Embed Size (px)
Citation preview

CONGENITAL VESICAL NECK OBSTRUCTION IN A FEMALE CHILD DUE TO CUP,VALVE FORMATION: OPEN OPERATION:
COMPLETE RECOVERY *
AUGUSTUS HARRIS, M.D., P.A.C.S.
BROOKLYN, N. Y.
P ATIENT E. B., aged five years, femaIe, was admitted to the Long IsIand CoIIege HospitaI on March 24, 1930, compIaining
She was weak, fussy and irritabIe, with moderate fever, more or Iess, everyday, accom- panied with some abdomina1 pain. These
FIG. I. Radiograph with opaque catheters in situ (March, 1930).
of pains in the back and abdomen, headache, intermittent fever and pus in the urine.
Family History: Mother had active tuber- culosis, requiring two therapeutic abortions in earIy married Iife. A grandmother had tuber- culosis and an aunt died of tubercuIosis.
Previous History: ChiId was weaned at the age of three and one haIf months on account of mother’s poor heaIth. Patient had never reaIIy been we11 since birth, in spite of specia1 atten- tion to diet and carefu1 hygienic supervision. Three years ago she was ill for three months with abscessed cervical gIands foIIowing whoop- ing cough.
FIG. 2. DoubIe UreteropyeIograms (March, 1930) show- ing doubIe hydro-uretero-nephrosis.
attacks would recur every few months, and, no doubt, were due to urinary obstruction. Of Iate, the attacks of backache and abdomina1 pain, especiaIIy on the right side, had been getting more frequent and more severe. Pains wouId occur for a few hours each day for a few days and then wouId subside after a few days. For three weeks the pain had been more severe, starting in the back and radiating to the ffank and abdomen. The mother stated that the chiId wouId throw herself on the fioor during severe attacks. In view of previous history and known pyuria, it is evident that, at that time, a uroseptic condition existed and was overIooked
* From the Department of Urology, Long Island CoIlege HospitaI.
64

FIG. 3. Cystogram (March, 1930) showing diIated bIad- FIG. 4. Cystogram (July, 1930) showing diIated bIadder der and reflux into both ureters and peIves. (Right but no manifest ureteral reffux. ureter incompIeteIy outlined.)
FIG. 5. Uroselectan (JuIy, 1930) fifteen minutes, FIG. 6. UroseIectan (July, 1930) thirty minutes, no shows good eIimination of right kidney, with no visua1 appearance from Ieft kidney. eIimination from Ieft.
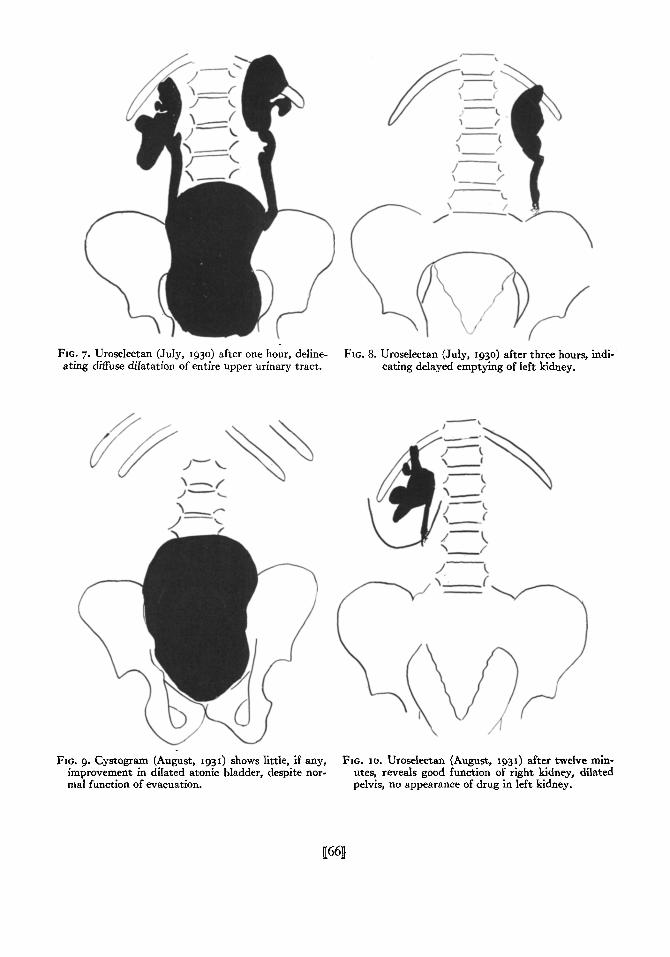
FIG. 7. Uroselectan (July, 1530) after one hour, deline- ating diffuse dilatation of entire upper urinary tract.
FIG. 8. UroseIectan (Juiy, 1930) after three hours, indi- cating delayed emptying of Ieft kidney.
FIG. 9. cystogram (August, 1931) shows little, if any, FIG. IO. Uroseiectan (August, 1931) after tweIve min- improvement in diIated atonic bIadder, despite nor- utes, reveals good function of right kidney, dilated ma1 function of evacuation. pelvis, no appearance of drug in left kidney.
uwl

NEW SERIES VOL. XX. No. I Harris-VesicaI Neck Obstruction American Journal of Surgery 67
because of the other cIinica1 manifestations. There was no history of hematuria, dysuria, vomiting, or convulsions.
F‘lc. II. Uroselectan (August, 1931) after two hours, reveals hydro-uretero-nephrosis and dilated bladder simiIar to that of a year ago preceding operation. (CompIete recovery, however, from residua1 urine and pyuria.)
Physical examination showed some enlarge- ment of the cervicat gIands. There were no lesions found in the heart or lungs. AbdominaI examination was negative, except for some tenderness on deep pressure over the right kidney. Reflexes were normal. The provisional pediatric diagnosis on admission was congenital abnormality of the right kidney or right renaI tuberculosis. The tubercuIin test was strongly positive. Nothing was found in the sinuses, ears, nose or throat to expIain the febriIe condition. UrinaIysis aIways showed a hundred or more pus ceIIs to the fieId and blood examination showed Ieucocytosis and negative Wassermann reaction.
Cystocopy March 27, 1930, performed by a colleague, showed a diIated bIadder with dilated ureters and renaI pelves, with B. coIi infection of bIadder and both kidneys. The
cystogram also showed uretera reflux. Tubercle bacilli were never found in the urine. The blood chemistry revealed definite nitrogen retention.
FIG. 12. Bladder showing cup-vaIve formation at vesi- cal outlet. Dotted Iine indicates line of incision used in operative procedure.
Gastrointestinal series of radiographs were negative. At this time cystotomy was advised, but it was finaIIy decided to try expectant treatment, incIuding a regime of rest and strict hygiene, this treatment to include bIadder irrigations and careful supervision.
Readmission. She was re-admitted to the hospita1 on JuIy 7, 1930 for compIete study, having improved considerab1y and having gained 9% pounds in weight since the last admission. At this time uroseIectan study, incIuding cysto- gram, showed no change in the genitourinary findings. In spite of these data, conservative treatment was carried out and the chiId aIIowed to go home under the same regime.
Third Admission to Hospital. She first came under my observation on September 4, 1930,
when she was admitted for the third time, with recurrence of pains in the back and side, and showing persistence of pyuria and with Iarge amount of residua1 urine. However, she had gained 3 pounds in weight since Ieaving the hospita1. In view of the recurrence of more severe symptoms, I advised open operation. The increased nitrogen retention and urosepsis

68 American Journal of Surgery Harris-VesicaI Neck Obstruction APRIL, 1933
required reIief from the vesica1 neck obstruc- the wound heaIed, moderate pyuria and a tion, which was evident. A second cytoscopic residua1 urine of about 2 ounces. examination was not deemed advisable. The Under the carefu1 supervision of a pediat-
FIG. 13. FIG. 14. FIG. 15.
FIG. 13. Cup-fold of mucous membrane held upward with forceps. FIG. 14. Raw surface exposed after resection of redundant membrane.
FIG. 15. CIosure of raw surface by interrupted sutures passed in opposite direction.
first cytoscopic examination had faiIed to visuaIize the vaIve condition, probabIy because the cytoscope caused the membrane to flatten out against the vesica1 mucosa. The preopera- tive diagnosis was, therefore, stenosis or fibrosis of the vesica1 neck.
Operation. After preIiminary bIadder drain- age and irrigation, cystotomy was performed on September 8, 1930. The bIadder was markedIy thickened but with very IittIe trabecuIation and no diverticuIum. We then exposed a cup- Iike, elevated, rather Iarge foId of redundant mucous membrane with the concavity upward, Iying transversely just behind the interna urethra and acting as a perfect cup-valve, shutting off the vesica1 outIet. This was care- fuIIy and compIeteIy resected, incIuding a portion of adjacent overstretched, redundant, and thickened mucous membrane on the fIoor of the bIadder. There was a moderate-sized fossa formation just posterior to the vaIve. The raw surface remaining was cIosed with interrupted, fine catgut sutures carrying the suture Iine in the opposite direction, to give Iength to, and funneIize the outIet. Su- prapubic tube drainage was provided in the usua1 manner.
ConvaIescence was satisfactory but some- what sIow. The phenoIsuIphonphthaIein and bIood chemistry tests showed a steady and continued improvement in function and the patient Ieft the hospita1 October 16, 1930, with
rician, at her home in the country, she gained very rapidIy and has apparentIy fuIIy recovered from her Iong-standing iIIness. There is no pyuria at present, no residua1 urine and the bIood chemistry is normaI. She attends schoo1 reguIarIy. She contracted infantiIe paraIysis during the 1931 epidemic, and recovered quickIy from this disease without compIica- tions. Intravenous urography, done about a year after operation, faiIed to show much im- provement in the evident diIation of the bIadder, ureters and peIves. (AI1 urograms showed deIayed function of the Ieft kidney, both before and after operation.) Despite the Iarge size of the bIadder, however, it is now emptying itseIf compIeteIy.
COMMENT
In conditions of diIated bIadder in infants and chiIdren, with or without diverticuIa, nerve and cord Iesions, urethra1 stricture and meata obstruction having been ruIed out, the urgent need for carefu1 instrumenta study of the vesica1 neck region and posterior urethra is apparent. I beIieve the true etioIogy wiI1 thereby be more frequentIy demonstrated, and re- moved before advanced disease changes have taken pIace; furthermore “idiopathic

NEW SERIES VOL. XX, No. I Harris-VesicaI Neck Obstruction American JUWI of surgery 69
dilatation” of the bladder wiII Iess often CampbeII reports a recent case of be the accepted diagnosis. trigonal curtain behind the vesica1 outIet
In congenita1 obstructive cases, the in a femaIe child of fifteen months. This degree of obstruction is naturaIly the case is in a measure somewhat simiIar, determining factor in the severity of but not the same Iesion. The effects symptoms, and in bringing the patient to a produced by the Iesion, however, are aI- correct diagnosis at an earher period of Iife. most identica1.
With the popuIarization of cysto-ure- I wish to express my sincere thanks to throscopic study in chiIdren, more vesica1 Dr. D. E. Overton of the Pediatric De- neck lesions are being demonstrated. A partment for his assistance and interest, number of vaIve formations in maIe chiI- and for the shadow-tracings of radiographs. dren associated with the embryoIogica1 defects of the verumontanum and hyper- trophied frenuIa are recorded. The Iatter REFERENCES
condition does not appIy in the case herewith presented.
I. YOUNG, FRONTZ and BALDWIN. J. Ural., 3: 289-365.
So far as I am aware, this is the first 1919.
2. BUGBEE, H. G., and WALLSTEIN. J. Ural., IO: 477-
case of congenita1 vaIve obstruction at 49% 1923.
the vesica1 neck in a femaIe chiId to be 3. KRETSCHMER, H. L. Surg. Gynec. Obst., 53: 129.
reported in the Iiterature. 193'.
4. CAMPBELL, M. F. J. U-ok, 27: 157-163, 1932.