Embed Size (px)
Citation preview

EARN
3 CECREDITS
This course was written for dentists, dental hygienists, and dental assistants.
SUPPLEMENT TO ENDEAVOR PUBLICATIONS
PUBLICATION DATE: MAY 2019
EXPIRATION DATE: APRIL 2022
Lip incompetence: Causes, symptoms, and treatment considerationsA peer-reviewed article written by Angie Lehman, RDH, COM
© M
arin
a M
oroz
ova
| Dre
amst
ime.
com

EARN
3 CECREDITS
Go online to take this course.
DentalAcademyofCE.comQUICK ACCESS CODE 15348
This continuing education (CE) activity was developed by the PennWell dental group, an operating unit of Endeavor Business Media, with no commercial support.
This course was written for dentists, dental hygienists, and dental assistants, from novice to skilled.
Educational methods: This course is a self-instructional journal and web activity.
Provider disclosure: Endeavor Business Media neither has a leadership position nor a commercial interest in any products or services discussed or shared in this educational activity, nor with the commercial supporter. No manufacturer or third party had any input in the development of the course content.
Requirements for successful completion: To obtain three CE credits for this educational activity, you must pay the required fee, review the material, complete the course evaluation, and obtain a score of at least 70%.
CE planner disclosure: Laura Winfield, Endeavor Business Media dental group CE coordinator, neither has a leadership nor commercial interest with the products or services discussed in this educational activity. Ms. Winfield can be reached at [email protected]
Educational disclaimer: Completing a single continuing education course does not provide enough information to result in the participant being an expert in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
Image authenticity statement: The images in this educational activity have not been altered.
Scientific integrity statement: Information shared in this CE course is developed from clinical research and represents the most current information available from evidence-based dentistry.
Known benefits and limitations of the data: The information presented in this educational activity is derived from the data and information contained in reference section. The research data is extensive and provides a direct benefit to the patient and improvements in oral health.
Registration: The cost of this CE course is $59 for three CE credits.
Cancellation and refund policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting Endeavor Business Media in writing.
PennWell / Endeavor Business Media designates this activity for three CE credits.
Dental Board of California: Provider 4527, course registration number CA code:
03-4527-15348.
“This course meets the Dental Board of California’s requirements for 3 units of continuing education.”
PennWell Corporation is designated as an approved PACE program provider by the Academy of General Dentistry (AGD). The formal continuing dental education programs of this program provider are accepted by the AGD for fellowship, mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from (11/1/2015) to (10/31/2019) Provider ID# 320452.
PennWell is an ADA CERP–recognized provider
ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP does not approve or endorse individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry.
Concerns or complaints about a CE provider may be directed to the provider or to ADA CERP at ada.org/goto/cerp.
Lip incompetence: Causes, symptoms, and treatment considerationsABSTRACTLip competency plays an important role in growth and development within the craniofacial complex. It is an essential component of proper oral rest pos-ture. When lip incompetency occurs, function, growth, esthetics, speech, and breathing can all be affected. Determining the underlying cause is an essential part of properly treating this aspect of oral rest posture. Traditionally, treatment has often included orthodontic treatment for correction of overjet, Botox injec-tions, or surgery. However, the most effective techniques include addressing the underlying cause and improving the function of the lips rather than only addressing the cosmetic appearance of the lips. Orofacial myofunctional ther-apy has proven to be effective in treating lip competency issues and should be considered a valid treatment option to be used in conjunction with orthodon-tic treatment, and before Botox and surgery are considered.
OBJECTIVES1. Understand the importance of lip competence as it relates to correct oral
rest posture2. Review anatomy of the orbicularis oris complex3. Learn how to recognize underlying factors that lead to lip incompetency4. Recognize how therapy for lip incompetence can be an essential adjunct to
orthodontic treatment and orthognathic surgery

Depressor labii inferioris
Mentalis
Zygomaticus minor
Zygomaticus major
Modiolus
Risorius
Platysma
Depressor anguli oris
Levator labii superioris
Buccinator
Levator anguli orisLevator labii superioris alaeque nasi
Orbicularis oris
86 DentalAcademyofCE.com
D E N T A L A C A D E M Y O F C O N T I N U I N G E D U C A T I O N
UNDERSTANDING PROPER LIP POSTUREOral rest posture refers to the positioning of the jaws, lips, tongue, and facial muscles in repose. Correct oral rest posture includes a tongue resting on the palate, 2–3 mm of freeway space between the molars, nasal breathing, and gently sealed lips. Properly positioned lips are a very important aspect of overall correct oral rest posture. When the lips are at rest, the ideal positioning would be gently sealed lips; however, an interla-bial gap of 1–3 mm is also considered to be within the normal limits of a correct lip posture.1-3 Correct oral rest posture is an essential component of maintaining good oral equilibrium.4 Sealed lips act as nature’s orthodontic retainers for the incisors when the lower lip covers a portion of the max-illary incisors. When muscles in the oro-facial complex are positioned properly for prolonged periods of time, they aid in guid-ing growth and development via light, con-stant forces.4 Inversely, when the orofacial muscles are positioned in an incorrect loca-tion for prolonged periods of time, there is a negative effect on growth, development, and function. This article is dedicated spe-cifically to exploring lip posture, the nega-tive consequences of lip incompetence, and various treatments for a short upper lip and/or poor lip seal.
When the lips are routinely positioned 4 mm or more apart, and the individual strug-gles to keep the lips sealed at rest, or he or she is unable to seal the lips without strain on
the surrounding facial muscles, we consider this to be lip incompetence.1,5,6 Although often concomitant, lip incompetence is not exclusively associated with mouth breath-ing. While chronic mouth breathers do have lip incompetency, it is physically possible for some individuals to have a poor labial seal, yet still primarily use the nose to breathe.4 In true mouth-breathing cases, the jaw is also open beyond the normal freeway space and the tongue is positioned low, and often for-ward, in the mandible. In these instances, full oral rest posture rehabilitation is necessary.
GROWTH OF THE LIPSOne consideration that needs to be made before addressing a lip incompetency issue is the age of the individual. During the period of mixed dentition, vertical growth of the lips lags slightly behind vertical growth of the facial skeleton.1-3 The upper lip grows at a steadier rate than the lower lip, reaching its full potential by age 17–19, while the lower lip experiences an acceleration of growth between the ages of nine and 13, with com-pletion of growth by age 18–19.3 Lip thick-ness peaks during adolescence, followed by gradual loss of thickness in adulthood.1 Learning to recognize the difference between normal, mixed-dentition-related lip parting and true lip incompetence is an important part of the treatment process.
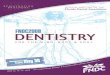
OVERVIEW OF ORBICULARIS ORIS COMPLEXAlthough we typically think of orbicularis
oris as a sphincter muscle that is responsi-ble for lip seal, this muscle is unique in that it is a complex muscle serving as a point of insertion for 10 different muscles, each with their own role to play in determining proper function of the lips. Orbicularis oris is inner-vated by the mandibular marginal and lower buccal branches of the facial nerve (cranial nerve VII) and receives its blood supply from the superior and inferior labial branches of the facial artery.7
The risorius and buccinator muscles insert at the corners of the lips and are responsible for retraction of the lips. For elevation of the upper lip, the levator labii superioris, zygomaticus minor, and levator labii superioris alaeque nasi all insert into the superior orbicularis oris to aid in elevation of the upper lip. Zygomaticus major inserts laterally and aids in elevation and retraction of the lips, assisting in the smile. Levator anguli oris pulls the corners of the mouth up and medially. The depressor labii inferi-oris depresses the lower lip (pout), while the depressor anguli oris depresses the angle of the mouth ( frown).7,8
It is also important to remember that mouth closure is not just dependent on com-petent lips, but on a stable jaw at rest. Proper jaw positioning includes a freeway space of 2–3 mm between molars3 as well as a deli-cate balance between the forces of strong masticatory muscles pulling above, and grav-ity and hyoid muscles pulling from below.9
CAUSES OF LIP INCOMPETENCEThere can be a variety of reasons that an indi-vidual is unable to keep the lips sealed at rest. It is often observed that those with bimax-illary dentoalveolar protrusion, commonly known as buckteeth, experience lip incom-petence due to tooth position. Although it seems logical to treat primarily with ortho-dontics, it is important to understand why the teeth are protruding, as it is often from an overlooked oral rest posture issue and subsequent orofacial muscle dysfunction. Form and function have a bidirectional rela-tionship. Changes in function of the lips can alter the form of the orofacial complex, just as abnormal alterations in form can cause function to suffer. Therefore, treatment needs to focus on both hard and soft tis-sues in order to both treat the underlying

DentalAcademyofCE.com 87
D E N T A L A C A D E M Y O F C O N T I N U I N G E D U C A T I O N
cause and improve the chances for good orthodontic retention.
One of the most commonly observed causes of poor lip seal and mouth breath-ing is allergic rhinitis and other airway obstructions such as enlarged tonsils and adenoids.10 When an individual is unable to breathe through the nose for prolonged periods of time, the lips must remain apart, and the tongue must drop low in the oral cavity in order to open the oral airway. If this only happens during the occasional cold or sinus infection, function returns to normal as soon as the nasal airway is again patent. However, in cases that involve poor nasal patency for extended periods of time, the muscles will alter their function as well as their rest posture, and a new, incorrect habit is established. In cases of chronic mouth breathing, upper lip tonicity is lost,2 resulting in a compounding inability to keep the lips gently sealed, sometimes even after the aller-gies or nasal obstructions are addressed.11 If you recall that good oral rest posture is essential in maintaining oral equilibrium and therefore good orofacial growth, it is easy to see how a chronically stuffy nose can not only lead to poor lip seal, but actually cause flaring of the incisors and supraerup-tion of posterior teeth (due to a prolonged increase in freeway space), making proper lip seal even more difficult. The end result is an elongated face with strained facial muscles that have developed numerous compensa-tions in order to function.
Although the airway’s influence on lip posture is the most recognizable, an under-developed mandible is also a common cause of poor lip approximation. A retrognathic mandible can be genetic (such as in Pierre Robin sequence) or caused by habits that result in either poor oral rest posture or insufficient use of masticatory muscles that stunt growth of the mandible.12 Structural soft-tissue issues such as tongue-tie can also influence growth of the mandible,13 and a tight maxillary labial frenum, or upper lip tie, can prevent the upper lip from comfort-ably meeting the lower lip.7,14
Low muscle tone in syndromic individu-als can also result in poor lip competence. These individuals typically have poor jaw stability and weak masseters, resulting in a habitual open-mouth posture.15 For these
particular individuals, it is important to have a larger team approach to treatment. They will benefit most from a team of profession-als—occupational therapists, physical thera-pists, and speech therapists who specialize in oral motor therapy as well as orofacial myofunctional therapy—working collab-oratively toward a common goal of good lip seal as well as proper feeding, breath-ing, and speech.
COMMON PROBLEMS ASSOCIATED WITH LIP INCOMPETENCEA change in occlusion and alterations in oro-facial growth can result from poor lip seal. As previously mentioned, poor lip compe-tence will actually lead to flaring of the inci-sors and an increase in overjet. When the lack of lip seal is combined with a jaw that is open beyond the normal freeway space, supraeruption can occur, leading to an ante-rior open bite and elongation of the facial skeleton. If soft-tissue dysfunction is not addressed during orthodontic treatment, retention will be difficult and orthodontic relapse may occur.14
Speech sounds can also be affected by lip incompetence. Bilabial sounds /p/, /b/, and /m/ require both the top and bottom lip to meet comfortably. It is common in individu-als with a short upper lip to make substitu-tions for bilabial sounds. These individuals would benefit from speech therapy as an adjunct to their treatment.
Drooling can be a common problem asso-ciated with poor lip seal. These individuals
may also have decreased awareness of their saliva, or poor handling of their saliva due to tongue posture issues.15 While some indi-viduals drool excessively, others suffer from xerostomia. Chapped lips and inflamed gin-giva on the maxillary anterior teeth can be common, as well as an increase in caries from reduced salivary flow.2
Poor lip competency also creates a cos-metic concern for patients and can change the way they are perceived by others.3 It is an unfortunate reality that those with poor lip seal and mouth-breathing habits are per-ceived as less intelligent by those around them. Several studies show that facial attrac-tiveness is directly related to our perception of an individual’s intelligence and social skills and has an influence on career success.3
TREATMENT GOALSIf we observe the natural smiles of males and females, we will notice that the lip line in females is an average of 1.5 mm higher than the lip line in males, showing an aver-age of 1–2 mm of gingival display, which is considered normal.16 Any amount greater than 2 mm could be considered a “gummy smile” and may be a contributing factor in the poor competency of the lips. When fully grown, the average length of the philtrum (measured from the subnasale to the ver-milion border at the midline of the upper lip) is 20 mm for females and 23 mm for males,16 but perhaps of more importance is the relationship of the lips to the maxil-lary incisors rather than the actual length of
When the lack of lip seal is combined with a jaw that is open beyond the normal freeway space, supraeruption can occur, leading to an anterior open bite and elongation of the facial skeleton.
Poor lip competency also creates a cosmetic concern for patients and can change the way they are perceived by others.

88 DentalAcademyofCE.com
D E N T A L A C A D E M Y O F C O N T I N U I N G E D U C A T I O N
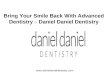
the upper lip.1,3 No matter what treatment modality is used, it is essential that the lips not only appear more esthetically pleasing, but that all aspects of function improve as well, specifically during chewing and swal-lowing, speech production, and saliva han-dling ( figure 1).
ADDING A NEW APPROACH TO TRADITIONAL TREATMENTWhen the focus is placed on bimaxillary pro-trusion as a “tooth problem” rather than a “lip problem,” the natural thought process in fixing the issue would be to retract the inci-sors, sometimes at the expense of extraction of healthy premolars, in order to create room and lessen the unwanted facial appearance that comes with protruding teeth. If the inci-sor flaring is a result of mouth breathing and poor tongue posture, just changing structure will not automatically mean that muscles will know how to overcome former com-pensatory patterns and begin to function
correctly. One factor of this treatment plan that is often overlooked is the negative con-sequence of lessening space for the tongue to rest and function appropriately, often mak-ing oral rest posture and breathing worse.17
When orthodontic treatment is used in conjunction with orofacial myofunctional therapy, both the dentist and the therapist can collaborate and change both form and function, leading to a much more favor-able outcome for the patient ( figure 2). It is often surprising to see how much inci-sor flaring is reduced simply by working on lip strength and competence using neuro-muscular exercises. When these exercises are used in conjunction with orthodontics, changes happen rapidly and set the patient up for better retention after completion of treatment.14
When surgery is the best solution for cor-rection of vertical maxillary excess, via either orthognathic or lip-repositioning surgery, special attention still needs to be paid to
rehabilitating proper function of the lips and surrounding facial muscles. Orofacial muscles share many functions, including breathing, speaking, swallowing, and facial expression. Proper function requires changes in both shape and positioning of these mus-cles. Acquiring, generalizing, and habituat-ing correct muscle patterns does not happen by chance, but by following specific neuro-physiological principles.14 If we consider the common practices of other areas of medi-cine such as orthopedics, it is expected that a surgeon will collaborate with a physical therapist in order to address function before and after orthopedic surgery. Yet, we rou-tinely perform orthognathic surgery without addressing oral function via a skilled orofa-cial myofunctional therapist. Collaboration between oral surgeons and therapists is an underutilized, yet essential part of patient treatment.
Botox injections can be beneficial ( fig-ure 3) when the upper lip is hypertonic and there is hyperactivity of the elevator mus-cles. It is important to note that the changes achieved with Botox are temporary and need to be repeated in order to maintain the posi-tive results. When Botox is injected into the muscles at the proper dose, it results in par-tial chemical denervation of the muscle.18 This localized reduction in muscle activity helps to relax the lip, leading to a decrease in gingival display. It can also be used to relax tension in the mentalis muscles. Botox, how-ever, cannot address or improve function of the lips, and in some cases, may temporar-ily make function worse. It is recommended that lip seal is improved first through ther-apy before considering Botox as an adjunct to treatment.
TREATMENT PLANNING AND THERAPY FOR LABIAL MUSCLESBefore starting an exercise program for incompetent lips, it is recommended that baseline measurements be taken in order to gauge progress. Lip strength can be obtained by a simple button pull and lip meter. The lips should be evaluated together and separately, as one lip is often much more toned than the other, espe-cially in cases of an everted lower lip.19 A normal range of lip strength is between three and five pounds.20 The length of the FIGURE 1: Changes in lip competence and facial appearance after five months of orofacial myofunctional therapy

DentalAcademyofCE.com 89
D E N T A L A C A D E M Y O F C O N T I N U I N G E D U C A T I O N
philtrum should also be recorded while the patient is in a relaxed state, with the lips in their usual position. From this position, it is also possible to measure the interla-bial gap, determining how far apart the lips are at rest.
Next, evaluation of the range of motion of the orbicularis oris complex is observed by having the patient round and spread his or her lips, accomplished by having the patient repeatedly say “ooo-eee.” The clinician should pay special attention to compensatory patterns, often employed by moving the mandible forward to assist in rounding of the lips. Asymmetry may also be observed. The correct or incorrect use of the lips during speech can also be eval-uated, specifically on bilabial sounds /p/, /b/, and /m/. Eating and drinking should be observed since poor labial posture sig-nificantly contributes to deficits in the oral phase of swallowing.7 An assessment of nasal patency is essential when deter-mining whether or not an ENT or allergist
should be involved in care. Finally, ques-tioning the patient (or parent) is important, as they can shed light on whether the lip incompetence is happening intermittently (perhaps only during times of concentration on a task), or if the lips never approximate during the day or night.
A variety of exercises can be used to improve lip competence.3,6,9,20 A combina-tion of passive and static stretching—either manually, or by use of a lip shield, cotton roll, or other tool—can be used to improve lip length, increase range of motion, and change lip morphology.9 In combination with stretching, resistance exercises, coor-dination exercises, and proprioceptive tasks are also beneficial to improve strength of the lips. Since oral muscle movements are associative in nature, working on a proper lip seal will help facilitate tongue retraction in patients with poor tongue posture.7 Add-ing systematic jaw exercises will also help aid in maintaining proper tongue posture and appropriate dental freeway space.13
When judging the value and efficacy of lip exercises, it is important to consider the effect of the exercise on tooth position, the morphology of the lips, and the nat-ural function of the lips.6 Once the exer-cises have been chosen, it is recommended that they be performed three times a day for a total of 10 minutes a day.6,20 Achiev-ing habituation of new muscle patterns is needed to maintain the positive changes made through therapy.
CONCLUSIONWhen treating lip incompetence, address-ing both form and function is essential. The clinician must first investigate the source of the poor lip seal, identify the symptoms that need to be addressed, and then implement a treatment plan that focuses on correcting both structure and soft-tissue dysfunction. Using neuromus-cular exercises in a systematic and sequen-tial way has been proven to work, but they are often underutilized.
FIGURE 2: Team approach between therapist and orthodontist leads to a stable outcome. Left: Pretreatment. Middle: After orofacial myofunctional therapy. Notice the
reduction in overjet/flaring. Right: After completion of orthodontic treatment.

90 DentalAcademyofCE.com
D E N T A L A C A D E M Y O F C O N T I N U I N G E D U C A T I O N
REFERENCES1. Graber LW, Vanarsdall Jr RL, Vig KWL, Huang GJ.
Orthodontics: Current Principles and Techniques.
6th ed. St. Louis, MO: Elsevier; 2016:217-272, 320.
2. Proffit WR, Fields HW, Sarver DM. Contemporary
Orthodontics. 5th ed. St. Louis, MO: Mosby;
2013:164-166.
3. Hanson ML, Mason RM, Vaidergorn B. Orofacial
Myology: International Perspectives. 2nd ed.
Springfield, IL: Charles C Thomas Pub. Ltd.;
2003:96-97.
4. Proffit WR. Equilibrium theory revisited: factors
influencing position of the teeth. Angle Orthod.
1978;48(3):175-186.
5. Mason RM. Lip Incompetence. Orofacial Myology
website. http://www.orofacialmyology.com/.
Accessed July 21, 2018.
6. Ingervall B, Eliasson GB. Effect of lip training
in children with short upper lip. Angle Orthod.
1982;52(3):222-233.
7. Gatto KK. Understanding the Orofacial Complex:
The Evolution of Dysfunction. Denver: Outskirts
Press, Inc.; 2016:41-44, 145.
8. Volker JH. Easy notes on orbicularis oris. Earth’s
Lab website. https://www.earthslab.com/anatomy/
orbicularis-oris/. Published February 1, 2018.
Accessed July 22, 2018.
9. von Piekartz HJM. Craniofacial Pain:
Neuromusculoskeletal Assessment, Treatment
and Management. Oxford: Butterworth
Heinemann; 2007:246, 617-632.
10. Valera FC, Travitzki LV, Mattar SE, Matsumo MA,
Elias AM, Anselmo-Lima WT. Muscular, functional
and orthodontic changes in preschool children
with enlarged adenoids and tonsils. Int J Pediatr
Otorhinolaryngol. 2003;67(7):761-770.
11. Valera FC, Trawitzki LV, Anselmo-Lima WT.
Myofunctional evaluation after surgery for tonsils
hypertrophy and its correlation to breathing
pattern: A 2-year-follow up. Int J Pediatr
Otorhinolaryngol. 2006 Feb;70(2):221-25.
12. de Jong WC, Korfage JAM, Langenbach GEJ. The
role of masticatory muscles in the continuous
loading of the mandible. J Anat. 2011;218(6):625-
636. doi: 10.1111/j.1469-7580.2011.01375.x.
13. Bahr D. Feed your baby and toddler right: Early
eating and drinking skills encourage the best
development. Arlington, TX: Future Horizons Inc.;
2018.
14. Paskay LC. Orofacial myofunctional disorders:
assessment, prevention and treatment. Journal
of the American Orthodontic Society. 2012;34-40.
15. Marshalla P. How to Stop Drooling. 2nd ed.
Marshalla Speech and Language; 2009:13, 49.
16. Sabri R. The eight components of a balanced
smile. J Clin Orthod. 2005;39(3):155-167.
17. Kahn S, Ehrlich PR. Jaws: The Story of a Hidden
Epidemic. Stanford, CA: Stanford University
Press; 2018:113-117.
18. Aly LA, Hammouda NI. Botox as an adjunct to lip
repositioning for the management of excessive
gingival display in the presence of hypermobility
of upper lip and vertical maxillary excess. Dent
Res J. 2016;13(6):478-483.
19. de Andrada e Silva MA, Marchesan I, Ferreira
LP, Schmidt R, Ramires RR. Posture, lips and
tongue tone and mobility of mouth breathing
children. Revista CEFAC. 2012;14(5):853-860.
20. Holtzman SR. Orofacial Myology: From Basics
to Habituation. 2nd ed. Orlando: Neo-Health
Services; 2014.
OTHER SOURCES• Moschik CE, Pichelmayer M, Coulson S, Wendl
B. Influence of myofunctional therapy on upper
intercanine distance. Journal of Dentistry, Oral
Disorders & Therapy. 2015;3(1):1-7.
• Rao AG, Koganti VP, Prabhakar AK, Soni S. Modified
lip repositioning: A surgical approach to treat
the gummy smile. J Indian Soc Periodontol.
2015;19(3):356-359. doi: 10.4103/0972-124X.152400.
• Subtelny JD. Oral respiration: facial
maldevelopment and corrective dentofacial
orthopedics. Angle Orthod. 1980;50(3):147-164.
ANGIE LEHMAN, RDH,
COM, has been certified by the
International Association of
Orofacial Myology (IAOM) and
has been practicing orofacial
myology exclusively since 2012.
She currently serves on the
board of directors for the IAOM. Angie is the owner
of Oral Myofunctional Therapy of York, a private
practice in York, Pennsylvania, that provides
myofunctional therapy to children and adults. She
also provides continuing education for dental and
medical professionals. Her passion is to see all
dental and medical professionals work
collaboratively to better understand oral function
and craniofacial development and incorporate
therapy into their specific areas of care.
FIGURE 3: Lip posture and natural smile before and after therapy. This patient was referred for Botox after
therapy due to lingering tightness in the mentalis muscle.

DentalAcademyofCE.com 91
Q U E S T I O N S
ONLINE COMPLETIONTake this test online for immediate credit. Go to dentalacademyofce.com and log in. If you do not have an account, sign up using enrollment key DACE2019. Then, find this course by
searching for the title or the quick access code. Next, select the course by clicking either the “ENROLL” or “$0.00” option. Continue by placing the course in your cart and checking out, or press
“Start.” After you have read the course, you may take the exam. Search for the course again and place the exam in your cart. Check out, take the exam, and receive your credit!
QUICK ACCESS CODE 15348
1. Correct oral rest posture does not include:A. 2–3 mm freeway space between the jawsB. Lips gently sealedC. Nasal breathingD. Tongue resting between the teeth
2. Which is considered a normal interla-bial gap?A. 3–4 mmB. 1–2 mmC. 1–3 mmD. 2–5 mm
3. Properly positioned orofacial muscles aid in guiding growth via:A. Heavy, intermittent forcesB. Light, constant forcesC. Light, intermittent forcesD. Heavy, constant forces
4. Signs of lip incompetence include:A. More than 4 mm interlabial gapB. Inability to seal the lips comfortably at restC. Strain on surrounding facial muscles upon
closureD. All of the above
5. Which statement concerning lip/facial growth is true?A. Horizontal growth of the lips lags behind
growth of the facial skeletonB. The lower lip grows at a steadier rate than
the upper lipC. Vertical growth of the lips lags behind ver-
tical growth of the facial skeletonD. The age of the individual does not matter
when addressing lip incompetence
6. Growth of the upper lip reaches its full potential by age:A. 17–19B. 16–18 C. 15–16 D. 18–20
7. Lip thickness peaks during:A. ChildhoodB. AdolescenceC. AdulthoodD. Never
8. The orbicularis oris muscle is a com-plex muscle that serves as the inser-tion point for:A. Seven different musclesB. Eight different musclesC. Nine different musclesD. 10 different muscles
9. Obicularis oris is innervated by which cranial nerve?A. Facial nerve B. Hypoglossal nerve C. Trigeminal nerve D. Vagus nerve
10. In addition to lip seal, mouth closure is dependent on:A. Jaw instability B. Jaw stabilityC. Weak masticatory musclesD. None of the above
11. A commonly observed cause of poor lip seal and mouth breathing is:A. Allergic rhinitisB. Enlarged tonsils C. Enlarged adenoids D. All of the above
12. Chronically stuffy noses can lead to: A. Poor lip sealB. Increase in dental freeway spaceC. Elongated face and flared incisorsD. All of the above
13. Retrognathia can be caused by:A. GeneticsB. Well-developed masticatory musclesC. Structural soft-tissue issues such as
tongue-tieD. Both A and C
14. Individuals with low muscle tone typi-cally have:A. Poor jaw stability and strong massetersB. Good jaw stability and weak massetersC. Good jaw stability and strong massetersD. Poor jaw stability and weak masseters
15. When lip incompetency is combined with an increase in the dental freeway space:A. Supraeruption of the molars can lead to an
open biteB. Elongation of the facial skeleton can occurC. Orthodontic retention is difficultD. All of the above
16. Bilabial sounds include:A. /p/, /b/, and /v/B. /p/, /v/, and /w/C. /p/, /b/, and /m/D. None of the above
17. Which are side effects of a poor lip seal?A. Drooling and poor saliva handlingB. Cosmetic concernsC. Chapped lips and inflamed gingivaD. All of the above
18. When observing natural smiles, we will notice that:A. Females have a lip line that is 1.5 mm lower
than malesB. Males have a lip line that is 1.5 mm higher
than femalesC. Females have a lip line that is 1.5 mm
higher than malesD. Lip lines of males and females are the same
19. In a fully grown adult, the average length of the philtrum is:A. 20 mm in males and 23 mm in femalesB. 15 mm in females and 17 mm in malesC. 20 mm in females and 23 mm in malesD. 18 mm in females and 20 mm in males

92 DentalAcademyofCE.com
Q U E S T I O N S
ONLINE COMPLETIONTake this test online for immediate credit. Go to dentalacademyofce.com and log in. If you do not have an account, sign up using enrollment key DACE2019. Then, find this course by
searching for the title or the quick access code. Next, select the course by clicking either the “ENROLL” or “$0.00” option. Continue by placing the course in your cart and checking out, or press
“Start.” After you have read the course, you may take the exam. Search for the course again and place the exam in your cart. Check out, take the exam, and receive your credit!
NOTES
QUICK ACCESS CODE 15348
20. More important than the numbers, it is essential that treatment helps to improve:A. Esthetics B. FunctionC. BothD. Neither
21. Orofacial muscles share which of the following roles?A. Speech and breathingB. Swallowing and breathingC. Facial expression and speechD. Breathing, speech, swallowing, and facial
expression
22. Orthognathic surgery can help:A. Correct vertical maxillary excess B. Reduce a gummy smileC. Teach proper function of lip musclesD. Both A and C
23. Botox is beneficial when elevator muscles are:A. Hypertonic and hyperactiveB. Hypotonic and hypoactiveC. Hypertonic and hypoactiveD. Hypotonic and hyperactive
24. Normal lip strength is between: A. 1 and 3 poundsB. 2 and 4 poundsC. 3 and 5 poundsD. 5 and 7 pounds
25. The philtrum length should be mea-sured while the lips are:A. Retracted into a smileB. Forced to closedC. In a natural, relaxed stateD. Pursed
26. Having the patient say “ooo-eee” allows the clinician to observe:A. Range of motion when rounding the lipsB. Range of motion when spreading the lipsC. Jaw compensations for poor range of
motionD. All of the above
27. Poor labial posture can contribute to deficits in the:A. Oral phase of swallowingB. Pharyngeal phase of swallowing C. NeitherD. Both
28. Assessment of lip function should include:A. Watching the patient eatB. Watching the patient speakC. Questioning parentsD. All of the above
29. Proper lip seal also helps to facilitate:A. Tongue elevationB. Tongue retractionC. Tongue cuppingD. Tongue narrowing
30. It is recommended that exercises be performed:A. Three times a weekB. Two times a dayC. Five times a monthD. Three times a day

Customer Service | Call (800) 633-1681
PUBLICATION DATE: JUNE 2019
EXPIRATION DATE: MAY 2022
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
28.
29.
30.
ANSWER SHEET
Lip incompetence: Causes, symptoms, and treatment considerations
Name: Title: Specialty:
Address: Email: AGD member ID (if applies):
City: State: ZIP: Country:
Telephone: Primary ( ) Office ( ) License renewal date:
Requirements for obtaining CE credits by mail/fax: 1) Read entire course. 2) Complete info above. 3) Complete test by marking one answer per question. 4) Complete course evaluation. 5) Complete credit card info or write check payable to Endeavor Business Media. 6) Mail/fax this page to DACE. A score of 70% is required for CE credit. For questions, call (800) 633-1681. Course may also be completed at dentalacademyofce.com.
EDUCATIONAL OBJECTIVES1. Understand the importance of lip competence as it relates to correct oral rest posture
2. Review anatomy of the orbicularis oris complex
3. Learn how to recognize underlying factors that lead to lip incompetency
4. Recognize how therapy for lip incompetence can be an essential adjunct to orthodontic treatment
and orthognathic surgery
COURSE EVALUATION1. Were the individual course objectives met?
Objective #1: Yes No Objective #2: Yes No
Objective #3: Yes No Objective #4: Yes No
Please evaluate this course by responding to the following statements using a scale of excellent (5) to poor (0).
2. To what extent were the course objectives accomplished overall? 5 4 3 2 1 0
3. Please rate your personal mastery of the course objectives. 5 4 3 2 1 0
4. How would you rate the objectives and educational methods? 5 4 3 2 1 0
5. How do you rate the author’s grasp of the topic? 5 4 3 2 1 0
6. Please rate the instructor’s effectiveness. 5 4 3 2 1 0
7. Was the overall administration of the course effective? 5 4 3 2 1 0
8. Please rate the usefulness and clinical applicability of this course. 5 4 3 2 1 0
9. Please rate the usefulness of the supplemental webliography. 5 4 3 2 1 0
10. Do you feel that the references were adequate? Yes No
11. Would you participate in a similar program on a different topic? Yes No
12. If any of the continuing education questions were unclear or ambiguous, please list them.
______________________________________________________________________________
13. Was there any subject matter you found confusing? Please describe.
______________________________________________________________________________
14. How long did it take you to complete this course?
______________________________________________________________________________
15. What additional continuing dental education topics would you like to see?
______________________________________________________________________________
Payment of $59 is enclosed. Make check payable to Endeavor Business Media
If paying by credit card, please complete the following: MC Visa AmEx Discover
Acct. number: ______________________________
Exp. date: __________________ CVC #: _________
Billing address: _____________________________
__________________________________________
Charges on your statement will show up as PennWell / Endeavor.
Mail/fax completed answer sheet to: Endeavor Business Media
Attn: Dental division 1421 S. Sheridan Rd.; Tulsa, OK 74112
Fax: (918) 212-9037
AGD Code 730
PLEASE PHOTOCOPY ANSWER SHEET FOR ADDITIONAL PARTICIPANTS.INSTRUCTIONS
All questions have only one answer. Grading of this examination is done manually. Participants will receive confirmation of passing by receipt of a verification form. Verification of Participation forms will be mailed within two weeks after taking an examination.
COURSE EVALUATION AND FEEDBACKWe encourage participant feedback. Complete the survey above and e-mail feedback to Aileen Gunter ([email protected]) and Laura Winfield ([email protected]).
COURSE CREDITS AND COSTAll participants scoring at least 70% on the examination will receive a verification form for three CE credits. The formal CE program of this sponsor is accepted by the AGD for fellowship and mastership credit. Please contact Endeavor for current term of acceptance. Participants are urged to contact their state dental boards for continuing education requirements. PennWell is a California CE provider. The California provider number is 4527. The cost for courses ranges from $20 to $110.
PROVIDER INFORMATIONPennWell is an ADA CERP–recognized Provider. ADA CERP is a service of the American Dental Association to assist dental professionals in identifying quality providers of continuing dental education. ADA CERP neither approves nor endorses individual courses or instructors, nor does it imply acceptance of credit hours by boards of dentistry. Concerns about a CE provider may be directed to the provider or to ADA CERP at ada.org/gotocerp/.
PennWell is designated as an approved PACE program provider by the Academy of General Dentistry. The formal continuing dental education programs of this program provider are accepted by the AGD for fellowship, mastership, and membership maintenance credit. Approval does not imply acceptance by a state or provincial board of dentistry or AGD endorsement. The current term of approval extends from 11/1/2015 to 10/31/2019. Provider ID# 320452.
RECORD KEEPINGEndeavor maintains records of your successful completion of any exam for a minimum of six years. Please contact our offices for a copy of your CE credits report. This report, which will list all credits earned to date, will be generated and mailed to you within five business days of receipt.
EDUCATIONAL DISCLAIMERCompleting a single CE course should not provide enough information to give participants the feeling that they are experts in the field related to the course topic. It is a combination of many educational courses and clinical experience that allows the participant to develop skills and expertise.
CANCELLATION AND REFUND POLICYAny participant who is not 100% satisfied with this course can request a full refund by contacting Endeavor in writing.
IMAGE AUTHENTICITYThe images provided and included in this course have not been altered.
© 2019 by the Academy of Dental Therapeutics and Stomatology, a division of Endeavor Business Media
PUBLICATION DATE: MAY 2019
EXPIRATION DATE: APRIL 2022