it will delivernational targets to meet local priorities in eight different ways. These are:
l Improving Health
l Supporting Independence
l A Better Start To Life
l Successful Young People
l Reducing High Volume Crime
l Stronger Safer Communities
l Improving Housing
l Improving Skills and Jobs
Sandwell PCT has played a full part in thedevelopment of these plans. It leads on two of theseeight LAA priorities – Improving Health and A BetterStart to Life – and is a major player in most of theothers.
Improving Health is perhaps the most obvious lead forthe PCT and requires us to make substantialimprovements in identifying people at risk fromcoronary heart disease and strokes and preventingthem from becoming ill. We cannot do this alone. It isa partnership activity which requires others to send usreferrals to the stop smoking service, to provide betteroccupational health screening and create workplaceconditions for better health.
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell
4

A Better Start to Life remains a major concern in the area – but substantial plans are inthe pipeline for better services and better prevention of ill health in pregnancy for motherand baby.
The PCT plays a strong role in Reducing High Volume Crime through its role in domesticviolence prevention and management, alcohol and drug prevention programmes. In theImproving Housing objective, the PCT plays a role developing better aids and adaptations,home care services, SMART housing and assistive technology and in tackling fuel poverty– a major cause of premature death and extra deaths in winter. A new Housing andHealth Strategy will be brought forward early in 2009.
The LAA priorities are reflected in an exercise the PCT has been going through on WorldClass Commissioning, which has been heavily influenced by public health priorities, butalso cross references with other partners’ priorities and initiatives. It has been asubstantial year for consolidating organisational policies – next year must be a year forimplementation.
Two Major MilestonesThis year has seen two great milestones in healthcare and wellbeing.It is the 60th birthday of the NHS – you can read more about that inthe next section – and it is also 60 years since the UniversalDeclaration of Human Rights.
Health is a basic human right but there is still much to be done toreduce the inequalities – or differences – in health within Sandwellitself and between Sandwell and the rest of England. The prioritiesset within the LAA and the World Class Commissioning priorities aredesigned to address some of those differences and we have work todo to improve the standard of healthcare for people with learningdisabilities, in particular.
The Universal Declaration of Human Rights seeks to secure the rightto freedom from danger and violence for all people and we havemuch more to do in the field of safeguarding vulnerable adults andchildren. The PCT is the third accountable body for crime reduction inthe LAA’s eight priorities. With the Local Authority (Council) and thePolice, the PCT must fulfil its responsibilities by investing in theprevention and management of domestic violence, tackling alcohol-related violence, drug-related harm and improving community safety.
Freedom from poverty and the right to a satisfying role in society isalso a human right. The draft Anti-Poverty Strategy for the Boroughcan be found in the CD at the back of this document. In brief,Sandwell PCT:
l Must contribute to efforts to alleviate the ill health caused by poverty and to support partnership efforts to improve welfare rights and tackle fuel poverty.
l Should review its commitment to welfare rights advice in General Practice and considerimproving the specialist services managed through the Local Authority service within the Joint Policy Unit.
l Increase efforts to reduce poverty and to tackle the ill health caused by fuel poverty, including the excess of winter deaths seen in Sandwell principally because of cold, stress and poor heating in our housing.
5

Work Is Good Work is important to keep healthy and well and our health services offer manychances for people to find meaningful work. Skills shortages and poor workingopportunities for Sandwell people are long-term local problems which health andcare services can contribute towards improving.
The section of this report called Working Towards Better Health and Wellbeingexplains more about what we are doing to help people back into work – and it isimportant that we do this. Returning to work is an intrinsic part of any worker’srecovery plan and the environment they return to should support this.
The employment rate in Sandwell is below the regional andnational average and those out of work and claiming benefitsaccount for 17% of the Borough’s population of just over 287,000people. In the worst neighbourhoods, this rises to a rate of 30%.
Fewer professional people work in Sandwell compared to otherplaces in the country with almost a third of those employedworking in process, plant, machinery and elementary occupations.Skills and qualifications in the Borough are low: one in fourworking people hold no qualifications at all, which is twice thenational average.
Work is more than just a source of cash. Work gives a structure topeople’s days, fills time, offers creative possibilities and givespeople the possibility to make things much bigger thanthemselves. All of these psychological and social benefits of workare lost to people who are unemployed. Some of these benefitsare also lost to people who are carers and to people who aredisabled or long-term sick – who are seen as dependants and notgiven enough chance to show what they can offer.
There are very few occupations where being in work is moreunhealthy than being unemployed. The health of people whobecome unemployed deteriorates and the life expectancy ofunemployed people is reduced. So we need to see work asimportant – but it has to be as rewarding and fulfilling as possible.We should strive for more than just ‘machine minding’.
As well as unemployment benefit claimants, Sandwell has a very high proportion ofits population receiving Incapacity Benefit: 18.3% in 2007/08. This reflects, tosome degree, the high levels of ill health in the Borough but it also reflects poorwork opportunities and inflexible working practices that are disability-unfriendly.
The health service is guilty of being among those employers who have not donevery much to help disabled people into jobs. New Deal for Welfare: EmpoweringPeople to Work began in 2007 to help disabled people and those receivingIncapacity Benefit to get into work. Seetec is the local company contracted todeliver Pathways to Work – the support programme helping to make this happen.
The principle of the initiative is welcome: that all people of varying abilities shouldbe able to participate in work in order to have the benefits that employmentbrings. There is also the political and economic desire to reduce the financial costof Incapacity Benefit and this is quite a proper objective. Looking at Sandwell’sfigures, it should be quite unacceptable that nearly one in five of our citizens claimIncapacity Benefit.
I recommend Sandwell PCT to:l Further develop its occupational health service for employers in Sandwell.
l Implement the draft service model, Sandwell Works (see the tiered diagram in the Working Towards Better Health and Wellbeing section).
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell
6

Skills Development Sandwell is still more involved in manufacturing than other parts of the country but, as withthe rest of the country, more of our jobs are now in the service sector. There is inequality inthe distribution of unemployment and Sandwell’s Neighbourhood Employment and SkillsPlans (NESPs) are intended to address these problems in the 13 areas with the highestunemployment. Sandwell’s Learning To Care Project was very effective in getting people fromsome of these high unemployment areas into work in social care, with the added benefit ofproviding a better diversity profile – a mix of people from all kinds of backgrounds more inkeeping with the communities they serve.
This work is now being taken forward to enable people to get jobs in healthcare and socialcare through the Routeways to Health and Social Care Careers project. The aim is to provideentry-level job opportunities from the age of 18 years, leading to progression anddevelopment opportunities through improving individuals’ skills.
The health service can make a major contribution towards skills development in lots ofdifferent ways:
l For its own staff. There are high levels of poor literacy and numeracy in the health service and we need to take part in the Skills For Life staff programme and other adult education to support our staff in acquiring skills that support their development and personal growth.
l For our patients, clients and carers. We should point people in the right direction for adult education and basic skills when needed.
l For potential new employees. We should offer encouragement and a first step on the ‘skills escalator’ to higher levels of health service work. We can do this by our support for schemes such as placements, volunteering opportunities, apprenticeships, supporting the new diplomas and developing a consortium to ensure that the current gaps are filled.
There are many opportunities for health and health service training in schools through healtheducation, personal skills, food technology and physical education. We are proud to be apartner in Holly Lodge School’s Smethwick Health Education and Wellbeing (SHEW)Foundation School project. Through this, the school majors on all aspects of health servicework in science and in health and social care.
I recommend Sandwell PCT to:l Play a full part in the development of Holly Lodge SHEW project.
l Work with other schools, such as Willingsworth and the Priory Family Centre, to develop their community agriculture proposals and with Alexandra High School with their health and citizenship work.
l Continue to develop our participation in the National Healthy Schools Programme. Currently 117 (97%) of Sandwell's 121 schools are participating.82 (68%) schools have achieved National Healthy School Status and 51 (42%) schools have Sandwell's Platinum Healthy Schools Award . This scheme has been successful in helping young people to healthier lifestyles but has also helped to develop whole school health policies which have contributed to improved academic results. Parents should ask schools what level of the Healthy Schools Programme they are at when they come to choose for their children.
l Fully support appropriate diplomas, in areas such as healthcare and public services, by developing a consortium with partners and provide good quality placements.
7

Unpaid Work ‘Work’ doesn’t just include paid employment. The work of unpaid workers in thehome, carers and voluntary work should not be ignored. The full Carers’ Strategy isincluded on the CD.
I recommend that Sandwell PCT: l Identifies and recognises carers as equal partners in providing care, such as: the
development of care pathways; health improvement programmes; GP practice registers; annual health checks and hospital discharge planning.
l Works more closely with the Local Authority and the voluntary sector to promoteand support the right of carers to a life outside caring, by safeguarding their employment and training opportunities.
l Develops support services for carers, including short breaks.
l Supports people after bereavement – often an overlooked issue.
l Develops a full portfolio of voluntary sector contracts that is publicly available.
l Considers voluntary sector options for the provision of services in all the PCT’s commissioning decisions.
l Recognises the need to develop the voluntary and community sectors to enable them to compete more equally in the developing ‘market’ for healthcare and lifestyle services.
l Agrees a Community Development Strategy by March 2009. This document will outline the contrasts and similarities between community development and public and patient involvement in health and describe the role of community development in raising the aspirations of local communities for better health – and support local communities to secure their rights and entitlements to better health and care. (The current draft Community Development Strategy and the agreed PCT Patient and Public Involvement Strategy can be found on the CD)
Citizen Wage In this time of economic hardship and insecurity, it is time toresurrect and debate the concept of the ‘citizen wage’. This is a levelof income provided to all citizens by the state. It differs from theminimum wage because it is not paid by employers but the stateand recognises and rewards unpaid house working, caring, beingcared for, voluntary work and other activities not covered by theconventional economic system.
It may appear inflationary – the state simply paying everybody someminimum subsistence level. However some of it is covered byexisting state handouts – the minimum rate tax band and existingbenefits payments, for example. It is not means tested and it is notdiscriminatory. There are advantages to employers and to industry inthat the first level of wage payment to their employers is paid by thestate meaning the chance to employ more people is generated.
I recommend Sandwell PCT will: l Initiate a debate on the ‘citizen wage’ at the 2009
Sandwell Health Other Economic Summit.
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell
8

9
Time BankIn this time of credit crunch – wouldn’t it be great to have a secure income that isinflation-proof so it will be worth the same in ten years’ time and that no-one cansteal from you? Welcome to the Time Bank.
This is a system through which people trade in time instead of cash – offering theirskills and services and making requests for things they want in return. It is notbartering because you do not have to trade one-to-one with another person and nomoney is exchanged. ‘Earnings’ – calculated in hours – go into the bank and youcan draw on them to get things you want from anyone else in it. Everyone’s time isvalued the same so no-one can cheat, steal or market their talents as being morevaluable than yours. Your time is not vulnerable to speculators, hedge fund high-rollers or computer viruses and will be worth the same in ten years as it is now.
People trade simple everyday skills and offer to do things for other people that maynot be bought in the conventional job market. Need someone to hang your cleancurtains up? Walk the dog? Do a small shop? This kind of community support is justwhat Time Bank is all about and it gives people with time on their hands, but verylittle income, the chance to do something to help. Those who take part could buildup credits now, whilst in good health, so they can be traded in a few years if theyare not so fit and able and need some help.
The ‘credit crunch’ is the ideal opportunity to reinvigorate this scheme.
As such, I recommend:l Sandwell PCT and Sandwell Partnership should seriously
expand investment and support to Sandwell Time Bank.
l The PCT should re-establish its volunteering scheme, enablingall members of the PCT staff to do one day’s volunteering work in a community organisation of their choice in Sandwell.
l Major employers should also join the Time Bank and use theircorporate volunteering scheme to massively stimulate the local ‘time market’.
l Major employers and Sandwell Partnership should reward patients and members of the public who take part in consultations with time credits cashable through the SandwellTime Bank. Other recipients should include: volunteer walk leaders; Dr Bike; those involved in the Green Gym and the enormous body of volunteer public health workforce providing public service every day of the week so the initiative can grow to an industrial scale.

Working in the NHSThe ‘Towards 2010’ programme for reconfigured health services in Sandwell andwest Birmingham will require new skills and, potentially, new workers in local GPand healthcare practices, redesigned clinical services and in the public healthprotection and health promotion services.
Over recent years, there has been less on-the-job training and, with plannedchanges to the education system, it is perhaps the right time to change this tomeet the future demands.
In General Practice and in hospitals, nurses’ roles are changing and evolving, andthey are taking on duties and responsibilities previously held by doctors.
All this gives Sandwell PCT the opportunity to increase the ‘diversity profile’ of itsworkforce. In other words, to increase the numbers of people with disabilities, fromminority ethnic groups, and those from the local population who need to improvetheir skills to get back into work.
To do this, we will work with projects such as Pathways to Work and Routeways toHealth and Social CareCareers to prepare and support local people through thepublic sector recruitment processes. We will also develop placement schemes foryoung people and adults in ‘sector tasters’, work experience and training support.
We will also increase the capacity and capability of the new public health workforceto include new roles including Health Trainers and will equip support staff with skillsto support health improvement (see the Healthy People and Towns section).
In our existing workforce:l The largest proportion of our staff are classified as White British at 73.21% -
which equates largely to the make-up of the local population.
l The next largest ethnic group is Asian or Asian British (Indian) at 9.47% - which mirrors the local health economies and the local population.
l Black or Black British (Caribbean) account for 6.44% of the workforce – which is larger compared to the percentage living in the local community.
l Staff of Asian or Asian British (Bangladeshi) and Asian or Asian British (Pakistani) origin are under-represented within Sandwell PCT compared to the local Sandwell population. This is not true of the other local health economies and wewill be taking action to address this.
l Women comprise the largest gender breakdownof Sandwell PCT which is not unusual in a healthcare setting. In all directorates, women arethe largest gender group, but the most significant difference is within the Operations Directorate with 86% of staff being women compared to 14% men.
l The majority of the workforce falls between ages 26 to 55 years with the largest group of staff aged between 46 and 50 years, followed by ages 41 to 45 and 36 to 40 years. The number of staff aged 55 and over drops significantly. As the general population moves toan ageing population the PCT should aim to reflect this in its workforce.
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell
10

Investment in skills and training in the health service, in healthcare and in lifestyleand health promotion services is one of the best investments public bodies canmake if they want to secure more jobs. Only transport and education provide betterreturns in jobs created per investment.
There is clearly much for the NHS to do in this difficult economic time to try tosecure the rights to health for local people and to find opportunities for them towork in health-promoting and health-protecting services.
I recommend that the PCT should:l Write a Workforce Development Strategy to include ideas for on-the-job training
and also to look at the mix of skills of staff in community care and General Practice to see if new ways of working can offer greater opportunities for non-qualified workers.
l Develop with partners a health and social care apprenticeship scheme.
l A substantial proportion of the next year’s Working Neighbourhoods Fund is usedto support the full implementation of health-related job creation and skills development. This will enable other health service resources and European funds to be secured in matching funding to greatly boost the number of jobs created.
l The PCT should review its existing training budgets and on-the-job training opportunities, together with its partners, to ensure maximum synergy with developments being taken forward through the Working Neighbourhoods Fund and European Regional Development Fund money.
11
12
Public HealthThe Sandwell Community Agriculture Strategy has been produced this year and hashad a period of consultation. It offers Sandwell a massive chance to improve localknowledge about healthy food, to give people healthy activity and the chance formore local jobs. At the same time the UK Research Partnership has produced for usa report on the state of the Sandwell food industry. Nourishing The Local Economyshows that Sandwell is still massively under-represented by jobs in the food industry,so there is a massive opportunity for local job creation in growing, supplying,processing and distributing. Both the strategy and the report can be found on theCD.
The CD also includes a short report on the Sandwell Health Other Economic Summitconference, held in July 2008, called Fat Chances for Food and Health. This reporthighlights the insecurity of the global food production system, the problems ofclimate change, crop failure, food commodity speculation, genetic engineering andintellectual property theft for food substances which all contribute to price rises andfood shortages.
On the back of these reports, I recommend that:l Sandwell needs to make itself as food aware and as food secure as it possibly
can.
l Sandwell Partnership gives its strong support to the implementation of the Community Agriculture Strategy.
l The Council, economic agencies and the PCT support the further development ofthe local food industry research and support the Find It In Sandwell initiative, working with local food industry representatives.
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell
In addition, people need more information so they can be healthy and well andcommunity projects like Murray Hall Community Trust and the Sandwell PublicInformation Network (SPIN) should receive more investment, development andpromotion.
Local people are already playing their part in improving thehealth of their own communities through the innovative newHealth Trainers programme. Through this, the PCT is looking at adifferent way of identifying and supporting those at risk of heartdisease by bringing together screening programmes, healthprofessionals, community support and trained local people –Health Trainers – to offer a package of support. There is moreabout this in the Healthy People and Towns section.
This initiative is complemented by the Communities for Healthpilot programme in Soho Victoria. This is a cardio vascular disease(CVD) project aimed at offering community health informationand support for people not identified as being at current risk ofCVD, as part of general health promotion activity in areas at highrisk of premature death and disease.
In addition, there is enormous potential for job creation in public health including:
l Promoting cycling through: cycle maintenance; cycle training for all ages and abilities; cycle clubs for leisure or transport and town planning developments.
l Public health nutrition: community food growing; supply; distribution; cooking skills and healthy eating educational developments such as Growwell, Eatwell, Shopwell and Slimwell.

Arts and Health The PCT will shortly receive an Arts and Health Strategy to consider adopting. Theinvolvement of the arts in health and health service development has historicallybeen seen as something of a luxury and a low priority – but there is a substantialrole for the arts in health and health services.
Use of the arts can help us improve:
l Our understanding and our communications.
l How our healthcare settings look and the appearance of aids and adaptations foreveryday living.
l Improve the quality and content of health promotion products.
l Our mass media communication.
l Non-competitive, highly socially acceptable, life-long physical activity through dance.
Working with artists is a low cost way to improve the effectiveness of healthservices and health promotion campaigns. It is also a useful means to create jobslocally. There are new opportunities in Sandwell with the opening of THE PUBLICbuilding in West Bromwich and it is essential that we capitalise on this excellentresource and develop Sandwell as a centre of excellence for the arts and health.
I recommend:l The PCT adopts an Arts and Health Strategy early in 2009.
l There is specific investment in dedicated arts and health projects – some of whichwill attract external funding from arts bodies, the National Lottery and trusts.
l All service commissions from the PCT should incorporate 1% for an art element to enable the improvement of the aesthetics of care delivery, communications andpublic information.
13

14
Applied Health Research Sandwell PCT is a partner with Birmingham University, which together made asuccessful funding bid earlier this year to become a centre of excellence for healthresearch – earning CLAHRC status (Collaboration for Leadership in Applied HealthResearch and Care). CLAHRC is a departure from previous research fundingregimes in that it matches an amount of research funding to an existing healthservice development. This means that new services can be subjected to properevaluation using the best available research methods from the start.
Sandwell PCT leads the housing and health research strand of the LAA which willevaluate the implementation of telephone care and assistive technology inSandwell and develop a data warehouse for housing and health. This will help usto track the health improvements associated with major housing improvement overfive years.
Sandwell PCT is participating in two other strands of CLAHRC. Firstly, the coronaryrisk programme, together with Heart of Birmingham Teaching PCT and SolihullPCT. Secondly, the health service reconfiguration evaluation, covering the ‘Towards2010’ programme in Sandwell and west Birmingham and service re-design inWalsall.
This renewed interest in high quality research throws up some excitingopportunities in Sandwell, including jobs through additional research work and theprospect of a new university campus in the Borough.
I recommend:l The PCT should play a key role in developing potential
training and research content with the candidate university when agreed.
l The PCT supports the development in principle of a Sandwell public health research and practice teaching base, which will be allied to the proposed developments of CLAHRC, the University of Sandwell and the Towards 2010 programme.
The full CLAHRC bid can be found on the CD.
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell

Social Marketing ‘Social marketing’ is a buzz phrase at the moment and there is considerable interest. It is a wayof analysing people’s behaviours, attitudes and beliefs so that advertising works more effectively.
For health organisations like ourselves, this means targeting health campaigns, promotions andinformation about redesigned health and care services more appropriately – to suit differentaudiences.
Now is the time to take a step into social marketing to assist with better-targeted preventive careprogrammes as well as service redesigns, such as diabetes and eye services. To do this, SandwellPCT should adopt the draft Social Marketing Strategy and invest in a rolling programme of socialmarketing studies.
I recommend:l The PCT seeks to develop local capacity to undertake social marketing using expert external
resources to undertake dedicated surveys and help staff to understand the value and power ofsocial marketing. Just ‘buying in’ external studies is not going to give us the intelligence we need to properly redesign services on the basis of what the surveys tell us.
l All service planners and commissioners consider a percentage addition to planning costs to be used for social marketing purposes. They should also include a research component in their investments. A working assumption for the combined social marketing and research evaluationshould be around 10% extra.
l The PCT, through the Director of Public Health and the Head of Public Health Information and Intelligence, should develop a Health Research Strategy for Sandwell by July 2009.
15Picture supplied by the National
Social Marketing Centre

A Bid for a Healthier Town Following publication of the National Obesity Strategy published in late2007, the Department of Health’s Department for Children and Familiesinvited expressions of interest in a Healthy Communities Challenge Fund.
Sandwell PCT put together a bid for a share of this national fund and hasbeen shortlisted.
The national strategy recognised that obesity is not simply the result ofeating too much and not exercising but is also a product of unhealthy – or‘obesogenic’ – environments. This includes the increased reliance on carswhich has created unfriendly, inhospitable environments in which peopleare afraid to walk to shops and services, leading to inactivity, obesity andthen more car reliance…
The PCT’s bid is for developments in food and fitness programmes andthere is more about this in the Healthy People and Towns section. In brief,the central part of the plan is to set up Sandwell Healthy UrbanDevelopment Unit (SHUDU) which will bring together health and planningexpertise to improve health and the environments that contribute toobesity.
The PCT is the body that is accountable for this proposal but it is jointly submittedwith the Council. If successful, it will initially cover West Bromwich and Wednesburyand could be rolled out across the Borough in the future. Whatever happens in thebidding round, we believe the work done so far is essential if we are to have anychance of hitting obesity reduction targets and creating healthier, safer and moreattractive environments for our children to grow up in.
I recommend: l That all those involved seek to implement everything that has been learned from
the bid submission through the Challenge Fund if successful – but through local resources if we are not.
Personalised Care Agenda forSocial CareThe Government has set a new agenda for health and social care – with the aim ofgiving people choice and independence through care packages devised bythemselves, for themselves.
That has to be a good thing to aim for – after all, who wants to go to a day centreevery day and why shouldn’t people choose to spend time in the communitygarden or a day on a self-build project instead?
In reality there are likely to be difficulties in the short term, getting services changedto deliver to the new models. The Learning To Care project in Sandwell has beensuccessful over many years in training people for jobs in the residential and nursingcare sector. Now training needs to be geared towards personal care provision forclients, supporting them in their homes and in their everyday activity.
I recommend:l That social care workforce needs are taken forward through strong consultation
with support agencies, client groups and voluntary organisations such as Ideal forAll, which has a strong track record in supporting clients and client-centred activity.
16
Cru
nch
tim
efo
rh
ealt
hin
San
dw
ell

Corporate Citizenship Corporate citizenship is the name given to the role organisations play in theirlocal community. Sandwell PCT’s ‘value statement’ says it will be environmentallyand socially responsible and it can be a good corporate citizen by:
l Buying goods and services from local sources.
l Using its land and buildings wisely.
l Setting a good example to others by providing high quality occupational health services and improving the working lives of its staff.
l Protecting its innovations – or intellectual property – so they may be developed for local job creation and patent royalty returns to the NHS. Sandwell PCT has recently secured two patents for products developed by our designer and ergonomist and the PCT has demonstrated its commitment to developing new aids, adaptations and products for health and care use through its role in the i-Health project.
l Reducing its carbon footprint, conserving physical resources such as heat and water and reducing pollution and waste.
Preventive services and services which can be locally delivered are likely to have alower carbon impact. Health promotion schemes such as food and fitness promotion, cycling and walking are ‘greener’ as well and an Exercise OnPrescription regime for obesity or peripheral vascular disease might be better for thelocal economy and environment than buying expensive imported drugs or surgeryrequiring imported equipment.
The PCT has responded to the NHS Carbon Reduction Draft Strategy and will beexpected to develop its awareness and responsiveness to the climate change agenda.
I recommend the PCT:l Gives greater attention to the environmental impacts of the decisions it takes.
l Allocates a reserve for investment towards its carbon reduction initiatives to be implemented in 2009/10.
l Includes a carbon reduction impact statement and a corporate citizen impact statement in its policy reports to the PCT Board.
l Gives strong support, together with Sandwell Partnership and other housing partners, to the development of the i-Health project in Sandwell, with intensive use of assistive technology in new and adapted housing.
l Considers extending the role of design in our health service development processes, recruiting an additional designer/ergonomist to assist health and care strategies and design new aids and adaptations for the commercial market.
l Invests more in occupational health services for its own staff. In the light of DameCarol Black’s recommendations for an NHS lead on occupational health for small business, the PCT should increase its investment in our local Workwell service.
l Reviews corporate citizenship responsibilities, along with all Sandwell partners, and considers its contributions to the local economy and local community resilience.
Dr John Middleton
Director of Public Health
17

60 Years of The NationalHealth ServiceThis year sees the 60th anniversary of the founding of the NHSand this is an opportunity to review how things have changed– and yet how some things have remained the same.
During this time, the health of Sandwell has seen somedramatic improvements, as you will see below. However, manyof the issues that concerned the Medical Officers of the sixtowns in 1948 remain a challenge to my Public Healthcolleagues and I today.
Boundaries have changed and the way conditions are recordedare different, so comparisons between ‘then and now’ are notexact but give a flavour of how things have changed.
There have been some incredible advances in health andhealthcare over this period, especially in the control ofinfectious diseases and the development of medications forheart disease and cancer. People are living longer and havebetter healthcare – but with progress comes a different set ofchallenges for us to face.
Mothers and BabiesChild and maternal health has been one of the great success stories for healthimprovement since 1948.
The development of vaccination programmes has almost eradicated infant deathsfrom infectious diseases. Until recently measles was on the decline due to asuccessful immunisation programme. However due to scare stories around themeasles, mumps and rubella (MMR) vaccination, measles is on the comeback andthe number of cases rose to 20 in 2007.
This echoes a situation from 60 years ago when Mr FAcker, the Medical Officer of Rowley Regis, despairedabout the unnecessary suffering and deaths caused bythe failure of parents to take up the effectivevaccination against diphtheria.
In 1948, births outside of marriage were seen as astigma with the challenge of reducing figures andcaring for mothers being overseen by Birminghamand Lichfield Diocesans. Back then, teenageconceptions were so rare as not to warrant mention.Social changes have brought big changes. The stigmahas disappeared from births outside marriage but theflipside of this is that teenage pregnancy hasdramatically increased.
18
60Y
ears
of
the
Nat
ion
alH
ealt
hSe
rvic
e

Causes of DeathAlthough many things have changed, some have remained the same. Today’sbiggest killers for adults are the same as they were in 1948. Circulatory disease –which includes heart disease and stroke – was responsible for 37% deaths in 1948and 36% in 2007.
However, there are significant differences. The percentage of people dying fromcancer has gone up from 17% in 1948 to 26% in 2007. Many of the causes ofdeath have changed, with the large numbers of deaths from respiratory andinfectious diseases being dramatically reduced.
The introduction of antibiotics had a huge effect on this and has seen tuberculosischange from being a major cause of death to a curable condition in all but a fewcases: but the challenge is still with us in Sandwell. Seven people died from thecondition last year and we have a higher prevalence rate than the rest of England.
Changes in the way we work and live has also played a major part in causes ofdeath. In 1948 respiratory disease was linked to industrial exposure to pollutants, inparticular smoke, with large numbers of deaths from bronchitis and pneumonia. In2008, deaths from industrial pollution have been largely replaced with personalpollution from tobacco. In 1948 lung cancer was rare, making up only 8% ofcancers compared with 22% today.
19
Mothers & Babies: Facts and Figures
Sandwell 60 Years Ago…l A child born in 1948 was five times less likely to
make their first birthday than one born today.
l 272 babies did not get to their first birthday and there was an infant mortality rate of 40.5 per 1,000 live births.
l A mother giving birth was at 16 times greater risk of dying than a mother today. In 1948, four mothers died as a result of child birth (one in every 1,000 births).
l 15 infants died from diarrhoea and enteritis aged under two, one from diphtheria and three from measles. There were over 3,097 cases of measles 1948.
l One in 330 babies were born out of marriage in 1948.
Sandwell Today…l The infant mortality rate is 7.8 per 1,000 population
(based on figures from 2004 to 2006). This is still 50% higher than the average for England (five per 1,000).
l Just one mother died as a result of childbirth in the last four years (one in 16,000 births).
l 43.5% babies are born outside of marriage.
l Latest figures (2006) show 62.7 per 1,000 women aged 15 to 17 are pregnant.

Perhaps surprisingly the number of people dyingfrom road traffic incidents has declined verysignificantly over six decades. Much of this is downto improvements in road layouts and drivertraining. Those who are dying are different now tothen: it is largely pedestrians and cyclists who losetheir lives and not car occupants. Drivers are rarelyexposed to life-threatening situations due to safetydevices such as safety belts and airbags.
Major causes of death: 1948 compared to 2007
20
60Y
ears
of
the
Nat
ion
alH
ealt
hSe
rvic
e
Circ
ulat
ory
dise
ase
Can
cers TB
Bro
nchi
tis
Pne
umon
ia
Sui
cide
s
Roa
dtr
affic
Dia
bete
s
Dia
rrho
ea
40%
35%
30%
25%
20%
15%
10%
5%
0%
37%36%
17%
26%
7%
0%
6% 6%4% 5%
1% 1% 1% 1% 1%0% 0% 0%
Per
cent
age
ofal
ldea
ths
Key
1948
2007
21
The Future: Now and ThenIn 1948 the Medical Officers were facing the same demographic challenges we face todaywith “the number of pensioners continuing to increase and, proportionally more important,placing a gradually increasing burden on the social services”. (Staffordshire CMO, 1948quoting Office of National Statistics)
In this year’s Joint Strategic Needs Assessment, produced by Sandwell PCT’s Public HealthDepartment, there is a very similar conclusion about our population.
We now know that the prediction of 1948 did not come true as the ‘baby boomer’generation of the post-war period filled the employment gap. It will be interesting to see ifthe same will happen again and whether the gap will be filled by newcomers from theEuropean Union.
As far as Sandwell’s future is concerned, it has a number of major challenges to ensure thenext 60 years see an improvement in local people’s health and wellbeing and the keychallenges are:
l To address obesity, physical activity and smoking.
l To strive to maintain the gains made in child health through immunisation.
l To continue to reduce infant mortality.
The Environment Sustainability and pollution were as much issues for the MedicalOfficers of 1948 as they are to us today, although their concernswere about smoke rather than carbon emissions and climatechange.
Sixty years ago, the Medical Officers recognised a role to informand educate the public to change their behaviours. Mr Eugene,Medical Officer of Oldbury, used his Annual Report to encouragepeople to adopt less polluting smokeless fuels in the home as partof the need to reduce overall smoke levels.
Improving people’s health by getting them to make changesdoesn’t happen overnight. It can take years to reap the benefitsand requires everyone to be involved, from the individualthemselves to those who have an effect on the services theyaccess or the environment in which they live.
Many of the interventions identified in 1948 to improve healthand social issues are largely the same today, albeit using differenttechnologies.
The need for improved social conditions, housing and bettermaternity services are now, as well as then, crucial to health andwellbeing. For example, the recommendations in 1948 to reduceaccidents in the home were to improve lighting, reduce slip risksin the home and to provide handrails – much the same as today.

Healthy People and TownsHealth Trainers: A Force for ChangeHelping people to help themselves to a better way of life: that is the key to ahealthier Sandwell.
Improved physical, emotional and mental health can only happen if people playtheir part in choosing healthier lifestyles – but they need proper support, in theirown communities, to help them achieve this.
That is where our innovative Health Trainers come in. These are local people trainedto offer personal health advice to people and give them the support they need toadopt healthier lifestyles.
The aim is for Health Trainers to be integrated with the cardiovascular riskstratification screening process within General Practice. These combined serviceswill provide a targeted approach to identifying those at risk and improving thehealth and wellbeing of people in disadvantaged wards and within their GPpractice. This will be rolled out across all Sandwell GP populations in 2009/10.High-risk people will see nurses and medium-risk will see Health Trainers.
At a population level we currently estimate 15,000 high-risk patients and 9,300medium-risk patients between 35 and 74 years of age are currently not on anytreatment or identified as being at risk.
It is hoped this new approach will prevent 1,020 heart attacks or strokes over thenext ten years in the high-risk category, saving an estimated 306 lives and sparingmany more from incapacity.
Health Trainers will play a crucial part with the medium-risk group, workingintensively to change lifestyles and help prevent patients becoming high-risk. Bydoing this we believe that, over ten years, Health Trainers can help prevent 465heart attacks or strokes and save 155 lives.
In the last two years:
l 3,075 people have been invited for screening.
l 1,699 people have been screened with an estimated 80 heart attacks and strokes prevented and 26 lives saved.
l Of the 1,699 people screened, 802 neededdrugs.
l 48 new diabetics have been diagnosed.
l Five patients were referred to a rapid access chest pain clinic.
l 482 referrals were made to lifestyle services (194 smoking and 288 activity anddiet).
Hea
lth
yPe
op
lean
dTo
wn
s
22

Why We Need a New ApproachPeople living in Sandwell have a shorter life expectancy than those in moreaffluent areas and some of the lifestyle choices they make – such assmoking, lack of exercise, unhealthy food and alcohol consumption – arecontributing to ill health.
According to the Public Health Observatory, people living in 17 out of 24wards in Sandwell have significantly worse life expectancy than the nationalaverage. These wards broadly match areas of material deprivation.
The difference in life expectancy between the lowest and highest wards inthe Borough is five years. The wards of highest need are:
l Soho and Victoria
l Great Bridge
l Wednesbury North
l Friar Park
l Hateley Heath
An analysis of lifestyle trends show:
l 19 of the 24 wards have smoking rates of between 28% and 48%
l 20 of the 24 wards have obesity rates of between 23% and 35% and coronary heart disease prevalence of 3.6% to 5%
Changing the way people behave to improve their health and wellbeing iscomplex but we believe that a community-based approach is the right way.This is supported by two Government White Papers: Choosing Health (2004)and Our Health Our Care Our Say (2006) alongside the Commissioning aPatient-Led NHS strategy (2004).
More locally, the West Midlands Regional Assembly has recently completed aconsultation exercise on a Regional Health and Wellbeing Strategy whichemphasises that good health and wellbeing relies on people living in strongcommunities. Health Trainers can help support this approach.
23

What Health Trainers Do Health Trainers are a friendly face who can offer something in addition tothe services of a health professional. They work one-to-one with patientswith a focus on health improvement and prevention.
They work in local communities, specifically those that are mostdisadvantaged, and help:
l Individuals make lifestyle changes to improve their health.
l Target people from deprived communities.
l Bring people into better contact with mainstream health improvement services.
l Recruit local people into these NHS roles.
l Maintain and develop excellent links to wider community and voluntary sector services.
This new workforce is already developing and, over time, will help us tomeet the Borough-wide targets we share with our partners, as laid out inthe Local Area Agreement, mentioned in the Introduction. Our health andwellbeing priorities include:
l Reducing number of people who smoke.
l Encouraging and supporting sensible drinking.
l Reducing obesity and improving diet and nutrition.
l Increasing exercise.
l Improving sexual health.
l Improving wellbeing and mental health.
By linking in Health Trainers to health screening projects and lifestyle services, wehope to make a real impact on the health and wellbeing of those people who aremost at risk from problems such as cardiovascular disease (CVD).
What Real People are Saying AboutHealth Trainers
Hea
lth
yPe
op
lean
dTo
wn
s
24
Irene, 70: “I feel much better since losing weight.I no longer get breathless and feelmuch healthier.”
Rohina, 38 and Paul, 42:“Health Trainers gave us the motivation tolose weight we needed to, to get us started.We were pleased with the detailed dietaryinformation we received compared topreviously.”
Janet, 51:“Very helpful. My health has improved,I’ve stopped smoking and started toeat more healthily.”
Monmohan, 41:“A big improvement in my health.My cholesterol and blood pressure arelower and I’ve lost weight.”
Rita, 63:“My diet is much better. I feelten times better since starting abetter way of living andcholesterol is lower.”
Keda, 58 and John, 59:“Very happy with the advice, assurance
and support in losing weight.”

25
A ‘Healthy Town’Health Trainers are helping individuals who want to help themselves – but what can we do tocreate a whole town that can encourage, support and offer opportunities to make life betterfor those who live there?
Creating a ‘healthy town’ doesn’t happen by chance – so we are going to try and make ithappen through an innovative two-year pilot project involving all kinds of different people andorganisations.
We want to bring together local people, town planners, highway engineers, food and physicalactivity experts, police, the fire service, social enterprises, businesses, community groups andcharities to create the right environment to improve health and wellbeing.
To do this, we are hoping to create the Sandwell Healthy Urban Development Unit (SHUDU) inWest Bromwich.
West Bromwich, Wednesbury and Great Bridge are the proposed areas for the pilot, largelybecause they contain two of the wards with the highest levels of childhood obesity inSandwell. In addition, there is a lot of redevelopment happening here and there are manyexisting facilities and environments that could be utilised, such as Sandwell Valley Country Parkand Sheepwash Local Nature Reserve in Great Bridge, Tipton.
The vision for the project is to create a sustainable ‘healthy town’ by raising awareness ofobesity, encouraging people to make healthy lifestyle changes and supporting them tosucceed in a fun and practical way.
The overall aim is to enable people to get more active and eat well by creating positiveexperiences in a healthy, safe and accessible environment.
How Will It Work?The idea is to explore new ways of delivering food andfitness programmes by pulling together all of the differentagencies and getting local communities involved. We arelooking to secure investment – potentially up to £4.2m overthe two years – and will carry out high-quality research, plusadditional research funding.
Local people will be able to access information about whereto get information or attend fun sessions near to where theylive and local Champions will work together with RoleModels and public and business sponsors to help it succeed.
The project will co-ordinate existing food policy activities –such as Eatwell, Slimwell, Shopwell and Growwell – withphysical activity programmes, such as the Get Active inSandwell campaign.
In addition, SHUDU will help to create the infrastructure andenvironment which will make it easier for people to getinvolved safely. This will include:
l Street improvements.
l Extended and upgraded cycle network.
l Improved town centre open space.
l Safer routes to school.
l Improvements in catering establishments.
l ‘Fitter for Walking’ scheme.
l Improved canal towpaths.
l A policy framework for all this to happen.
Hea
lth
yPe
op
lean
dTo
wn
s
Target Town: Facts and FiguresIn the pilot areas of West Bromwich, Wednesbury and Great Bridge thetotal population is 116,376 of which:
l 21.1% are under 16 years old.
l 22.8% are over 60 years old.
l 18.6% of the population is black and minority ethnic.
l The 2006 Health Survey for England shows that 29% of adults are obese.
l The National Child Measurements for Year 6 children showed that an average of 21.4% were obese.
l The Active People Survey for 2005/06 shows that 16.67% of adults take part in moderate activity three times a week.
l Disease prevalence is higher and life expectancy in these wards is lower.
26
What We Hope To AchieveOur targets are to:
l Raise obesity as an issue.
l Create a desire to do something about it.
l Create demand for, and be able to supply, more healthy food choices and activity opportunities.
l Create neighbourhoods that encourage healthier lifestyles.
l Visible improvements to the environment.
l Deliver a model that influences the policies of others.
l Embed health in a sustainability policy.
l Contribute to reducing health inequalities and improve health.

Working Towards BetterHealth and WellbeingImproved diet and increased activity will make a difference to health – but workingis good for you, too. Evidence shows that having a job is generally good forphysical health and mental wellbeing. The flipside is that worklessness – or nothaving a job – has a strong association with poor physical health and mental healthwellbeing.
Research has demonstrated that once someone hasbeen off work for two years they are more likely todie or retire than return to work and will have shorterlives than the Sandwell average, so it is importantthat we do what we can to get people back into theworkplace as soon as possible.
Here in Sandwell, worklessness is a real issue. Almosta third of working-age people in the Borough do nothave a job because of health reasons, which is morethan the national average.
The employment rate in Sandwell is 65% - which is7% below the regional average and 9% below thenational average. This breaks down further to anemployment rate among the white population ofaround 69%, compared with 54% for ethnicminorities.
Those out of work and claiming benefits account for17% of the Borough’s population of just over287,000 people. In the worst neighbourhoods, thisrises to a rate of 30%.
Fewer professional people work in Sandwellcompared to other places in the country. Just under athird – 29% of the workforce – are professionals orassociate professionals compared to 43% in England.Process, plant, machinery and elementary occupationsaccount for 29% of the working population – whichis 11% higher than the national average.
Skills and qualifications in the Borough are low withjust 45% of residents having NVQ qualifications at Level 2 or above – compared to64% across England – and one in four working people hold no qualifications at all,which is twice the national average.
Increasing employment and supporting people into work are linked to improvingpeople’s health and wellbeing and are a key part of the Government’s public healthand welfare reform programmes.
Sandwell Metropolitan Borough Council (SMBC) has undertaken detailed analysis atward level of 13 hotspots for employment and worklessness in Sandwell. Theseclosely correlate with deprivation and poor health indicators and back up the theorythat worklessness is linked to poor health and reduced life expectancy.
Full details of the Neighbourhood Education and Skills Plans (NESPs) to improvethings are included in the CD but here is an overview of the top priorities andchallenges for our ‘hotspots’:
27
Tipton and Rowley Regisl Princes End: lone parents; benefit dependency; people with low qualifications;
over 50s; access to transport links;16-24 age group high % benefit claimants.
l Tipton Green: black and minority ethnic (BME) community; lone parents; people with low qualifications; benefit dependency.
l Great Bridge: lone parents; benefit dependency; people with low qualifications; over 50s; access to transport links; claims for all benefits in 16-24 age range.
Smethwick and Oldbury l St Paul’s: lone parents; residents with low
qualifications; BME groups; more female benefit claimants than men; 3rd highest number of jobs in the Borough after West Bromwich and Oldbury; high levels of long-term benefit claimants.
l Smethwick: lone parents; BME groups; high % of Job Seekers Allowance claimants of 6-12 months – low number in 12-month category; high proportion of people with higher level qualifications.
l Soho & Victoria: lone parents; BME groups; life expectancy lowest in Borough; high % of people with no qualifications; high % of females claiming benefit than Borough average.
l Oldbury: BME groups; Incapacity Benefit claim rate increased; high proportion of residents claiming Job Seekers Allowance; unemployment rate has increased compared to Borough average.
l Bristnall: low number of males in employment; high % with no qualifications; high % of Incapacity Benefit; worklessness high in over 50s.
Wednesbury and West Bromwich l Friar Park: residents with low qualifications; lone parents; highest proportion of
people with no qualifications; lowest proportion of people with higher level qualifications.
l Greets Green and Lyng: BME groups; people with low qualifications; high manufacturing employment rate – double the Borough; high % of long-term claimants of Job Seekers Allowance.
l Hateley Heath: residents with low qualifications; high number of unemployment benefit claimants; high % of Incapacity Benefit claimants.
l Wednesbury South: over 50s; the older population; high % with no qualifications.
l West Bromwich Central: BME groups; Incapacity Benefit claimants; over 50s; high % of long-term unemployed.
28
Wo
rkin
gTo
war
ds
Bet
ter
Hea
lth
and
Wel
lbei
ng

What We Are PlanningTo DoThe Department for Work and Pensions (DWP) hasrecently introduced a new programme calledPathways to Work, which enables people onIncapacity Benefit to return to work. First-timeclaimants, or those renewing claims, will beautomatically referred to this new scheme. Anyoneon the benefit can refer themselves for support backinto employment.
The scheme has a keen focus on those who aren’tworking because of mental health problems,muscular-skeletal issues and coronary heart disease.
We want to build on this by identifying andsupporting those people who may have disabilities orhealth-related issues – but do not qualify for thePathways to Work programme. We want to helpthem access employment and work closely withSeetec, the organisation that provides the Pathwaysto Work programme in Sandwell.
Sandwell already has a dedicated mental healthemployment service for people with severe andenduring mental health issues. However, no suchprovision exists for others with learning difficulties,physical disabilities or a chronic disease outside ofthe Workstep-supported employment programme.This is run by Sandwell MBC through Working Linkat Beeches Road and Ideal for All in Smethwick.
29
Worklessness: Facts and Figuresl The number of people in Sandwell who have a disability or limiting
illness is higher than the national average at 12.7%: that’s 33,800 people.
l Of those who work, 10.62% have a disability – which is 3% below the national average.
l Of all of those who are unemployed in Sandwell almost a quarter – 24.67% (1,900 people) – have health-related issues, which is 10% higher than the national average.
l A total of 26,400 (28.32%) people of working age in Sandwell have a health issue and are economically inactive. This is 6% higher than the national average.
l 8.93% of the working age population in Sandwell receive Incapacity Benefit which is higher than the national average.
l According to the Population Survey 2006, there are around 2,900 people on long-term sick leave from work, and possibly claiming Incapacity Benefit, who actively wish to work.

This existing structure gives us a starting point to help those people with healthissues who would either risk losing their jobs due to their ill health or who wouldlike to return to or start work.
We want to use this, together with input from GPs, consultants and other healthprofessionals, to create a ‘tiered’ package of services that start once a sick note isrequested. These would offer the patient an assessment, rehabilitation,occupational therapy or even a ‘prescription’ for voluntary or therapeutic workthat could help them back into paid employment.
It is envisaged that a tiered approach is taken to identify service provision, whichcan encompass the work already done in the Borough and the possibilities forfuture work. Primary care – such as GP practices – would be able to concentrateon tiers 1 and 2 with separate funding or scope for further work with partners fortier 4.
30
Wo
rkin
gTo
war
ds
Bet
ter
Hea
lth
and
Wel
lbei
ng
1st long-term sick note >6 weeks
Rehabilitation
Incapacity Benefit claimantmild / moderate
Severe disability orhealth issue
Tier 1
Tier 2
Tier 3
Tier 4
A tiered approach

Each of these tiers will have a slightly different approach todealing with clients but within these patient and GPdiscussions it is likely that a return to work plan will benegotiated to include such items as:
l Agreeing realistic goals and expectations of healthcare.
l Encouraging a gradual increase in activity levels.
l Agreeing clear goals and a timeline for return to work.
l Discussing what the patient can do rather than telling them what they can’t.
l Discussing how to overcome any obstacles to return to work and thinking about communication with the employer.
l Talking about possible sources of support to help cope with the condition.
If these guidelines are implemented within Sandwell it ispredicted that the number of sickness certificates issuedwill decrease, along with the number of benefit claims.
Our plans for the coming year will see us develop theseservices to help tackle worklessness in Sandwell. The aimsare to:
l Enable people with health and/or long-term unemployment issues to successfully enter employment or training.
l Provide volunteering and placement opportunities in a range of different settings – including charities and community groups.
l Keep people in work who have had a period of ill health.
l Provide support to employers.
l Enable people with learning and/or physical disabilities opportunities for paid or unpaid work.
l Have a healthy workforce.
31
WestBromwich
Wednesbury
Tipton
RowleyRegis
Smethwick
Oldbury
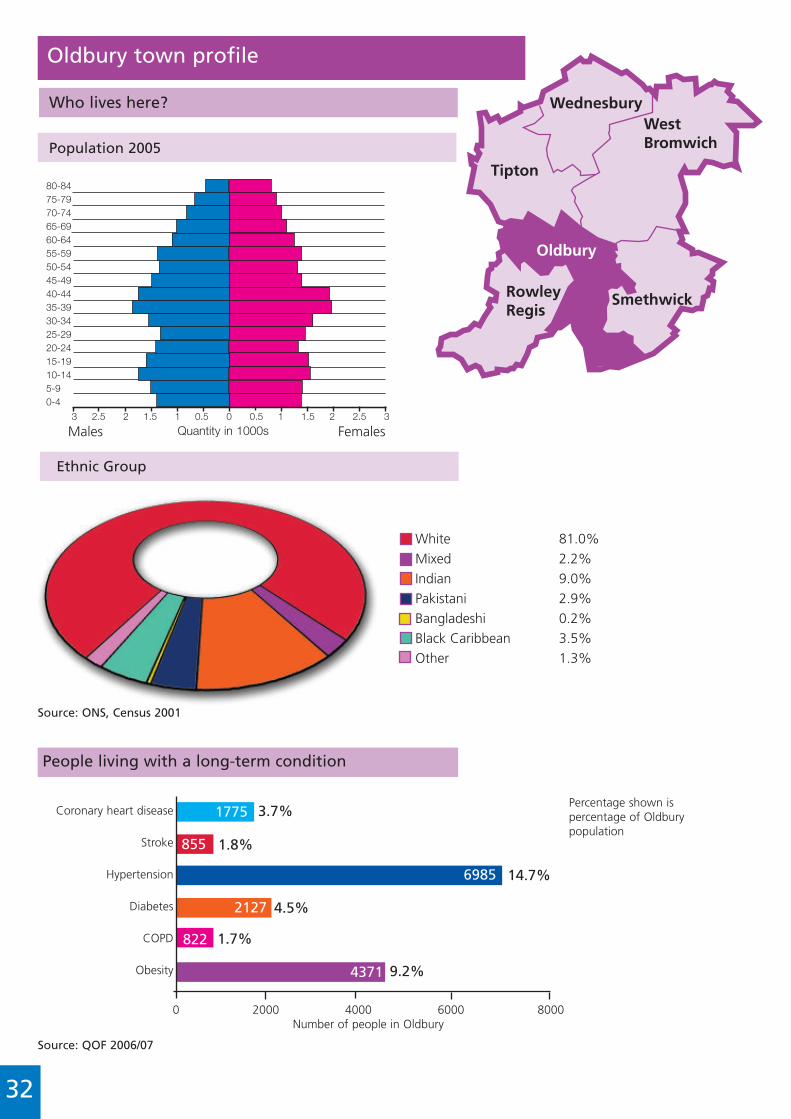
Oldbury town profile
Who lives here?
Population 2005
3 2.5 2 1.5 1 0.5 0 0.5 1 1.5 2 2.5 3
80-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Males Females
oldbury
Source: ONS, Census 2001
White 81.0%Mixed 2.2%Indian 9.0%Pakistani 2.9%Bangladeshi 0.2%Black Caribbean 3.5%Other 1.3%
People living with a long-term condition
Ethnic Group
Coronary heart disease
Stroke
Hypertension
Diabetes
COPD
Obesity
0 2000 4000 6000 8000Number of people in Oldbury
1775
855
6985
2127
822
4371
3.7%
1.8%
14.7%
4.5%
1.7%
9.2%
Source: QOF 2006/07
Quantity in 1000s
32
Percentage shown ispercentage of Oldburypopulation

0 50 100 150 200 250 300
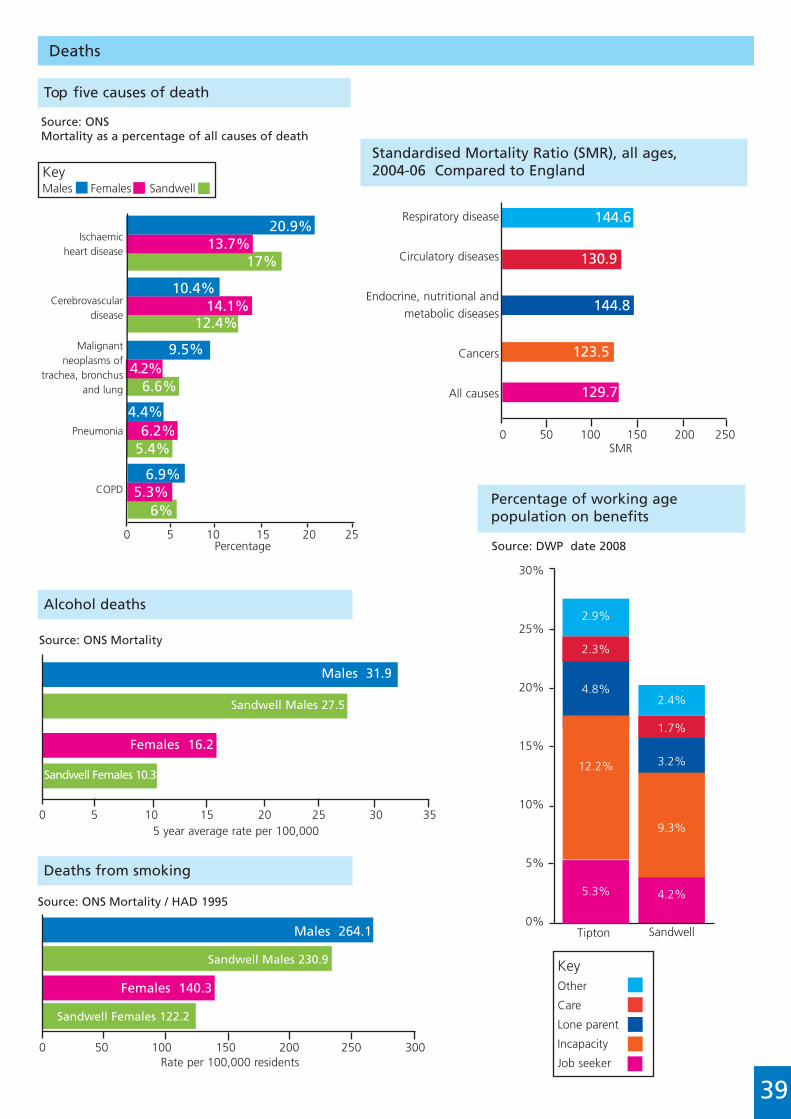
Deaths
Top five causes of death
Standardised Mortality Ratio (SMR), all ages,2004-06 Compared to England
Percentage of working agepopulation on benefits
Source: ONSMortality as a percentage of all causes of death
Source: DWP date 2008
Ischaemic heart disease
Cerebrovascular disease
Malignant neoplasms of
trachea, bronchus and lung
Pneumonia
COPD
0 5 10 15 20 25Percentage
KeyMales Females Sandwell
Respiratory disease
Circulatory diseases
Endocrine, nutritional andmetabolic diseases
Cancers
All causes
SMR
5 year average rate per 100,000
99.7
103.3
120.1
101.8
99.4
0 50 100 150 200 250
25%
20%
15%
10%
5%
0%SandwellOldbury
Town
Source: ONS Mortality
Source: ONS Mortality / HAD 1995
0 5 10 15 20 25 30 35
Males 24.5
Females 6.6
Sandwell Males 27.5
Sandwell Females 10.3
Rate per 100,000 residents
Males 209.7
Females 113.5
Sandwell Males 230.9
Sandwell Females 122.2
Alcohol deaths
Deaths from smoking
21.6%16.7%
19.1%
8.4%12%
10.2%
8.3%3.6%
5.9%
5.2%5.4%5.3%
4.8%4.5%4.7%
33
2.4%
1.7%
3.2%
9.3%
4.2%
2.5%
1.7%
2.7%
8.5%
3.9%
KeyOther
Care
Lone parent
Incapacity
Job seeker

Wednesbury
Tipton
Oldbury
RowleyRegis
Smethwick
WestBromwich
Rowley Regis town profile
Who lives here?
Population 2005
3 2.5 2 1.5 1 0.5 0 0.5 1 1.5 2 2.5 3
80-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Males Females
rowley regis
Source ONS: Census 2001
White 92%Mixed 1.6%Indian 1.8%Pakistani 2.1%Bangladeshi 0.3%Black Caribbean 1.4%Other 0.8%
People living with a long-term condition
Ethnic Group
Coronary heart disease
Stroke
Hypertension
Diabetes
COPD
Obesity
0 2000 4000 6000 8000Number of people in Rowley Regis
1610
792
6100
1864
834
4736
3.8%
1.9%
14.4%
4.4%
2.0%
11.2%
Source: QOF 2006/07
Quantity in 1000s
34
Percentage shown is percentageof Rowley Regis population

0 50 100 150 200 250 300
Deaths
Top five causes of death
Standardised Mortality Ratio (SMR), all ages,2004-06 Compared to England
Source: ONSMortality as a percentage of all causes of death
Ischaemic heart disease
Cerebrovascular disease
Malignant neoplasms of
trachea, bronchus and lung
Pneumonia
COPD
0 5 10 15 20 25Percentage
KeyMales Females Sandwell
Respiratory disease
Circulatory diseases
Endocrine, nutritional andmetabolic diseases
Cancers
All causes
SMR
119.2
118.4
152.5
106.3
112.2
0 50 100 150 200 250
Source: ONS Mortality / HAD 1995
Rate per 100,000 residents
Males 239.9
Females 128.2
Sandwell Males 230.9
Sandwell Females 122.2
Alcohol deaths
Deaths from smoking
20.4%15.4%
17.7%
10.6%14.8%
12.9%
7.9%
4.6%5.7%5.2%
5.4%4.9%5.2%
5.3%3%
35
Percentage of working agepopulation on benefits
Source: DWP date 2008
25%
20%
15%
10%
5%
0%SandwellRowley
Regis
2.4%
1.7%
3.2%
9.3%
4.2%
2.7%
1.7%
3.6%
9%
4.3%
5 year average rate per 100,000
Source: ONS Mortality
0 5 10 15 20 25 30 35
Males 22.2
Females 10.5
Sandwell Males 27.5
Sandwell Females 10.3
KeyOther
Care
Lone parent
Incapacity
Job seeker

Wednesbury
Tipton
Oldbury
RowleyRegis
Smethwick
WestBromwich
Smethwick town profile
Who lives here?
Population 2005
3 2.5 2 1.5 1 0.5 0 0.5 1 1.5 2 2.5 3
80-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Males Females
smethwick
Source: ONS, Census 2001
White 55.8%Mixed 3.7%Indian 18.7%Pakistani 8.6%Bangladeshi 2.9%Black Caribbean 6.9%Other 3.4%
People living with a long-term condition
Ethnic Group
Coronary heart disease
Stroke
Hypertension
Diabetes
COPD
Obesity
0 2000 4000 6000 8000Number of people in Smethwick
1822
815
7534
2495
687
4310
3.3%
1.5%
13.8%
4.6%
1.3%
7.9%
Source: QOF 2006/07
Quantity in 1000s
36
Percentage shown ispercentage of Smethwickpopulation

0 50 100 150 200 250 300
Deaths
Top five causes of death
Standardised Mortality Ratio (SMR), all ages,2004-06 Compared to England
Source: ONSMortality as a percentage of all causes of death
Ischaemic heart disease
Cerebrovascular disease
Malignant neoplasms of
trachea, brochus and lung
Pneumonia
COPD
0 5 10 15 20 25Percentage
KeyMales Females Sandwell
Respiratory disease
Circulatory diseases
Endocrine, nutritional andmetabolic diseases
Cancers
All causes
SMR
128.6
127.0
234.6
108.1
121.2
0 50 100 150 200 250
Source: ONS Mortality / HAD 1995
Rate per 100,000 residents
Males 190.7
Females 100.1
Sandwell Males 230.9
Sandwell Females 122.2
Alcohol deaths
Deaths from smoking
19.7%17.7%
18.7%
9.2%12.7%
10.9%
7.2%
4.8%7%
5.9%
5.9%3.8%4.8%
5.9%4.5%
37
Percentage of working agepopulation on benefits
Source: DWP date 2008
SandwellSmethwick
2.4%
1.7%
3.2%
9.3%
4.2%
2.1%
1.3%
3.1%
7.6%
4.2%
25%
20%
15%
10%
5%
0%
5 year average rate per 100,000
Source: ONS Mortality
0 5 10 15 20 25 30 35
Males 27.2
Females 7.1
Sandwell Males 27.5
Sandwell Females 10.3
KeyOther
Care
Lone parent
Incapacity
Job seeker

Wednesbury
Oldbury
RowleyRegis
Smethwick
WestBromwich
Tipton
Tipton town profile
Who lives here?
Population 2005
3 2.5 2 1.5 1 0.5 0 0.5 1 1.5 2 2.5 3
80-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Males Females
tipton
Source: ONS, Census 2001
White 85.5%Mixed 1.5%Indian 6.0%Pakistani 2.6%Bangladeshi 1.0%Black Caribbean 2.3%Other 1.0%
People living with a long-term condition
Ethnic Group
Coronary heart disease
Stroke
Hypertension
Diabetes
COPD
Obesity
0 2000 4000 6000 8000Number of people in Tipton
1486
650
5064
1513
787
3456
4.1%
1.8%
13.8%
4.1%
2.1%
9.4%
Source: QOF 2006/07
Quantity in 1000s
38
Percentage shown ispercentage of Tiptonpopulation
0 50 100 150 200 250 300
Deaths
Top five causes of death
Standardised Mortality Ratio (SMR), all ages,2004-06 Compared to England
Source: ONSMortality as a percentage of all causes of death
Ischaemic heart disease
Cerebrovascular disease
Malignant neoplasms of
trachea, bronchus and lung
Pneumonia
COPD
0 5 10 15 20 25Percentage
KeyMales Females Sandwell
Respiratory disease
Circulatory diseases
Endocrine, nutritional andmetabolic diseases
Cancers
All causes
SMR
144.6
130.9
144.8
123.5
129.7
0 50 100 150 200 250
Source: ONS Mortality / HAD 1995
Rate per 100,000 residents
Males 264.1
Females 140.3
Sandwell Males 230.9
Sandwell Females 122.2
Alcohol deaths
Deaths from smoking
20.9%13.7%
17%
10.4%14.1%
12.4%
9.5%
4.4%6.2%
5.4%
6.9%5.3%
6%
6.6%4.2%
39
Percentage of working agepopulation on benefits
Source: DWP date 2008
SandwellTipton
2.4%
1.7%
3.2%
9.3%
4.2%
2.9%
2.3%
4.8%
12.2%
5.3%
30%
25%
20%
15%
10%
5%
0%
5 year average rate per 100,000
Source: ONS Mortality
0 5 10 15 20 25 30 35
Males 31.9
Females 16.2
Sandwell Males 27.5
Sandwell Females 10.3
KeyOther
Care
Lone parent
Incapacity
Job seeker
Oldbury
RowleyRegis
Smethwick
WestBromwich
Tipton
Wednesbury
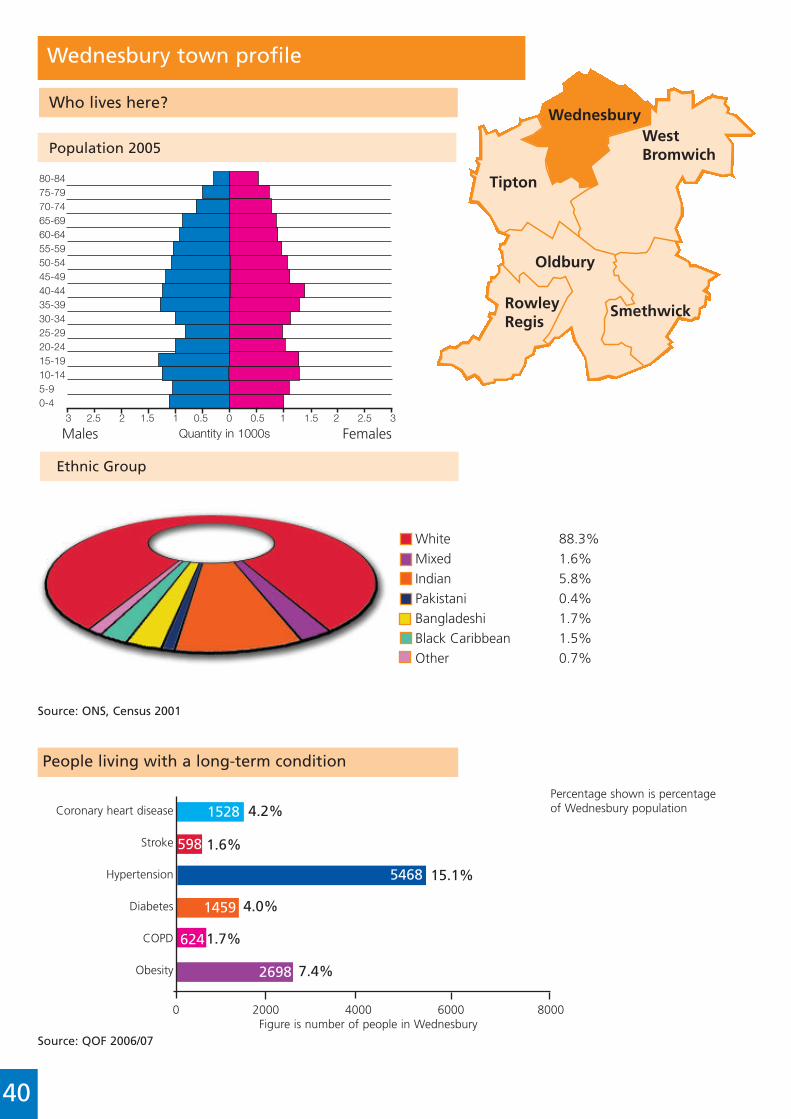
Wednesbury town profile
Who lives here?
Population 2005
3 2.5 2 1.5 1 0.5 0 0.5 1 1.5 2 2.5 3
80-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Males Females
wednesbury
Source: ONS, Census 2001
White 88.3%Mixed 1.6%Indian 5.8%Pakistani 0.4%Bangladeshi 1.7%Black Caribbean 1.5%Other 0.7%
People living with a long-term condition
Ethnic Group
Coronary heart disease
Stroke
Hypertension
Diabetes
COPD
Obesity
0 2000 4000 6000 8000Figure is number of people in Wednesbury
1528
598
5468
1459
624
2698
4.2%
1.6%
15.1%
4.0%
1.7%
7.4%
Source: QOF 2006/07
Quantity in 1000s
40
Percentage shown is percentageof Wednesbury population

0 50 100 150 200 250 300
Deaths
Top five causes of death
Standardised Mortality Ratio (SMR), all ages,2004-06 Compared to England
Source: ONSMortality as a percentage of all causes of death
Ischaemic heart disease
Cerebrovascular disease
Malignant neoplasms of
trachea, bronchus and lung
Pneumonia
COPD
0 5 10 15 20 25Percentage
KeyMales Females Sandwell
Respiratory disease
Circulatory diseases
Endocrine, nutritional andmetabolic diseases
Cancers
All causes
SMR
141.9
135.6
213.4
121.6
129.6
0 50 100 150 200 250
Source: ONS Mortality / HAD 1995
Rate per 100,000 residents
Males 274
Females 149.8
Sandwell Males 230.9
Sandwell Females 122.2
Alcohol deaths
Deaths from smoking
21.3%17.4%
19.2%
8.5%12.2%
10.4%
8.4%
3.8%5.7%
4.8%
5.5%5.4%5.5%
6.4%4.7%
41
Percentage of working agepopulation on benefits
Source: DWP date 2008
SandwellWednesbury
2.4%
1.7%
3.2%
9.3%
4.2%
2.6%
2.0%
3.5%
10.6%
3.9%
25%
20%
15%
10%
5%
0%
5 year average rate per 100,000
Source: ONS Mortality
0 5 10 15 20 25 30 35 40
Males 38.3
Females 13.2
Sandwell Males 27.5
Sandwell Females 10.3
KeyOther
Care
Lone parent
Incapacity
Job seeker
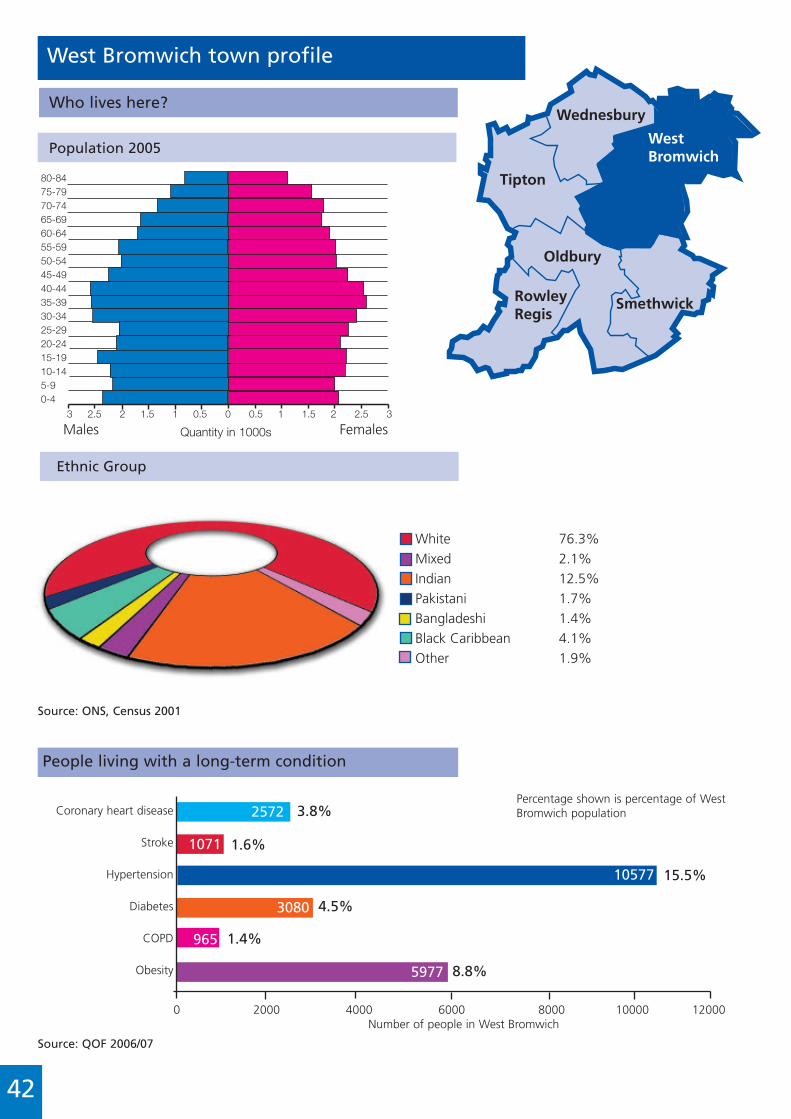
0 2000 4000 6000 8000 10000 12000Number of people in West Bromwich
Oldbury
RowleyRegis
Smethwick
Tipton
Wednesbury
WestBromwich
West Bromwich town profile
Who lives here?
Population 2005
3 2.5 2 1.5 1 0.5 0 0.5 1 1.5 2 2.5 3
80-8475-7970-7465-6960-6455-5950-5445-4940-4435-3930-3425-2920-2415-1910-145-90-4
Males Females
west bromwich
Source: ONS, Census 2001
White 76.3%Mixed 2.1%Indian 12.5%Pakistani 1.7%Bangladeshi 1.4%Black Caribbean 4.1%Other 1.9%
People living with a long-term condition
Ethnic Group
Coronary heart disease
Stroke
Hypertension
Diabetes
COPD
Obesity
2572
1071
10577
3080
965
5977
3.8%
1.6%
15.5%
4.5%
1.4%
8.8%
Source: QOF 2006/07
Quantity in 1000s
42
Percentage shown is percentage of WestBromwich population

0 50 100 150 200 250 300
Deaths
Top five causes of death
Standardised Mortality Ratio (SMR), all ages,2004-06 Compared to England
Source ONSMortality as a percentage of all causes of death
Ischaemic heart disease
Cerebrovascular disease
Malignant neoplasms of
trachea, bronchus and lung
Pneumonia
COPD
0 5 10 15 20 25Percentage
KeyMales Females Sandwell
Respiratory disease
Circulatory diseases
Endocrine, nutritional andmetabolic diseases
Cancers
All causes
SMR
111.3
110.4
170.0
101.1
107.4
0 50 100 150 200 250
Source: ONS Mortality / HAD 1995
Rate per 100,000 residents
Males 230
Females 116.3
Sandwell Males 230.9
Sandwell Females 122.2
Alcohol deaths
Deaths from smoking
21%15.7%
18.3%
10.1%12.6%
11.3%
6.7%
3.9%6.1%5%
5.3%3.8%4.5%
5.4%4.1%
43
Percentage of working agepopulation on benefits
Source: DWP date 2008
SandwellWestBromwich
2.4%
1.7%
3.2%
9.3%
4.2%
2.2%
1.7%
2.5%
9.0%
3.9%
25%
20%
15%
10%
5%
0%
5 year average rate per 100,000
Source: ONS Mortality
0 5 10 15 20 25 30 35
Males 26.0
Females 10.6
Sandwell Males 27.5
Sandwell Females 10.3
KeyOther
Care
Lone parent
Incapacity
Job seeker

Achievements 2007/08
AwardsRalph Smith
Appointed Honorary Research Fellow with the University of Leicester Geography Department.
Health Service Journal (HSJ) Award
CVD Project, ‘Highly Commended’ in computer-based decision making category,November 2007.
CVD Project, ‘top 5’ in chronic disease management category, November 2007.
PublicationsAli S, O’Callaghan V, Middleton J, Little R. The challenges of evaluating a health impactassessment, Journal of Critical Public Health (in press).
Ali S, O’Callaghan V, Middleton J. A case study of the ‘Towards 2010’ Programme HealthImpact Assessment. Journal of Environmental Assessment Policy and Management (JEAPM) (inpress).
Middleton J, Sidel V. Terrorism and public health. In Douglas J et al eds. Open University.Reader in Public Health. London: Sage books, 2007.
Dean A, Parkes M, Middleton J. Seamless delivery: the work of the Sandwell Joint PolicyUnit. Environmental Health News, 9th February 2007, p9.
Middleton J, Latif F. Gambling with the nation’s health. BMJ 2007: 334: 828-829.
Middleton J. Oceans of work: arms conversion revisited. Book review. Medicine Conflict andGlobal Survival 2007; 23: 325-327.
Middleton J, ed. Cares well? The 18th annual public health report for Sandwell, for 2006.West Bromwich: Sandwell Primary Care Trust, 2007.
Middleton J. Environmental health, climate chaos and resilience. Medicine Conflict andSurvival, Medicine Conflict and Survival, Volume 24, Supplement 1, S62-S79, April-June 2008.
Arif N, Middleton J. Towards an inclusive local economy: the work of Sandwell Ideal for all.Medicine Conflict and Survival, Volume 24, Supplement 1, S114-S117, April-June 2008.
Middleton J. Health and human rights in Sandwell and abroad, editorial. Medicine Conflictand Survival, Volume 24, Supplement 1, S2-S7, April-June 2008.
Commentary on: Goldberger J, Waring CH, Tanner WF (1923). Pellagra prevention by dietamong institutional inmates. Public Health Reports 38:2361-68. cite as: Middleton J (2008).Pellagra and the blues song ‘Cornbread, meat and black molasses’. James Lind Library(www.jameslindlibrary.org). Accessed Friday 21 March 2008
Marshall T, Westerby P, Fairfield M, Chen J, Fairfield M, Harding J, Westerby R, Ahmad R,Middleton J. Evaluation of a pilot project for primary care based prevention, BMC PublicHealth 2008, 8: 73.
Pitches D, Middleton J. Teenage pregnancy: the influence of the school calender.(submitted).
Ach
ieve
men
ts20
07/0
8
44
PresentationsShaukat Ali and Ralph Smith
Geographical Information Systems (GIS) as a tool for aiding health impact assessments. 8thInternational Health Impact Assessment Conference, Dublin, 2007.
Marie Carroll
A collaborative approach to delivering a workplace health programme. Royal College of NursingOccupational Health Conference, Cardiff.
A collaborative approach to preparing local businesses for smoke-free legislation and reducingprevalence in routine and manual workers. A Call to Action! Successful Tobacco Control for theFuture. Wales
Dr John Middleton
Doctor write me a prescription for the blues. Birmingham University, School of Public Health andMusic Faculty, January 17th 2007.
Commissioning for health and wellbeing, the West Midlands meeting of the Association ofDirectors of Social Services March 9th 2007.
Teaching Public Health Networks. Welcome to the West Midlands Network. Opening presenta-tion, Holly Lodge School, Smethwick, June 7th 2007.
Faculty of Public Health Conference Eastbourne. Organised seminar on floor target action plansfor spearhead PCTs; presented teenage pregnancy work. June 2007.
Environmental health, climate chaos and resilience Birmingham University International Appliedsocial science students conference. Organised by Sandwell PCT, JPU in Sandwell Independent liv-ing Centre on Diversity and Health. July 2007.
Motovun Istria Croatia, international Summer School in Health Lectures x 2 on mental health pol-icy and alcohol and young people. July 2007.
School nursing: from nit nurse to eco warrior? Presentation and participation in school nursesconference. Sandwell, September 2007.
Twenty years of Sandwell Health; PCT AGM, September 2007.
Black Country Public Health Teaching Network presentation: Casinos, gambling and public health(not registered in FPH submission. 14/12/07)
Ralph Smith
Mapwell – 3 decades of Health GIS and joint working in Sandwell. Mapping the way to health:AGI Health Special Interest Group seminar, November 2007
Dr Jenny Chen, Paul Westerby, Mary Fairfield and Dr Tom Marshall
The Sandwell Programme: Piloting Cardiovascular Disease Prevention in Primary Care. Faculty ofPublic Health Annual conference 2007
Conferences organisedDr John Middleton
Sandwell Health’s Other Economic Summit, Sandwell PCT, Sandwell Council, SandwellIndependent Living Centre, June 8th 2007
Diversity and health seminar Sandwell PCT, Sandwell MBC, Sandwell Independent Living Centre,Birmingham University Applied Social Studies International Division. July 13th 2007
45

AcknowledgementsThis report has been produced by the joint efforts of the following people who eithercontributed to the writing or provided data and information:
Individuals in the Public Health Team Shaukat Ali
Marie Carroll
Dr Jenny Chen
Dr Chris Chiswell
Alan Dean
Sam Hay
Kath Hosskinson
Wafia Hussain
Eileen Kibbler
Dr Adam Low
Dr John Middleton
Hope Ojukwu
Vicky O’Callaghan
Ralph Smith
Katie Spence
Mary Tooley
Dr Kate Warren
Dr Richard Wilson
Responsibility for the opinions expressed in this report rest with the Editor, Dr John Middleton,Director of Public Health. Any errors or points of clarification that need to be further addressedshould be forwarded to him at [email protected]
Additional InformationDetailed reports that make up Sandwell’s Public Health Annual Report for 2007/08 are containedon the enclosed CD. It features a full set of the Public Health Archive data sets for reference.
l If the CD is not attached, you can request a copy by telephoning: 0845 155 0500
This document is also available for download on Sandwell PCT’s website.Go to: www.sandwell-pct.nhs.uk and click on ‘Publications’.
46
Ack
no
wle
dg
emen
ts

l Arts in Health Strategy
l Arts in Health Strategy Plan
l Bowel Cancer Screening
l Cancer Awareness Case Study
l Carers Strategy
l Draft Anti-Poverty Strategy
l Draft Community Development Strategy
l Draft Personalisation Strategy
l Draft response to the Communities in Control consultation
l Full CLAHRC bid
l Growing Healthy Communities: A Draft Community Agriculture Strategy
l Health Protection Report
l Health Trainers Strategy
l Joint Strategic Needs Assessment (JSNA)
l Leeds University Sandwell Carers Report
l Neighbourhood Employment and Skills Plans(NESPs) for Sandwell Towns
l Parenting Needs Assessment
l PCT Patient Public Involvement Strategy
l Public Health Archive
l Report on Sandwell Health Other Economic Summit: Fat Chances for Food and Health
l Respiratory Health
l Review of Children & Young People With Special Education Needs and/or Disabilities
l Sandwell Local Area Agreement (LAA) Implementation Plan
l Sandwell Works
l Scrutiny briefing paper on the Communities in Control White Paper
l UK Research Partnership's report: Nourishing the Local Economy
l Urban Living – older people living in larger properties
l Valuing People: A Review of Learning Disabilities in Sandwell
l Workwell
47
Contents of the CD
This CD contains PDF files in high andlow resolution of the Sandwell PCT 2007/08
Public Health Annual Reportand further support documents for the
annual report
Crunch Time for Health in Sandwell
Public Health Annual Report 2007/08
SandwellPrimary Care Trust
NHS

ISBN 978-1-900471-09-1Designed and produced by Hyland Freeman Ltd
Content: Red Cat [email protected]





























