Embed Size (px)
Citation preview

D
Prot
lWSW
41
9
ialysis
Cost-Effectiveness of Breast Cancer Screening in Women on Dialysis
Germaine Wong, MBBS, MMed(Clin Epi),1,2
Kirsten Howard, MAppSc(Biopharm), MHthEcon, MPH, PhD,2 Jeremy R. Chapman, MD,3
and Jonathan C. Craig, MD, PhD1,2
Background: Breast cancer screening is recommended for women 50 years and older in mostdeveloped countries. Women on dialysis therapy have a risk of acquiring breast cancer similar to that forother women, but a greater all-cause mortality rate because of mortality from other competing causes. Itis uncertain whether routine screening is cost-effective in women on dialysis therapy. In this study, wedetermine the costs and health outcomes of annual mammographic breast cancer screening in womenon dialysis therapy.
Study Design: We performed a cost-effectiveness analysis. Sensitivity and scenario analyses wereperformed to assess uncertainties in the model’s parameter estimates.
Base Case: A cohort (n � 1,000) of women on dialysis therapy aged 50 to 69 years in Australia.Model, Perspective, and Time Frame: A deterministic Markov model was developed from the
perspective of a health care payer. Patients were followed up over their life time.Intervention: We compared a cohort of women who underwent annual mammography with a cohort
that did not.Outcomes: Life-years saved (LYS), costs, and incremental cost-effectiveness ratio (ICER).Results: Average costs for a program of annual screening for a woman on dialysis therapy were
$4,805 over 30 years. Incremental costs of screening were $403, and benefits were 0.0037 LYS. Fivebreast cancer deaths occurred in the screened arm and 6 breast cancer deaths occurred in theunscreened arm, a difference of 1 breast cancer averted by screening, with an estimated ICER of$109,852/LYS. The absolute reduction in breast cancer mortality was 0.1%, with a net gain in lifeexpectancy of 1.3 days. The ICER was strongly dependent on age, with the most favorable ICERapproximately $100,000/LYS at age 45 years.
Limitations: Costs and clinical data were obtained from the nonindigenous Australian population andmay not be generalizable to African Americans on dialysis therapy and indigenous populations fromother countries.
Conclusion: Using the most optimistic assumptions, survival gains expected from screening forbreast cancer in women on dialysis therapy are very small. Annual population breast cancer screeningshould not be recommended for all women on dialysis therapy, but should be an individual decisionbetween the patient and health care provider.Am J Kidney Dis 52:916-929. © 2008 by the National Kidney Foundation, Inc.
INDEX WORDS: Breast neoplasm; mass screening; cost-effectiveness.
sfslawcit
Editorial, p. 830
opulation-based breast cancer screening withannual or biennial mammography is the
ecommended practice for women 50 years andlder in most developed countries. Breast cancer,he most frequently occurring cancer and the
From the 1NHMRC Centre for Clinical Research Excel-ence in Renal Medicine, Children’s Hospital at Westmead,estmead; 2School of Public Health, University of Sydney,ydney; and 3Centre for Transplant and Renal Research,estmead Hospital, Westmead, NSW, Australia.Received March 17, 2008. Accepted in revised form June
, 2008. Originally published online as doi:
0.1053/j.ajkd.2008.06.015 on September 16, 2008.American Journal of Kidn16
econd leading cause of cancer deaths in women,ulfils accepted criteria for an evidence-basedcreening program. A meta-analysis based on 8arge well-conducted randomized controlled tri-ls has shown that mammographic screening foromen aged 50 to 74 years decreases breast
ancer mortality rates by 23% (95% confidencenterval, 13 to 31).1 These trials have also shownhat this benefit is mediated by the detection of
Address correspondence to Germaine Wong, MBBS,Med(Clin Epi), Centre for Transplant and Renal Research,estmead Hospital, Westmead, NSW 2145, Australia.-mail: [email protected]© 2008 by the National Kidney Foundation, Inc.0272-6386/08/5205-0013$34.00/0
MWE
doi:10.1053/j.ajkd.2008.06.015
ey Diseases, Vol 52, No 5 (November), 2008: pp 916-929

l(tsdw9bpmmblU
wciwtirggpepttetpmvgeoup
speiiabmils
dapoThst
toetpcdaheitietm
S
Tm1wucrtiIaatbcsdrdPbTmmo
Breast Cancer Screening and ESKD 917
ess advanced malignancy by using screeningstage shift) compared with routine clinical detec-ion, which confers a more favorable progno-is.2-4 Mammography is sensitive and specific inetecting preclinical early-stage breast cancersith sensitivity and specificity ranges of 65% to1% and 80% to 95%, respectively.5 Population-ased breast cancer screening in the generalopulation is also cost-effective compared withost other screening programs, with the incre-ental cost-effectiveness ratio (ICER) from trial-
ased economic analyses varying from $28,000/ife-year saved (LYS) to $40,000/LYS in thenited States, Australia, and across Europe.6-9
Breast cancer is the most common cancer inomen on dialysis therapy, but unlike most other
ancers, the risk of breast cancer is not increasedn women on dialysis therapy compared withomen in the general population.10 Although
here are no specific guidelines for cancer screen-ng in women on dialysis therapy, the compa-able risk has prompted some to extrapolateuidelines for breast cancer screening for theeneral population to the dialysis and transplantopulations.11,12 Others have also suggested strat-gies to increase cancer screening in the dialysisopulation, which is much less common than inhe general population.13 Considerable uncer-ainty exists about whether standard methods forarly detection of cancers in the general popula-ion offer similar survival benefits in the dialysisopulation, in which the age-specific all-causeortality rate (predominantly driven by cardio-
ascular disease) is much greater than in theeneral population. No randomized trials of theffects of mammographic screening in womenn dialysis therapy have been conducted and arenlikely in the future because of feasibility andower issues.Decision analytical models for breast cancer
creening in the general population cannot sim-ly be extrapolated to the end-stage kidney dis-ase population because of potential differencesn the natural history of disease, tumor character-stics, screening test performance, treatment costs,nd quality-of-life issues and the relative contri-ution of cancer and other causes to overallortality rates. Previously published studies us-
ng the declining exponential approximation ofife expectancy methods have failed to show
urvival benefits with cancer screening in the tialysis population.14,15 However, these studiesssumed a simplistic constant linear survivalrobability and did not comprehensively assessther uncertainties by using sensitivity analyses.he aim of this study is to estimate the costs andealth outcomes of annual mammographiccreening for breast cancer in women on dialysisherapy by using decision analytical modeling.
METHODS
A deterministic Markov model was developed to simulatehe natural history of breast cancer in a hypothetical cohortf women on dialysis therapy over time. A Markov modelvaluates the disease of interest by modeling its progressionhrough mutually exclusive health states during a definederiod.16 We first structured the model to include all possibleonsequences of the preclinical and clinical stages of theisease processes. We then incorporated all costs, benefits,nd harms of breast cancer screening across the differentealth states. Using cohort simulation, which modeled theffects of the “average” patient, rather than relying onndividual patient data, allowed us to calculate the incremen-al costs and benefits of screening compared with no screen-ng. To determine the robustness of the model, we tested thextent to which this model’s assumptions were sensitive tohe uncertainties within the parameters by using 1-way andultiway sensitivity analyses.
tructure of theModel
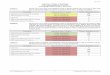
The simplified structure of the model is shown in Fig 1.his model compared annual breast cancer screening usingammography with no screening in a cohort of women (n �
,000) on dialysis therapy with a starting age of 50 years. Allomen stopped screening at age 70 years and were followedp until they all died (assuming a period of 30 years). Eachycle represented a 1-year period. Mammography screeningates in the dialysis population varied from 12% to 69%.17 Inhe general population, participation rates varied from 40%n observational studies to 70% in trial-based analysis.2,18,19
n our base-case analysis, we took an average of these resultsnd assumed a 50% participation rate in the screening cohortnd no participation in the nonscreening cohort, but testedhe uncertainty in sensitivity analyses.2 Invasive and in situreast cancers were diagnosed by using mammography orlinical diagnosis in the screened population. In the un-creened population, all cancers could be detected andiagnosed only clinically. All women with positive screenesults were investigated by using such diagnostic proce-ures as radiological confirmation and surgical biopsies.otential downsides of false-positive screen results haveeen well-documented in mammography screening trials.20
o examine the implications of false-positive results ofammography, we included all costs of false-positive mam-ogram results (eg, such additional intervention as radiol-
gy and biopsy). We assumed that no women underwent
ransplantation in this analysis.
T
bsicaogpatb
siaidttsitawsdu
tmcoc
ac
nssemecaa
I
cbmmTigodudd
ctD2d
Wong et al918
reatmentAlgorithm
There is now convincing trial evidence to show a clearenefit of combination radiation therapy and surgery overurgery alone for women with a diagnosis of ductal carcinoman situ, with a decrease in 12-year rates of ipsilateral breastancer recurrence of 32% to 16%.21,22 In this model, wessumed that all women on dialysis therapy given a diagnosisf in situ cancer received combination breast-conserving sur-ery and radiation therapy to decrease the probability of cancerrogression and incidence of cancer recurrences. In situ cancerslone are benign conditions and not life threatening. However,hey could progress to invasive cancers and cause significantreast cancer mortality and morbidity.
Women with invasive cancers in the screened and un-creened populations were managed according to stages atnitial diagnoses. Women with early breast cancers, defineds tumors no greater than 5 cm in diameter with eithermpalpable or palpable lymph nodes and no evidence ofistant metastasis received surgical intervention in combina-ion with radiotherapy as first-line treatment. Depending onhe degree of nodal extension, hormonal receptor, and HER-2tatus, these women also received systemic adjuvant therapyn the form of combination anthracycline-based chemo-herapy and/or such antiestrogen hormonal or monoclonalntibody therapy as trastuzumab postoperatively. Womenith early breast cancer could respond to treatment and
urvive the cycle with cure; respond, but experience relapse;ie of breast cancer; or die of other causes related and/ornrelated to their end-stage kidney disease.Women with advanced-stage breast cancers, defined as
hose with locally advanced disease or evidence of systemicetastasis, were incurable and required a multidisciplinary
are team. The team included a medical and radiationncologist, palliative consultant, surgeon, specialist nurse,
ounselor, and therapists with special needs. Women with advanced-stage disease could not be cured, but died of breastancer or other causes in the current and subsequent cycles.
Women with no breast cancer on dialysis therapy who didot die of other causes cycled back to the beginning of thecreening/no screening decision node and were eligible forcreening in the following year. Women who survived witharly-stage cancers entered a surveillance state for intensiveonitoring for cancer recurrence or new diagnoses. At the
nd of each cycle, the model accrued the effectiveness andosts for women in each health state. Cumulative benefitsnd costs were calculated to 30 cycles (year), when almostll women in the entire cohort had died (99.5%).
nput Parameters of theModel
ClinicalData
Table 1 lists all parameter estimates included in the model. Aomprehensive literature search was performed to identify theest available evidence as input transition probabilities esti-ates for the model (search details provided as online supple-entary material available with this article at www.ajkd.org).hese were time-dependent probabilities of an event occurring
n the model from published literature in the dialysis andeneral populations. These variables included test performancef mammography (at initial and subsequent screens), stageistribution, and stage-specific survival in the screened andnscreened populations; probability of cure; probability ofisease relapse posttreatment; and probability of new cancerevelopment.
Age-specific prevalence of disease and age-specific breastancer and all-cause mortality data for women on dialysisherapy were obtained from the Australian and New Zealandialysis and Transplant (ANZDATA) Registry in 1995 to006. The age-specific non–breast cancer competing risk ofeath rate for women on dialysis therapy was defined as the
Figure 1. Simplified struc-ture of the model. Light greyovals, data from the ANZDATARegistry; white ovals, data ex-trapolated from the generalpopulation. Rx, treatment.
ge-specific all-cause mortality for women on dialysis therapy

A
S
S
A
S
S
A
A
A
A
A
Breast Cancer Screening and ESKD 919
Table 1. Base-Case Values Used as Clinical Inputs Into the Model
nnual age-specific prevalence of breast cancers (reference 47 [dialysis population])35-44 y 0.001945-54 y 0.002455-64 y 0.004365-74 y 0.0031�75 y 0.0054
ensitivity of mammography (reference 19 [dialysis population])Prevalent screen 0.88 (0.50-1)Incident screen 0.84 (0.45-1)
pecificity of mammography, by age (reference 48 [general population])30-39 y 0.90 (0.50-1)40-49 y 0.93 (0.50-1)50-59 y 0.93 (0.50-1)60-69 y 0.93 (0.50-1)�70 y 0.99 (0.50-1)
nnual probability of progression from in situ breast cancers to invasive cancers (references 49-52 [general population])0.025-0.06
tage distribution of cancers in the unscreened population (references 53-55 [general population])1 0.382 0.423 0.134 0.07
tage distribution of cancers in the screened population (references 53-55 [general population])1 0.49 (0.35-0.52)2 0.38 (0.35-0.45)3 0.09 (0.03-0.15)4 0.05 (0.02-0.10)
nnual age-specific probability of invasive and in situ breast cancers at prevalent screen (reference 19 [general population])Invasive In Situ
30-39 y 0.753 0.24740-49 y 0.789 0.21150-59 y 0.867 0.16360-69 y 0.8 0.2
nnual age-specific probability of invasive and in situ breast cancers at incident screen (reference 19 [general population])Invasive In Situ
30-39 y 0.741 0.25940-49 y 0.667 0.33350-59 y 0.837 0.16360-69 y 0.813 0.187
nnual age-specific all-cause mortality in the dialysis population (reference 42 [dialysis population])All Women Diabetics
30-39 y 0.050 0.07540-49 y 0.080 0.11350-59 y 0.110 0.15060-69 y 0.150 0.19070-79 y 0.210 0.292�80 y 0.250 0.30
nnual age-specific breast cancer-specific mortality in the dialysis populationAll Women*
30-39 y 0.00340-49 y 0.00850-59 y 0.01160-69 y 0.01170-79 y 0.012
nnual age-specific mortality from causes other than breast cancers†All Women Diabetics
30-39 y 0.047 0.07240-49 y 0.072 0.105
(Continued)

A
P
P
A
E
A
A
A
P
D
m
Wong et al920
Table 1 (Cont’d). Base-Case Values Used as Clinical Inputs Into the Model
nnual age-specific mortality from causes other than breast cancers†All Women Diabetics
50-59 y 0.099 0.13960-69 y 0.139 0.17970-79 y 0.239 0.288
robability of annual breast cancer recurrence by stage (reference 56 [general population])1 0.0132 0.0173 0.020
robability of survival postrecurrence of disease by stage (reference 57 [general population])1 0.8702 0.3753 0.350
ge-specific probability of clinical diagnosis (reference 58 [general population])30-39 y 0.42940-49 y 0.41350-59 y 0.42460-69 y 0.417
strogen receptor positivity (reference 59 [general population])50-64 72% (75%-80%)65-79 82% (78%-86%)
ge-specific distribution of surgical treatment for stage 1 and 2 disease (reference 60 [general population])BCS (%) BCS � RT (%) MST (%)
50-54 y 12.1 54.1 33.855-59 y 10.9 51.1 38.060-64 y 10.2 47.8 42.165-69 y 10.5 43.6 45.970-74 y 12.0 41.2 46.875-79 y 17.1 34.3 48.680-84 y 26.4 24.8 48.8�85y 45.5 11.6 42.8
ge-specific distribution of surgical treatment for stage 3 disease (reference 60 [general population])BCS (%) BCS � RT (%) MST (%)
50-54 y 11.4 29.5 59.155-59 y 9.3 27.5 63.260-64 y 9.4 26.7 63.965-69 y 7.1 22.3 70.670-74 y 6.1 21.0 72.975-79 y 6.2 18.2 75.680-84 y 8.7 12.4 79.0�85 y 17.7 5.5 76.8
ge-specific distribution of surgical treatment for stage 4 disease (reference 60 [general population])BCS (%) BCS � RT (%) MST (%)
50-54 y 17.4 12.2 70.455-59 y 16.7 13.6 69.760-64 y 22.0 15.0 63.065-69 y 26.5 12.3 61.370-74 y 21.7 13.0 65.475-79 y 25.3 9.8 64.980-84 y 37.0 11.6 51.4�85 y 29.2 11.3 59.4
articipation rate (references 2 and 54 [general population])0.50 (0.40-1.0)
iscount rate0.05 (0.03-0.08)
Note: Values in parentheses indicate 95% confidence interval or plausible range used in sensitivity analyses.Abbreviations: BCS, breast-conserving surgery; MST, modified radical mastectomy; RT, radiotherapy.*Including women with diabetes.†Annual age-specific all-cause mortality in the dialysis population, less annual age-specific breast cancer-specific
ortality in the dialysis population.
mwpisfp
UoMSstbucuwcia
pDdcc
S
wttyOotwytSpsppscdtau
p
dcowstcbmttsdoctbcbt
beIc
Fcut
B
scstciweigcDfpcr
Breast Cancer Screening and ESKD 921
inus the age-specific breast cancer–specific mortality foromen on dialysis therapy. Previous screening trials andrograms in the general population had shown an increase inncidence of cancers detected at initial screen compared withubsequent screens. A multiplier using data extrapolatedrom Breast Screen Australia was included to simulate thisattern of early cancer detection by screening.23
CostData
Table 2 lists all direct health costs included in the analysis.nit costs for breast cancer screening and treatment werebtained from theAustralian Refined Diagnosis Related Groups,edicare Benefits Schedule, and Cancer Institute of New
outh Wales. The analysis assumes that all women in both thecreened and unscreened cohorts continue dialysis therapy;hus, the costs of dialysis therapy have not been includedecause they are the same in both cohorts. If data werenavailable in Australian dollars, all costs in foreignurrencies were converted to 2004 Australian dollars bysing the Purchasing Power Parities, and Australian costsere adjusted to 2004 dollars by using the Medicare
omponent of the Consumer Price Index.24,25 The variabil-ty in the costs schedule was also tested in sensitivitynalyses.
SubgroupAnalysis
A subgroup analysis was also performed in the diabeticopulation by using age-specific mortality data from the ANZ-ATA Registry (1995 to 2006). Women with diabetes onialysis therapy had a greater excess burden of comorbidonditions and significantly decreased overall life expectancyompared with the nondiabetic dialysis population.
ensitivityAnalysis
A series of 1-way sensitivity analyses on the key parametersas conducted to assess the robustness of the uncertainties in
he model’s assumptions. Previous studies have confirmed thathe overall cancer risk in transplant recipients is greater inounger women (�35 years) than in the older population.26
ne-way sensitivity analysis was performed to assess the effectf age on the overall cost-effectiveness of screening. We variedhe starting age for screening from 30 to 60 years. All womenere followed up until they died (assuming follow-up of 50ears for women aged 30 to 39 years, 40 years for those aged 40o 49 years, and 30 years for those aged 50 to 69 years).pecifically, we also assessed the effects of varying the relativerevalence of cancers, age-specific screening test accuracies,tage distribution of cancers in the screened and unscreenedopulations, probability of clinical diagnosis in the unscreenedopulations, participation rate of screening, stage- and age-pecific survival after treatment, relative risk reduction in breastancer–specific mortality in the screened population, futureiscount rates on benefits/costs, and the all-costs parameters inhe model. Two-way sensitivity analyses were conducted tossess interactions between the most influential variables foundsing 1-way sensitivity analyses.
ScenarioAnalysis
There is little information about the progression and
rognosis of undiagnosed breast cancers in the general and oialysis populations. Extreme case scenario analyses, a pro-ess that considers and analyzes alternative events andutcomes in uncertain circumstances, were conducted foromen with undiagnosed disease in the unscreened and
creened populations. In the base-case analysis, we assumedhat the cumulative probability of all undiagnosed breastancers being diagnosed clinically increased over time,ased on varying incremental probabilities. We assigned aultiplier to the overall age-specific breast cancer mortality
hat was dependent on the stage and cycle of diagnosis, withhe assumption that clinically diagnosed breast cancers inubsequent cycles had a much poorer prognosis than cancersiagnosed clinically in preceding cycles. Under the mostptimistic assumption, all women with undiagnosed breastancers (both screened and unscreened arms) cycled back tohe population and attained a constant probability of havingreast cancer diagnosed in subsequent cycles. In the worst-ase scenario, we assumed that all women with undiagnosedreast cancers (both screened and unscreened arms) died inhe next cycle.
ModelOutcomes
Model outcomes included average costs and benefits ofreast cancer screening and no screening measured in LYS, anstimate of the number of breast cancer deaths averted and theCER of screening compared with no screening. ICERs werealculated according to the following formula:
ICER �CostNew � CostComparator
Ef fectivenessNew � Ef fectivenessComparator
uture costs and benefits were discounted by using a dis-ount rate of 5%/annum, and half-cycle corrections weresed. TreeAge Pro Suite 2007 (TreeAge software, Williams-own, MA) was used to develop the model.
RESULTS
ase-CaseAnalysis
Assuming a participation rate of 50% and atarting age of 50 years for all women in the entireohort (without and with diabetes), the total cost ofcreening per woman was $4,805 compared withhe cost of no screening of $4,402, giving an extraost for screening of $403. Total benefits of screen-ng per woman were 5.9769 life-years comparedith 5.9732 life-years for no screening, a differ-
nce of 0.0037LYS, or 1.3 days of lives saved. Thencremental cost-effectiveness of annual mammo-raphic screening in women on dialysis therapyompared with no screening was $109,852/LYS.uring 30 years, there were 5 deaths/1,000 women
rom breast cancer in the screened population com-ared with 6 deaths/1,000 women from breast can-er in the unscreened population, with a relativeisk reduction of 17% and absolute risk reduction
f 0.1%. Total incremental costs to screen and save
1s$
W
i
is4ohm
I
P
I
T
C
O
CCC
hemoth
Wong et al922
extra cancer death approximated A$403,000/lifeaved from breast cancer and corresponded to US276,027/life saved.
omenWithDiabetes
For women with diabetes, total costs of screen-
Table 2
maging testsMammographyUltrasound Computed tomography
Chest and abdomenBrachial plexus
Bone scanathological testsGeneral blood testHER-2 statusHormone receptor status
nterventionsFine needle biopsiesOpen core biopsiesTotal mastectomyPartial mastectomyBreast reconstructionChemotherapy (doxorubucin � docetaxel � cyclophospHormonal therapy (tamoxifen)TrastuzumabRadiotherapy
otal costs for treatment according to cancer stage*Stage 1Stage 2Stage 3Stage 4osts for diagnosing and treating relapsesSpecialist visitsBiopsiesImagingAdditional surgeryChemotherapyHormonal therapyRadiotherapythersPhysician visitsElectrocardiogramosts of dying of breast cancersosts of dying of other causesosts of false-positive screen resultPhysician visitsPsychological complications (includes physician visits an
psychotherapy)Surgical biopsies
*Inclusive of such systemic therapies as tamoxifen and c
ng per woman were $4,887 compared with $4,516 $
n the unscreened arm, with the incremental cost ofcreening of $371. Total benefits of screening were.4896 life-years compared with 4.4892 life-yearsf no screening, a difference of 0.0004 LYS, or 3.5ours of lives saved. The overall ICER of annualammography in women with diabetes was
t Data
Average Costs/Input (ranges used insensitivity analysis in A$) References
90 for both breasts (50-500) 25109 for both breasts (80-800) 25
25400492
600 (500-2,000) 25
250 2551.6 —81.5 —
344 (200-500) 25500 (400-1,000) 25
5,812 24, 253,069 24, 25
13,669 24, 25) 16,230 24, 25, 61
40/mo 24, 25, 613,600/cycle 24, 25, 61
250/dose —
33,555 (20,000-60,000) 24, 25, 6155,793 (25,000-80,000) 24, 25, 6171,287 (30,000-100,000) 24, 25, 6166,606 (40,000-100,000) 24, 25, 61
127 25214 25
1,100 253,609 24
66,606 24, 25, 61480 61
3,200 —
127 25150 25
6,140 62, 635,000 62, 63
150/visits 25700 —
500 25
erapy, surgery, radiotherapy, and hospital stay.
. Cos
hamide
d
965,781/LYS.

S
tcFca4o$
O
tistpmfiosavmU$w$cavs
fittsrvIL1tbtelt0mI
T
eibtom$ipgce
ecsait
Breast Cancer Screening and ESKD 923
tartingAge
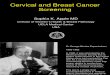
One-way sensitivity analysis was performedo assess the effect of starting age on the overallost-effectiveness of the screening program. Inig 2, the curve represents ICERs for screeningompared with no screening at different startingges. The optimal starting age for screening was5 years. If screening started at ages younger orlder than this, the ICER substantially exceeded50,000/LYS, indicated by the horizontal line.
ne-WaySensitivityAnalyses
The model was most sensitive to changes inhe following variables: screening test specific-ty, participation rate of screening, prognosis andurvival posttreatment in the screened popula-ion, stage distribution of disease in the screenedopulation, prevalence of disease, costs of mam-ography, and costs of diagnosis and treatment
alse-positive results. Figure 3 shows the variabil-ty in ICERs, with the influential variables testedver a range of values in 1-way sensitivity analy-es. The black vertical line represents the ICERt the base case, $109,852/LYS. The dashed greyertical line represents an arbitrary, but com-only cited, cost-effectiveness threshold in thenited States and Australia for intervention of50,000/LYS.27-29 We also compared our resultsith a “higher” willingness to pay threshold at100,000/LYS, indicated by the solid grey verti-al line, which previously was found to be ancceptable cost-effectiveness threshold for inter-ention in the dialysis population.30 Previous
Figure 2. Incremental cost-ffectiveness ratios (ICERs)omparing screening and nocreening at different startingges for breast cancer screen-
ng in women on dialysisherapy.
tudy reported an increased risk of benign calci- w
cation of the breasts in women on dialysisherapy, which may or may not affect the overallest accuracy of screening mammography.31 Asuch, we varied the test specificity of mammog-aphy between the plausible extremes. If wearied the test specificity from 0.50 to 0.99, theCER decreased from $431,068/LYS to $77,333/YS. By improving participation from 40% to00%, the ICER decreased from $189,950/LYSo $99,598/LYS. Despite varying between theest and worst parameter estimates for all inputs,he ICER remained consistently high. The onlyxception was prevalence of disease. If the preva-ence of breast cancer was 3 times greater thanhe age-specific base-case estimates of 0.002 to.004 between ages 50 and 69 years, screeningay offer reasonable value for money with an
CER of $34,444/LYS.
wo-WaySensitivityAnalysis
Two-way sensitivity analyses enabled us toxamine the combined effects of uncertainty in 2nput parameters. Figure 4 shows interactionsetween disease prevalence and 4 other influen-ial variables: test specificity, stage distributionf disease, participation rate, and costs of mam-ography, assuming a willingness to pay ratio of
50,000/LYS. This analysis confirmed the find-ngs of the 1-way sensitivity analysis that cancerrevalence was the single determining factor thatoverned the overall cost-effectiveness of breastancer screening in the dialysis population. Forxample, even if the presumed participation rate
as 100%, it was only cost effective to imple-
mwdaf
S
suuc$T$5L
susgccta$wsg
sfubgdwwoaoloaLt
iwfiirtsd
tiep5 52%, 3
Wong et al924
ent population breast cancer screening foromen on dialysis therapy if the underlyingisease prevalence was at least 1.15 times thege-specific base-case estimates of 0.002 to 0.004rom ages 50 to 69 years.
cenarioAnalyses
Under the most favorable conditions for thecreened population (in which all women withndiagnosed breast cancers in the screened andnscreened population died in the subsequentycle), total costs of screening per woman were4,596, and total benefits were 5.9606 life-years.otal costs of no screening per woman were4,050, and total benefits of no screening were.9452 life-years, giving an ICER of $35,347/YS.Under the least favorable conditions for the
creened population (in which all women withndiagnosed disease in the screened and un-creened populations survived the cycle, pro-ressed back to the population, and acquired aonstant probability of being diagnosed clini-ally and a constant cancer-specific mortality),otal costs of screening per woman were $6,161,nd total costs of no screening per woman were5,452. Total benefits of screening per womanere 5.9991 life-years, and total benefits of no
creening per woman were 5.9962 life-years,
Figure 3. One-way sensitivity analyses of influentialhreshold at $50,000/life-year saved (LYS); solid grey linencremental cost-effectiveness ratio (ICER) at base case oach variable: costs of mammography, values vary frorevalence, from 3.0, 0.5 times of the age-specific base-ca8%; distribution of stage 1 disease in screened arm, from
iving an overall ICER of $237,800/LYS. a
DISCUSSION
Using the best available data, our analysisuggests that routine mammographic screeningor breast cancer in women on dialysis therapy isnlikely to be cost-effective. This is driven largelyy very small survival gains because of muchreater competing risks from other causes ofeath in women on dialysis therapy comparedith the general population. In a cohort of 1,000omen during a screening period of 30 years,nly 1 extra death from breast cancer would bevoided. Given the greater risk of death fromther primarily cardiovascular causes, this wouldead to an expected gain in life expectancy ofnly approximately 1 day. The overall ICER ofnnual mammographic screening is $109,852/YS compared with $20,000 to $40,000/LYS ofhe same program in the general population.
In this setting, in which there are no random-zed trials of the intervention of interest (andith no trials in prospect) and the effects there-
ore are very uncertain, decision analytic model-ng is particularly useful to evaluate whether thentervention may be effective within plausibleanges for input variables and identify priorityopics for future research. For breast cancercreening using mammography in women onialysis therapy, apart from disease prevalence,
les in the model. Dashed grey line, willingness to payness to pay threshold at $100,000/LYS; solid black line,
852/LYS. Range of values used in sensitivity analyses forto $500; specificity, from 99%, 50%; relative disease
mates (0.002 to 0.004); survival posttreatment, from 79%,0%; participation rate, from 100%, 40%. RX, treatment.
variab, willingf $109,m $50se esti
ll other factors that influence the overall cost-

edtcbesocairFimaps
lctbcadtaiaManmt
ukwRbasursuoria
tin the model.
Breast Cancer Screening and ESKD 925
ffectiveness, such as benefits of early canceretection, treatment effectiveness, prognosis, andest accuracies, are undefined. Benefits of earlyancer detection through screening are achievedy a shift to less advanced stage diseases, withffective treatment to improve overall cancer-pecific mortality. Cancer screening tools withptimal sensitivities and specificities ensure trueancer diagnoses and minimize false-positivend false-negative results. Unnecessary invasiventerventions with false-positive results couldesult in both physical and psychological harms.alse-negative findings with false assurances may
ncrease the chance of delayed diagnoses andisdiagnoses. There are reasons to believe that
ll these attributes are different from the generalopulation and lead to less favorable effects ofcreening in the dialysis population.
The benefits of cancer screening are estab-ished in the general population through well-onducted adequately powered randomized con-rolled trials.2-4,32 In the dialysis population, anyenefits achieved through screening may be eradi-ated by the excess mortality and morbiditiesssociated with end-stage kidney disease. In ad-ition, with the advent of newer breast chemo-herapeutic agents and such hormonal therapiess aromatase inhibitors and monoclonal antibod-es, there is limited information about the benefitsnd harms specific to the dialysis population.any of these agents, such as platinum-based
nd anthracycline-containing regimens, are bothephrotoxic and cardiotoxic,33,34 which may beore detrimental to women on dialysis therapy
han to those with normal renal function.Uniformly, there is a lack of informative and
nbiased prognostic cancer data in the end-stageidney disease and renal transplant populationsorldwide. Nonetheless, data from the ANZDATAegistry suggested a trend of decreased overallreast cancer survival in renal transplant recipientsnd patients with end-stage kidney disease on dialy-is therapy than in the general population. Overallnadjusted 5-year breast cancer survival rates inenal transplant recipients and women on dialy-is therapy are 58% and 28%, which comparesnfavorably with the general population with anverall 5-year survival rate greater than 80%,espectively.35 In a state of chronic uremia, whichtself may be carcinogenic, responses to surgical
Figure 4. Two-way sensitivity analyses varying be-ween relative disease prevalence and influential variables
nd adjuvant therapies for earlier stage diseases

iparg
hmcnprtsiwmtctltpopmtca
caiDhdcvOhltwrcmedl
t
dpbagfgtiabdscf
chgbcabtiStFpeeytTfwbc
wpptiaits$s
Wong et al926
s unlikely to be as effective as in the generalopulation. Women undergoing dialysis may notchieve the cancer-specific mortality benefits withoutine screening compared with women in theeneral population.The breasts of women on dialysis therapy also
ave different morphological appearances onammography, including more calcification be-
ause of secondary hyperparathyroidism in be-ign adenomas, which may affect the overall testerformance by producing more false-positiveesults.31,36 Women undergoing dialysis poten-ially may have more complications from inva-ive surgical interventions because of greaternfection risks and complications from pooround healing.31 Instituting unnecessary treat-ent for cancers detected by using a more sensi-
ive test could cause harm because many of theseancers would remain insignificant and not affecthe individual’s overall survival and quality ofife during the lifetime of a woman on dialysisherapy without active treatment. The long-termsychological and physical impact, overall costsf false-positive mammographic results, and im-act of inconsequential diseases detected byeans of screening are well studied and charac-
erized in the general population.20,37,38 In thehronic kidney disease population, these effectsre largely unknown.
Given the uncertainties inherent in the base-ase analyses, the robustness of our results wasssessed and tested in the 1- and 2-way sensitiv-ty analyses and scenario sensitivity analyses.espite varying between the best and worstypothetical estimates for these variables, withisease prevalence the only exception, breastancer screening does not appear to be a goodalue for the money in women on dialysis therapy.f all participants, patients with diabetes, whoave the shortest life expectancies, attained theeast benefits and incurred the greatest incremen-al costs to save 1 extra death from breast cancerith annual screening. This is expected for 2
easons: cardiovascular disease, rather than can-er, contributes to more than 30% of all-causeortality in patients with diabetes, and the life
xpectancy of an individual with diabetes onialysis therapy is markedly shorter than the timeived to develop breast cancers.39
Annual mammography in women on dialysis
herapy may be cost-effective only if the actual nisease prevalence is much greater than the ex-ected base-case estimates. If the absolute num-ers of the diseased individuals are higher, over-ll costs of screening are shared and offset by thereater number of individuals who may benefitrom screening. If the underlying relative risk isreater for the individual or population, the rela-ive harms of screening are decreased and screen-ng with early disease detection may be desir-ble. Although it may not be favorable andeneficial to screen women of average risk in theialysis population, it may be cost-effective tocreen nondiabetic healthier individuals with in-reased cancer risk, such as those with a strongamily history.
Breast cancer screening in younger women isontroversial because of an uncertain benefit-arm trade-off. In contrast to findings in theeneral population, in which screening may note as effective in women younger than 50 yearsompared with women older than 50,40,41 ournalysis suggests that if we were to implementreast cancer screening in the dialysis popula-ion, it is probably most cost-effective if screen-ng commences at age 45 rather than 50 years.tarting at ages younger or older than this value,
he ICER will be exceedingly high, as shown inig 4. The observed differences between the 2opulations could be attributed to the acceleratedffects of aging with chronic kidney disease. Forxample, the estimated life expectancy of a 50-ear-old woman on dialysis therapy is similar tohat of a 75-year-old in the general population.42
he augmented risk of breast cancer and there-ore potential increased benefits from screeningith older age is mitigated by decreased relativeenefits because of coexisting morbidities andompeting risks of death with age.43
Under the influence of immunosuppression,e cannot confidently assume that breast cancersrogress in the same manner as in the generalopulation. As such, we considered these uncer-ainties by means of scenario analyses by vary-ng between the most pessimistic and optimisticssumptions of disease progression and mortal-ty in patients with undiagnosed disease. Substan-ial variability in the estimated ICERs for annualcreening was observed between an extreme of237,800/LYS if we assumed that all womenurvived the subsequent cycles with undiag-
osed disease to $35,349/LYS assuming that all
wctasdc
oowtqbnyfsdpiWipgfibttotltf
iAfto
bdiurtifu
hawtiattfw
ctemstdgedebtictobcasdi
Seto2t
BsS
e
Breast Cancer Screening and ESKD 927
omen with undiagnosed disease died with breastancers in subsequent cycles. Given the uncertain-ies in the model’s assumptions, primary studiesssessing the natural history and overall progno-is of breast cancers in the end-stage kidneyisease population are needed to resolve andlarify uncertainties in the model estimates.
There are a number of potential limitations inur study. First, we have not valued the survivalutcomes by using quality-adjusted life-years,hich would capture both the quality and quan-
ity of life differences in the model. Utility-baseduality-of-life studies allows us to convert healthenefits uniformly into a single globally recog-ized and accepted value (quality-adjusted life-ears) that reflects each individual’s preferenceor different health states. There is evidence tohow that the quality of life of individuals onialysis therapy is different from the generalopulation, but we are uncertain about the qual-ty of life of dialysis patients with cancers.44,45
ith the accompanying comorbid conditions, its most likely that the quality of life of theseatients will be very different from that of theeneral populations with cancers. There is a needor utility-based quality-of-life primary studiesn the dialysis population using such preference-ased techniques as standard gamble and timerade-off to ensure a more realistic evaluation ofhe true impact on the survival and quality of lifef having breast cancer in the dialysis popula-ion. Inclusion of quality-of-life weights to calcu-ate quality-adjusted life-years will also changehe cost-effectiveness ratio and may lead to a lessavorable ICER.
Second, our study results may not be general-zable and applicable to indigenous Australians,frican Americans, or indigenous populations
rom other countries because information ob-ained for this analysis was predominately basedn the nonindigenous Australian population.Third, given limited information about the
enefits, harms, and costs of screening in theialysis population, we developed a determin-stic model and evaluated the uncertaintiessing the “extremes” of parameter estimates,ather than estimating joint parameter uncer-ainties in a probabilistic sensitivity analysis,n which values of uncertainties are sampledrom statistical or empirical distributions by
sing Monte Carlo simulation. Finally, we fave not considered and identified the benefitsnd harms of breast cancer screening in womenho underwent kidney transplantation. Given
he similar disease prevalence and variabilityn screening test performance, but better over-ll life expectancy and cancer prognosis in theransplant population, the benefits to harmrade-off for routine mammographic screeningor transplant recipients may be different fromomen on dialysis therapy.46
In summary, even under the most favorableonditions, our analysis suggests that popula-ion breast cancer screening in patients withnd-stage kidney disease on dialysis therapyay not be a good value for the money. De-
pite having the same breast cancer risk, mor-ality benefits from screening and early diseaseetection are considerably lower than in theeneral population. The poorer overall lifexpectancy and increased number of excesseaths from such causes as cardiovascular dis-ases other than cancers provide the rationaleehind these findings. From a patient’s perspec-ive, the decision to screen should be personal-zed and informed. For policy makers andlinicians, information and preferences abouthe benefits and harms of screening should notnly be given in an unbiased manner, but alsoe stratified according to the individual’s can-er risk, underlying comorbidities, life expect-ncy, and quality of life. Greater effort andtrategies are needed to identify women onialysis therapy for whom benefits from screen-ng outweigh the overall harms.
ACKNOWLEDGEMENTSThis report was presented in part at the 43rd Annual
cientific Meeting of the Australian and New Zealand Soci-ty of Nephrology, Gold Coast, Queensland, Australia, Sep-ember 8-12, 2007, the 40th American Society of Nephrol-gy Meeting, San Francisco, CA, October 31-November 5,007, and in cancer report for the Annual ANZDATA Regis-ry report (2007).
Support: G.W. is a recipient of a Kidney Health Australiaiomedical Scholarship and the Centre for Clinical Re-
earch Excellence in Renal Medicine Postgraduate Medicalcholarship.Financial Disclosure: None.
SUPPLEMENTARY MATERIALTable S1: Literature search to identify the best-available
vidence for use as input transition probabilities estimates
or the model.
aa
wv
bS
a
GmN
tm3
ep
uS
kb8
m1
CJ
ptIc1
mpS
As5
Cd
Ce2
m4
Ta1
if9
tiAl
lt
Cn&
Ewne
Bva
abH
AtA
Cas2
Wy3
af1
ofM
Ss
Wong et al928
Note: The supplementary material accompanying thisrticle (doi: 10.1053/j.ajkd.2008.06.015) is available at www.jkd.org.
REFERENCES1. Gotzsche PC, Nielsen M: Screening for breast cancer
ith mammography. Cochrane Database of Systematic Re-iews 4:CD001877, 20062. Andersson I, Janzon L, Sigfusson BF: Mammographic
reast cancer screening—A randomized trial in Malmo,weden. Maturitas 7:21-29, 19853. Shapiro S: Evidence on screening for breast cancer from
randomized trial. Cancer 39:2323-2964, 1977 (suppl 82)4. Tabar L, Fagerberg G, Duffy SW, Day NE, Gad A,
rontoft O: Update of the Swedish two-county program ofammographic screening for breast cancer. Radiol Clinorth Am 30:187-210, 19925. Shen Y, Zelen M: Screening sensitivity and sojourn
ime from breast cancer early detection clinical trials: Mam-ograms and physical examinations. J Clin Oncol 19:3490-
499, 20016. Gyrd-Hansen D, Holund B, Andersen P: A cost-
ffectiveness analysis of cervical cancer screening: Healtholicy implications. Health Policy 34:35-51, 19957. Hall J, Gerard K, Salkeld G, Richardson J: A cost
tility analysis of mammography screening in Australia. Socci Med 34:993-1004, 19928. Leivo T, Sintonen H, Tuominen R, Hakama M, Puk-
ala E, Heinonen OP: The cost-effectiveness of nationwidereast carcinoma screening in Finland, 1987-1992. Cancer6:638-646, 19999. Lindfors KK, Rosenquist CJ: The cost-effectiveness ofammographic screening strategies. JAMA 274:881-884,
99510. Vajdic CM, McDonald SP, McCredie MR, et al:
ancer incidence before and after kidney transplantation.AMA 296:2823-2831, 2006
11. EBPG Expert Group on Renal Transplantation: Euro-ean best practice guidelines for renal transplantation. Sec-ion IV: Long-term management of the transplant recipient.V.6.3. Cancer risk after renal transplantation. Solid organancers: Prevention and treatment. Nephrol Dial Transplant7 Suppl 4:32,34-36, 200212. Kasiske BL, Vazquez MA, Harmon WE, et al: Recom-endations for the outpatient surveillance of renal trans-
lant recipients. American Society of Transplantation. J Amoc Nephrol 11:S1-S86, 2000 (suppl 86)13. Winkelmayer WC, Owen W, Glynn RJ, Levin R,
vorn J: Preventive health care measures before and aftertart of renal replacement therapy. J Gen Intern Med 17:588-95, 200214. Chertow GM, Paltiel AD, Owen WF Jr, Lazarus JM:
ost-effectiveness of cancer screening in end-stage renalisease. Arch Intern Med 156:1345-1350, 199615. LeBrun CJ, Diehl LF, Abbott KC, Welch PG, Yuan
M: Life expectancy benefits of cancer screening in thend-stage renal disease population. Am J Kidney Dis 35:237-
43, 2000 m16. Briggs A, Sculpher M: An introduction to Markovodelling for economic evaluation. Pharmacoeconomics
:397-409, 199817. Walter LC, Lindquist K, O’Hare AM, Johansen KL:
argeting screening mammography according to life expect-ncy among women undergoing dialysis. Arch Intern Med66:1203-1208, 200618. Tabar L, Duffy SW, Yen MF, et al: All-cause mortal-
ty among breast cancer patients in a screening trial: Supportor breast cancer mortality as an end point. J Med Screen:159-162, 200219. The Australian Institute of Health and Welfare and
he Australian Government Department of Health and Age-ng for the BreastScreen Australia Program. BreastScreenustralia Monitoring Report 2001-2002. Canberra, Austra-
ia, Australian Institute of Health and Welfare, 200320. Brewer NT, Salz T, Lillie SE: Systematic review: The
ong-term effects of false-positive mammograms. Ann In-ern Med 146:502-510, 2007
21. Silverstein MJ, Recht A, Lagios M: Overview ofonservation Surgery and Radiation Therapy: Ductal Carci-oma In Situ (ed 2). Philadelphia, PA, Lippincott WilliamsWilkins, 2002, pp 287-30222. Fisher B, Land S, Mamounas E, Dignam J, Fisher
R, Wolmark N: Prevention of invasive breast cancer inomen with ductal carcinoma in situ: An update of theational surgical adjuvant breast and bowel project experi-nce. Semin Oncol 28:400-418, 2001
23. Australia Institute of Health and Welfare, Nationalreast Cancer Centre: Breast Cancer in Australia: An Over-iew, 2006. Canberra, Australia, Australian Institute of Healthnd Welfare, 2006
24. Austalian Government Australia Institute of Healthnd Welfare: AR-DRG Data Cubes From 2004-2005. Can-erra, Australia, Australian Government Department ofealth and Ageing, 200525. Australian Government Department of Health and
geing: Medicare Benefits Schedule Book. Canberra, Aus-ralia, Australian Government Department of Health andgeing, 200626. Webster AC, Craig JC, Simpson JM, Jones MP,
hapman JR: Identifying high risk groups and quantifyingbsolute risk of cancer after kidney transplantation: A cohorttudy of 15,183 recipients. Am J Transplant 7:2140-2151,00727. Hirth RA, Chernew ME, Miller E, Fendrick AM,eissert WG: Willingness to pay for a quality-adjusted life
ear: In search of a standard. Med Decis Making 20:332-42, 200028. George B, Harris A, Mitchell A: Cost-effectiveness
nalysis and the consistency of decision making: Evidencerom pharmaceutical reimbursement in Australia (1991 to996). Pharmacoeconomics 19:1103-1109, 200129. Harris A, Hill SR, Chin J, Li JJ, Walkom E: The role
f value for money in public insurance coverage decisionsor drugs in Australia: A retrospective analysis 1994-2004.
ed Decis Making 2008 Mar 31 [Epub ahead of print]30. Quinn RR, Naimark DM, Oliver MJ, Bayoumi AM:
hould hemodialysis patients with atrial fibrillation undergoystemic anticoagulation? A cost-utility analysis [see com-
ent]. Am J Kidney Dis 50:421-432, 2007
bI4
NatI
Ma2
Gtc
Tes
c3
ti
of4
Awr
ir9
mJ
CAlR
spA
Hc
r
fr
R
ea
tA
Ib
s9
Io
Tty
cR
ihC
csS
rtO
ibm
Nt
Kpct5
WBt
Ac
BoM
cr
Breast Cancer Screening and ESKD 929
31. Castellanos M, Varma S, Ahern K, et al: Increasedreast calcifications in women with ESRD on dialysis:mplications for breast cancer screening. Am J Kidney Dis8:301-306, 200632. Miller AB, To T, Baines CJ, Wall C: The Canadian
ational Breast Screening Study-1: Breast cancer mortalityfter 11 to 16 years of follow-up. A randomized screeningrial of mammography in women age 40 to 49 years. Annntern Med 137(Pt 1):305-312, 2002
33. Basnakian AG, Apostolov EO, Yin X, Napirei M,annherz HG, Shah SV: Cisplatin nephrotoxicity is medi-
ted by deoxyribonuclease I. J Am Soc Nephrol 16:697-702,00534. Pinder MC, Duan Z, Goodwin JS, Hortobagyi GN,
iordano SH: Congestive heart failure in older womenreated with adjuvant anthracycline chemotherapy for breastancer. J Clin Oncol 25:3808-3815, 2007
35. Chapman JR, Webster AW: Cancer Report, chap 10.he 25th Annual ANZDATA Registry Report 2002. Ad-laide, South Australia, Australian and New Zealand Dialy-is and Transplant Registry, 2003, pp 83-90
36. Evans AJ, Cohen ME, Cohen GF: Patterns of breastalcification in patients on renal dialysis. Clin Radiol 45:343-44, 199237. Brett J, Bankhead C, Henderson B, Watson E, Aus-
oker J: The psychological impact of mammographic screen-ng. A systematic review. Psychooncology 14:917-938, 2005
38. Brodersen J, Thorsen H, Cockburn J: The adequacyf measurement of short and long-term consequences ofalse-positive screening mammography. J Med Screen 11:39-4, 200439. Bloembergen WE, Port FK, Mauger EA, Wolfe RA:comparison of cause of death between patients treated
ith hemodialysis and peritoneal dialysis. J Am Soc Neph-ol 6:184-191, 1995
40. Berrington de GA, Reeves G: Mammographic screen-ng before age 50 years in the UK: Comparison of theadiation risks with the mortality benefits. Br J Cancer3:590-596, 200541. Glasziou P, Irwig L: The quality and interpretation ofammographic screening trials for women ages 40-49.Natl Cancer Inst 22:73-77, 199742. Wong G, Howard K, Craig JC, MacDonald S,
hapman JR: Cancer Report, chap 10. The 29th AnnualNZDATA Registry Report 2006. Adelaide, South Austra-
ia, Australian and New Zealand Dialysis and Transplantegistry, 2006, pp 137-14243. Barratt AL, Les IM, Glasziou PP, Salkeld GP, Hous-
ami N: Benefits, harms and costs of screening mammogra-hy in women 70 years and over: A systematic review. Med Just 176:266-271, 200244. Gorodetskaya I, Zenios S, McCulloch CE, et al:
ealth-related quality of life and estimates of utility inhronic kidney disease. Kidney Int 68:2801-2808, 2005
45. Gudex CM: Health-related quality of life in endstageenal failure. Qual Life Res 4:359-366, 1995
46. Kiberd BA, Keough-Ryan T, Clase CM: Screeningor prostate, breast and colorectal cancer in renal transplantecipients. Am J Transplant 3:619-625, 2003
47. Australia and New Zealand Dialysis and Transplant
egistry (ANZDATA): Special Data Request (2005). Ad- Elaide, South Australia, Australian and New Zealand Dialysisnd Transplant (ANZDATA) Registry, 2005
48. Mushlin AI, Kouides RW, Shapiro DE: Estimatinghe accuracy of screening mammography: A meta-analysis.m J Prev Med 14:143-153, 199849. Betsill WL Jr, Rosen PP, Lieberman PH, Robbins GF:
ntraductal carcinoma. Long-term follow-up after treatmenty biopsy alone. JAMA 239:1863-1867, 197850. Rosen PP, Braun DW Jr, Kinne DE: The clinical
ignificance of pre-invasive breast carcinoma. Cancer 46:919-25, 1980 (suppl 25)51. Page DL, Dupont WD, Rogers LW, Landenberger M:
ntraductal carcinoma of the breast: Follow-up after biopsynly. Cancer 49:751-758, 198252. Sanders ME, Schuyler PA, Dupont WD, Page DL:
he natural history of low-grade ductal carcinoma in situ ofhe breast in women treated by biopsy only revealed over 30ears of long-term follow-up. Cancer 103:2481-2484, 200553. Andersson I, Sigfusson BF: Screening for breast
ancer in Malmo: A randomized trial. Recent Res Canceres 105:62-66, 198754. Frisell J, Glas U, Hellstrom L, Somell A: Random-
zed mammographic screening for breast cancer in Stock-olm. Design, first round results and comparisons. Breastancer Res Treat 8:45-54, 198655. Tabar L, Gad A, Holmberg L, Ljungquist U: Signifi-
ant reduction in advanced breast cancer. Results of the firsteven years of mammography screening in Kopparberg,weden. Diagn Imaging Clin Med 54:158-164, 198556. Pejavar S, Wilson LD, Haffty BG: Regional nodal
ecurrence in breast cancer patients treated with conserva-ive surgery and radiation therapy (BCS�RT). Int J Radiatncol Biol Phys 66:1320-1327, 200657. Faneyte IF, Peterse JL, Van Tinteren H, et al: Predict-
ng early failure after adjuvant chemotherapy in high-riskreast cancer patients with extensive lymph node involve-ent. Clin Cancer Res 10:4457-4463, 200458. Barratt A, Howard K, Irwig L, Salkeld G, Houssami
: Model of outcomes of screening mammography: Informa-ion to support informed choices. BMJ 330:351-356, 2005
59. Rhodes A, Jasani B, Balaton AJ, Barnes DM, MillerD: Frequency of oestrogen and progesterone receptorositivity by immunohistochemical analysis in 7016 breastarcinomas: Correlation with patient age, assay sensitivity,hreshold value, and mammographic screening. J Clin Pathol3:688-696, 200060. Bland KI, Menck HR, Scott-Conner CE, Morrow M,inchester DJ, Winchester DP: The National Cancer Dataase 10-year survey of breast carcinoma treatment at hospi-
als in the United States. Cancer 83:1262-1273, 199861. Cancer Institute NSW: Standard cancer treatment.
vailable at: https://www.treatment.cancerinstitute.org.au/ancerinstitute. Accessed September 29, 2007
62. Fassbender K, Fainsinger R, Brenneis C, Brown P,raun T, Jacobs P: Utilization and costs of the introductionf system-wide palliative care in Alberta, 1993-2000. Palliated 19:513-520, 200563. Guest JF, Ruiz FJ, Greener MJ, Trotman IF: Palliative
are treatment patterns and associated costs of healthcareesource use for specific advanced cancer patients in the UK.
ur J Cancer Care 15:65-73, 2006














![Screening for Breast Cancer[1]](https://img.dokumen.tips/doc/110x75/577d2c841a28ab4e1eac7094/screening-for-breast-cancer1.jpg)