Embed Size (px)
Citation preview

Documenta Ophthalmologica 58, 45-50 (1984}. �9 Dr 141. Junk Publishers, The Hague. Printed in the Netherlands.
Cont ra s t sensi t ivi ty d i f fe rences b e t w e e n s t rab i smic and
a n i s o m e t r o p i c a m b l y o p i a : ob jec t ive cor re la te b y m e a n s of visual evoke d responses
EMILIO C. CAMPOS, MARIA LUISA PRAMPOLINI and ROZANNA GULLI
Pediatric Ophthalmology and Strabismus Service, Department of Ophthalmology, University of Modena, Modena, Italy
Key words: amblyopia, strabismus, anisometropia, contrast sensitivity, modulation, transfer function, visual evoked responses
Abstract. The visual evoked response transfer function of amblyopic subjects was studied. Strabismic amblyopes showed abnormalities only in the high spatial frequency range. Anisometropic amblyopes on the contrary, showed an abnormal function both in the low and high spatial frequency range. This is an objective correlate of functional differences between strabismic and anisometropic amblyopes.
Introduction
Animal neurophysiological studies and clinical evidence (yon Noorden, 1977, 1983) consider functional amblyopia as a syndrome, with common caracter- istics, independently from its cause. Thus, visual deprivation, anisometropic and strabismic amblyopia have been generally included in the same group. However, these types of amblyopia respond differently to treatment. More- over, different subjects with a clinically diagnosed identical form of ambly- opia (in terms of severity, age of onset, beginning of treatment, etc.) may behave in dissimilar ways. A differentiation of amblyopias in various classes seems therefore tempting.
The Cambridge Physiological Insitute Group (Campbell, 1974) has shown that contrast sensitivity provides in normals more refined information on visual functions than conventional visual acuity testing. Based on this assump- tion Hess et al. (1979, 1980) were able to show that strabismic and anisome- tropic amblyopes exhibit different contrast sensitivity functions when convenient illumination is used. The first type of patients shows only a high spatial frequency cut-off, whereas the second one is caracterized both by low and high spatial frequencies abnormalities. Campbell and Mallei (1970) showed that the pattern visual evoked responses (VER) amplitude of normals is proportional to the logarithm of the stimulus contrast and has been also shown to correlate well with the magnitude of perceived contrast (Fiorentini and Mallei, 1972).
The aim of this paper is to report on our experiments in which pattern VER for various spatial frequencies were recorded in strabismic and anisome- tropic amblyopes and differences between the two groups have been found.
46
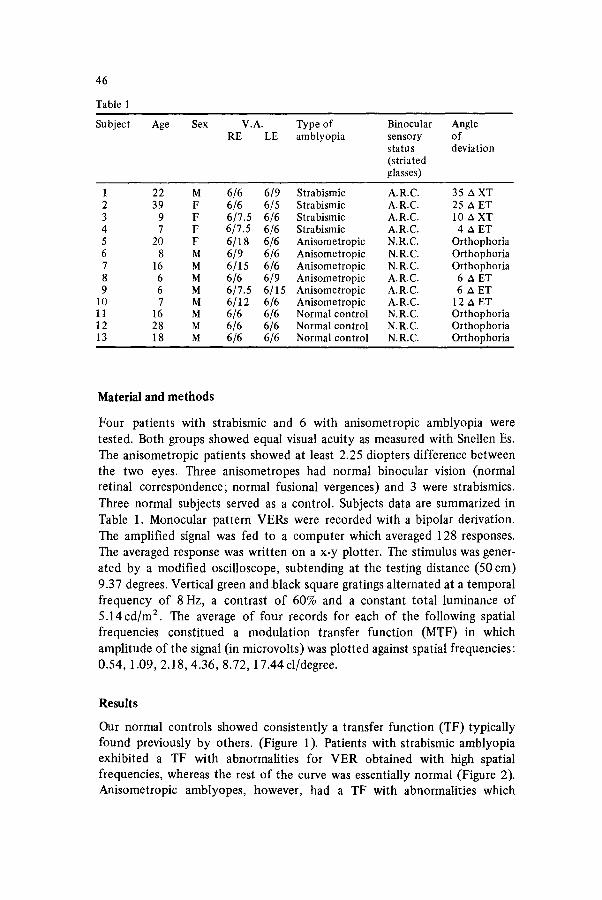
Table 1
Subject Age Sex V.A. RE LE
Type of Binocular Angle amblyopia sensory of
status deviation (striated glasses)
1 22 M 6/6 6/9 Strabismic A.R.C. 35 A XT 2 39 F 6/6 6/5 Strabismic A.R.C. 25 A ET 3 9 F 6/7.5 6/6 Strabismic A.R.C. 10 A XT 4 7 F 6/7.5 6/6 Strabismic A.R.C. 4 A ET 5 20 F 6/18 6/6 Anisometropic N . R . C . Orthophoria 6 8 M 6/9 6/6 Anisometropic N . R . C . Orthophoria 7 16 M 6/15 6/6 Anisometropic N . R . C . Orthophoria 8 6 M 6/6 6/9 Anisometropic A.R.C. 6 A ET 9 6 M 6/7.5 6/15 Anisometropic A.R.C. 6 A ET
10 7 M 6/12 6/6 Anisometropic A.R.C. 12 A ET 11 16 M 6/6 6/6 Normal control N . R . C . Orthophoria 12 28 M 6/6 6/6 Normal control N . R . C . Orthophoria 13 18 M 6/6 6/6 Normal control N . R . C . Orthophoria
Material and methods
Four patients with strabismic and 6 with anisometropic amblyopia were tested. Both groups showed equal visual acuity as measured with Snellen Es. The anisometropic patients showed at least 2.25 diopters difference between the two eyes. Three anisometropes had normal binocular vision (normal retinal correspondence; normal fusional vergences) and 3 were strabismics. Three normal subjects served as a control. Subjects data are summarized in Table 1. Monocular pattern VERs were recorded with a bipolar derivation. The amplified signal was fed to a computer which averaged 128 responses. The averaged response was written on a x-y plotter. The stimulus was gener- ated by a modified oscilloscope, subtending at the testing distance (50 cm) 9.37 degrees. Vertical green and black square gratings alternated at a temporal frequency of 8 Hz, a contrast o f 60% and a constant total luminance of 5 .14cd/m ~. The average of four records for each of the following spatial frequencies constitued a modulation transfer function (MTF) in which amplitude of the signal (in microvolts) was plotted against spatial frequencies: 0.54, 1.09, 2.18, 4.36, 8.72, 17.44 cl/degree.
Results
Our normal controls showed consistently a transfer function (TF) typically found previously by others. (Figure 1). Patients with strabismic amblyopia exhibited a TF with abnormalities for VER obtained with high spatial frequencies, whereas the rest of the curve was essentially normal (Figure 2). Anisometropic amblyopes, however, had a TF with abnormalities which

A (~v) o
16
12
.~. r ight eye
.....~ lef t e y e
. " i I %.~,
,~ I
, . . . \ I I . : l , .. , \ , .s
- \
- \
47
| | m i | |
0,84 2,18 8,74 $.F (r
Figure 1. Abscissa: spatial frequency; ordinate: VER amplitude in microvolts. Transfer function of a normal subject.
A (pv) n o r m a l eye 0
16 a m b l y o p i c eye
12
�9 �9 o~ ~ ~ . ~
I , ..9,
"~ ~ '0~ .0
| i i i |
0,54 2,18 8,74 S.F (cla)
Figure 2. VER transfer function of a patient with strabismic amblyopia. Abnormalities are present only in the high spatial frequency range.
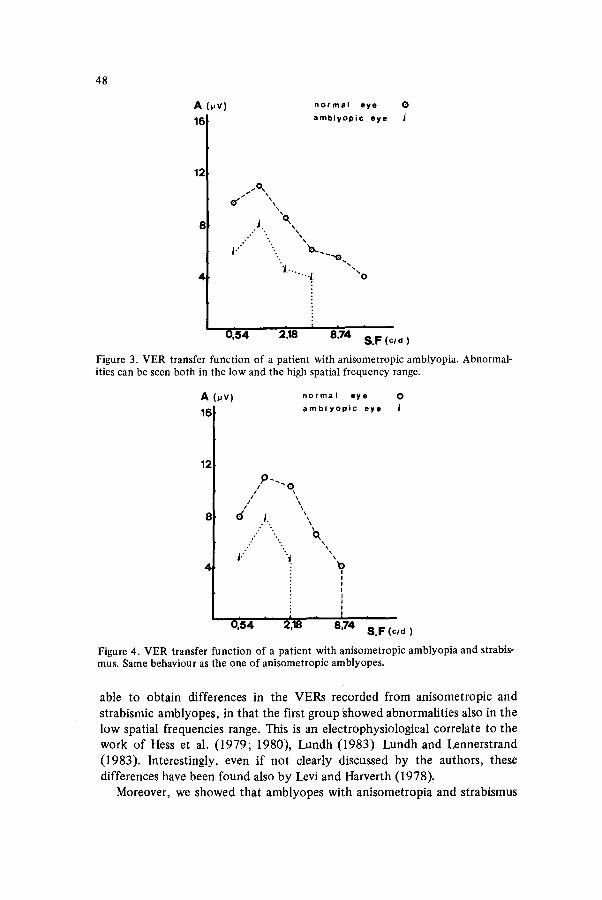
involved both the high and the low spatial frequency region (Figure 3). More- over, amblyopes with anisometropia and strabismus behaved as anisometropic amblyopes (Figure 4).
Discussion and conclusion
Our results confirm the high-frequency cut-off in the TF obtained with pattern VERs, which is typical of this condition. Moreover, we have been
48
A (~,v) 16
12
4
normal eye O
amblyopic eye
~. 'o ~ x
l : ' .. "o...,
'i ........ i ""O
| i | | |
0,54 2,18 8,74 S.F (cln)
Figure 3. VER transfer function of a patient with anisometropic amblyopia. Abnormal- ities can be seen both in the low and the high spatial frequency range.
A 0JV) n o r m a l eye O
16 a m b l y o p i c eye J
12 ~ ) ~
d,
| 0,84
.
"O
i i
2,18 8,74 S.F (cld)
Figure 4. VER transfer function of a patient with anisometropic amblyopia and strabis- mus. Same behaviour as the one of anisometropic amblyopes.
able to obtain differences in the VERs recorded from anisometropic and strabismic amblyopes, in that the first group showed abnormalit ies also in the low spatial frequencies range. This is an electrophysiological correlate to the work of Hess et al. (1979; 1980), Lundh (1983 ) Lundh and Lennerstrand (1983). Interestingly, even if not clearly discussed by the authors, these differences have been found also by Levi and Harverth (1978).
Moreover, we showed that amblyopes with anisometropia and strabismus

49
behave as anisometropic amblyopes do. In fact, in these patients anisome- tropic amblyopia may be considered as the cause of strabismus, because it makes probably motor fusion uneffective. Hess (1981) has pointed out that the contrast threshold abnormalitites found in amblyopia are an expression of neural disfunction. The latter obvi- ously shows different characteristics in anisometropic and strabismic ambly- opia. However, it cannot be yet excluded that the different behaviour of strabismic and anisometropic amblyopes is due to the aniseikonic effect present in the second group (Bradley and Freeman, 1981).
A more extended analysis of amblyopic patients is needed, particularly during the plastic period of the visual system, in order to follow in time changes which may occur in the MTF in course of treatment. This can be done using VER techniques.
Visual acuity and contrast sensitivity tested during treatment in children of unspecified age (Howell et al.~ 1983) or in the final part of the plastic period (Lundh and Lennerstrand, 1983) do not show a parallel behaviour. Hopefully VER recordings at an early age may cast some light on the differential functional prognosis of amblyopic patients. It will thus be poss- ible to devide in sub-classes the various types of amblyopia, according to the response to treatment of various MTF components. In fact, it has to be stressed that visual acuity testing relates only to high frequency bands, whereas contrast sensitivity allows to gather information also in the low and middle frequency ranges. Sensitivity changes in these ranges affect heavily the visual function producing important deficits in the picture quality, orientation and motion perception (Leibowitz et al., 1980) otherwise
undetectable.
References
Bradley A and Freeman RD (1981) Contrast sensitivity in anisometropic amblyopia. Invest Ophthalmol Visual Sci 21:467
Campbell FW (1974) The transmission of spatial information through the visual system. In: The Neurosciences Third Study Program. FO Schmitt and FG Worden (eds). Cambridge, Mass., MIT Press, pp 95-103
Campbell FW and Maffei L (1970) Electrophysiological evidence for the existence of orientation and size detectors in the human visual system. J Physiol 20:263
Fiorentini A snd Maffei L (1972) Suprathreshold contrast perception and its electro- physiological correlate. Optica Acta 190:363
Gstalder RJ and Green DG (1971) Laser interferometric acuity in amblyopia. J Pediatric Ophthalmol 8:251
Hess RF (1981) Application of contrast-sensitivity techniques to the study of functional amblyopia. In: Clinical Applications of Visual Phsychophysics. LM Proenza, JM Enoch and A Jampolsky (eds). Cambridge, Cambridge University Press, pp 11
Hess RF, Campbell FW and Zimmern R (1980) Differences in the neural basis of human amblyopias: the effect of mean luminance. Vision Res 20:295
Hess RF, Zimmern R and Campbell FW (1979) Do anisometropic and Strabismic ambly- opia have different neural bases? Suppl Invest Ophthalmol Vis Sci April 1979, p 139

50
Howell ER, Mithchell DE and Keith CG (1983) Contrast thresholds for sine gratings of children with amblyopia. Invest Ophthalmol Vis Sci 24:782
Leibowitz H, Post R and Ginsburg A (1980) The role of fine detail in visually controlled behaviour. Invest Ophthalmol Vis Sci 19:846
Levi DM and Harwerth RS (1977) Spatio-temporal interactions in anisometropic and strabismic amblyopia. Invest Ophthalmol Vis Sci 16:90
Levi DM and Harwerth RS (1978) Contrast evoked potentials in strabismic and anisome- tropic amblyopia. Invest Ophthalmol Vis Sci 17:571
Lundh BL (1983) CLinical contrast sensitivity. Methodolical aspects. Link6ping Univer- sity Medical Dissertations 144:1
Lundh BL and Lennerstrand G (1983) Effects of amblyopia therapy on contrast sensi- tivity as reflected in the visuogram. Acta Ophthalmo161:431
Noorden GK yon (1977) Mechanism of amblyopia. Adv Ophthal 34:93 Noorden GK yon (1983) Practical management of amblyopia. Int Ophthalmol 6:7 Sj6sstrand J (1981) Contrast sensitivity in children with strabismic and anisometropic
amblyopia. A study of the effect of treatment. Acta Ophthalmo159:25