Embed Size (px)
DESCRIPTION
Tulburari la varstanici.
Citation preview

ComorbiditiesPub-Med search with comorbidity 115.826 records
Michael Davidson MD
(multi-morbidities, complications, disease burden, patient complexities, frailty)

Content• Definition(s) and general comments
• Dementia and medical comorbidities
• Depression, apathy and medical comorbidities
• Psychosis and medical comorbidities
• More comments

Questions to you• First physician that psychiatrist ?• The reverse ?• Who is the case manager of your patient? • What do you know about the relationship between
your elderly patient and her offspring?• Silly questions ?• Is the benefit/risk ratio of psychotropics in young and
elderly the same? • Do you treat with psychotropics a depressed, agitated,
slightly cognitively impaired elderly who is already on 8 medications?

The Definition of comorbidity is:
1. “Any distinct additional clinical entity that has existed or may occur during the course of a patient who has the INDEX disease under study
2. A medical condition existing simultaneously but independently with another condition in a patient
3. A medical condition in a patient that causes, is caused by, or is otherwise related to another condition in the same patient
4. All of the above

What statement regarding comorbidity among mental illnesses is not true?
1. The large number of psychiatric comorbidities is due to splitting into distinct categories which do not exist in nature
2. The term comorbidities apply rather to medical-psychiatric or medical-medical condition than to psychiatric-psychiatric conditions
3. Narrow distinction into discrete diseases severs daily clinical practice
4. Patients can easily meet criteria for 2-3 mental disorders

Which of the following is more likely to determine what is the index illness and what is
the comorbidity?
1. The relative importance of the co-occurring condition(s)
2. The chronology of presentation of the conditions3. The research question 4. The disease that prompted a particular episode of
care(hospitalization) 5. The specialty of the attending physician


Types of comorbidities
• Chance– CHF (dyspnea) and osteoarthritis leading to poor
mobility• Selection bias
– People who seek care have more comorbidities than the general population
• Causal association– CHF and venous peripheral edema leading to
poor mobility



Which of the following is not a contributor to comorbidities
1. Socio-economical status 2. Education 3. Age 4. Type of health care system (private, public or
mixed)

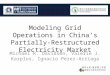
Percentage with more than one condition by age and sex
18-24 25-34 35-44 45-54 55-64 65-74 75-84 85+0
5
10
15
20
25
30
35
40
45
50
MALE
FEMALE
Age-group
%
> 50% of the elderly have >3 medical comorbidities

Epidemiology of multimorbidity
• Among the 65 years old 2/3 have >2 chronic conditions, and 1/3 have >4
• The age of multimorbidity onset is lower by 10 among the low income populations
• Arthritis and heart disease coexist in 20% of older adults
• The odds of developing disability from arthritis or heart disease is x4 by each condition separately but the risk for disability increases 14-fold if both are present



Content
• Definition(s)• Dementia with medical comorbidities• Depression, apathy and medical
comorbidities• Psychotic illnesses and medical
comorbidities

Dementia
• Falls• Epilepsy• Weight loss and/or malnutrition• Poor reporting of “alarm
sensations” pain, nausea• Incontinence • Disruption of sleep/wake cycle• Depression/Apathy
Aging
• Frailty• Hypertension • Ischemic cardiovascular
disease• Metabolic and endocrine
(diabetes, thyroid)• Malignancies• Bone, Muscular• Skin• Sensory
Comorbidities in elderly demented are mostly related to dementia or to aging?


What is not true about falls in the elderly demented?
1. The most likely reasons for falls in demented elderly are abnormal gait and muscle weakness
2. Only 5% of the falls result in fractures3. Rehabilitations is made difficult by the
cognitive impairment 4. Fractures affect survival

Etiology of falls
• Accidents / environment 37%• Weakness, balance, gait 12%• Dizziness or vertigo 8%• Orthostatic hypotension 5%• Acute illness, medications, vision
18%• Unknown 8%
Rubenstein et al JAGS 1988

Changes in Bone Mass Density with age
Peak bone density
Puberty
Menopause
Osteopenia
Osteoporosis
Age


Incidence of all-limb fractures
0-4 5-14 15-24
25-34
35-44
45-54
55-64
65-74
75-84
85+0
100
200
300
400
500
Rate
per
100
,000
pop
ulati
on
FallsFr 5%

Survival probability with and without fracture
Time to follow-up (year)
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Cum
mul
ativ
e su
rviv
al p
ropo
rtio
n
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Non-fracture
Any fracture
B Men
Time to follow-up (year)
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Cum
mul
ativ
e su
rviv
al p
ropo
rtio
n
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Non-fracture
Any fracture
A Women

Where are elderly likely to fall?
Home 60%* Public Places 30%
Nursing Home 10%**
*Most falls happen to women in their homes in the afternoon **Falls in nursing homes occur during the first week after admission and tends to result in injury. Higher use of psychotropic drugs have been associated with risk of falling.

Which statement is not true regarding
epilepsy in dementia
1. 5% to 10% of demented individuals have seizure which is X 6 normal population
2. Epilepsy is more prevalent in early rather than late onset dementia
3. Incidence is higher in patients with vascular compared to AD
4. Treatment of seizure in elderly demented is as effective as it is in non-demented individuals

Which statement is not true regarding dementia, malnutrition and weight loss?
1. Demented patients are likely to lose 10-15 % of their weight during the course of the disease
2. Serum albumin is a good marker of malnutrition 3. A large number of medications might impair appetite4. Gastrostomy is the accepted solution in end stage
dementia to prevent malnutrition and aspiration

Drugs that can cause anorexia
• digoxin• phenytoin• SSRI’s / lithium• Ca++ channel blockers• H2 receptor antagonists /
PPIs• Any chemotherapy• metronidazole
• narcotic analgesics• K+ supplements• furosemide• ipratropium bromide• theophylline• spironolactone• levodopa• fluoxetine
More than 250 medications reportedly disturb gustatory sensationMore than 40 drugs reportedly disturb the sense of olfaction

What is not true regarding urinary incontinence in dementia
1. Loss of cognitive ability to interpret the sensation of a full bladder
2. Inability to plan how to self-toilet. 3. Occurs earlier in vascular dementia, dementia with
Lewy bodies and FTD than in Alzheimer’s disease4. The majority of the patients with a MMSE <18 are
incontinent

Hints to assess pain in dementia
• Facial expression• Bracing (clutching or holding onto furniture,
equipment)• Rubbing (massaging affected area)• Restlessness and agitation• Verbal vocal complaints such as “ouch” or “stop”• Sympathetic arousal

Which statement is true about demented patients ?
1. RCT found antidepressant effective in treating depressed mood
2. RCT found antipsychotics effective in treating psychosis
3. RCT found amphetamine-like drugs effective in treating apathy
4. All of the above



Why do we prescribe drugs with poor benefit/risk ration?

Content
• Definition(s)• Dementia with medical comorbidities• Depression, apathy and medical
comorbidities• Psychotic illnesses and medical
comorbidities

Prevalence of Depressive Disorders in Various Patient Populations*
* There is a range of percentages depending on the study.
Prevalence
General population
Chronically ill
Geriatric inpatients
Cancer outpatients
Cancer inpatients
Stroke
MI
Parkinson’s disease 39.0%
45.0%
47.0%
42.0%
33.0%
36.0%
33.0%
9.4%
5.8%
0% 10% 20% 30% 40% 50%
Adapted from WPA/PTD Educational Program on Depressive Disorders
Hospitalized

Which of the following statement has not been proven
1. Depression can be the presenting symptoms of several somatic diseases
2. Depression is associated with decreased self-care and adherence to medical regimens
3. Direction of causality (presence of depression increases mortality due to medical condition)
4. Of all patients with Cardiovascular Diseases (CVD) 40 % have depressive symptoms and 20% MDD
Katon. Gen Hosp Psychiatry. 1996;18:215.

What is not true regarding depression and CVD
1. There is an OR of 1.6 for developing CVD in those who are depressed
2. Depression increases risk for death Post-MI OR 2.5
3. Depression increases risk for death post-bypass and angioplasty
4. Antidepressant drugs are effective in depression associated with CVD

SADHEART Trial
• 369 patients with MDD, mean HAM-D=19.6• 74% had an MI; 26% had unstable angina• RCT sertraline (50-200mg) vs placebo for 24
weeks • No significant difference in MI, re-
hospitalization, death or HAM-D scores

The explanation for the Depression-CVD association is?
1. Life style choices (e.g. smoking, exercise, diet) and non-compliance with medication
2. Hyperactivity of HPA axis (cortisol, CRF, NE)3. Autonomic nervous system dysregulation
resulting in BP and HR abnormal variations 4. Non of the above

Pain in the elderly depressed
• 1/3 elderly in the community and 1/2 in nursing homes report pain
• 20% above 65 are taking pain medications • 31% of women & 19% of men > 75 years report pain
in 3 or more sites • Pain makes recognition of depression more difficult
and treatment less successful• Depression makes recognition and treatment of pain
more difficult
CDC s National Center for Health Statistics 2006,′

What is true regarding pain and ageing
1. Some degree of pain is “natural” with aging
2. Pain medication should be limited since elderly are vulnerable to addiction to pain medications
3. Pain is under-reported due to sensory and cognitive impairments
4. All of the above

Depression and apathy in the elderly
• Components of apathy:– Decreased goal directed activity– Lack of motivation – Indifference to previously emotionally exciting experiences
• Nosology:– Apathy– Abulia– Negative symptoms

Is the phenomenology the same and are the
underlying mechanism the same?

Epidemiology Average point prevalence, cortical 60% Sub-cortical 40%
Variability between studies up to 100%

The reason for the variability in prevalence of apathy is
1. Population studied2. Threshold for severity3. Scale used and rater training 4. All of the above

How Homogenous an Entity is Apathy ?
What is involved? • Neurotransmitters • Focal lesion (stroke) or diffuse
lesion (AD)?• Cortical or (frontal lobe
dementia) or basal ganglia (Huntington)?
• Abnormal circuits or local lesion (Fronto-sub-cortical circuit lesion)?
• Personality• Life events
Which neurotransmitter(s)?• Ach: awakening, motivation
and attention• NA: motivation, novelty
seeking and resistance to distraction
• DA: motivation and reward• GABA: interacts and
modulates Ach, NE, DA

Depression vs Apathy the overlap

Should apathy be treated pharmacologically?
• No– Patient does not complain– No direct danger to self or others– It rarely reflects the core disease– AE– Cost
• Yes– Patient maybe suffering?– Caregiver burden and frustration– Potential to improve functionality
• Amphetamines, DA agonists, ChEI, Memantine, MAOI, TCA, SSRI, NSRI?

Content
• Definition(s)• Dementia and medical
comorbidities• Depression, apathy and medical
comorbidities• Psychotic illnesses and medical
comorbidities

The increased prevalence of CVD in chronic psychotic patients (schizophrenia, schizoaffective, bipolar) compared
to controls is due to:
1. Long-term administration of antipsychotics and other psychotropics
2. Over-diagnosis of CVD in this population3. Inadequate access to treatment 4. Poor life style habits (smoking, exercise, weight)5. Inadequate selection of the control group

Final considerations

Complexities • 79-year-old woman with hypertension, diabetes , osteoporosis,
osteoarthritis, COPD and depressed mood is caring for her 80 year old husband affected by severe dementia with behavioral disturbances
• The hypothetical woman patient would need to take 13 medications ( $ 600 per month) and follow 14 recommendations)
• CDC report, 37 percent of older Americans use five or more prescription drugs
• Patient with five chronic conditions would result in the prescription of 19 doses of 12 different drugs, taken at five time points during the day, and carrying the risk of 10 attendant interactions or adverse events

What is the main knowledge gap in making treatment decisions on psychotropic treatment in elderly with comorbidities
• Paucity of EBM for older adults with multimorbidity.• Finding a balance between poor life expectancy, and
QL during the remaining years• Unpredictable variability in pharmacokinetics • The fact that psychotropics have been developed and
proven effective in young and middle age healthy individuals not in elderly, many of whom are affected by brain degenerative diseases


Optometrist
Medical Buracracy
Acute ward
Income
Outpatient
General Practicioner
Specialist
General hospital
Crisis
Alcohol & Drugs
Rehab
Day hospital
Disparate entities (based on profession, jurisdiction and function) that communicate but are not “integrated”
AO = Assertive Outreach
Social Services
The Maze

What to do when the ramp becomes too stiff?

The role of the psychiatrist in the care of the elderly psychiatric/demented patient
with medical comorbidities
• Specialist/consultant
• Primary care physician
• Care coordinator


Age-dependent success
3 years: not wetting your pants10 having friends18 having a driver’s license20 having sex35 having money50 having money60 having sex70 having a driver’s license75 having friends80 not wetting your pants
“Age is not a particularly interesting subject; anyone can get old. All you have to do is live long enough.” - Groucho Marx
Getting old is not so bad, considering the alternative.” Maurice Chevalier