Embed Size (px)
Citation preview

Convulsive Status epilepticus
Dr. Jithangi Wanigasinghe Senior Lecturer
Consultant Paediatric Neurologist MPhil, MD, DCH

Scope
• What is CSE in the ED? – Operational definition and new definition
• What are we dealing with? – Underlying aetiology
• What do we do? – Optimal management

Definition
Single seizure lasting more than 30-min duration or a series of epileptic seizures during which function is not regained between ictal events in a 30-min period Commission of Epidemiology and prognosis ILAE 1993

Operational definition for management of SE
Generalized, convulsive status epilepticus in adults and older children refers to a 5 min of (a) continuous seizures or (b) two or more discrete seizures between which there is incomplete recovery of consciousness Lowenstein D H 1999

New definition of CSE
Status epilepticus is a condition resulting either from the failure of the mechanisms responsible for seizure termination or from the initiation of mechanisms, which lead to abnormally, prolonged seizures (after time point t1). It is a condition, which can have long-term consequences (after time point t2), including neuronal death, neuronal injury, and alteration of neuronal networks, depending on the type and duration of seizures.
Trinka E. 2015

Conceptual definition with two operational time points
Length of the seizure and the time point (t1) beyond which the seizure should be regarded as “continuous seizure activity.”
t1 t2 Onset
The time of ongoing seizure activity after which there is a risk of long-term consequences
Epidemiology
• 50 per 100,000 population • Highest in children • Bimodal increase in incidence • Significant mortality
– 22%-23% for children – 26% for adults
• Neurological morbidity in 11-16% • Refractory SE (RSE) is common (31-44%)

Early phase Premonitory SE, Impending SE
Established SE
Refractory SE Subtle SE, stuporous SE
Super-refractory SE : SE that continuous in spite of treatment with anaesthetics for > 24 hrs
Stage 1
Stage 2
Stage 3
Stage 4
5-10 min
10-30 min
30-120 min
>24 h
Stages of SE
Scope
• What is CSE in the ED? – Operational definition and new definition
• What are we dealing with? – Underlying aetiology
• What do we do? – Optimal management

Underlying aetiology
• Commonest single group of causes is acute symptomatic aetiology
• Same for adults and children • In adults
– CVA commonest in developed countries and elderly
– CNS infections commonest in developing countries Murthy J M K
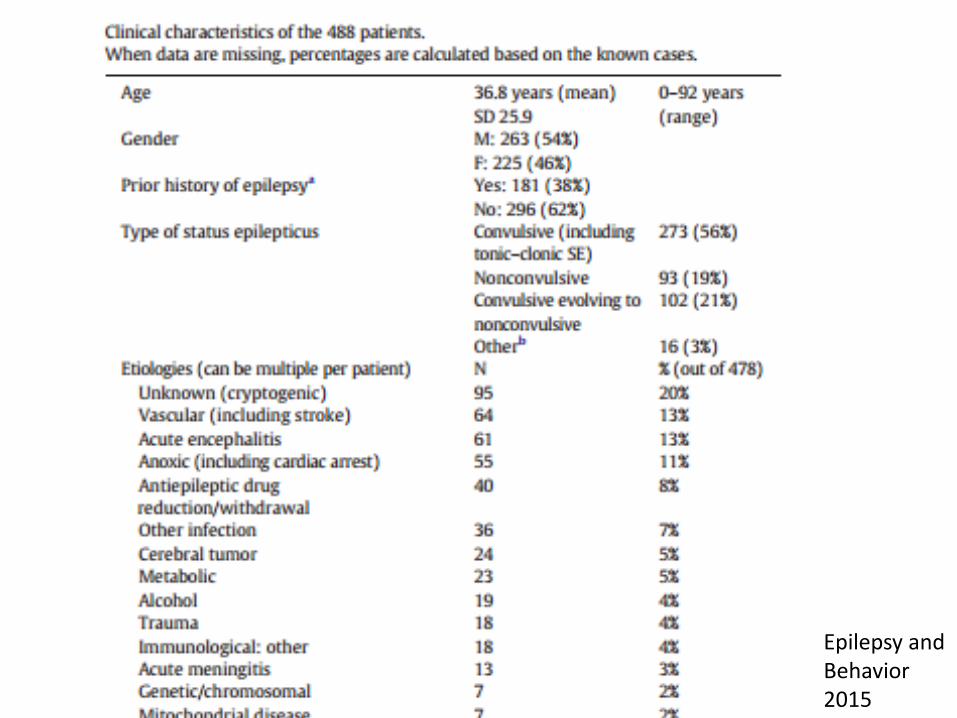
Epilepsy and Behavior 2015

Causes of CSE in children
Shorvon S 2006
• Hypoxic brain injury • CNS Infections • Traumatic brain injury • Metabolic derangements • CNS demyelinataion • Vascultis, Autoimmune encephalitis

Acute symptomatic 9 (31%) Febrile status 4 (13%) Remote symptomatic 4 (13%) Epilepsy 7 (24%) Unclassified 2 (06%) n=29

Scope
• What is CSE in the ED? – Operational definition
• What are we dealing with? – Underlying aetiology
• What do we do? – Optimal management

Therapeutic principles
• Address pathophysiology – GABAA Agonists – NMDA antagonists – multiple receptors or ion channels
• Rx plan according to stages • Considerations
– ease of administration – onset of action (rapid) – duration of action (intermediate to long) – spectrum of activity (broad) – minimal morbidity

Therapeutic principles
• Commence rapidly and continue sequentially • Use therapeutic doses ALWAYS • Critical care treatment and monitoring • Treatment of underlying cause • Commencement of neuro-protective
mechanisms • Constant management of complications

Early phase Premonitory SE, Impending SE
Established SE
Refractory SE Subtle SE, stuporous SE
Super-refractory SE : SE that continuous in spite of treatment with anaesthetics for > 24 hrs
Stage 1
Stage 2
Stage 3
Stage 4
5-10 min
10-30 min
30-120 min
>24 h
Stages of SE

Early phase (MAY BE PRE or IN HOSPITAL) Premonitory SE, Impending SE
Stage 1 5-10 min
Stages of SE
BDZ first choice for out-of- hospital Mx IV – Lorazipam (Alldredge BK 2001)
IM – Midazolam Rectal Diazepam in children (Dreifuss FE 1998)
IV Diazepam Nasal or buccal – MDZ (Scott RC 1999, McIntyre J 2005)
Clear benefit of prehospital Rx with LRZ or DZP

Early phase SE
Trinka E 2015
Key highlights
• Out of hospital administration – Clear benefit shown due to early SE abolition – Buccal MDM favoured over DZP
• In hospital when resuscitation facilities available – Use the IV preparations recommended – Lorazepam favoured

Established SE Stage 2
5-10 min
10-30 min
Stages of SE
Second-line drugs when BDZ fail to terminate IV phenytoin/fosphenytoin IV phenobarbate IV sodium valproate IV leveteracetam
• water solubility and neutral pH • more rapid administration with less adverse effects • compatibility with all IV fluids
No clear evidence to support one over the other for CSE termination
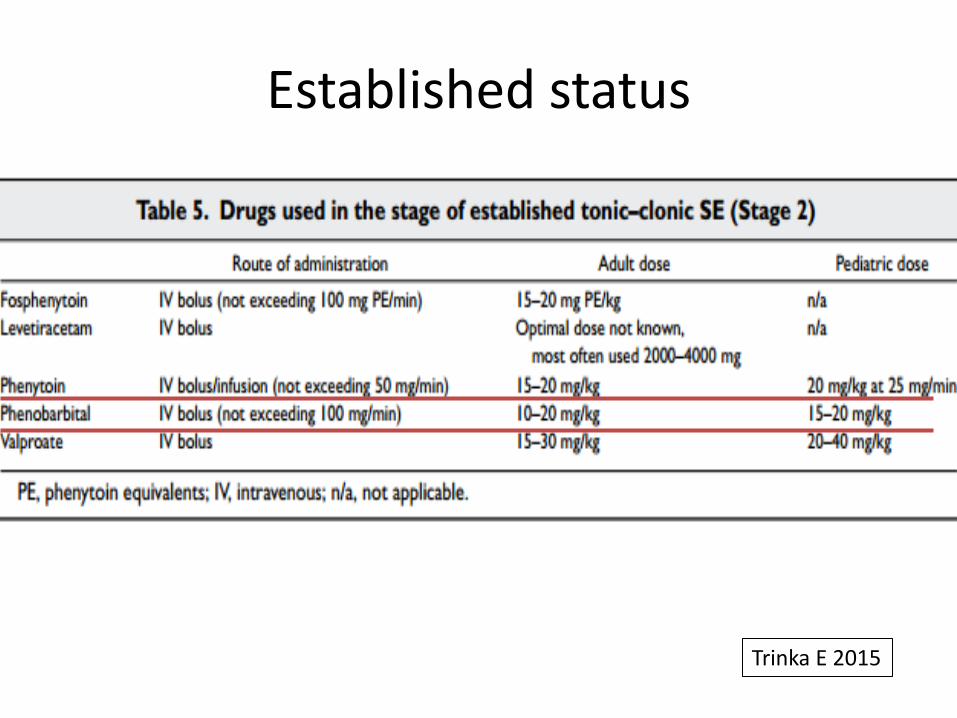
Established status
Trinka E 2015

Refractory SE Subtle SE, stuporous SE
Stage 3
5-10 min
10-30 min
30-120 min
Stages of SE
• NO RCTs • Continuous infusion (cIV) of anesthetic agents: - Thiopental/ pentabarbital, midazolam and propofol (Shorvon S 2012) • Successful Rx with propofol in 2/3 of RSE • For 24–48 hours of electrographic control by cEEG
monitoring • Dosing titrated to cessation of electrographic seizures or burst suppression
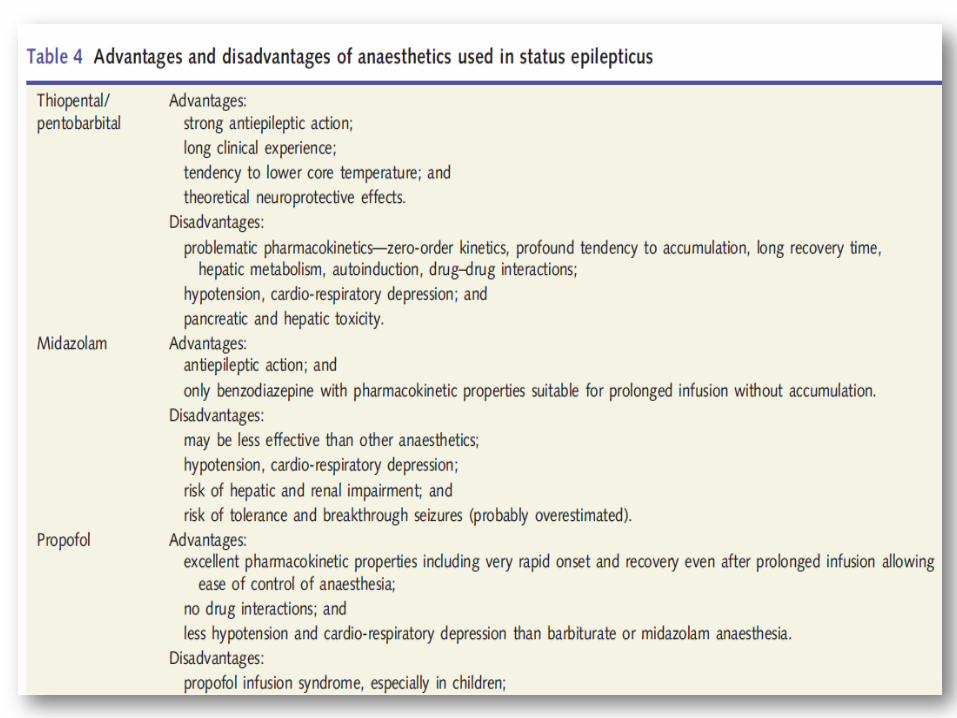

• Propofol: IV bolus 2 mg/kg, repeated if necessary, followed by a continuous infusion of 5–10 mg/kg/hour initially, reducing to maintain a burst suppression (usually 1–3 mg/kg/hour)
• Thiopental: IV bolus 100–250 mg given over 20 s with further 50 mg boluses every 2–3 min until seizures are controlled, followed by a continuous IV infusion to maintain a burst suppression (usually 3–5 mg/kg/hour)
• Midazolam: IV bolus 0.1–0.3 mg/kg at a rate not exceeding 4 mg/min initially, followed by a continuous IV infusion to maintain a burst suppression pattern (0.05–0.4 mg/kg/hour).

Super-refractory SE : SE that continuous in spite of treatment with anaesthetics for > 24 hrs Stage 4
5-10 min
10-30 min
30-120 min
>24 h
Stages of SE No RCTS Use different conventional AEDs – TPM (via NG), Lacosamide, LEV Inhalational agents - isoflurane and desflurane IVIG, High dose steroids Ketamine (NMDA receptor Antagonist) Budesonide Ketogenic diet Magnesium Sulphate, pyridoxine Epilepsy surgery, Vagal nerve stimulation, DBS
10-15% of all CSE Outcome – 35% mortality, 35% recovery to baseline (Shorvon S 2012)

Anaesthetics in SRE
• How long to use? – Exotoxic damage already occurred – ?Risk of anaesthesia exceed risk of SE?
• Complications of anaesthesia • How to cycle?
– Initially 24-48 hour cycles and then longer • Should one switch anaesthetics?
– Prolonged propofol carries specific risk – What stage to switch ??
• NO DATA ON THESE POINTS

Anti Epileptic drug therapy
• Approach to use AEDs in SRE (via NG / PEG) • Purpose – coverage when anaesthetic effects are
withdrawn • Principles
– Polytherapy with two – High dose – Avoid frequent switching – Favour those with lower interaction potential,
predictable kinetics and without renal or hepatic toxicity
– Avoid GABAergic AEDs

Concommittent multimodal approach

Common reasons for treatment failure
• Under-dosing at the stage of established SE • Neglecting maintenance therapy • Misdiagnosis- i.e. psychogenic nonepileptic
status, drug-induced or metabolic encephalopathy
• Failure to identify and treat the underlying etiology
• Failure to address Iry complications

Continuous EEG (cEEG) monitoring
• Initiated for RSE (after one hour) • Useful for titration of other maintenance AEDs • Duration – at least 48 hours if NCSE • treatment endpoints for cEEG monitoring
– cessation of nonconvulsive seizures – diffuse beta activity – burst suppression 8–20 seconds’ intervals – complete suppression of EEG

Supportive management
• Assisted ventilation and cardiovascular monitoring
• Vasopressor agents • Cerebral oedema lowering agents • Continuation of maintenance AEDs • Brain cooling
Systemic complications of SRE
• Complications due to therapy with inhalational Anaesthetics – Hypothermia, infection, death
• Complications due to prolonged ICU stay and immobility – PE, DVT – Pulmonary complications – Sepsis,colitis – Skin complications, fungal infections – Critical illness nopathy/ neuropathy

• Complications due to status and treatment
• Complications due to treatment
Systemic complications of SRE

Prognostic factors
• Poor outcome related to – underlying etiology – de novo development of SE in hospitalized
patients – older age – impairment of consciousness – duration of seizures – focal neurological signs at onset – presence of medical complications


Summary
• What is CSE in the ED? – Operational definition
• What are we dealing with? – Underlying aetiology
• What do we do? – Optimal management































