Embed Size (px)
Citation preview

Community Integrated Paramedicine (CIP) Fact vs. Fiction.
Where we are in Michigan

CONTACT INFORMATION
Kristine Kuhl, Paramedic, I/C, BA, MACommunity Integrated Paramedicine CoordinatorDivision of EMS and TraumaBureau of EMS, Trauma and PreparednessMichigan Department of Health and Human Services
Office: 517-241-4304Mobile: 517-582-5155
Michigan Emergency Medical Services System website

OBJECTIVES
Describe the structure of Community Integrated
Paramedicine (CIP) in Michigan
Explain why other program models across the country
will not necessarily work in Michigan.
List two benefits an EMS agency and their personnel may
experience from a CIP program
Be able to make a statement for and a statement against
Community Integrated Paramedicine in Michigan
FACT FICTION?
In Michigan, a paramedic license allows you to work in a
variety of places such as hospitals or urgent cares.
FACT FICTION?
EMS is part of public health

Public
HealthBETP
EMS & Trauma
Kathy Wahl
Linda Scott
Trauma
EMS
Sabrina
Kerr
Preparedness
Director Gordon
Dr. Joneigh Khaldun

FACT FICTION?
Only an EMS agency can be approved as Community
Paramedicine program.

FACT FICTION?
There is a huge cost to start a Community Paramedicine program

REINVENTING THE WHEEL?
Q: Why can’t we just copy successful programs from other states? Why reinvent the wheel?
This Photo by Unknown Author is licensed under CC BY
A: Difference in regulatory structure
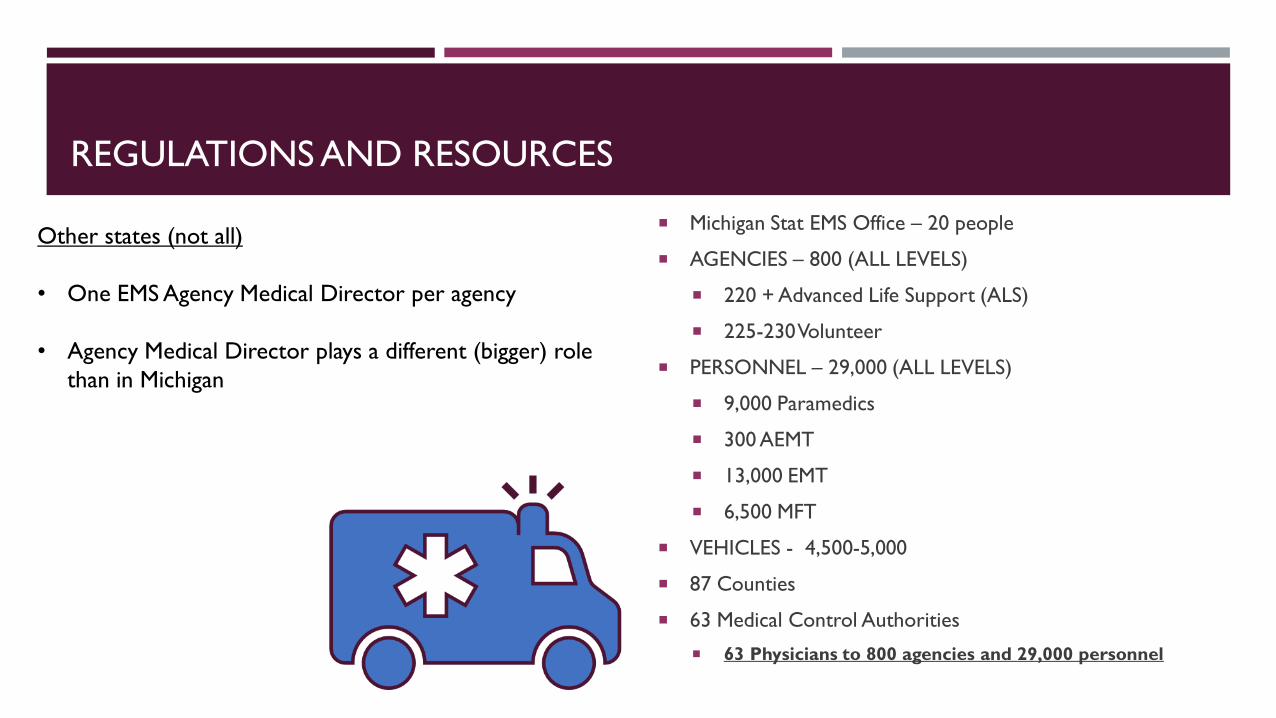
REGULATIONS AND RESOURCES
Michigan Stat EMS Office – 20 people
AGENCIES – 800 (ALL LEVELS)
220 + Advanced Life Support (ALS)
225-230 Volunteer
PERSONNEL – 29,000 (ALL LEVELS)
9,000 Paramedics
300 AEMT
13,000 EMT
6,500 MFT
VEHICLES - 4,500-5,000
87 Counties
63 Medical Control Authorities
63 Physicians to 800 agencies and 29,000 personnel
Other states (not all)
• One EMS Agency Medical Director per agency
• Agency Medical Director plays a different (bigger) role
than in Michigan

MICHIGAN: PLAN & IMPLEMENT
Education
Protocols
Replication
Data
Regulation
Sustainability

THIS MIGHT NOT FIT
Retrieved from: https://www.reddit.com/r/funny/comments/8n0f4y/pretty_sure_thats_not_gonna_fit_bro/

ON FURTHER ANALYSIS…
Language
Education
Standardize and must match a scope of practice
define a scope of practice
Protocols
Standardize (must fit with education & scope)
Replication
Will need standardization of above things first
Data
EMS documentation is for acute care – can’t define elements until we have defined their scope
Regulation
All above in place first
Sustainability
Dependent on regulation

Retrieved from: https://images.app.goo.gl/xme7EgtCzbTRj5Cd7Retrieved from: https://images.app.goo.gl/yFZEM3FDuBfj3rr58

#1 LANGUAGE
COMMUNITY INTEGRATED PARAMEDICINE
Mobile Integrated Health
CHW
Community Paramedicine
EMS
Nurse
Social Worker Physical Therapy
Health Plan
Physician
Dietitian
May not even include EMS
Somewhat of a closed system Heavy on bidirectional referrals
PCP CHWLHDCardiac
Rehab

#2 SCOPE AND ROLE
#2.5 STANDARDIZED EDUCATION
Scope and Role Workgroup: hospital physicians, MCA physicians, EMS providers, CPs,
hospitals
Current MI programs, national programs, wish list
Curriculum Workgroup: Educators, ICs, CPs, hospital
Created objectives for the scope
Place objectives in some semblance of order
Standardized minimum curriculum

#3 PROGRAM REPLICATION
CURRENT PROCESS - Special Study Application PA 368
Application Guide
FUTURE PROCESS
Regulated & assimilated into the EMS system

#4 PROTOCOL SUITE
Correspond with scope and curriculum
Standardized
3 Categories within the suite of protocols: CIP Protocols Table of Contents & Adoption Status
Program protocols (system) – ADOPT ALL
Procedure protocols – Flexible – Plug and play
Approved procedure protocols
Treatment/Population – Flexible – Plug and play
CIP Patient General Assessment and Care
Populations
Complaints

#5 DATA
EMS documentation is not geared toward MIH/CP care
Data collected should be related to the deliverable (scope & role/protocols)
Definitions need to be universal (or at least state-wide)
17 vendors for EMS documentation in the state of Michigan (ESO, Stryker, Zoll, ImageTrend, etc.)
All into ImageTrend (repository)
Mapping and acceptance matter

#6 REGULATORY
Special Study - 3 years – adopt, extend, or reject
Endorse, certify, license
All three pose barriers but licensure appears to be the easiest and the most sustainable route
Allows integration into the EMS system

#7 SUSTAINABILITY
The final piece
Currently – contracts between a program and a payer
Payers know it works and it will save them money
ET3
Statewide partners from MDHHS are interested


LET’S TALK ABOUT
YOUR FEELINGS
Good idea?
Bad idea?
Good use of
resources?
Does it really help
us (EMS)?
This Photo by Unknown Author is licensed under CC BY-NC

POLL QUESTION #1
What is your current stance on Community Paramedicine?
1) Adamantly against it. CP does not belong in EMS at all.
2) I’m on the fence
3) Good idea

NOT NEW
Internationally (Australia, Canada, England, Germany, Ireland, Israel,
Norway, Switzerland)
Some form of community paramedicine or mobile integrated healthcare
established in over half of the states in the U.S.
Early 2000’s
No state reports ‘zero activity’ – everyone is at least exploring it
Most established programs report success (reducing ED utilization,
reducing readmissions, bridging gaps in access to care)
This ship has already set sail regardless of our willingness/unwillingness
to embrace it
This Photo by Unknown Author is licensed under CC BY-NC-ND

WHAT COMMUNITY PARAMEDICINE IS NOT
An answer for everything
A resource available everywhere
Duplication or competition of established services
A good idea for everyone
Being a good EMS provider does not make someone a good CP provider
WHAT COMMUNITY PARAMEDICINE IS
Gap filler
Utilization of an untapped resource (EMS)
More time consuming than an EMS call
Maybe a way to help ourselves

EMS SYSTEM RESOURCES – PART OF OUR ‘WHY’
AGENCIES – 800 (ALL LEVELS)
220 + Advanced Life Support (ALS)
225-230 Volunteer
PERSONNEL – 29,000 (ALL LEVELS)
9,000 Paramedics
300 AEMT
13,000 EMT
6,500 MFT
VEHICLES - 4,500-5,000
87 Counties
63 Medical Control Authorities
63 Physicians to 800 agencies and 29,000 personnel
*2015 Nursing was approximately 1,230 per 100,000 people
Survey of Nurses
*EMS Paramedics are <1 per 100,000 people (approximately 1 per 111,000 people)

Michigan• Population of 10 million
• 83 countiesRural county - 57Metropolitan county containing identified rural census tract(s)Metropolitan county
• Wayne: 1.8 million people/673 square mile = 3,000 people per square mile• IF - 1 ambulances per 5 square miles (15,000 people).
Busy, hospital is likely near, turn around time is short.
• Keweenaw 2,000 people/540 square miles = 4 people per square mile• IF - 1 ambulance per 5 square miles (20 people). No
calls, long transport time – not sustainable. 1 ambulance per 540 square miles – long response, transport and turn around times – also not sustainable.

CHALLENGES
Resources
2 people wear 6 hats
Can’t staff our regular trucks
Access
No public transportation (rural)
The ED is all care
Inclement weather
Time
It take hours to turn a call around
Sitting point for hours is horrible

This Photo by Unknown Author is licensed under CC BY-SA-NC
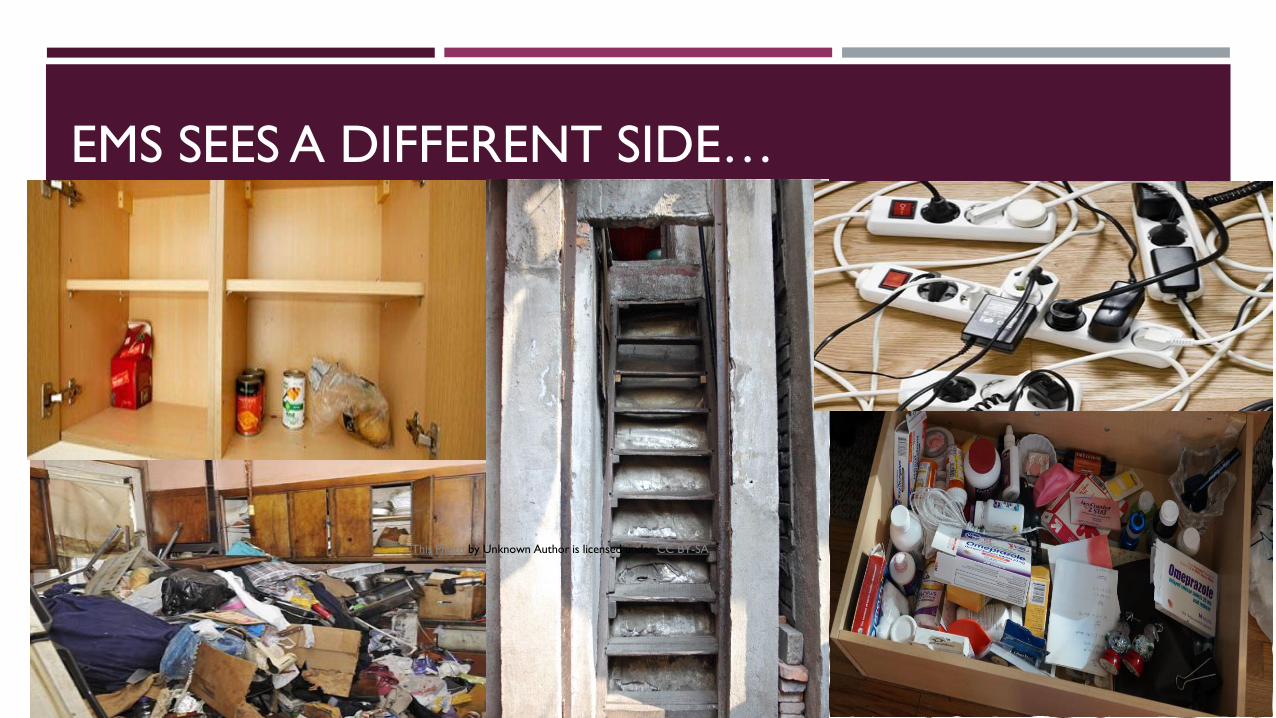
EMS SEES A DIFFERENT SIDE…
This Photo by
Unknown Author is
licensed under CC
BY-SA
This Photo by Unknown Author is licensed under CC BY-SA

MAYBE WE CAN HELP OURSELVES WHILE WE HELP THEM
❑ Think of one patient that was your frequent.
❑ Why were you always there?
❑ Root cause?
❑ Think of one call you ran that was an unnecessary transport.
❑ Could it have been treated on scene?
❑ Treated the next day?
❑ Think of a call that you transported to the ED just to have to turn around to transport back within hours.
❑ What did the ED do?
❑ASK WHY

Procedures
CIP Fall Risk Reduction Assessment CIP SDOH Assessment CIP Medication Audit CIP Feeding Tube CIP Urinary CatheterCIP Nasal PackingCIP Specimen Collection CIP Point of Care Testing for Blood Analysis CIP Suture RemovalCIP PICC Access CIP Vaccinations
Treatment
CIP Diabetic CareCIP Asthma CareCIP Chronic Obstructive Pulmonary Disease CareCIP Congestive Heart Failure CareCIP Chronic Hypertension CareCIP Post MI or Cardiac Intervention CareCIP Post Orthopedic Surgery CareCIP Post Stroke CareCIP Prenatal CareCIP Mom/Baby Postpartum CareCIP Wound CareCIP Substance Use Disorder Care CIP Urinary ComplaintsCIP Gastrointestinal ComplaintsCIP Nontraumatic Nosebleed Complaints
Possibilities
WHAT IS THE REAL COST OF DOING BUSINESS?
Staff, wage, truck, time
Return on Investment (ROI)
I challenge you to think differently about this. (Time on task for non billable services)
Compassion fatigue/burn out
We are human and we are not all built the same
Sitting point/system status management
Utilization vs. me being alseep
IS IT WORTH IT?
CONS
Staffing
Time
Education
Resources
Oversight
Compensation/Sustainability
PROS
Staffing preservation
Time preservation
Resource awareness
Community Engagement
Patient Outcomes
Networks
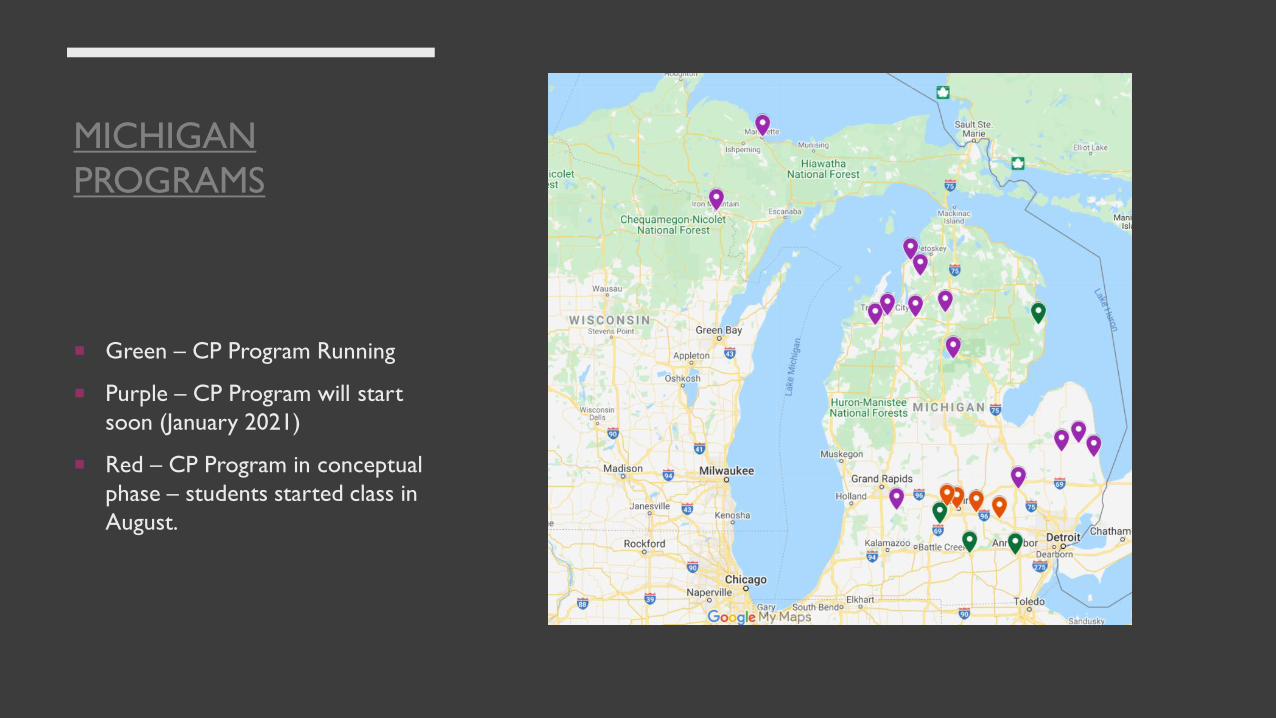
MICHIGAN
PROGRAMS
Green – CP Program Running
Purple – CP Program will start
soon (January 2021)
Red – CP Program in conceptual
phase – students started class in
August.
INFRASTRUCTURE
Documentation and data
HIE
Sustainable Education
Regulatory
Sustainability


CONTACT INFORMATION
Kristine Kuhl, Paramedic, I/C, BA, MACommunity Integrated Paramedicine CoordinatorDivision of EMS and TraumaBureau of EMS, Trauma and PreparednessMichigan Department of Health and Human Services
Office: 517-241-4304Mobile: 517-582-5155
Michigan Emergency Medical Services System website

EMS CONTINUING EDUCATION QUIZ AND EVALUATION
To receive continuing education credits you
must complete the quiz and evaluation within 2
weeks of the webinar here:
https://msu.co1.qualtrics.com/jfe/form/SV_escur
HxbjzAe3hr
Please allow 2-3 weeks for CE distribution to
your email.
You can also find this link in your email.





























