Embed Size (px)
Citation preview

CPAP therapyin the Newborn
Thrathip Kolatat M.D.
Neonatal Intensive Care Unit
Department of Pediatrics
Faculty of Medicine Siriraj Hospital

Continuous Positive Airway Pressure (CPAP)

CPAP
ll the application of positive the application of positive airway pressure airway pressure throughout the respiratory throughout the respiratory cycle during spontaneous cycle during spontaneous respirationrespiration
ll historyhistoryll Harrison 1968: described Harrison 1968: described
grunting in neonates as grunting in neonates as naturally producing endnaturally producing end--expiratory pressureexpiratory pressure
ll Gregory et al, 1971: Gregory et al, 1971: introduced the clinical use introduced the clinical use of distending pressure in of distending pressure in neonatesneonates

Physiologic effects of CPAP
ll pulmonary mechanicspulmonary mechanicsll cardiovascular stabilitycardiovascular stabilityll pulmonary vascular resistancepulmonary vascular resistance

Pulmonary effects
l decrease respiratory rate, tidal volume and minute volume
l regularization of respirationl increase FRC and thoracic gas volumel decrease lung compliance and
dynamic compliancel decrease total airway resistancel protective effect on surfactant

Control
+4 torr
2 3 4Age (days)
0
5
10
15
20FR
C (ml
/kg)
Effect of CPAP on FRC in the infants with RDS

CPAP (torr)4 8 12 16 200
100
200
300
Pa (t
orr)
o 2
Effect of different CPAP levels on PaO2
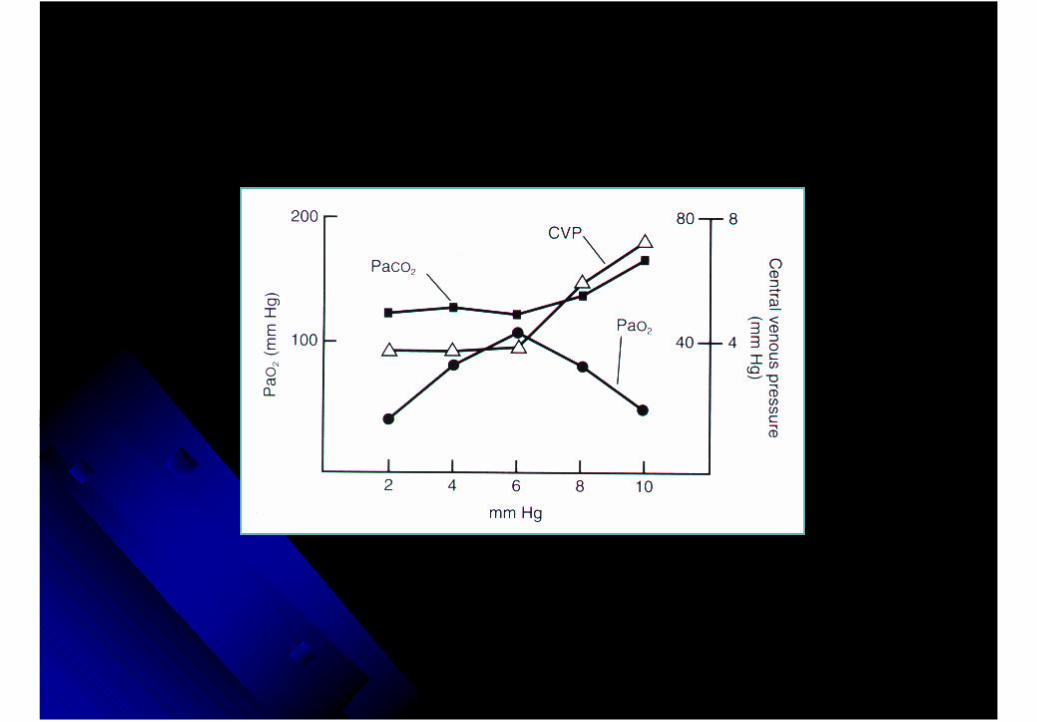
Cardiovascular effects
ll compromise venous return results in diminished cardiac compromise venous return results in diminished cardiac
outputoutput
ll depend on lung compliancedepend on lung compliance
ll sign and symptom: tachycardia, metabolic acidosis, sign and symptom: tachycardia, metabolic acidosis,
hypotension, decreased dynamic compliance, carbon dioxide hypotension, decreased dynamic compliance, carbon dioxide
retentionretention
ll decrease peripheral and regional blood flowdecrease peripheral and regional blood flow
ll decrease oxygen available to tissuedecrease oxygen available to tissue
ll increase extraincrease extra--pulmonary shunting secondary to an pulmonary shunting secondary to an
increase in pulmonary vascular resistanceincrease in pulmonary vascular resistance

Effects of CPAP
l Renal function
l decrease renal blood flow
l decrease urine output and urinary sodium excretion
l increase antidiuretic hormone and aldosterone
l Gastrointestinal function
l decrease gastrointestinal blood flow
l abdominal distention (CPAP belly syndrome)
l Intracranial pressure (head box CPAP) l increase intracranial pressure
l intracranial bleeding

Pressure volume curve
is divided into 3 regionsl region A: low lung
volume, low compliance and high resistance. The P/V slope is low
l region B: optimal lung volume and increases lung compliance
l region C: high lung volume, low lung compliance
0 5 10 15 20
Airway Generation
10,000
1000
100
10
2
Airw
ay Cross-S
ection in cm2
.08
.06
.04
.02
TurbulentHigh-VelocityFlow Region
LaminarLow-VelocityFlow Region
Res
ista
nce
(cm
H2O
/L p
er s
) NormalNewborn
Lung
HMD Lung
Pressure (cmH2O)V
olum
e (m
l)
Pressure- volume curve

Type of
CPAP

Clinical applications of CDP or CPAP
l respiratory distress syndrome
l meconium aspiration syndrome
l apnea of prematurity
l postoperative thoracotomy
l patent ductus arteriosus
l postoperative celosomia
l weaning patients from primary lung disease
l differentiation of primary lung disease from primary cardiac disease
l as adjunct to intermittent positive ventilation
l sleep apnea
l bronchomalacia
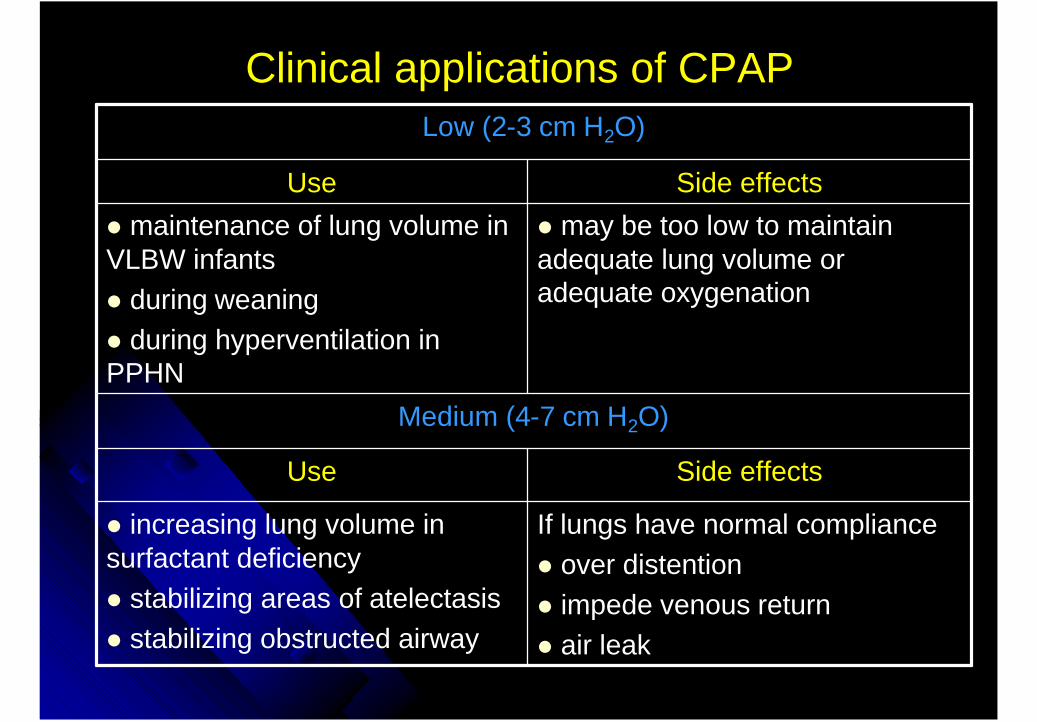
Clinical applications of CPAP
Side effectsUse
If lungs have normal compliancel over distentionl impede venous returnl air leak
l increasing lung volume in surfactant deficiencyl stabilizing areas of atelectasisl stabilizing obstructed airway
Medium (4-7 cm H2O)
l may be too low to maintain adequate lung volume or adequate oxygenation
l maintenance of lung volume in VLBW infantsl during weaningl during hyperventilation in PPHN
Side effectsUse
Low (2-3 cm H2O)
Side effectsUse
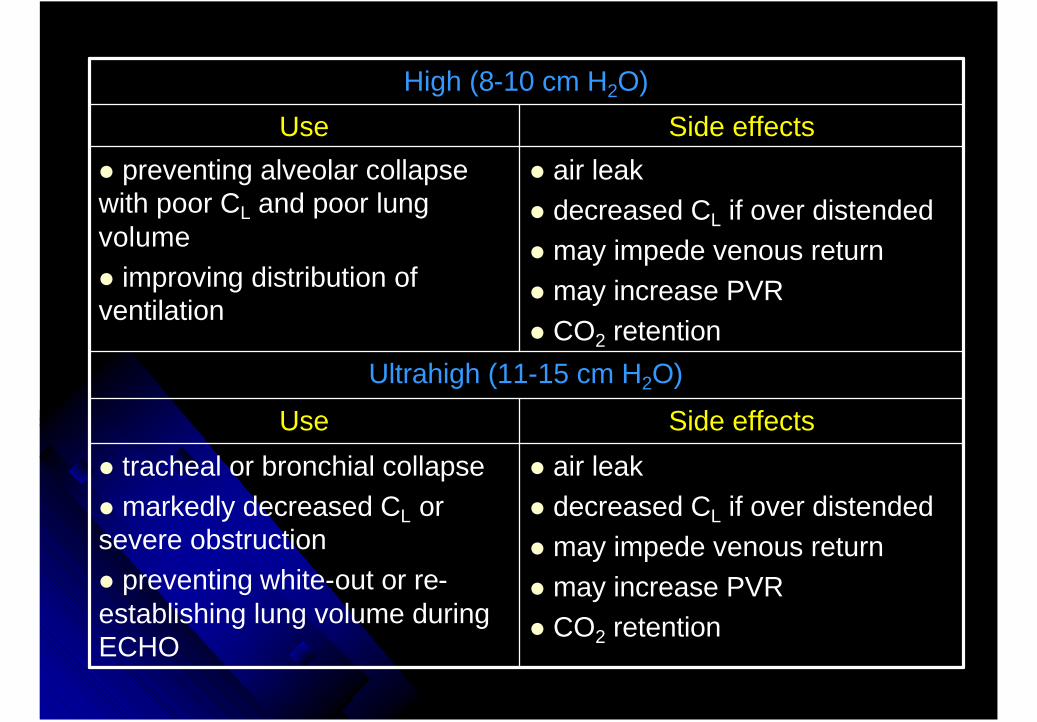
l air leakl decreased CL if over distendedl may impede venous returnl may increase PVRl CO2 retention
l tracheal or bronchial collapsel markedly decreased CL or severe obstructionl preventing white-out or re-establishing lung volume during ECHO
Ultrahigh (11-15 cm H2O)
l air leakl decreased CL if over distendedl may impede venous returnl may increase PVRl CO2 retention
l preventing alveolar collapse with poor CL and poor lung volumel improving distribution of ventilation
Side effectsUse
High (8-10 cm H2O)

Tracheomalacia

Optimal CPAP level
l balance between cardiac output and pulmonary blood flow
l congestive heart failure and pulmonary edema
4-day-old RDS and PDA
l pulmonary mechanics: resistance, compliance
l decreased compliancel increased resistance
BPD on 60% oxygen
l lung compliancel small A-a gradientl weak respiratory musclesl increased chest wall compliance
Small premature infant weaning off CPAP
l PaO2
l oxygen consumptionl oxygen delivery
l significant A-a gradientl rapid change compliance
Acute RDS
Optimal CPAP levelPhysiologyDisease

Clinical use of CPAP
l clinical indicationsl sign of atelectasis on
chest filml chest wall retractionl require FiO2>0.5l display rapidly
progressive lung disease
l initial pressure settingl nasal or nasopharyngeal:
6 cm H2Ol endotracheal: 4 cm H2O
l follow up and weaningl follow-up PaO2 within
15-20 min.l weaningl after oxygenation
was improvedl extubation from
CPAP 3-4 cm H2O

Nursing care of CPAP
l methodlnasallnasopharyngeallendotracheal tubel face mask
l componentsloxygenl temperature and humidity
lpressure
l nursing carelcontinuous care (oxygen, pressure)lcare of airway
l prevent obstructionl prevent irritation of nares
l skin carel abdominal distentionlNPO
Indication of CPAP
Atelectatic disordersl PaO2 below 50-60 mm Hg in FiO2>0.6
l recurrent apnea
Initial setupl CPAP 6 cm H2O
l increase 2-cm. increments q 15 min. to a max. of 10 cm H2O or 12 cm H2O
l increase FiO2 0.05-0.10 if PaO2<50 mm H2O

Respiratory distress syndrome
l improve survival rate, especially larger infants
l modify course of the disease l lower max.FiO2 required,
reduce total amount of time under O2 and the need for mechanical ventilation

Early CPAP in RDS
ll was proved to be more beneficial in the was proved to be more beneficial in the atelectaticatelectatic disease disease
ll lower peak pressure required in infants treated lower peak pressure required in infants treated with CPAPwith CPAP
ll enhance surfactant conservationenhance surfactant conservationll reduce the need for IMV by 20%, except infants reduce the need for IMV by 20%, except infants
with birth weight <1500 g.with birth weight <1500 g.ll improve mortality and decrease the incidence improve mortality and decrease the incidence
of BPDof BPDll prevent need for prolong intubation which prevent need for prolong intubation which
reduce the incidence of acquired subglottic reduce the incidence of acquired subglottic stenosis stenosis

Failure of CPAP therapy in RDS
l very low birth weight infantl late application of CPAPl severity of RDSl associated disease e.g. sepsis,
hypotensionl infants with severe degree of extra-
pulmonary shunt (Fox and coworkers, 1977)

CPAP in apnea of prematurity
l the application of low-level CPAP decrease the incidence of apnea of prematurity (compared to other forms of stimulation)l improve oxygenationl stimulation or inhibition of pulmonary reflexesl alveolar stabilizationl mechanical splinting of airway; reduce
supraglottic resistance in both inspiration and expiration
l some investigators recommended the early use of CPAP as a preventive measure of apnea of prematurity

CPAP in an infant with MAS
l pathology of meconiumaspirationl atelectasisl large airway obstructionl V/Q abnormalities
l application of low-to moderate level CPAPl resolution of atelectasisl stabilization of terminal
airwayl incidence of pneumothorax:
not increasedl precautions in case with PPHN

Adverse effects of CPAP
l pulmonary air leaksl type of CPAP l lung compliance l gestational age
l gastric dilation and rupture l hypotensionl increase pulmonary vascular resistancel chronic lung disease ?

Complication of face mask CPAP





























