Embed Size (px)
Citation preview

*CorrespondVascular SurPerugia, ViaE-mail address
1078–5884/00
Conversion to Open Repair After Endografting for AbdominalAortic Aneurysm: Causes, Incidence and Results
F. Verzini, P. Cao,* P. De Rango, G. Parlani, D. Xanthopoulos,G. Iacono and G. Panuccio
Department of Vascular Surgery, University of Perugia, Azienda Ospedaliera di Perugia, Perugia, Italy
Objective. To evaluate frequency, causes and results of conversion to Open repair (OR) after endovascular repair (EVAR) ina single centre during an 8-year period.Design. Six hundred and forty-nine consecutive patients undergoing EVAR were followed up prospectively for endograft-related complications.Outcomes. Early conversion was any OR during or within 30 days from the primary EVAR. Late conversion was any ORwith removal of the endograft after 30 days since a completed EVAR procedure.Results. Median patient follow-up was 38 months (1–93 months). Conversion to OR was performed in 38 patients; nineearly and 29 late. Most (7/9) early conversions were due to extensive vessel calcification. Peri-operative mortality was 22%(2/9). Late conversions occurred at a median of 33 months after primary EVAR: 29 were elective and 4 urgent. During thesame interval, 79 secondary endovascular interventions were performed, 7 of which failed. The risk of conversion to OR was9% at 6 years. At multivariate logistic regression analysis, no single factor (short, large or angulated neck, suprarenalfixation, large pre-operative diameter, iliac aneurysms, ASA score risk) was associated with the risk of late failure requiringconversion to OR.Conclusion. The risk of death after early conversion should be recognized, to avoid forcing morphological indications forprimary EVAR. Occurrence of late conversion after EVAR is not negligible, affecting almost 1 out of 10 patients after 6 years.In the presence of an expanding aneurysm after EVAR, especially after a failed secondary endovascular correction, anaggressive attitude in fit patients allows outcomes at similar to those of primary OR.
Keywords: Conversion; Abdominal aortic aneurysm; Endovascular repair; Open repair.
Introduction
Recently published trials comparing endoluminalrepair of abdominal aortic aneurysm (EVAR) versusopen surgery have shown no differences in overallsurvival rates, although a lower risk of aneurysm-related death at a cost of a higher reintervention ratehas been reported.1,2 These data confirm the results ofmonocentric non-randomised series in which theadvantage of EVAR over open repair (OR) wasmaintained at least 7 years, even though the risk ofreintervention was about 50% for longest availablefollow-up.3,4 Usually, most EVAR complications even-tually leading to aneurysm rupture, such as migration,endoleak and structural graft failures, can be treatedwith adjunctive endovascular procedures and rarely
ing author. Prof Piergiorgio Cao, MD, FRCS, Chief ofgery, University of Perugia, Azienda Ospedaliera diBrunamonti, Perugia 06122, Italy.: [email protected]
0136 + 07 $35.00/0 q 2006 Elsevier Ltd. All rights reser
require conversion to OR.5–8 Open surgery under suchcircumstances is usually considered more risky thanthe primary operation, due to the presence of theendograft in the operating field and the urgentcondition.9 Initial experiences showed high mortalityand morbidity rates mainly associated with immediateconversions performed during the course of theprimary planned EVAR procedure.9 The aim of thisstudy is to evaluate frequency, causes and results of allconversions to OR after EVAR in our series of 649consecutive patients treated during an 8-year period.Predictive factors of late conversion also wereinvestigated.
Material and Methods
Between April 1997 and March 2005, a total of 1303consecutive patients with AAA underwent electiverepair in our department: 654 (50.2%) with OR and 649
Eur J Vasc Endovasc Surg 31, 136–142 (2006)
doi:10.1016/j.ejvs.2005.09.016, available online at http://www.sciencedirect.com on
ved.

Table 1. Demographic data and risk factors on 38 patientsconverted to open repair
%
Median age (years) 72Gender (male) 33 87Smoking 27 71Hypertension 23 61Diabetes 1 3Cardiac disease 14 37Respiratory disease 18 47Renal insufficiency 5 13ASA class (III or IV) 29 76
Conversion After Endovascular Repair of Aortic Aneurysm 137
(49.8%) with EVAR. The indications for EVAR versusOR have been described in a previous report.3
A wide variety of endografts were used: theAneuRx stent graft (Medtronic, Santa Rosa, CA,USA) was implanted in 238 procedures, the Zenithgraft (William Cook Europe, Biaeverskow, Denmark)in 181, the Talent graft (World Medical-Medtronic,Sunrise, FL, USA) in 98, the Excluder (WL Gore andAssociates, Flagstaff, AZ, USA) in 81, the Fortron(Cordis, Warren, NJ, USA) in 36, the Anaconda in 11(Sulzer Vascutek, Edinburgh, UK), the Endologix(Bard, Irvine, CA) in 3, and the Endofit (Endomed,Phoenix, AZ, USA) in 1. Endograft configurationincluded 4 tubes, 624 bifurcated grafts, and 21 aorto-uniliac grafts.
Follow-up schedule consisted of physical exam-ination, color duplex scan and plain abdominalX-ray repeated at 1, 6, 12 months after theprocedure and every 6 months thereafter. Contrast-enhanced CT scan was performed 1 month aftersurgery and then annually. All data were collectedprospectively in a database. Median follow-up was38 months (range 1–93 months). Three patientsrefused regular imaging follow-up after the first-year.
Early conversion was considered as any open AAArepair during or within 30 days from the primaryendovascular operation. Late conversion was con-sidered as any OR with removal of the entireendograft, or at least the main body of the endograft,occurring anytime 30 days after a completed EVARprocedure.
Indications for late conversions were: AAAgrowthO5 mm with or without endoleak, late onsetof high flow type I or III endoleak with or withoutaneurysm growth, loss of contact between theendograft and the aortic neck due to graft migrationor neck dilation and AAA rupture. Type II endoleakswere observed, without treatment, when these werenot associated with AAA diameter increase. In cases ofAAA growth, conversion to OR was offered to patientsfit for surgery, whereas a lumbar CT guided percuta-neous puncture with embolization of the aneurysmalsac was offered to higher risk patients with type IIendoleak.
In the presence of complications indicative of EVARfailure, from CT examination, the indication forconversion was established after evaluation of thefeasibility of a secondary endovascular procedure andaccording to patient choice when fit for open surgery.In all cases a complete risk/benefit assessment wasperformed for each patient.
Statistical analysis
For risk factors and pre-operative findings statisticalsignificance was assessed using two-tailed c2 test withYates correction or Fisher exact test. For each outcomeeither an odds ratio (OR) or hazard ratio (HR) with95% confidence intervals (95% CI) were calculated bystandard methods. Continuous variables were dis-played as median values and ranges. Risk of lateconversion was calculated by life table analysis(Kaplan–Meier method with log-rank test). To identifypotential predicting factors of late conversion, multi-variate analyses with conditional logistic-regressionmodels were used. Variables chosen for inclusion inthis model were age, female gender, AAA diameter,proximal neck diameter, neck length, neck angulation,extensive iliac aneurysmal involvement (Eurostarclass D or E), ASA score and infrarenal fixation.Significance was at the 5% level. Statistical packageSoftware SPSS (SPSS Inc., Chicago, IL, USA) was usedfor analysis.
Results
Of 649 patients who underwent EVAR, successful graftdeployment was achieved in 640 patients (98.6%).Conversion to OR was performed in 38 patients.Immediate conversion was required in nine patients(1.4%), while 29 patients (4.5%) required late ORduring a median follow-up of 38 months.
Median age of 38 patients undergoing conversion toOR was 72.2 years (range 55–85 years). Demographicdata and risk factors for all conversions are shown inTable 1.
Early conversion
Early conversions occurred at all stages of the primaryoperation, in eight males and one female with amedian age of 76 years (range 71–81 years).
Eur J Vasc Endovasc Surg Vol 31, 2 2006

F. Verzini et al.138
The endograft removed was the AneuRx device in sixcases and Talent in the remaining three.
Causes for early conversion were:
(1) extensive vessel calcification (NZ7) leading toproximal graft migration during deployment,mechanical deployment failure or impossibilityof device progression,
(2) aortic neck rupture (NZ1),(3) failed catheterisation of the contralateral limb
(NZ1).
All early conversions were carried out with amidline trans-peritoneal approach. In seven patientsaortic cross-clamping below the renal arteries wasused, one patient required supra-renal clamping andanother patient supra-celiac clamping. A tube graftwas placed in seven cases. In one patient an aorto-
Table 2. Details and causes of late conversion to open repair in 29 pa
Case N AAA pre-oper-ative diameter(mm)
AAA diam-eter at con-version (mm)
Type ofdevice
Secondaprocedubefore O
1 44 44 AneuRx No
2 51 52 AneuRx No
3 52 57 AneuRx Prox cu
4 51 42 Anaconda No5 72 81 AneuRx No6 55 55 Talent Iliac cuf7 45 60 AneuRx Prox cu
8 78 80 AneuRx No9 46 46 Anaconda No10 40 35 AneuRx No11 50 48 Anaconda No12 60 65 Excluder No13 50 59 AneuRx Prox cu
14 70 80 Excluder No15 42 38 AneuRx No16 45 49 AneuRx No17 52 46 Anaconda No18 77 85 AneuRx No19 77 88 Talent No20 70 92 Aneurx No21 43 56 Aneurx No
22 50 58 Talent No23 48 53 Aneurx No24 73 100 Talent No
25 46 45 Endologix No26 40 53 AneuRx No27 52 46 AneuRx No28 52 84 AneuRx No
29 50 57 Aneurx Prox cu
AND= aortic neck dilatation; Migr= distal migration; Type I–III= type
Eur J Vasc Endovasc Surg Vol 31, 2 2006
femoral by-pass was needed for iliac dissection,secondary to the endovascular attempts; the remain-ing patient had a bifurcated graft to the iliac arteries.Median blood loss was 1837 ml (range 1000–3500 ml,excluding the aortic rupture case where blood losswas 10,000 mlc). All patients were transferred tointensive care unit, with a median stay of 20 h(range 6–24 h).
Two patients died peri-operatively (22%), one formultiple organ failure after massive bleedingsecondary to aortic rupture and the other formyocardial infarction after reoperation for acute limbischemia. Three non-fatal major complicationsoccurred (33%), one myocardial infarction, oneabdominal wall dehiscence requiring re-operationand prolonged hospitalisation, and one post-operativebleeding requiring surgical exploration. Median post-operative hospital stay was 12 days (range 5–27 days).
tients
ryreR
Elapsed timefrom EVAR toOR (months)
Indications for conver-sions
Intraopera-tive findings
23 MigrCANDCsecond-ary type I
Confirmed
16 MigrCANDCsecond-ary type ICback pain
Confirmed
ff 27 ANDCtype IICAAAgrowth
Confirmed
6 ANDCMigrCKinking Confirmed23 AAA growth Hygroma
f 22 Type III Microleakff 41 AAA ruptureCsecond-
ary type IIIConfirmed
30 AAA growthCtype II Confirmed13 MigrCAND Confirmed45 MigrCsecondary type I Confirmed16 MigrCAND Confirmed32 AAA growthCtype II Confirmed
ff 46 AAA growthCsecond-ary type III
Confirmed
23 AAA growth Hygroma38 Migr Confirmed43 AAA growthCAND Confirmed23 ANDCMigr Confirmed32 AAA growth Microleak33 AAA growth Microleak56 AAA ruptureCtype I Confirmed27 ANDCMigrCAAA
growthConfirmed
46 ANDCAAA growth Confirmed75 AAA growthCMigr Confirmed32 AAA ruptureCAAA
growthCANDCMigrCsecondary type I
Confirmed
26 MigrCtype I Confirmed74 ANDCAAA growth Confirmed73 ANDCMigr Confirmed62 AAA growthCANDC
MigrCseondary type IConfirmed
ff 82 AAA growthCtype III ConfirmedCfabric tear
of endoloeak.

Conversion After Endovascular Repair of Aortic Aneurysm 139
Late conversion
Late conversions were necessary in 29 patients. Detailsand causes are indicated in Table 2. During the sameinterval 79 patients underwent one or more secondaryendovascular reinterventions for EVAR complications.In 72 patients, the secondary procedures wereaccomplished successfully, with benefit persisting inthe long-term. The remaining seven patients requiredlate conversion to OR. Median interval from primaryendovascular procedure to secondary OR was 33months (range 7–85 months). Median AAA diameterat the time of endografting for these patients was52 mm (range 40–78 mm), while median aortic diam-eter at the time of conversion was 60 mm (range35–100 mm).
Four of the 29 patients required urgent surgery forrupture (NZ3) or acute occurrence (NZ1) of second-ary type I endoleak leading to impending rupture. Ofthe three patients treated for rupture, one hadpreviously refused a planned secondary interventionfor migration of the proximal graft, another did notcomply with the imaging follow-up protocol and after3 years presented a ruptured AAA secondary to graftmigration, the third patient experienced acute type IIIendoleak for disconnection between the proximal cuffand the main body of the graft.
Of the entire cohort of 649 EVAR, three otherpatients presented with ruptured aneurysm at otherhospitals, where they did not undergo any surgicaltreatment. These three patients were not included inthe present cohort of 29 late conversions. Overall, therewere six ruptures during EVAR follow-up.
The remaining 25 late conversions were elective. Avariety of endografts were explanted: 18 AneuRx, 4Anaconda, 4 Talent, 2 Gore e 1 Endologix (Table 2).Four of these conversions were carried out in otherhospitals and the retrieved data were cumulated in thesame database.
Table 3. Risk factors in 634 patients with and without late conversio
Conversion
Yes (NZ29) No (NZ605)
Gender (female) 4 (14%) 36Age (R80 years) 2 94ASA IV score 0 111Proximal neck length%15 mm
3 (%) 61 (%)
Proximal neckdiameter R26 mm
2 (%) 66 (%)
Neck angulation O608 4 (%) 22 (%)AAA diameterR55 mm
9 (%) 200 (%)
Infrararenal fixation 25 (%) 479 (%)EUROSTAR class D/E 2 (%) 164 (%)
Surgical access was obtained in 24 cases through amidline trans-peritoneal approach and in five with aleft retro-peritoneal incision. Intra-operative findingsdid not confirm the pre-operative indication in sixpatients who presented growing AAA due to causes(three microleaks, one fabric tear and two hygromas)different from those suspected, or not detected at thepre-operative CT scan. The other causes of graft failurewere accurately detected by pre-operative imaging(Table 2). Only one out of three patients with microleakwas on anticoagulant therapy (for atrial fibrillation).
Aortic cross-clamping was suprarenal in 12 casesand infrarenal in the remaining 16 cases. Completeremoval of the endograft was possible in all but twocases. In one patient the supra-renal stent of the Talentgraft was left in place, using a wire cutter to removethe covered portion of the endograft, while in theother an AneuRx iliac extension was not removed.Aorto-iliac reconstruction was performed in 23patients; aorto-femoral in four, aorto-aortic in one.Median intra-operative estimated blood loss was2200 ml (range 100–7000 ml); 18 patients requiredblood transfusion (median 3 units, range 1–8 units).Median intensive care stay was 24 h (0–72 h). Post-operative median hospital stay was 6 days (4–7 days).There was no mortality at 30 days either in elective orin urgent surgery for late conversion. The majormorbidity rate (non-fatal) was 20.7%, with two casesof pneumonia, one case of atrial fibrillation, one case ofworsening renal failure and one post-operativebleeding requiring transfusion.
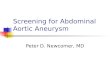
Risk of conversion during follow-up is shown inFig. 1, the risk of late conversion after EVAR was 9% at6 years (Kaplan–Meier estimate). After this point, therewere too few patients to allow meaningful evaluation.Median follow-up after conversion was 27 months(range 1–60 months). Two patients died of causesunrelated to their AAA, one from stroke at 3 monthsand one from myocardial infarction at 27 months after
n (Univariate analysis)
OR 95% CI p
0.4 0.13–1.2 0.100.4 0.09–1.7 0.29– – 0.0050.9 0.29–3.3 1
0.6 0.14–2.6 0.76
4.2 1.35–13.2 0.030.9 0.41–2.0 1
1.6 0.56–4.8 0.50.2 0.04–0.84 0.02
Eur J Vasc Endovasc Surg Vol 31, 2 2006

Fig. 1. Conversion rate after EVAR in 649 patient (Kaplan–Meier).
F. Verzini et al.140
conversion. One case of inguinal infection requiringfemoral limb graft in situ replacement occurred duringfollow-up; no other late complications secondary toOR occurred in any of the converted patients. Multi-variate analysis failed to identify any factor associatedwith late conversion. Risk factors in patients with andwithout conversion are shown in (Table 3).
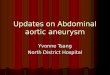
Fig. 2. CT scan 82 months after EVAR showing type IIIendoleak.
Discussion
Our results confirm that early conversion after EVARis a rare event (1.4%) but carries a high operative risk(22% peri-operative mortality rate) mainly due to thelength of the procedure and the possibility ofassociated vascular injuries. The single and fatal caseof aortic rupture occurred at the bottom of a conicalangulated neck, during deployment of the endograft.In all other patients, challenging iliac anatomy withsevere vessel calcifications was the primary cause ofunsuccessful deployment. These findings suggest thatpatients should not be considered for EVAR when, atthe pre-operative CT imaging, the iliac arteries appearto be severely calcified and angulated. Alternatively,an iliac conduit may be used from the beginning of theendovascular procedure to avoid iliac dissection orrupture after repetitive forceful introduction of largesize introducer devices.
The rate of early conversion, with attendantincrease of operative risk, can be reduced withtechnical improvements and better patient selection.A thorough anatomical evaluation of the access vesselsas well as the aortic neck is crucial to ascertain patientsuitability for EVAR and avoid unsuccessful deploy-ment. Obviously, less stringent anatomical criteria
Eur J Vasc Endovasc Surg Vol 31, 2 2006
may be used in elderly, high-risk patients with largeAAA. Under these circumstances the acceptable risk ofpossible late endograft failure, manageable with asecondary endovascular re-intervention, alwaysshould be balanced against the risk of an unsuccessfuldeployment highly harmful in this subset of patients.
Late conversions after EVAR were more frequent(9% at 6 years, Kaplan–Meier estimate) but were notassociated with peri-operative mortality in the presentcohort. OR is believed to be a ‘hazardous procedure’after a failed EVAR, as stated by May et al. whoreported a mortality rate as high as 17%.9 Thiscontrasts with our experience, where there was noperi-operative mortality in the 29 patients undergoinglate OR.
Stringent patient follow-up after EVAR and accu-rate analysis of any morphological or structuralchange over the time may reduce the risk of acuteonset of complications with the following need ofurgent open conversion, to allow safer scheduling ofelective OR when needed. The incidence of lateconversion after EVAR is reported widely in theliterature, ranging from 4 to 50% and is dependenton centre experience, type of graft used, length offollow-up and compliance with follow-up protocols.1,
2,5,8–14 The EUROSTAR registry reported a cumulativeconversion risk of 2.1% per year, statistically associ-ated with type I–III endoleak, graft migration and graftkinking.14 This risk seems to be reduced withcontemporary results and grafts. In the recentlypublished EVAR 1 trial mid-term results, crude rateof conversion to OR, at an average follow-up of 3.3

Conversion After Endovascular Repair of Aortic Aneurysm 141
years, was 2.6%. Comparison with our results isdifficult because of differences in the length offollow-up and methodology (in the EVAR 1 trialconversion rate was measured as a crude rate, and thefollow-up was shorter).1
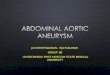
It is not surprising that, as in our cohort, the risk ofconversion from primary EVAR increases with time(Fig. 1). For the same reason, most of the lateconversions involved the AneuRx endograft, sincethis model was used predominantly in the earlyexperience at our centre and therefore contributedheavily to long-term follow up and presumablycontributed most to the learning curve. Interestingly,the patient with the oldest EVAR implant requiringconversion had a sudden onset of type III endoleak at82 months due to a large size fabric tear, as shown inFigs. 2 and 3. This was the only case of clinicallyrelevant structural failure in our cohort other than
Fig. 3. Explanted endograft showing l
three cases of microleak due to suture holes, probablypresent since the time of implant. It also is noteworthythat in 6 of 29 patients requiring conversion the causesof graft failure were not identified pre-operatively andunexpected findings were discovered intra-opera-tively (Table 2).
The endovascular approach was routinely con-sidered first-line treatment in late endograft failure.However, in almost 10% (7/79) of cases, in spite ofearly success of the secondary endovascular pro-cedures, patients required conversion to OR later infollow-up. Progressive AAA growth without signs ofmorphological, structural or haemodynamic failure atCT/ultrasound or X-ray imaging was interpreted asthe most reliable indicator of the need for conversion.Consequently, when there is no evident cause foraneurysm growth and the patient has an acceptablesurgical risk, elective surgical conversion is considered
arge size fabric tear in the left limb.
Eur J Vasc Endovasc Surg Vol 31, 2 2006

F. Verzini et al.142
a valuable first option. It is possible that thisaggressive strategy, together with the increasedawareness of our EVAR patients and practitioners torefer immediately any sudden onset of symptoms toour centre, may have had a beneficial effect onreducing the number of urgent cases requiringconversion to OR.
Surprisingly, at multivariate analysis we could notfind any single factor associated with late failure. Allfactors widely believed to influence adversely EVARoutcome, such as AAA diameter, proximal neckdiameter, length or angulation, extensive iliac aneur-ysmal involvement, infrarenal/suprarenal fixationendograft, were not significantly associated with riskof late conversion. Perhaps the decision for conversionis the conclusion of a complex decision-makingprocess based on multiple co-existing adverse factorsoccurring at different follow-up intervals.
In cases of AAA rupture, some authors report arelatively low post-operative mortality and havepostulated that the presence of an endograft exertssome protection and haematoma confinement. Incontrast, Bernhard et al. reported an overall mortalityrate of 50% following AAA rupture post-endograftingwith the Guidant devices.15 Our three cases ofruptured AAA underwent immediate CT scan,followed by prompt conversion to OR, with a veryshort delay from the onset of symptoms, hadstraightforward infrarenal aortic cross-clamping andexperienced no major complications. Our absence ofmortality after ruptured AAA is potentially biased byexclusion of the three fatalities in patients referred toother hospitals, who died without undergoing oper-ation. Perhaps those were the most critical patientsand intervention was denied because of their criticalcondition, associated with the advanced age of thepatients (78, 80 and 83 years). If we included thesethree patients with rupture who died without repair,our mortality for ruptured AAA after endograftingwould have risen to 50%.
In conclusion, early open conversion frequently isdue to severe vessel calcifications and has high peri-operative mortality. Recognition of this should preventthe endovascular specialist from forcing morphologi-cal indications for primary EVAR. The risk ofconversion after abdominal aortic endografting is notnegligible, affecting almost one out of 10 patientssurviving 6 years. No single anatomical factor wasassociated with an increased risk of late failure. Thesedata suggest that, at present, a more relaxed long-termfollow-up schedule after endoluminal repair cannot bejustified. In cases of aneurysm growth (without signsof morphological, structural or haemodynamic failure)either after primary EVAR or a subsequent failed
Eur J Vasc Endovasc Surg Vol 31, 2 2006
endovascular reintervention, an aggressive attitudefor OR in patients fit for open surgery permitsadequate planning for conversion and yields to resultsnot inferior to those of primary open aneurysm repair.
References
1 EVAR Trial participants. Endovascular aneurysm repair versusopen repair in patients with abdominal aortic aneurysm (EVARtrial 1): randomised controlled trial. Lancet 2005;365:2179–2186.
2 Blankensteijn JD, de Jong SE, Prinssen M, van der Ham AC,Buth J, van Sterkenburg SM et al. Two-year outcomes afterconventional or endovascular repair of abdominal aorticaneurysms. N Engl J Med 2005;352:2398–2405.
3 Cao P, Verzini F, Parlani G, Romano L, De Rango P,Pagliuca V et al. Clinical effect of abdominal aortic aneurysmendografting: 7-year concurrent comparison with open repair.J Vasc Surg 2004;40:841–848.
4 Goueffic Y, Becquemin JP, Desgranges P, Kobeiter H. Midtermsurvival after endovascular versus open repair of infrarenalaortic aneurysms. J Endovasc Ther 2005;12:47–57.
5 Van Marrewijk CJ, Fransen G, Laheij, Harris PL, Buth J and forthe Eurostar Collaborators. Is a type II endoleak after EVAR aharbinger of risk? Causes and outcome of open conversion andaneurysm rupture during follow-up. J Vasc Endovasc Surg 2004;27:128–37.
6 Cao P, Verzini F, Zannetti S, De Rango P, Parlani G,Lupattelli L et al. Device migration after endoluminalabdominal aortic aneurysm repair: analysis of 113 caseswith a minimum follow-up period of 2 years. J Vasc Surg 2002;35:229–235.
7 Beebe HG, Cronenwett JL, Katzen BT, Brewster DC,Green RM, Vanguard Endograft Trial Investigators. Results ofan aortic endograft trial: impact of device failure beyond 12months. J Vasc Surg 2001;33:S55–S63.
8 Dattilo LB, Brewster DC, Fan CM, Geller SC, Cambria RP,Lamuraglia GM et al. Clinical failures of endovascularabdominal aortic aneurysm repair: incidence, causes, andmanagement. J Vasc Surg 2002;35:1137–1144.
9 May Y, White GH, Yu W, Waugh R, Stephen M, Sieunarine Ket al. Conversion from endoluminal to open repair of abdominalaortic aneurysm. A hazardous procedure. Eur J Vasc EndovascSurg 1997;14:4–11.
10 Bockler D, Probst T, Weber H, Raithel D. Surgical conversionafter endovascular grafting for abdominal aortic aneurysms.J Endovasc Ther 2002;9:111–118.
11 Terramani TT, Chaikof EL, Rayan SS et al. Secondaryconversion due to failed endovascular abdominal aortic aneur-ysm repair. J Vasc Surg 2003;38:473–478.
12 Jacobowitz GR, Lee AM, Riles TS. Immediate and lateexplantation of endovascular aortic grafts: the endovasculartechnologies experience. J Vasc Surg 1999;29:309–316.
13 Walschot LH, Laheij RJ, Verbeek AL. Outcome after endovas-cular abdominal aortic aneurysm repair: a meta-analysis.J Endovasc Ther 2002;9:82–89.
14 Harris PL, Vallabhaneni SR, Desagranges P, Becquemin JP,VAN MARREWIJK C, Laheij RJ. Incidence and risk factors of laterupture, conversion, and death after endovascular repair ofinfrarenal aortic aneurysms: the EUROSTAR experience. Euro-pean Collaborators on Stent/graft techniques for aortic aneur-ysm repair. J Vasc Surg 2000;32:739–749.
15 Bernhard VM, Mitchell RS, Matsumura JS, Brewster DC,Decker M, Lamparello P et al. Ruptured abdominalaortic aneurysm after endovascular repair. J Vasc Surg 2002;35:1155–1162.
Accepted 29 September 2005