Embed Size (px)
Citation preview

Cooling the Injured Brain in Children in 2015
Where are we in the cold light of day?
To Cool or Not Cool the Brain?

Hypothermia reduces all aspects of secondary injury
• Energy failure
• Excitotoxicity – Excitatory amino acids such as glutamate stimulate NMDA and other receptors
• Mitochondrial injury
– Increased permeability dysfunction apoptosis and free radicals
• Oxidative stress/free radicals
• Apoptosis
• Inflammation

Optimal Duration and Therapeutic Window of Hypothermia after Global Cerebral Ischaemia
• Optimal temperature is 32 - 33°C
• Narrow therapeutic window – 4 hours
• Optimal duration 48 hrs minimum

Delay-dependent protection with hypothermia
Gunn et al 1997, 1998, 1999

Fever in Acquired Brain Injury
• Fever is common after acquired brain injury
– 40-45% within first 24hrs children and adults
• Fever is bad – it is associated with worse outcome in acquired brain injury

Hyperthermia increases all aspects of secondary injury

Fever is bad for the injured brain
• Association not cause – In animals active cooling of fever reduces damage
• Adults
– Fever associated with increased mortality and worse neurological outcome – Each degree >37.0°C, OR 2.3 unfav neuro outcome
• Children
– Temp persistently >38°C in first 24hrs (5.5%), OR 2.7 unfav neuro outcome
• Neonates
– Each degree >37.0°C, OR 3.6-4 death/disability
Zeiner, Arch Int Med,2001; Bembea, PCCM, 2010; Laptook, Pediatrics, 2008

Therapeutic Hypothermia
• The most studied neuroprotective therapy so far
• Clinical trial evidence – TBI Primary/early - neuroprotective
– TBI Secondary/late - adjuvant therapy for intracranial hypertension
– HIE after cardiac arrest
– Other • Stroke
• Meningitis

Traumatic Brain Injury
• There is no evidence for a beneficial effect of early hypothermia on outcome in TBI
• All multi-centre RCTs in adults and children have been negative
• This could be because – Not early enough (POLAR – ANZICS CTG) – Not long enough – Rewarming too fast – It doesn’t work
• Early hypothermia should not be used in TBI outside of an RCT

Georgiou, BJA, 2013

Trials in Children – CoolKids, HiTBIC
020
40
60
80
10
0
Cu
mula
tive
Pro
po
rtio
n
6 5 4 3 2 1PCPCS at 12 months
Hypothermia Normothermia
Adelson, Lancet Neurology, 2013 Hutchison, Lancet Neurology, 2013 Beca, HiTBIC, CCM, 2015
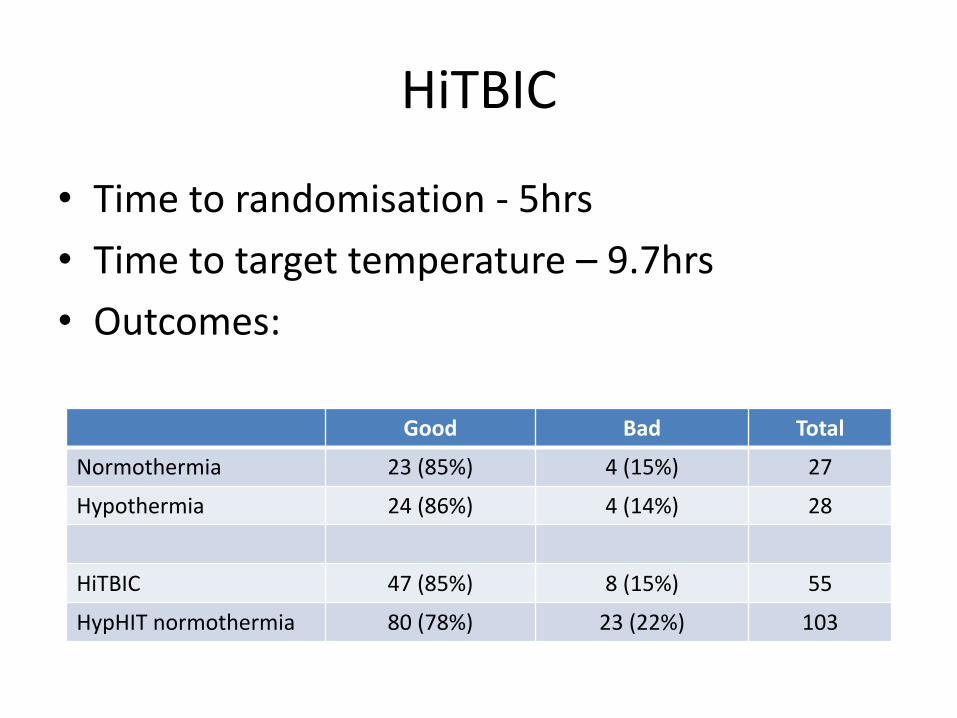
HiTBIC
• Time to randomisation - 5hrs
• Time to target temperature – 9.7hrs
• Outcomes:
Good Bad Total
Normothermia 23 (85%) 4 (15%) 27
Hypothermia 24 (86%) 4 (14%) 28
HiTBIC 47 (85%) 8 (15%) 55
HypHIT normothermia 80 (78%) 23 (22%) 103

Clifton, NABIS II, Lancet Neurology, 2010
• Adult TBI
• Enrolled < 2.5hrs
• Cooled for 48hrs
• No difference overall
• Surgically removed haematomas did better with TH
• Diffuse brain injury did worse
• POLAR study awaited

TBI – Late Hypothermia
• Almost all studies show that ICP is lower during TH
• No outcome studies (Eurotherm)
• After sedation/paralysis/osmotherapy, other options either show harm (decompression) or there are no outcome data
• Good evidence for safety of TH in all ages
01
02
03
0
Me
an
IC
P ±
SD
0 20 40 60 80 100Hours after randomisation
Hypothermia Normothermia
0-72 hrs p 0.043 & 72-100 hrs p 0.877

Traumatic Brain Injury
• TH should not be used early for neuroprotection outside of an RCT
• TH may have a role as adjuvant therapy to control ICP. One of several unproven options and safety established
• Temperature control in normothermia groups often poor
• Goal should be strict normothermia

Hypothermia for Neonatal HIE

Cooling in neonates - multiple pragmatic clinical trials
• Mortality • 1555 infants in 11 trials
• Neurodevelopmental outcome at >=12 months:
• 1395 infants in 8 trials
• High consistency between trials • Period of hypothermia: 48 to 72 hours
• Target temperature 34.5°C for head cooling, 33.5°C for WBC
• Outcome assessment: death or moderate-severe disability

Death or disability at 12 or 18m
• NNT 6 (5, 9)
• Absolute risk reduction: 0.16

Components of outcome are concordant

Smaller effect with severe HIE RR 0.83 vs 0.67, p<0.04
NNT 5 (3, 7)
NNT 8 (5, 20)

Head vs whole body cooling? About the same

Long term follow up
• TOBY study @ 6-7 years of age
• Outcomes HYPO NORM
– Mortality rates similar 29% 30%
– IQ ≥ 85 52% 39%
– CP 21% 36%
– Mod-severe disability 22% 37%
Azzopardi, NEJM, 2014

What we know now
High rate of poor outcome despite cooling
Death/disability: 45% vs 61%
Intact survival: 40% vs 24%
Cooling improves outcome after moderate-severe encephalopathy in newborn infants.
• Outcome improved, but to a lesser extent, after severe encephalopathy
• Functional recovery delayed by cooling
• Similar results from all cooling methods

Hypothermia for Neonatal HIE
• “The remarkable homogeneity of trial results provides unequivocal evidence of therapeutic benefit of prolonged hypothermia”
Edwards, BMJ, 2010
• Mechanism of injury somewhat different
– More prolonged – Cardiac arrest rates unclear – 2/3 in 2 trials – Early implementation possible
• Normothermic control
– ICE (2011) 14%>38°C, assoc with increased mortality – Simbruner (2010) 13%>38°C – Azzopardi (2009) 23%>38°C – NICHD (2005) 39%>38°C, assoc death/disability
• Role for a study of 36°C vs 33°C?

Cooling in adults
• 2 studies published in NEJM in 2002
• Bernard
– 77 patients, quasi-randomisation, unusual outcome
– Good outcome 49% vs 26% (OR 5.25)
• HACA
– Randomised 275 (8%) of 3551, no predefined power calculation, stopped early
– Good outcome 55% vs 39%
• 12-24 hours hypothermia became standard of care for adults after community
VF arrest
• Neither study maintained strict normothermia in control group
• Is it better than strict normothermia?


Scandanavian TTM RCT
• Cooling protocol – 4hrs to cool, 24hrs at goal temperature, 8hrs to
rewarm (0.5°C per hour max)
– Sedation weaned or stopped once rewarmed
– Temperature <37.5°C till 72hrs after arrest
– Neurological assessment 72hrs after rewarmed (108hrs after start protocol)
• 36°C is still active therapy – ?more difficult than 32-34°C

Scandanavian TTM RCT
• 939 patients – More than twice the size of the original trials combined
– Superb methodology and performance
– Protocol for withdrawal of life-sustaining therapies
– Approximately 50% “good” outcome

TTM Reactions
• Stephen Bernard (BMJ, 2014, 11 April) – The TTM trial should change practice immediately – Patients resuscitated from OHCA…should not receive TH (32-34°C) – Prognostication should be delayed for at least 72hrs after sedation
stopped, unless BD or myoclonus with bilaterally absent SEPs
• Kees Polderman (Crit Care, 2014,04 April)
– We urge our colleagues not to abandon TH in favour of strict fever management on the basis of one study
– ?enrolment bias – Relatively rapid rewarming from 33-36°C – ?slight imbalance

Cooling in children • What should we do?
– “may be considered for children who remain comatose after resuscitation”
• No difference in mortality in 2 cohort studies Fink, PCCM, 2010; Doherty, Circulation, 2009
• HypCAP, Hutchison – Toronto, Auckland, GOS – Phase 2 pilot RCT
Hypothermia Group (N=19)
Normothermia Group (N=19)
P-value
PCPC 4-6 (6 months) 13 (68) 10 (53) 0.60
Mortality (28 days) 12 (63) 8 (42) 0.19

• 295 patients randomised • Age >48hrs and <18yr • Randomised within 6hr
• 32-34°C vs 36-37.5°C • TTM for 120hr in both groups i.e. active normotheria
• Temperature maintained for 48hr, rewarmed over 16hr • Both groups <37.5°C till 120hr
• Mechanism of cardiac arrest different to adults
• 8% VT/VF
• Outcomes worse than in adults
NEJM, April 2015, p1898
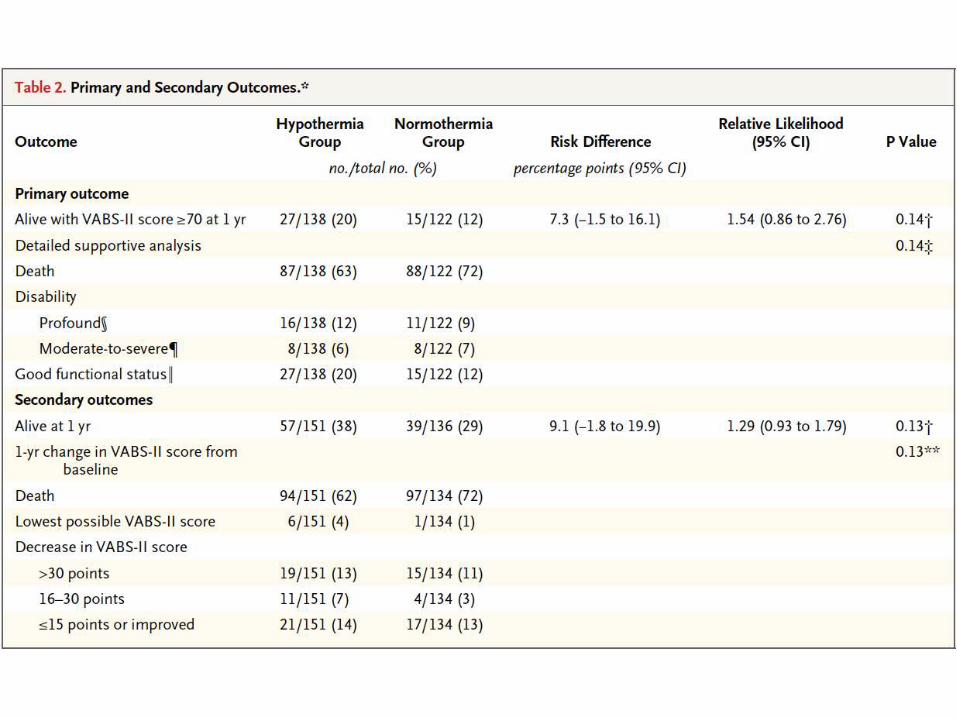

THAPCA
• No difference in primary or secondary outcome – 20% (hypo) vs 12% (norm) with VABS-II ≥70 – 14% (hypo) vs 13% (norm) with VABS-II ≤15
• Issues
– Power • Outcome rate 15-35%, absolute effect size 15-20% • If outcome rate 12% and effect size 8%, need ≈ 900 patients
– Time to be cold • Median time to start cooling 5.9hr, reach goal 2.6hr • Is this too slow?
– 120hr is a long time to maintain TTM

Hypothermia after Cardiac Arrest
• Evidence does not currently support moderate (32-34°C) hypothermia apart from in birth asphyxia
• Fever is common with HIE and associated with worse outcome
• Excellent large adult RCT that suggests equivalent outcomes with temperature 36°C
• THAPCA trial does not show a benefit
• Is 36°C mild hypothermia or controlled normothermia?

How well do we control temperature?
• First 24hrs after IHCA in children – 43.5% ≥1 temperature >38.0°C – 5.5% persistently >38.0°C (OR 2.7 unfav outcome) – No difference after 2005 guidelines
Bembea, PCCM, 2010
• Most trials set upper limit 37.5°C in control group
– CoolKids – 68% exceeded 37.5°C over first 48hrs – HiTBIC (<37.0°C) – 40% exceeded 38.0°C over first 72hrs
• Technical challenges of temperature control and
cooling blankets

Hypothermia for Meningitis
• Mourvillier et al, JAMA, 2013, 98 adults
• Outcome not improved and may be harmful

Predicting Outcome with TTM
• 20 studies, 1845 patients
• 3 tests most accurate – Absent pupil reflexes > 24rs FPR 2% (1-6%)
– Absent corneal reflexes > 24hrs FPR 4% (1-9%)
– Bilat absent SEPs days 1-7 FPR 3% (1-7%)
• All tests better >72hrs after ROSC – Care when predicting earlier than this

Prediction of Outcome with TTM
Sensitivity Specificity FPR (%) Positive LR
Corneal reflex ≤72hrs 0.33 0.98 2 8.4
>72hrs 0.20 1.00 0 4.3
Pupillary reflex ≤72hrs 0.27 0.99 1 16.5
>72hrs 0.18 1.00 0 4.7
Motor score M1 or M2 ≤72hrs 0.63 0.90 10 6.8
>72hrs 0.59 0.96 4 9.5
Unfavourable EEG ≤72hrs 0.57 0.96 4 8.7
>72hrs 0.80 1.00 0 7.3
SEPs ≤72hrs 0.40 1.00 1 16.1
>72hrs 0.44 1.00 0 7.5
Myoclonic status ≤72hrs 0.27 0.98 2 5.2
NSE >33 ≤72hrs 0.51 0.89 11 4.1
Golan, CCM, 2014

Hypothermia in Acquired Brain Injury
• TBI – NO (unless part of a RCT) – May have role as adjuvant therapy for intracranial hypertension
• After cardiac arrest – NO, except
– Birth asphyxia in neonates – YES – In hospital or if can be applied very early – unknown
• In meningitis or stroke - NO
• Fever is common in acute brain injury and associated with worse outcome
• All children with an acute brain injury should have strict TTM – Duration uncertain but probably at least 72hr
• Currently in TBI and HIE we maintain temp 36-37°C (set point 36.5°C) for 72hr
– In HIE set point 36.0°C (35.5-36.5) for initial 24hr – Then assess in HIE – Duration in TBI will be influenced by ICP



What is normal temperature?
• 35.5-37.5°C – Diurnal rhythm of ±0.5°C, lower in morning – Varies with site and method of measurement – Variable relationship to brain temperature – NICE define as 36.5-37.5°C
• Definitions of hypothermia vary
– Is 36.0°C hypothermia or normothermia?
• Mild hypothermia is required to avoid fever

How much? 32-34°C
Parasagittal neuronal loss (%)
30 32 34 36 38 400
25
50
75
100
Sham Hypothermia
Hypothermia, 90 min
Extradural temperature, 4-8 h (oC)
Between 32-34°C is
optimal
Term fetal sheep studies

Who would you cool to moderate TH? (15 years later)
1. An 8 year old with severe TBI (GCS 5) and a CT showing contusions and shear injury 2hrs after injury?
1. A 4 week old infant 2hrs after OHCA from presumed SIDS?
2. A 14 year old 2hrs after OHCA from a witnessed VF arrest during sport?
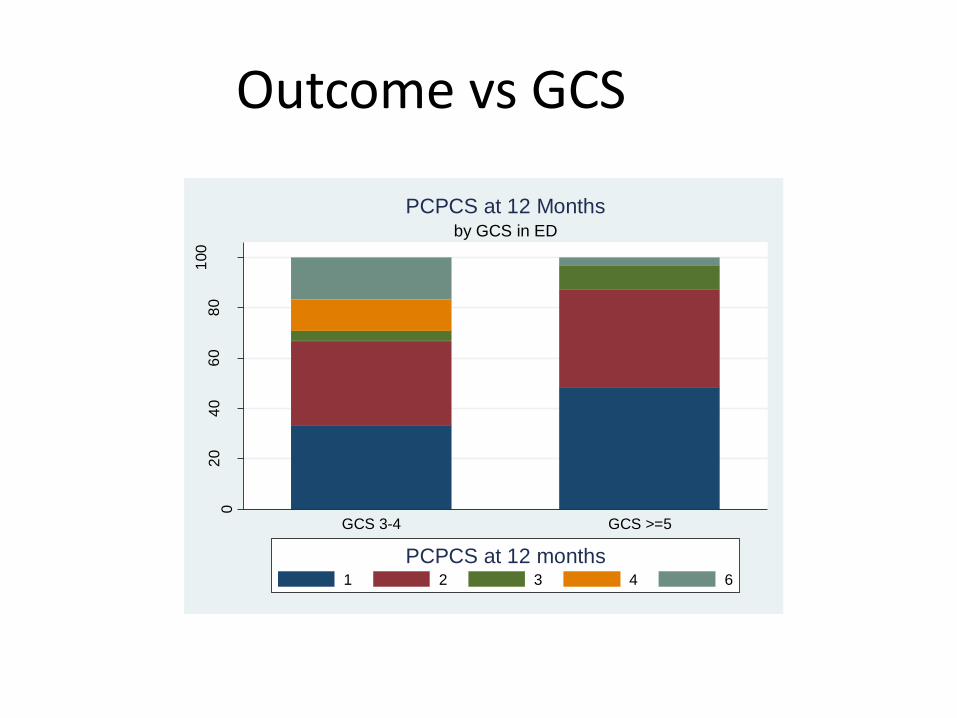
02
04
06
08
01
00
perc
ent
GCS 3-4 GCS >=5
by GCS in ED
PCPCS at 12 Months
1 2 3 4 6
PCPCS at 12 months
Outcome vs GCS

Survival with MDI>84, PDI>84 and no neuromotor impairment and normal vision and hearing.
NNT 6 (95% CI: 5-10)
Normal survival, with no disability

Hypothermia in Stroke
• Phase 1 and 2 studies have shown – Reduction in ICP, especially with large MCA strokes – Proactive shivering protocols are necessary – Shivering less of a problem with intravascular cooling compared
to surface cooling – Appears to be safe both with thrombolysis and caffeinol
• 2 large phase 2/3 studies underway of TH in patients also
receiving thrombolysis – ICTuS 2/3 – 1600 patients – EuroHYP-1 – 1500 patients
• Currently should only be used as part of a RCT





























