Embed Size (px)
Citation preview

Community Based Group Intervention for Tobacco
Cessation in Rural Tamilnadu: A Cluster Randomized Trial
Dr.M.Santhosh Kumar
Dissertation submitted in partial fulfilment of the requirements for
the award of the degree of Master of Public Health
Achutha Menon Centre for Health Science Studies
Sree Chitra Tirunal Institute for Medical Sciences and Technology
Thiruvananthapuram, Kerala
October 2010

This work is dedicated to my beloved parents Mrs.Sellammal and Mr.Muthusamy
for their untiring efforts to produce this first graduate in the family

Acknowledgements
First I would like to thank Dr.Paul Kumaran, Assistant Director, Tuberculosis
Research Centre, Chennai for showing me the way towards AMCHSS. I would like to
acknowledge Dr.Revathi, Medical officer, Thuvaakudi Primary Health Centre and
Ms.Shanthi, Entomologist, Thanjavur medical college for nurturing my interest in public
health.
I am very much grateful to my guide Prof.K.R.Thankappan for his constant
encouragement and support without whom this trial would be impossible to conduct as part
MPH dissertation. I thank all the faculty members of AMCHSS, Dr.V.Raman Kutty,
Dr.T.K.Sundari Ravindran, Dr.P.Sankara Sarma, Dr.Mala Ramanathan, Dr.K.Srinivasan,
Dr.Manju R Nair and Dr. Biju Soman for their valuable suggestions during the presentations.
I would like to thank the Indian team of Project QTI for their help in designing the
intervention.
I thank all my class mates of MPH 2009 for making these two years most
memorable in my life. My special thanks are to Dr.Aarthy and Dr.Anshul Avijit for their
support during stressful times in the past two years.
I thank the corresponding authors of several articles for sending me the full
text of the articles which helped me to include some of the key references.
I thank my friends Mr.Jothibas MSW, Mr.Selvaraj and Dr.Purushothaman for
their help in preparation for the field work. I thank Mrs.Valli Ramakrishnan for her timely
financial support for this project. I thank Tennur printers, Trichy for their timely delivery of
the booklets and for providing 200 booklets free of cost. I thank Sr.Dr.Rita Adaikalam,
Administrator, Holy Family Hansenorium and the staff members for their support in the
field work.
I thank all the study participants, volunteers and youth club members for
their support during the data collection period. I thank Mr.Sivakumar, Vaadipatti, an active
volunteer for accompanying me to most of the intervention villages.
I am grateful to Dr.Abhay Bhang, SEARCH Gadichiroli and Mr.P.Sainath,
Rural Affairs Editor The Hindu, from whom I have drawn the inspiration to do community
intervention in rural areas.

CCEERRTTIIFFIICCAATTEE
I hereby certify that the work embodied in this dissertation titled
“Community based group intervention for tobacco cessation in
rural Tamilnadu: A cluster randomized trial” is a bonafide record of
original research work undertaken by Dr.M.Santhosh Kumar, in
partial fulfilment of the requirements for the award of the degree of
‘Master of Public Health’, under my guidance and supervision.
Guide
Dr. K. R. Thankappan, MD, MPH
Prof and Head
Achutha Menon Centre for Health Science Studies
Sree Chitra Tirunal Institute for Medical Sciences and Technology
Thiruvananthapuram
October 2010

DDEECCLLAARRAATTIIOONN
I hereby declare that the work embodied in this dissertation work
titled “Community based group intervention for tobacco cessation
in rural Tamilnadu” is the result of original research of mine and
has not been submitted for any degree in any other institution or
university.
Dr.M.Santhosh Kumar
MPH Scholar
Achutha Menon Centre for Health Science Studies
Sree Chitra Tirunal Institute for Medical Sciences and Technology
Thiruvananthapuram
October 2010

TABLE OF CONTENTS
LIST OF TABLES
LIST OF FIGURES
ABSTRACT
CHAPTERS Page No.
Chapter 1 INTRODUCTION AND REVIEW OF LITERATURE
1.1. Introduction.............................................................................................................1
1.2. Review of Literature...............................................................................................1
1.2.1. Global tobacco epidemic............................................................................1
1.2.2. Global trends in tobacco related mortality and morbidity..........................2
1.2.3. Tobacco as a threat to Indian public health system....................................3
1.2.4. Tobacco use in rural India..........................................................................5
1.2.5. Tobacco cessation – A global health priority.............................................5
1.2.6. Benefits of tobacco cessation.....................................................................7
1.2.7. Economic argument for tobacco cessation.................................................8
1.2.8. Tobacco cessation – Part of comprehensive tobacco reduction strategies.8
1.2.9. Tobacco cessation in India..........................................................................9
1.2.10. Group intervention for tobacco cessation..................................................11
1.3. Rationale for the study...........................................................................................12
1.4. Objectives of the study...........................................................................................13
Chapter 2 METHODOLOGY
2.1. Study setting...........................................................................................................14
2.2. Study design...........................................................................................................14

2.3. Sample size............................................................................................................14
2.4. Timeline.................................................................................................................15
2.5. Sample selection procedure...................................................................................15
2.6. Participant flow......................................................................................................16
2.7. Study participants...................................................................................................16
2.8. Field area................................................................................................................17
2.9. Data collection techniques.....................................................................................18
2.10. Blinding..................................................................................................................18
2.11. Ethical considerations............................................................................................18
2.12. Intervention procedures – Intervention arm...........................................................19
2.13. Intervention procedures – Control arm..................................................................26
2.14. Definition of variables............................................................................................26
2.15. Statistical analysis..................................................................................................30
Chapter 3 RESULTS
3.1. Baseline characteristics..........................................................................................31
3.1.1 Socio-demographic profile...........................................................................31
3.1.2 Tobacco use status........................................................................................33
3.1.3 Determinants of tobacco cessation...............................................................34
3.2. Follow up...............................................................................................................35
3.3. Effects on tobacco cessation at two months...........................................................35
3.4. Results of bivariate analysis to identify predictors of abstinence..........................37
3.5. Multivariate analysis (Binary logistic regression).................................................40
3.6. Barriers, facilitators and acceptance of intervention..............................................41

Chapter 4 DISCUSSION AND CONCLUSION
4.1. Discussion..............................................................................................................45
4.1.1. Baseline characteristics.................................................................................46
4.1.2. Effects on tobacco cessation at two months.................................................48
4.1.3. Predictors of abstinence................................................................................49
4.1.4. Tobacco cessation in India: Time for action.................................................50
4.2. Strengths of the study.............................................................................................52
4.3. Limitations of the study..........................................................................................52
4.4. Conclusions............................................................................................................53
4.5. Recommendations..................................................................................................54
REFERENCES
APPENDICES
Appendix I : Participant information sheet
Appendix II : Written informed consent form for the participants
Appendix III : Check list – Eligibility screening form
Appendix IV : Baseline interview schedule
Appendix V : Interview schedule to measure outcome
Appendix VI : Fagerstrom Test for Nicotine Dependence for smokers
Appendix VII : Fagerstrom Test for Nicotine Dependence for smokeless tobacco
Appendix VIII : Intervention tools

LIST OF TABLES AND FIGURES
TABLE
3.1. Socio-demographic characteristics of the participants................................................32
3.2. Tobacco use status of the participants.........................................................................33
3.3. Determinants of tobacco cessation..............................................................................34
3.4. Effects on tobacco cessation at two months using complete case analysis.................36
3.5. Effects on tobacco cessation at two months using intention to treat analysis.............36
3.6. Bivariate analysis to identify predictors of abstinence...............................................38
3.7. Multivariate analysis (Binary logistic regression)......................................................40
3.8. Barriers, facilitators and acceptance of intervention...................................................41
FIGURES
1.1. Projections of global tobacco related mortality in the 21st century...............................2
1.2. Prevalence of tobacco use in India by location and sex................................................3
1.3. Tobacco deaths in the next 50 years under current smoking patterns...........................6
1.4. Cumulative risk of lung cancer mortality in UK males, 1990 rates..............................7
3.1. Geographical location of houses in a village..............................................................42

ABSTRACT
Objective: To determine the efficacy of community based group intervention for tobacco
cessation.
Design: Cluster randomized trial
Setting: Manaparai taluk, Tiruchirappalli district, Tamilnadu, India
Participants: In this trial, 20 clusters with a total of 400 men who were current users of
any form of tobacco between the ages of 20 and 40 years were randomized to two groups
of 10 clusters each.
Intervention: The intervention group received two sessions of health education delivered
five weeks apart by a physician and self help material, with each session lasting for 30
minutes. The control group received only self help material. The content of the
intervention was developed based on the formative research done by the Project Quit
Tobacco International (QTI). Follow up data were available for 366 (91.5%) at two
months.
Main outcome measures: The main outcome was self reported point prevalence
abstinence at two months. Secondary outcomes included quit attempt and reduction of
more than 50% of baseline tobacco use.
Results: More participants quit tobacco at two months in the intervention group
compared to control group: 13.8% Vs 6.5%, adjusted OR 2.86 [95% Confidence Interval
1.23-6.64]. Reduction of > 50% of baseline tobacco use four times higher in the
intervention than the control group [OR 3.69, 95% CI 1.82-7.47]. The number of
participants who made a quit attempt was two times higher in the intervention group than
the control group [OR 2.02, 95% CI 1.15-3.54].
Conclusion: Brief group intervention has the potential to increase the quit rate, quit
attempts and reduction of more than 50% of the tobacco use in the short term among rural
young men. Future research should provide the assessment of long term quit rates.

CHAPTER – 1
INTRODUCTION AND REVIEW OF LITERTURE
1.1. Introduction:
Tobacco use is one of the leading preventable causes of death in the world today.
Tobacco is a risk factor for six of eight leading causes of death in the world. It is an
important risk factor for ischaemic heart disease, cerebro vascular disease, lower
respiratory infections, chronic obstructive pulmonary disease, tuberculosis and cancer of
trachea, bronchus, lungs, mouth and oesophagus. Tobacco kills half of the individuals
who are consuming it.1
The tobacco products are made entirely or partly of leaf tobacco as raw material.
These products are intended to be smoked, snuffed or chewed. All these products have
highly addictive psychoactive ingredient nicotine.1
In early days chewing or smoking
with pipes were the common forms of tobacco use. But use of these forms of tobacco has
declined over a period of time. Now manufactured cigarettes and hand rolled bidis
account for 85% of tobacco consumption in the world. Cigarette smoking can cause more
danger to health than earlier forms of tobacco use.2
1.2. Review of literature:
1.2.1. Global tobacco epidemic:
Globally, 29% of the population aged 15 years and older, or 1.1 billion people
smoke daily, of which 82% live in low and middle income countries. Overall smoking
prevalence was found to be highest in East Asia, the Pacific, Europe and Central Asia
(34%) and lowest in sub-Saharan Africa (18%). Male smoking exceeds female smoking,
with a small gender difference in high income countries. Among females, smoking

prevalence was highest in Latin America (22%) and lowest in South Asia (4%).3 The
smoking prevalence continues to increase in low and middle income countries, whereas
high income countries have shown a declining trend especially among men.4
1.2.2. Global trends in tobacco related mortality and morbidity:
Tobacco has been estimated to cause two to three percent of DALYs (Disability
Adjusted Life years) throughout the world. The massive increase in tobacco consumption
during the last few decades will increase the tobacco related mortality from three million
deaths in 1990 to more than eight million in 2020. DALYs due to tobacco will increase
from 40 million (2.6% of all DALYs in 1990) to 120 million (Nine percent of all DALYs
in 2020) which will make tobacco as the single most important public health problem.5
Another estimate showed that global burden of disease due to tobacco has increased from
2.6% in 1990 to 4.1% of DALYs (59 million DALYs). This increase is due to
accumulated hazards in developing countries.6
Figure 1.1: Projections of global tobacco related mortality in the 21st century
Source: Jha P 2009

An alternate projection of burden of disease showed that mortality due to tobacco
will increase from three million deaths in 1990 to 8.4 million deaths in 2020. In the
developed countries deaths due to tobacco will increase from 1·6 million in 1990 to 2·4
million in 2020. The largest increases in the epidemic of tobacco-related mortality will be
in India, China, and other Asia and islands, where tobacco related deaths will increase
from 1·1 million to 4·2 million by 2020. 7
The global tobacco epidemic is going to threaten the life of one billion people in
this century. So reversing this epidemic is one of the top most priorities in public health.1
1.2.3. Tobacco as a threat to Indian public health system:
Tobacco consumption in India can be divided into smoked and smokeless forms.
The common smoking forms of tobacco are bidis, cigars and cigarettes. The common
smokeless form of tobacco use is tobacco chewing in various forms like pan, pan-masala
or gutkha and mishri.8
Figure 1.2: Prevalence of tobacco use in India by location and sex
Source: NFHS-3

Prevalence estimates from the National Family Health Survey (NFHS-2) showed
that 16% of population smoked tobacco 20% chewed tobacco/pan masala and 30% either
smoked or chewed tobacco.9 According to NFHS -3, 57% of men and 11% of women
used some form of tobacco.10
All forms of tobacco use are increasing in India. An
analysis of two nationally representative surveys NFHS-2 and NFHS-3 showed that the
greatest increase in tobacco use occurred in persons aged 15 to 24 years, in rich castes
and urban areas.11
Global Adult Tobacco Survey-2010 identified India as world‟s second largest
consumer of tobacco. Smokeless tobacco use in India was found to be one of the highest
in the world. The current tobacco use in any form was found to be 47.9% among adult
males. The average age at initiation of tobacco use was 17.8. Five in 10 current smokers
(46.6%) and users of smokeless tobacco (45.2%) planned to quit or at least thought of
quitting in the last year. Among smokers and users of smokeless tobacco who visited a
health care provider, 46.3% of smokers and 26.7% of users of smokeless tobacco were
advised to quit by a health care provider.12
A nationally representative case control study estimated that the number of excess
deaths among adult smokers in the year 2010 will be 930,000 which include 580,000
deaths among men and 90,000 deaths among women between the ages of 30 and 69
years. Because of population growth, the annual number of smoking-associated deaths
among adults will be about one million during the year 2010. Of the million annual
deaths from smoking in India, approximately 70% will occur in middle age, rather than
old age.13
Tobacco related deaths in India are projected to increase from 100,000 deaths
(3.3% of world deaths) in 1990 to 1.5 million deaths (17.9% of world deaths) in 2020. 7

1.2.4. Tobacco use in rural India:
The rural India contributes to the major part of tobacco consumption. Almost 79%
of the tobacco users live in rural areas. The prevalence of both chewing tobacco and
smoking was found to be significantly higher in rural, poorer, uneducated population
when compared to urban, wealthier and more educated population. 9
A study done by Asthma epidemiology study group found that increasing age, low
socio economic status and rural residence as important factors for smoking. Bidi is the
most common form of smoking in rural areas. The average number of bidi/cigarettes
smoked in rural areas is 15 per day. The mean age of starting smoking in rural areas was
found to be 20.1 years.14
According to NFHS-3, 40% of men and three percent of women use some form of
tobacco in Tamilnadu. In rural Tamilnadu, 53.1% of men and 4.3% of women use
tobacco.15
1.2.5. Tobacco cessation- A global health priority
Cessation by current smokers is the only practical way to avoid a substantial
proportion of tobacco deaths worldwide before 2050. Although cessation has become
common in high income countries, it is still rare in most low and middle income
countries. Unless there is a widespread cessation of smoking, 450 million deaths will
occur by 2050.16
Ex-smoking rates are a good measure of cessation at population level. In
developed countries the prevalence of ex-smokers has increased over past three decades.
In UK smoking prevalence among adult men above 30 years has fallen from 70% in 1950
to 30% in 2000. Now more than thirty percent of UK male population comprises of ex-

smokers. Much of this decline was due to smoking cessation interventions. But in
developing countries like India, Vietnam and China the prevalence of ex-smokers among
men were only five percent, 10 percent and two percent respectively.17
The prevention of substantial proportion of tobacco deaths before 2050 requires
adult cessation. Reducing the adult tobacco consumption to half by 2020 will avoid about
180 million deaths. But reducing the percentage of children who start to smoke will
prevent many deaths, but its main effect will be on mortality rates after 2050.16
Figure 1.3: Tobacco deaths in the next 50 years under current smoking patterns
Source: Jha and Chaloupka 2000; Peto and Lopez 2001
Tobacco dependence is a chronic condition that requires repeated intervention.
Effective treatment can produce long term or even permanent abstinence. Brief tobacco
dependence treatment is effective, and every tobacco user should be offered at least brief
treatment.18

1.2.6. Benefits of tobacco cessation:
Existing evidence indicates that tobacco cessation reduces the risk of death from
tobacco related diseases. Smoking cessation at any age is beneficial. The benefits of
smoking cessation were found to be largest in those who quit before middle age, between
ages 25 and 34 years. Cessation before middle age avoids more than 90% of the lung
cancer risk attributable to tobacco, with ex-smoker possessing the pattern of survival
similar to that of persons who have never smoked.19
Figure 1.4: Cumulative risk of lung cancer mortality in UK males, 1990 rates
Source: Peto 2000
More than half of the tuberculosis deaths can be avoided only through smoking
cessation among tuberculosis patients.20
The absolute reduction in mortality due to
cessation of smoking might be even greater for other diseases, particularly vascular
diseases, than for lung cancer in the first decade or two after stopping smoking.15

The only randomized single factor trial to measure the health outcomes of anti-
smoking advice was conducted among 1445 smokers with highest cardio respiratory
scores from Whitehall study. The intervention group received advice on the relation of
smoking to health. During the next 20 years comparing the intervention group with the
control group, total mortality was seven percent lower, fatal coronary heart disease was
13% lower, and lung cancer was 11% lower. The study concluded that smoking cessation
by middle aged men substantially improves their chances of avoiding lung cancer or a
fatal heart attack.21
1.2.7. Economic argument for tobacco cessation:
Direct medical costs of treating tobacco related diseases in India were estimated to
be $907 million for smoked tobacco and $285 million for smokeless tobacco. The indirect
morbidity costs of tobacco use were found to be $398 million for smoked tobacco and
$104 million for smokeless tobacco. The total economic cost of tobacco use amounted to
$1.7 billion. Tuberculosis accounted for 18% of tobacco-related costs ($311million) in
India. The cost of tobacco use was many times more than the expenditures on tobacco
control by the government of India and about 16% more than the total tax revenue from
tobacco. The tobacco-attributable cost of tuberculosis was three times higher than the
expenditure on tuberculosis control in India. Tobacco taxes in India are much lower, so
an increase in tobacco taxes is justified and the money can be used for scaling up the
tobacco cessation services.22
1.2.8. Tobacco cessation - Part of comprehensive tobacco reduction strategies:
The prevalence of tobacco use can be reduced in a population through prevention
of initiation by adolescents and cessation by the current tobacco users.4 The promotion of
tobacco cessation would be more likely to be effective with a comprehensive evidence

based tobacco reduction strategy including school and community based prevention
programs, enforcement of laws restricting sale of tobacco products to minors, restriction
on tobacco advertising and promotion, counter advertising and strong smoke free
policies. Cessation is found to be most effective in a context in which there are strong
restrictions on smoking, tobacco prices are high and tobacco use is not seen as
normative.23
Article 14 of the WHO Framework Convention on Tobacco Control obliges
countries to develop evidence based treatment guidelines and take effective measures to
promote adequate treatment for tobacco dependence.24
1.2.9. Tobacco cessation in India:
India does not have an official government policy or guidelines on tobacco
dependence treatment. India has a tobacco control division in the Ministry of Health &
Family Welfare and a national program on tobacco control which includes treatment for
dependence. In 2001 under a program supported by the Indian government and WHO, 18
Tobacco Cessation Centres (TCCs) were set up in major cities. Since then an additional
12 TCCs have been established, although these are the initiative of respective institutes
and do not have government support. Although there is not yet a national treatment
system, TCCs provide brief advice, intensive behavioural support and medications, and
are developing outreach programs in communities outside the major cities. However, they
still offer very limited access to India‟s population as a whole and are not publicized
widely. TCCs are based in hospitals, regional cancer centres, tuberculosis (TB) centres,
medical and dental colleges and primary health-care centres, and are run by counsellors
trained by WHO under the supervision of doctors. They serve as training and resource
centres for the state, assist in scaling-up treatment services, and also act as advocacy and
resource centres supporting tobacco control legislation at state level. The centres are

involved in training health workers, nurses, doctors and other health professionals and
students.25
Project Quit Tobacco International (QTI) is an attempt to develop culturally
appropriate approaches to tobacco cessation within the health sectors of India and
Indonesia. It is initiated based on the assumption that cessation has the potential to save
millions of lives and health care providers must be at the forefront of the tobacco
cessation efforts to tackle this epidemic. The three aims of the QTI are to design a
tobacco cessation curriculum for medical colleges, develop culturally appropriate
approaches to clinic and community based cessation and to build tobacco cessation
research and training networks within India and Indonesia. As part of their community
based outreach activities smoke free households and work places were promoted.
Promotion of smoke free households was strategically chosen by QTI as a primary
activity in an effort to introduce smoking cessation as a family health initiative, and not
merely a male health priority.26-28
A study carried out in the Vishali district of Bihar used potential volunteer groups
and individuals in the community and trained them to provide cessation activities. The
intervention led to a four percent quit rate (not using the tobacco for more than 12
months), three percent reduction and two percent reduction in multiple habits at the end
of two years. The study concluded that community centered mass approaches with
minimal intervention was cost effective than a clinic centered, intensive and individual
approach.29
1.2.10 Group intervention for tobacco cessation:
Group interventions can help people to learn from each other and can provide
mutual support to stop tobacco use. Cochrane database reviewed sixteen studies which

compared group intervention with self help programs. It was found that quit rates in the
group intervention were higher than the self help programs. The group interventions were
found to be more effective than no intervention.30
Project MYTHRI was a group randomized trial conducted to assess the efficacy
of multi component intervention to prevent tobacco use among Indian adolescents.
Students from 32 schools in Chennai and Delhi were group randomized into intervention
and delayed intervention control groups. This two year school based intervention had four
components which consisted of behavioural component, display of posters, parent
involvement by sending post cards and peer leadership component. After two years the
tobacco use increased by 68% in the control group and decreased by 17% in the
intervention group.31
A demonstration project aimed at reduction of cardiovascular risk factors among
Indian industrial population included avoidance of tobacco as one of the component of
the intervention. The tobacco use dropped from 38.8% to 28.7% in the intervention group
and increased from 17.2% to 19.8% in the control group at the end of four years.32
An intervention study conducted among 36471 tobacco users in rural India to find
out whether quitting tobacco has any effect on the incidence and regression rate of oral
precancerous lesions. The intervention included professional advice from a dentist and
social scientist after screening for leukoplakia and a film show with group discussion.
The percentage of subjects at the end of one year who has given up or reduced tobacco
ranged from three percent in Ernakulam to 21% in Srikakulam.33
Overall tobacco
cessation research, training and coverage are at nascent stage in developing countries like
India and there is a lot of work need to be done to prevent millions of premature deaths.

1.3. Rationale for the study:
In India 79% of tobacco users are living in rural areas. But there are only few
tobacco cessation clinics in cancer centres and tertiary care hospitals. One key issue for
countries beginning their development of treatment services is whether to start with lower
efficacy but broader-reach population approaches, such as brief advice in primary care,
quit lines and wide access to low-cost medications, or more effective but expensive
intensive support delivered through trained specialists, often based in hospitals and
clinics. India introduced specialist clinics at an early stage of the response to tobacco
epidemic. However if only this approach is adopted, coverage will be a critical issue, and
it may work best where the population is smaller and population density is high. Scaling
up such intensive specialist treatment is clearly going to be difficult and expensive in a
huge, diverse country like India.25
The limitations of the clinic approach are that it reaches only a limited number of
predominantly urban and educated tobacco users. In a vast country like India where
reaching the individuals for tobacco cessation may be limited and there is a need to
promote community based methods reaching a wider audience. This has the advantage of
forming spontaneous peer groups within the community, which support an individual‟s
decision to quit.34
Therefore there is a need to develop tobacco cessation techniques
which focus on group and community settings not just individuals.
In India particularly in rural areas tobacco consumption is considered as
normality. So there is an urgent need to bring the tobacco cessation services to their
doorstep and break the social norms which enhance tobacco consumption. There are no
studies from India looking at the efficacy of community based group intervention for

tobacco cessation in rural areas. Therefore this study was undertaken with the following
objectives.
1.4. Objectives:
1) To determine the efficacy of community based group intervention for
tobacco cessation in rural Tamilnadu.
2) To study the facilitators, barriers and acceptance for conducting group
interventions in the rural community.

CHAPTER 2
METHODOLOGY
2.1. Study setting:
The study was conducted in Tiruchirappalli district, Tamilnadu, South India. The
district was administratively divided into 14 community development blocks and eight
taluks. The total number of villages in the district was 479. The total population in this
district was 2,418,366 and the rural population was 1,279,204 (52.9%). The literacy rate
in this district was 77.9% but in rural areas it was only 69.8%.35
Agriculture is the main
occupation in rural areas. Beedi making is one of the important cottage industries in this
district. Cigar industry located in Woraiyur, Tiruchirappalli was a prosperous industry at
one time and cigars made in this industry had good demand in the international market.8
2.2. Study design: Cluster randomized trial
2.3. Sample size:
The sample size was calculated using Epiinfo version 3.5.1.
The sample size was calculated based on the primary outcome quit rate i.e. Point
prevalence abstinence at six weeks. The study was designed to have 80% power at the
five% significance level to detect 15% quit rate at two months after intervention. The
expected quit rate for control arm was two percent.
Ratio (Number of people in the intervention: Number of people in the control arm) was
1:1
Since there are no data available to take into account the effect of intra cluster correlation,
sample size was multiplied by two to account for the design effect.

Total sample size = 344
Sample size was rounded to 400
No. of clusters was 20 and No. of subjects within a cluster was 20
2.4. Time line:
2.5. Sample selection procedure:
Villages are the smallest administrative units in Tamilnadu. In Manaparai taluk,
out of 97 villages, 20 villages were selected based on probability proportional to the size
of the population and randomized equally to intervention and control groups. The
randomization process was done by a person who was not involved in this project. After
randomization it was found that some of the control villages were contiguous with
intervention villages. To avoid contamination adjacent villages that were not contiguous
with the intervention villages were selected as intervention villages. Each village was
considered as a cluster and twenty participants were selected from a cluster.
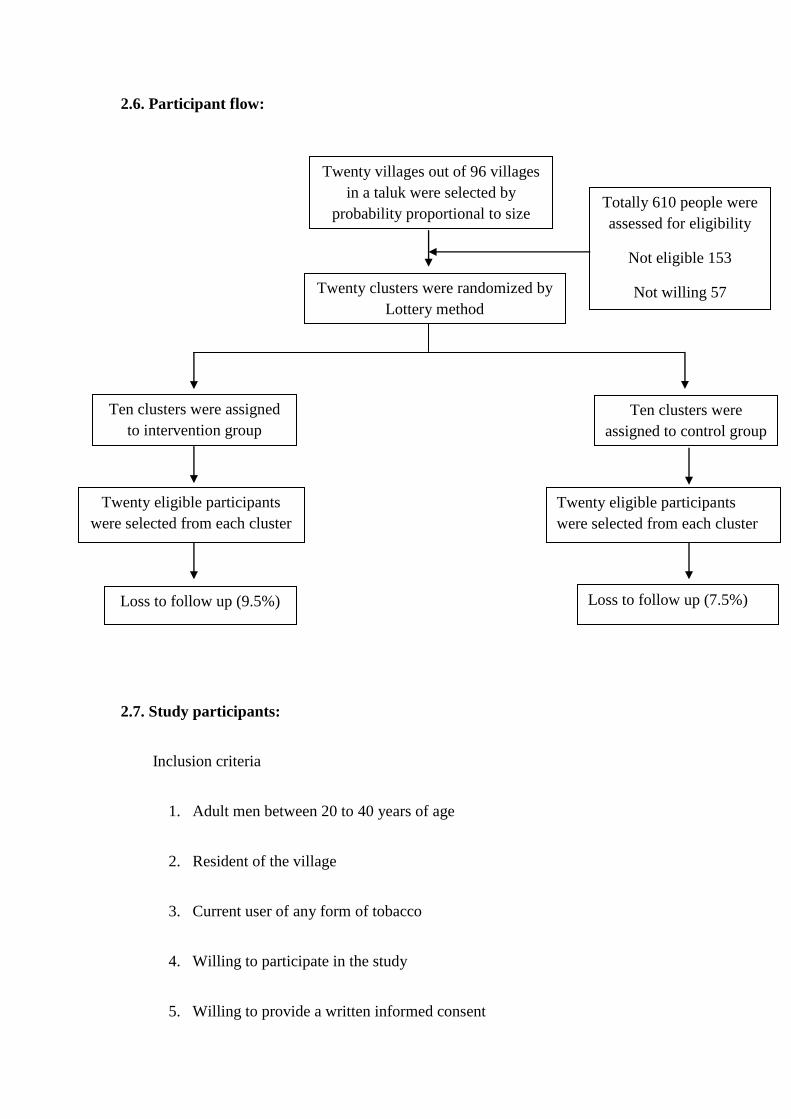
2.6. Participant flow:
2.7. Study participants:
Inclusion criteria
1. Adult men between 20 to 40 years of age
2. Resident of the village
3. Current user of any form of tobacco
4. Willing to participate in the study
5. Willing to provide a written informed consent
Twenty clusters were randomized by
Lottery method
Ten clusters were assigned
to intervention group
Ten clusters were
assigned to control group
Twenty eligible participants
were selected from each cluster
Twenty eligible participants
were selected from each cluster
Loss to follow up (9.5%) Loss to follow up (7.5%)
Twenty villages out of 96 villages
in a taluk were selected by
probability proportional to size
sampling method
Totally 610 people were
assessed for eligibility
Not eligible 153
Not willing 57
Exclusion criteria
1. Bed ridden patients with debilitating illness
2. People who were planning for migration in the next three months
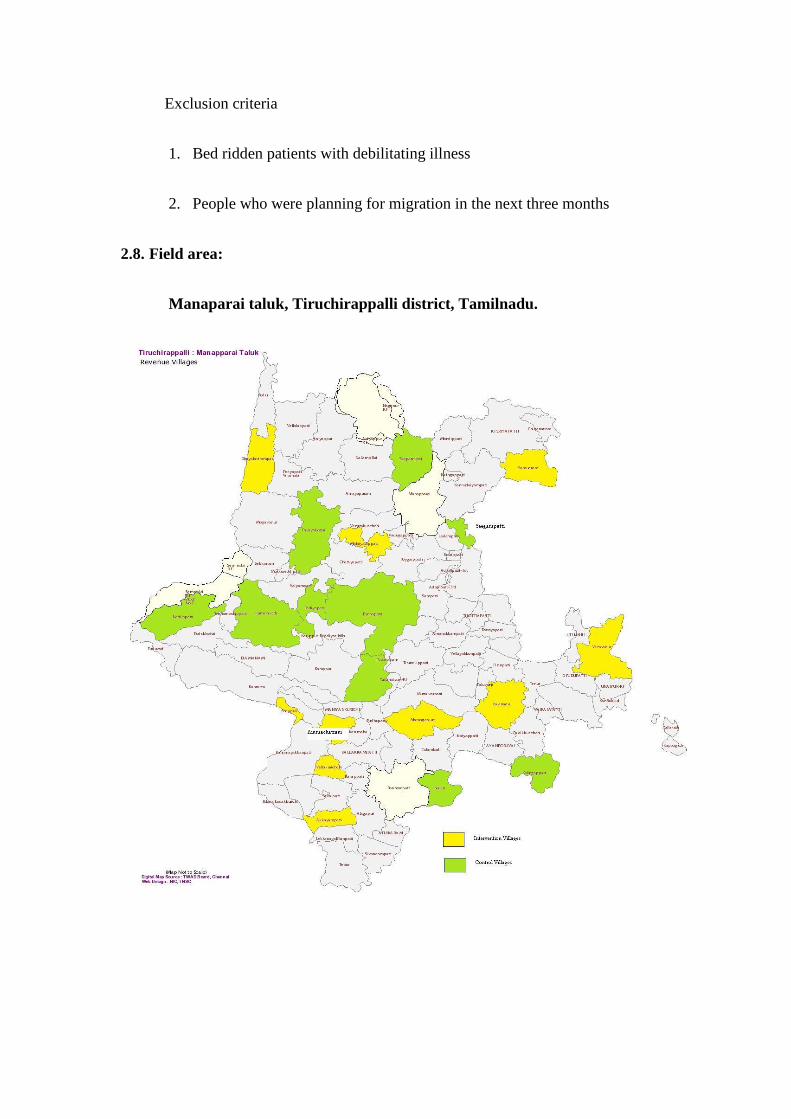
2.8. Field area:
Manaparai taluk, Tiruchirappalli district, Tamilnadu.

2.9. Data collection techniques:
Baseline Interview:
The socio demographic details, tobacco use pattern and determinants related to
outcome were collected using structured interview schedule.
Measurement of outcome:
The outcomes were measured using structured interview schedule. Self reported
point prevalence abstinence (No tobacco use in the past seven days) at two months after
receiving the intervention.
• Any attempt to quit tobacco which last more than 24 hours.
• Reduced tobacco consumption to more than 50% of initial use.
• Field notes were maintained to identify facilitators, barriers and acceptance of this
intervention in the community.
2.10. Blinding:
This study is an open label trial, the participants, the physician who delivered the
intervention and the outcome assessor were not blind to the allocation status. Since the
data collection, delivery of intervention, and the measurement of outcome was done by
single investigator, the potential for investigator bias has been minimized.
2.11. Ethical considerations:
Ethical clearance was obtained from Institute Ethics Committee (IEC), SCTIMST.
Participant information sheet was distributed to the individuals found to be eligible and
willing to participate in the study. The purpose of the study was explained to them.

Participation was voluntary. Written informed consent was obtained from the study
participants.
There were two ethical dilemmas arising from the study. The first one was the
timing of informed consent. Usually in simple randomized controlled trials informed
consent is obtained before the randomization process. But in cluster randomized trials
informed consent is obtained after the randomization process. This dilemma was solved
by informing the participants that their village was allotted under intervention/control
group based on a lottery method.
The second dilemma was whether this intervention study could lead to
stigmatisation of tobacco users in the community. But considering the high prevalence
and normality of tobacco use in the community, this study was less likely to stigmatise
the tobacco users.
2.12. Intervention Procedures – Intervention arm:
Two groups were formed in a cluster and each group comprised of 10 members.
After baseline data collection, convenient time and place for group intervention was
fixed. The intervention comprised of two sessions delivered five weeks apart. Each
session lasts for 30 minutes. The intervention was delivered by the principal investigator.
The intervention group received self help material (booklet) at the end of the first session.
Attendance of the group members was maintained. The group members benefitted from
physical examination and health advice free of cost. The content for this intervention was
designed based on the formative research done by Quit Tobacco India project.26-28
Components of first session:
1. Tobacco related facts: (Four minutes)

a. Ask the participants about the various forms of tobacco use?
b. According to your view which is harmful and safe for your health?
c. “All forms of tobacco are harmful to health” (Show pictures of commonly
used forms of tobacco)
d. According to your view which age group is more likely to die due to
tobacco use?
e. In India 10 lakh adults are dying due to smoking every year. 70 out of 100
smoking related deaths occur in middle age and not in old age.
f. Male smokers die six years earlier than non smokers (show life span
picture)
g. Tobacco kills one in every two users.
h. Ask the participants, whether the deaths due to tobacco can be prevented?
i. Tell them that the deaths due to tobacco use are entirely preventable.
2. Raising consciousness through photographs of diseased body parts: (Five
minutes)
a. According to you which are the body parts affected by tobacco use?
b. “Tobacco harms all parts of the body”
c. Some of the body parts affected by tobacco were shown to the
participants.
E.g. Oral cancer, normal teeth and smokers teeth, normal lung and healthy
lung, normal eye and cataract eye, chronic bronchitis and stroke.

3. Some common myths and facts related to tobacco use: (Five minutes)
Myths Facts
Chewing tobacco will help in relieving
tooth ache and it will protect the teeth.
You may lose your teeth overtime if you
continue to chew tobacco.
Chewing tobacco and pan parag will
control bad odour from the mouth
Chewing tobacco will lead to poor oral
hygiene and aggravate the symptoms of bad
odour.
Chewing betel quid will colour the lips,
mouth and will look more attractive.
In this computer era it is not considered as
attractive and people who are spitting this
red juice in public places are now
considered as uncivilised.
Smoking expensive cigarettes, foreign
cigarettes and filter cigarettes is not
harmful to health
Tobacco used in any form is harmful to
health. There is no safe cigarette.
Smoking few cigarettes/bidis in a day is
not harmful to health
Smoking even one cigarettes/bidis in a day
is harmful to health
Many old people who smoke are healthy People who had smoking related disease
might have died or have been admitted to
the hospital. We are not seeing them.
I am a daily wager, I need to smoke to be
able to work hard
People who do not smoke can work harder
than smokers. Smoking will reduce the
ability to work hard due to health problems.
4. Illness narratives to explain tobacco related burden of disease: (Six minutes)
a. Story of patient with oral cancer

5. Story of patient who suffered from heart attack (See the appendix VIII for the
stories)
6. Benefits of quitting tobacco: (Four minutes)
a. Ask the group members about the benefits of quitting tobacco.
b. If you quit tobacco you can protect yourself from cancer, heart disease,
stroke and respiratory diseases.
c. If you quit tobacco your appetite will increase, you can eat good food with
the money saved, your smell and taste for food will improve, your
immunity will improve, you can work better, your sleep will improve and
in total you and your family can lead a healthy and happy life.
d. If you quit smoking your breathing will improve and you can breathe fresh
air.
e. Now ask the group members to weigh the disadvantages due to tobacco
use and advantages of quitting. Ask the group members about their future
goals and help them to identify that their current behaviour (Tobacco use)
is not consistent with their future goals.
f. Ask the group members if they have any dilemmas in quitting tobacco.
Help to resolve the dilemma.
g. Ask the group members to take a decision to quit or not to quit based on
their understanding. If someone is not willing to quit ask him the reasons
behind his decisions and resolve his ambivalence.
7. Plan for quitting tobacco: (Six minutes)

a. Decide your date for quitting
b. Decide your choice between sudden quitting and gradual quitting and there
is no harm in quitting either suddenly or gradually.
c. Tell friends and family about your plan to quit- for encouragement and
support from others
d. Don‟t buy more than one packet of tobacco at a time in the next two
weeks.
e. Try to abort or postpone each smoking/chewing episode for at least five
minutes.
f. Destroy all unused cigarettes/Hans/Pan parag/Bidis and clean the house to
remove these products
g. Practice deep breathing (Demonstrate deep breathing exercise)
h. Tobacco chewers can buy some chewing gums for the first few weeks.
Components of second session:
1. Discussion of the experience of group members in quitting tobacco in the last
one month (ten minutes)
2. Withdrawal symptoms and measures to overcome them: (Eight minutes)
a. If you quit tobacco you will develop withdrawal symptoms
b. Withdrawal symptoms will last for one to two weeks.
c. Dryness of mouth - drink more water
d. Constipation- Drink more water, eat vegetables and fruits

e. Restlessness and throbbing of head – Soak a piece of cloth in cold water
and apply on the forehead.
f. Sleepiness and feeling of dullness – Go for a walk or wash your face.
g. Consumption of special foods, extra water or exercise cannot remove toxic
chemicals from our body.
h. The longer you have smoked, the longer it will take for the body to
recover fully.
3. Coping strategies/Prevention of relapse:(Seven minutes)
a. Your commitment to quit tobacco will become easier if you have strong
support from your friends and family members.
b. If you develop urge to use tobacco, take a deep breath and hold on for five
minutes, and the urge will go. (Demonstrate deep breathing exercise)
c. If you develop urge, drink more water and you can have a meal.
d. If you develop anger and frustration, share your feelings with your family
members and friends.
e. Don‟t be lonely. Involve yourself in some kind of work which you like
most.
f. The doctor said that tobacco use is the cause for my tiredness and lethargy
and it will reduce my ability to work.
g. The doctor said that tobacco use is the cause for my symptoms (any
symptoms convenient for you) and I may get many other diseases if I
continue to use tobacco.

h. Most people try to quit several times before they are successful. So don‟t
get frustrated with small failures.
4. Hazards of second hand smoke: (Explain with photographs related to passive
smoking) – Five minutes.
a. Smoking in your home will affect the health of your wife and children.
b. If a father smokes his son is more likely to become a smoker compared to
a non-smoking father. If you don‟t want your son to be a smoker please
quit immediately. Your child is more likely to suffer from respiratory
infections and asthma, if you continue to smoke.
c. If you smoke near a pregnant woman, she is prone for complications like
abortion and premature delivery and she is more likely to give birth to a
low birth weight baby.
d. People who are exposed to tobacco smoke also suffer from tobacco related
diseases.
e. If you smoke in public places people around you are affected by your
behaviour. Smoking in public places is a punishable offence.
2.13. Control Arm:
Control arm received self help material (Booklet) immediately after baseline data
collection. The content of the material had information regarding harmful effects of
tobacco, health benefits of quitting tobacco and advice on how to stop tobacco use.

2.14. Definition of variables:
Measurement of outcome:
1. Point prevalence abstinence: No tobacco use in the past seven days
2. Quit attempt: Any attempt to quit tobacco which last for more than 24 hours.
3. Reduction of tobacco use: Reduction of tobacco use more than 50% of the
baseline consumption.
Independent variables:
1. Age in completed years: Only adult men between 20 to 40 years of age were
included in the study. Age can determine the severity of nicotine dependence and
the outcome of intervention.
2. Marital status: Current marital status was assessed to find whether support from
spouse has any influence on quit rate.
3. Years of schooling: Number of completed years of schooling was collected to
look for any association with educational status and quit rate.
4. Per capita monthly expenditure: Total household expenditure in the last month
and total number of household members were collected to estimate the per capita
monthly expenditure. Some studies have found wealthier people were more likely
to stop tobacco use compared to their counterparts.
5. Occupation: The current occupation in the last twelve months was assessed and
classified into six strata. The six strata were
i. Professional/ Executive/ Big business
ii. Clerical/ Medium business
iii. Skilled / Self employed workers
iv. Unskilled/ landless labourers
v. Student

vi. Unemployed
The type of occupation can influence tobacco cessation.
6. Religion: The common religions in India are Hindu, Muslim and Christian.
Spirituality and religious practices can affect the perception of tobacco use and
chances of quitting. In Tamilnadu most Hindu men quit tobacco and alcohol
during their visit to Sabarimala temple in Kerala.
7. Caste: Caste is an important social determinant of health in India. The government
of India has identified people in the lower rung of social hierarchy as the most
disadvantaged and classified them as Scheduled Castes (SCs) and the Scheduled
Tribes (STs). The government has identified some occupational castes as socially
backward and classified them as Other Backward Castes (OBCs). It was found
that tobacco use is significantly higher among SCs than OBCs.
8. Alcohol use: History of alcohol consumption in the last one month was assessed.
Since alcohol consumption will affect the participation in the intervention and
subsequent outcomes. Studies show that people who are chronic alcoholic are less
likely to quit tobacco.
9. Family history of tobacco use: History of tobacco use by family members was
assessed. Particularly tobacco use by spouse was shown to affect the chances of
quitting.
10. Peer use of tobacco use: Culturally young men in rural areas learn to use tobacco
together and exchange of tobacco products is considered to facilitate social
solidarity, bonding and affiliation. Peer support is very important for an individual
to quit tobacco.
11. Forms of tobacco use: The different products of tobacco use was collected and
then grouped as smoking, and smokeless forms.

Smoking: Cigarettes and Bidis
Smokeless: Cut leaves tobacco, Khaini, Gutkha and Snuff.
12. Number of years of tobacco use: Some studies have found out that the chance of
success with a cessation attempt decrease with the length of time spent as tobacco
user. So number of years of tobacco use was collected.
13. Self rated health status: Participants were asked to compare their physical
condition with that of others of the same age. They were asked to rank their health
status as good, fair or poor. Participants with poor health status may quit tobacco
use citing their health reasons.
14. Perceived harm about tobacco use: Participants were assessed whether they
perceive tobacco use is harmful to their health. Participants who perceive tobacco
use as harmful to their health may quit tobacco.
15. Stage of change: Prochaska‟s Stages-of-change model is a widely used model in
tobacco cessation interventions. This model views the behaviour change as series
of actions or events. This model proposes that stages of behavioural change can be
conceptualised into six stages.36
1. Precontemplation 2. Contemplation 3. Preparation 4. Action
5. Maintenance 6. Relapse
In this study the Precontemplation stage and contemplation stage were defined as
Precontemplation stage:
Both did not try to quit in the last year and did not wish to quit in the next
year.
Contemplation stage:
i. Tried to quit in the last year or
ii. Wish to quit in the next year or

iii. Both tried to quit or wish to quit.
16. Fagerstrom Test for Nicotine Dependence:
This is a standard instrument used for assessing the intensity of physical dependence.
It is one of the most widely accepted evaluative instruments to establish and quantify
nicotine dependence and has been found to be reliable and valid in different settings. It
consists of six items and has a score range from 0 to 10. A study done among Indian
sample of smokers with poly drug use showed that FTND had good construct reliability
since all items of FTND scale had significant item-total correlations. But the internal
consistency reliability was found to be low with a cronbach‟s alpha of 0.58 which is near
to the cut off 0.6 for exploratory research.37
In this study FTND-Smoking38
and FTND-ST39
were used to assess the
dependence of smokers and subjects using smokeless tobacco. For individuals who were
using both forms of tobacco, both scales were administered and the highest score was
taken as final score. There were two assumptions behind using the Fagerstrom scale in
Indian setting,
1. Bidi was considered as equal to cigarette in terms of size and nicotine content
2. The sizes of the different smokeless products were considered as the same.
3.8. Statistical analysis:
The data was analysed using SPSS version17. Univariate analysis was done. The
baseline characteristics of the intervention and control group were compared to look for
any statistically significant difference. P value of <0.05 was considered to be statistically
significant. The outcomes measures were analysed using both complete case analysis and
intention to treat analysis. Bivariate analysis and multi variate analysis was done to
identify the predictors of abstinence.

CHAPTER 3
RESULTS
5.1. Baseline characteristics:
The baseline characteristics of the participants were collected under three domains
and they were compared between intervention and control group.
1. Socio demographic profile
2. Baseline tobacco use status
3. Determinants of tobacco cessation
3.1.1. Socio-demographic characteristics:
Overall, the mean (SD) age of the participants was 30.46(6.49). The mean (SD)
age of the intervention group and control group were 31.69(6.7), 29.22(6.04)
respectively. The difference in the mean age between the intervention and control group
was found to be statistically significant (p= <0.001). The intervention and control group
were not comparable by age. Overall mean (SD) number of years of schooling was 7.46
(3.5).
The mean (SD) per capita expenditure of the intervention and control group was
Rs.535.08 (469.31), Rs.639.59 (520.8) respectively. Overall, 62% of the participants
spent less than Rs.587 in the last month. The difference in the per capita expenditure
between the intervention and control group was not statistically significant (p=0.08). The
socio-demographic profile of the intervention and control group was comparable except
for the age and occupation.

Table 3.1: Socio-demographic characteristics of the participants
Variable Intervention
n (%)
Control
n (%)
Overall
n (%)
p value
No. of Participants 200 200 400
Age group
20-24
25-29
30-34
35-40
37(18.5)
38(19)
46(23)
79(39.5)
56(28)
52(26)
44(22)
48(24)
93(23.3)
90(22.5)
90(22.5)
127(31.8)
0.003
Years of schooling
<=10 years
>10 years
172(86)
28(14)
175(87.5)
25(12.5)
347(86.8)
53(13.3)
0.66
Marital status
Unmarried
Currently married
Others*
43(21.5)
155(77.5)
2(1)
58(29)
141(70.5)
1(0.5)
101(25.3)
296(74)
3(0.7)
0.27
Per capita expenditure
<Rs.587/month
>=Rs.587/month
133(66.5)
67(33.5)
116(58)
84(42)
249(62.3)
151(37.8)
0.08
Occupation
Clerical/medium business
Self employed/skilled
Unskilled/landless labourer
Student
Unemployed
4(2)
63(31.5)
120(60)
6(3)
7(3.5)
1(0.5)
103(51.5)
89(44.5)
2(1)
5(2.5)
5(1.3)
166(41.5)
209(52.3)
8(2)
12(3.1)
<0.001
Caste
Other Backward caste
Scheduled caste
112(56)
88(44)
123(61.5)
77(38.5)
235(58.8)
165(41.3)
0.31
Religion
Hindu
Others**
196(98)
4(2)
194(97)
6(3)
390(97.5)
10(2.5)
0.7
*Divorced and separated. **Muslim and Christians
Source: Community group intervention trial (CGIT), 2010

3.1.2. Tobacco use status of the participants:
Table 3.2: Tobacco use status of the participants
Variable Intervention
n (%)
Control
n (%)
Overall
n (%)
p value
Forms of tobacco use
Smoking
Smokeless
Both forms
67(33.5)
93(46.5)
40(20)
77(38.5)
76(38)
47(23.5)
144(36)
169(42.2)
87(21.8)
0.23
Years of tobacco use
<10
>=10
90(45)
110(55)
107(53.5)
93(46.5)
197(49.3)
203(50.8)
0.1
Nicotine dependence
Low and moderate
High and very high
131(65.5)
69(34.5)
144(72)
56(28)
275(68.8)
125(31.3)
0.19
Source: Community group intervention trial (CGIT), 2010
Overall mean (SD) age at initiation was 19.98(5.88). The mean age at initiation
for the intervention and control group were 20.08(6.27), 19.87(5.48) respectively and the
difference was not statistically significant (p=0.72). Overall mean (SD) number of years
of tobacco use was 10.34 (7.27).
Nicotine dependence was measured using Fagerstrom Test for Nicotine
Dependence (FTND). Those with less than score six were considered as having low and
moderate nicotine dependence. Those with more than or equal to score six were
considered as having high and very high nicotine dependence. The overall mean (SD)
Fagerstrom score was found to be 4.06 (2.71). The mean Fagerstrom score for smoking
and smokeless forms of tobacco were 3.68(2.92), 3.66(2.46) respectively. The Fagerstrom
score was positively correlated with age (r=0.32, p <0.001), number of years of tobacco
use (r=0.46 p <0.001) and negatively correlated with age at initiation (r = -0.21, p <0.001)

3.1.3. Determinants of tobacco cessation:
Table 3.3: Determinants of tobacco cessation
Variable Intervention
n (%)
Control
n (%)
Overall
n (%)
p value
Alcohol consumption 136(68) 142(71) 278(69.5) 0.58
Family H/O of tobacco use 104(52) 112(56) 216(54) 0.48
Peer use of tobacco 173(86.5) 185(92.5) 358(89.5) 0.07
Mean number of quit
attempts (SD)
2.09(2.04)
1.67(1.2)
1.86(1.63)
0.07
Self reported health status
Good
Fair
Poor
100(50)
86(43)
14(7)
135(67.5)
52(26)
13(6.5)
235(58.8)
138(34.5)
27(6.8)
0.001
Perceived harm related to
tobacco use 176(88) 183(91.5) 359(89.8)
0.32
Received advice to quit
tobacco in the last year 67(33.5) 76(38) 143(35.8)
0.4
Source of advice
Friends
Family members
Relatives
Health professionals
Others
17(25.4)
23(34.3)
8(11.9)
12(17.9)
7(10.4)
24(31.6)
27(35.5)
6(7.9)
13(17.1)
6(7.9)
41(28.7)
50(35)
14(9.8)
25(17.5)
13(9.1)
0.85
Stage of change
Precontemplation stage
Contemplation stage
30(15)
170(85)
18(9)
182(91)
48(12)
352(88)
0.09
Source: Community group intervention trial (CGIT), 2010
Overall 57% of the participants reported to have made at least one quit attempt in
the last year which lasted for more than 24 hours, 83.8% of the participants reported their
wish to quit tobacco in the next year. Among those who tried to make a quit attempt,

56.3% (one attempt), 26.6% (two attempt), 7.4% (three attempt), 9.3% (more than three
attempt) in the last year. The intervention and control groups were comparable except for
age, occupation and self reported health status.
3.2. Follow up:
Follow up data were available for 366 (91.5%) subjects at two months. The follow
up rates for the intervention and control group were 90.5% and 92.5% respectively. The
difference in the follow up rates between the intervention and control group was not
statistically significant (p=0.59).
3.3. Effects on tobacco cessation at two months:
The outcome measures were analysed using two approaches
1. Complete case analysis: Excluding participants with missing data
2. Intention to treat analysis: Including all participants who were randomized into
treatment conditions and treating the individuals with missing data as continue to
use tobacco.
Primary outcome: Self reported point prevalence abstinence at two months
Secondary outcomes: Quit attempt, reduction of tobacco use more than 50% at two
months.

Table 3.4: Effects on tobacco cessation at two months using complete case analysis
Outcome Intervention
n (%)
Control n
(%)
Unadjusted OR
(95% CI)
*Adjusted OR
(95% CI)
p value
Abstinence
25 (13.8) 12 (6.5) 2.31 (1.12, 4.75) 2.86 (1.23, 6.64) 0.014
Quit attempt
47 (30.1) 37 (21.4) 1.58 (0.96, 2.6) 2.02 (1.15, 3.54) 0.014
Reduction
>50%
38 (24.4) 17 (9.8) 2.95(1.59, 5.49) 3.69 (1.82, 7.47) <0.001
*Adjusted for age, marital status, occupation, caste, forms of tobacco use, alcohol use,
years of tobacco use, stage of change and nicotine dependence.
Table 3.5: Effects on tobacco cessation at two months using intention to treat analysis
Outcome Interve
-ntion
(%)
Control
(%)
Unadjusted OR
(95% CI)
*Adjusted OR (95%
CI)
p
value
Abstinence
12.5 6 2.24 (1.09, 4.59) 2.59 (1.14, 5.94) 0.024
Quit attempt
26.9 19.7 1.49 (0.92, 2.45) 1.84 (1.07, 3.17) 0.029
Reduction
>50%
21.7 9 2.79 (1.51, 5.16) 3.44 (1.72, 6.88) <0.001
*Adjusted for age, marital status, occupation, caste, forms of tobacco use, alcohol use,
years of tobacco use, stage of change and nicotine dependence.
Source: Community group intervention trial (CGIT), 2010
After adjusting for age, marital status, occupation, caste, forms of tobacco use,
alcohol use, years of tobacco use, stage of change and nicotine dependence OR showed
slight improvement. This improvement in OR may be due to the difference in the age and
occupation between the intervention and control groups. The odds ratio estimates for the
outcome measures were not substantially altered in intention to treat analysis. Brief group

intervention had increased the quit rate, quit attempt and reduction of tobacco use more
than 50% in the short term among young rural Indian men.
3.4. Results of bivariate analysis to identify predictors of abstinence:
The outcome variable was seven days point prevalence abstinence at two months.
Bivariate analysis was done to identify the predictors of abstinence. Age between 20-24
years, unmarried, no history of alcohol consumption in the last month, smokeless form of
tobacco use, tobacco use less than 10 years, low and moderate nicotine dependence were
found to be significantly associated with abstinence.

Table 6: Bivariate analysis to identify predictors of abstinence
Variable Abstinence
OR 95% CI p value Yes N (%) No N (%)
Age
20-24
25-29
30-34
35-40
14(17.1)
5(6)
9(10.7)
9(7.7)
68(82.9)
78(94)
75(89.3)
108(92.3)
2.47
0.77
1.44
1
1.01, 6.02
0.25, 2.38
0.55, 3.79
--
0.05
0.65
0.46
--
Years of schooling
<=10
>10
31(9.7)
6(12.5)
287(90.3)
42(87.5)
0.75
1
0.29, 1.9
--
0.56
--
Per capita expenditure
<Rs.587/month
>=Rs.587/month
23(10)
14(10.3)
207(90)
122(89.7)
0.97
1
0.48, 1.95
--
0.93
--
Occupation
Unskilled /Manual
Skilled /self employed
19(9.9)
13(8.6)
172(90.1)
139(91.4)
1.18
1
0.56, 2.47
--
0.66
--
Marital status
Unmarried
Married
15(17)
21(7.6)
73(83)
254(92.4)
2.48
1
1.22, 5.06
--
0.01
--
Caste
Other Backward Caste
Scheduled Caste
22(10.3)
15(9.9)
192(89.7)
137(90.1)
1.05
1
0.52, 2.09
--
0.89
--
Alcohol consumption
Yes
No
19(7.5)
18(16.1)
235(92.5)
94(83.9)
1
2.37
--
1.19, 4.71
--
0.01

Table 6: Bivariate analysis to identify predictors of abstinence (Continued...)
Variable Abstinence
OR 95% CI p value Yes N (%) No N (%)
Family H/O tobacco use
Yes
No
19(9.7)
18(10.6)
177(90.3)
152(89.4)
0.906
1
0.459, 1.789
--
0.78
--
Forms of tobacco use
Smoking
Smokeless
Both forms
10(7.5)
23(15)
4(5)
123(92.5)
130(85)
76(95)
1
2.176
0.647
--
0.995, 4.758
0.196, 2.137
--
0.051
0.475
Years of tobacco use
<10
>=10
27(15)
10(5.4)
153(85)
176(94.6)
3.106
1
1.457, 6.623
--
0.003
Nicotine dependence
Low and moderate
High dependence
33(13)
4(3.5)
220(87)
109(96.5)
4.087
1
1.412, 11.831
--
0.009
--
Self rated health status
Good
Fair
Poor
26(11.9)
10(8.2)
1(4)
193(88.1)
112(91.8)
24(96)
1
0.663
0.309
--
0.308, 1.425
0.04, 2.383
--
0.29
0.26
Received advice to quit
Yes
No
14(10.6)
23(9.8)
118(89.4)
211(90.2)
1.09
1
0.540, 2.195
--
0.813
--
Stage of change
Precontemplation
Contemplation
2(4.5)
35(10.9)
42(95.5)
287(89.1)
1
2.561
--
0.594, 11.042
--
0.207
Source: Community group intervention trial (CGIT), 2010
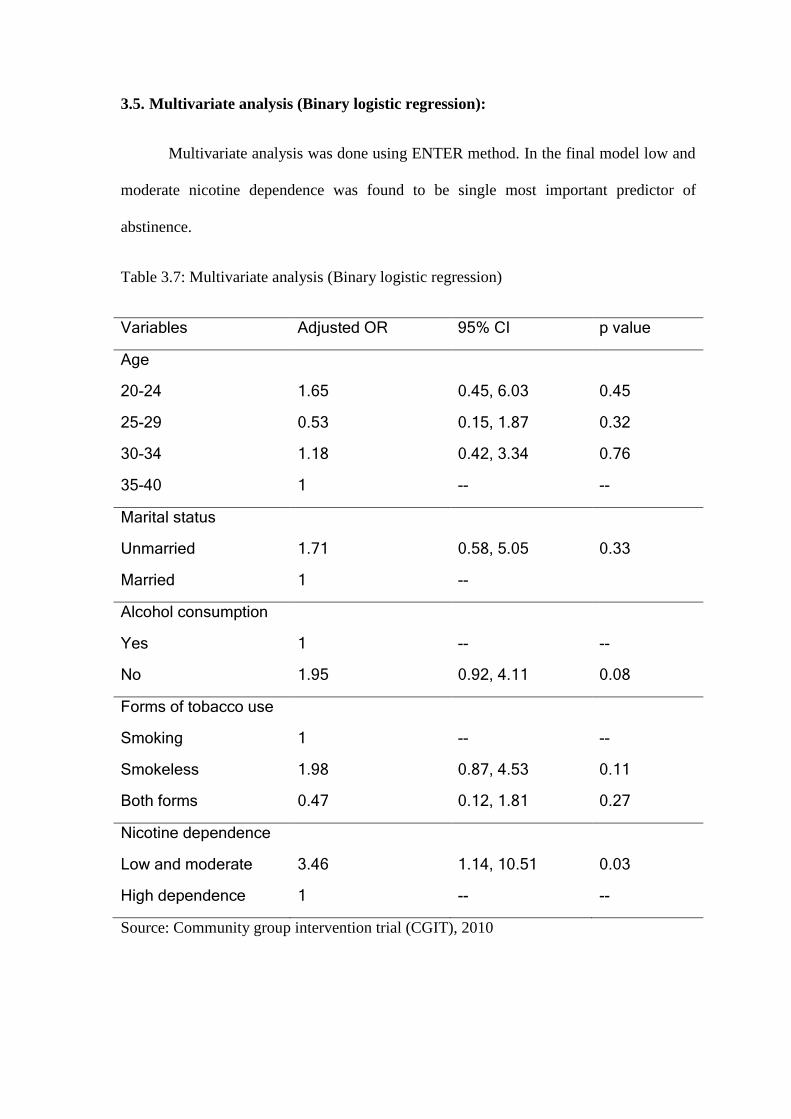
3.5. Multivariate analysis (Binary logistic regression):
Multivariate analysis was done using ENTER method. In the final model low and
moderate nicotine dependence was found to be single most important predictor of
abstinence.
Table 3.7: Multivariate analysis (Binary logistic regression)
Variables Adjusted OR 95% CI p value
Age
20-24
25-29
30-34
35-40
1.65
0.53
1.18
1
0.45, 6.03
0.15, 1.87
0.42, 3.34
--
0.45
0.32
0.76
--
Marital status
Unmarried
Married
1.71
1
0.58, 5.05
--
0.33
Alcohol consumption
Yes
No
1
1.95
--
0.92, 4.11
--
0.08
Forms of tobacco use
Smoking
Smokeless
Both forms
1
1.98
0.47
--
0.87, 4.53
0.12, 1.81
--
0.11
0.27
Nicotine dependence
Low and moderate
High dependence
3.46
1
1.14, 10.51
--
0.03
--
Source: Community group intervention trial (CGIT), 2010

3.6. Barriers, facilitators and acceptance of intervention:
To find out the potential barriers, facilitating factors and acceptance of this
intervention, field notes were maintained during the intervention period. Attendance of
the group members were maintained for both the health education sessions. The
attendance in the first and second session was 88.5% and 60.5% respectively.
Barriers for implementation of intervention:
1. Timing: Most of the rural men go for their work at 7.30 AM and return to their
home after 6.00 PM. So the intervention can be delivered as envisaged only after
7.00 PM. In some of the villages most of them were construction workers,
electricians and factory workers, they leave to Trichy at 6.30 AM and return to
their house at 9.00 PM and they can be seen only on the Sundays.
Table 3.8: Barriers, facilitators and acceptance of intervention
Barriers Facilitating factors Acceptance
Timing of the intervention Formation of spontaneous
peer groups
Community perception of
alcohol as a major problem
has lead to poor acceptance
for tobacco cessation
intervention
Alcohol consumption Good logistics Indifference to non-
pharmacological
intervention
Migration Blood pressure
measurement and
examination of oral cavity
Participants demand for
supply side intervention
Geographical location
of houses
Mobile phones
Gambling,
Unexpected events
Support from youth clubs,
shop keepers, tea shops and
village head man
Source: Community group intervention trial (CGIT), 2010

2. Alcohol consumption: Alcohol intake impedes the implementation of the
intervention. In all the villages men after returning from their work leave to the
nearby place where state owned liquor shop was located. So it was difficult to find
men in their village during the evening time and they return to their home at 7-
7.30 PM.
3. Out migration: Most rural young men in the age group 20-40 migrate for their
work to nearby cities and towns. Most men were working in Trichy, Coimbatore,
Thirupur, Chennai, Bangalore, Arab countries, Kerala (Kannur) and Singapore. In
some villages recruitment became very difficult because of migration.
4. Geographical location of houses: In this taluk few villages were a group of eight
hamlets. In each hamlet there will be 20-30 houses. It was difficult to form group
of ten members in one hamlet. The dominant caste in this taluk was „Oorali
gounders‟. They used to construct the house in their farmland not in the villages
so the houses were scattered. Most villages in this taluk have four „kalams‟ (group
of 10-15 houses). There were four kalams in each village; each kalam was located
one kilometre away from the village. This lead to scattering of houses in the
village.
Figure 3.1: Geographical location of houses in a village

5. Gambling. In four of the intervention villages a group (10-15) of men were found
to be playing cards for money. It was found that most of them were tobacco users
and the advantage was that they can be seen together for the second session. But
the response was poor from these people and they refused to participate. They
were busy in playing the game.
6. Unexpected events: Since this study was done without prior communication to
the community, unexpected events like temple festivals, deaths, marriages, clash
between groups of men has affected the implementation of the trial.
Facilitating factors:
1. Spontaneous peer groups: In rural areas young men learn to use tobacco
products together, share tobacco products on occasions, particularly during
situations of shortage with any one of their friends. When notions of male bonding
include sharing of risks, almost all of them share information about the
consumption patterns of each other and are in a position to report accurately about
each other. This camaraderie has the potential to facilitate cessation efforts.
2. Good logistics: The ideal time for conducting group intervention was after 7.00
PM. Since most of the villages were remote and did not have frequent transport
facilities, motor cycle was helpful for the timely completion of the project.
3. Physical examination: Blood pressure measurement was found to be a major
incentive for the participation in this intervention. Some of them said they have
participated in this intervention only to check their blood pressure. Many new
hypertension and accelerated hypertension cases were identified and referred to
primary health centres.

4. Mobile phones: Overall 51.75% of the participants provided their mobile phone
numbers and this was helpful to fix the timings for the second session and follow
up interview.
5. Support from the community: Support from the community was found to be
crucial for mobilising the people to one place. Youth clubs, young volunteers,
village head man, petty shop and tea shop owners helped in recruitment and
delivery of the intervention.
Acceptance of the intervention:
1. Alcohol as important problem: Community perception of alcohol as a major
problem has lead to poor acceptance for tobacco cessation intervention. Alcohol
consumption in Tamilnadu is increasing at an alarming level after the government
owned liquor shops were opened throughout the state.
2. Indifference to non-pharmacological intervention: Some participants believed
that the tobacco addiction can be overcome only through medication and
impossible through booklet or health education.
3. Demand for supply side intervention: Many of the participants demanded,
argued and fought for supply side intervention like complete ban on tobacco.

Chapter 4
Discussion and conclusion
4.1. Discussion:
This study aimed to determine the efficacy of group health education for tobacco
cessation in rural areas of Tamilnadu, India. It also aimed to look at the issues like
potential barriers and facilitating factors for successful implementation of the
intervention. This intervention was based on the formative research done by Project QTI
to develop culturally appropriate approaches for tobacco cessation in developing
countries. The intervention was targeted at rural young men between 20-40 years of age
who are most affected by the tobacco epidemic in India.
The age group 20-40 years was chosen based on two premises. The first one was
to ensure group homogeneity and it had the potential for spontaneous peer group
formation.34
In rural areas young men learn to use tobacco products together, sharing
tobacco with their peers facilitates the social solidarity, bonding and affiliation. In this
context, quitting tobacco will compromise the social relationships and reduce the
opportunities for socializing. So focussing an individual to quit tobacco without
considering the social environment can place the individual at „social risk‟. Peers are
likely to question the ability of the individual to quit tobacco, rather than supporting the
quit attempts.28
The importance of focussing peer groups has been reiterated in this study
since 89.5% of the participants reported peer history of tobacco use. This calls for an
approach which focuses on community and groups rather than an individual centric,
clinic based cessation services.

The second premise was that 70% of the one million smoking related mortality in
India was projected to occur in the middle age rather than old age.13
It has been shown
that half of the long term smokers will die during their productive middle age, losing 20-
25 years of life.2 On the other hand it had been shown that the benefits of smoking
cessation were found to be largest in those who quit in the middle age between 25 and 34
years.19
4.1.1. Baseline characteristics:
The mean age (30.5 ± 6.5), mean number of years of tobacco use (10.3 ± 7.3) and
Fagerstrom score (4.06 ± 2.7) of this study was found to be lower than a study done in
Indian sample of smokers with poly substance abuse attending a tobacco cessation clinic.
The mean age (37 ± 11), mean number of years of tobacco use (18 ± 10) and Fagerstrom
score (5.6 ± 2.4) was on the higher side for clients attending tobacco cessation clinic.37
So
the results of this trial should be interpreted carefully as it was targeted among young
tobacco users with less nicotine dependence.
Nearly 69% of the study sample had either low or moderate dependence for
tobacco, the rest 31% had either high or very high dependence. Behavioural interventions
alone can help 69% of the participants to quit tobacco. Individuals with high or very high
dependence may require both behavioural and pharmacological interventions. The study
done among smokers with poly substance abuse found that 58% of the study population
were heavily or very heavily dependent on smokable tobacco products. This was found to
be consistent with the literature that substance abusers tend to be heavy smokers and are
more nicotine dependent.37
But at the community level majority of the tobacco users had
either low or moderate dependence on tobacco when compared to the tobacco cessation
clinics.

In this study use of smokeless (42%) tobacco was found to be higher than NFHS-
3 data (18.8%). According to NFHS-3 rural men use smokeless tobacco (18.8%) more
than smoking form of tobacco (34.3%) in Tamilnadu.10
According to NFHS-3 41.5% of men between the age group 15-49 drink
alcohol in Tamilnadu.10
In this study 69.5% of men between the age group 20-40 reported
alcohol consumption in the last month. Alcohol consumption was found to be an
important barrier which affected the delivery of the intervention. People with alcohol
dependence were more likely to be heavy smokers with high nicotine dependence.37
Alcohol consumption was shown to increase the relapse rates after successful cessation.40
A study done in urban Assam found that 97.3% of the study participants were
aware of any tobacco related health problem. But in this trial, only 89.8% of the
participants perceived that tobacco is harmful to health.41
Only 35.8% of the study participants received advice to quit tobacco in the last
year. Majority of them received advice from social networks like family members, friends
and relatives. Very few of them received advice to quit tobacco from the health
professionals. Young men in the age group of 20-40 years were less likely to fall ill and
get hospitalised. If we focus only on „teachable moments‟ when tobacco users come to
the hospitals or cessation clinics we will not be able to reach these young men. Proactive
efforts should be taken to reach these men in the community.
In the present study 57% of the participants made at least one quit attempt in the
last year which was found to be higher than a survey done in the United States in 1995. In
US 45.8% of current smokers had stopped smoking for at least one day in the preceding
12 months.42

Baseline characteristics of the intervention and control group were comparable
except for age, occupation and self reported health status. Intervention group had more
people in the age group 30-40, unskilled/landless labourers with self reported health
status as „Fair‟ than the control group. The odds ratios of the outcome variables were
adjusted for these variables to make intervention and control groups comparable.
4.1.2. Effects on tobacco cessation at two months:
Group intervention significantly increased the point prevalence abstinence, quit
attempt and reduction of tobacco use more than 50% of initial use at the end of two
months compared to the control group.
Abstinence was found to be 2.6 times higher in the intervention group when
compared to the control group. Cochrane review of group behaviour therapy programs for
smoking cessation included 13 trials which compared a group program with a self help
program. There was an increase in cessation with the use of a group program (Relative
Risk = 1.98, 95% CI, 1.6 to 2.46).30
A meta analysis of behavioural interventions for
smoking cessation reviewed 12 Randomized controlled trials on group counselling and
estimated that the treatment effects was 1.76 (OR =1.76,95% CI, 1.11-2.93).43
Another meta analysis which reviewed 58 studies found that the estimated odds
ratio was 1.3 (95% CI, 1.1 to 1.6) for group counselling when compared to no
counselling.18
When compared to these meta analyses the OR was found to be higher in
the present study. But these meta analyses included only trials with biochemically
verified outcomes at six or twelve months. The important limitation of the present study
was that it looked at short term self reported outcomes.

Reduction of tobacco use more than 50% of the initial use was found to be 3.4
times more in the intervention group than the control group. In the intervention group
21.7% of the participants reduced tobacco consumption and this was comparable to the
tobacco cessation clinics in India (22%).44
4.1.3. Predictors of abstinence:
In the bivariate analysis, age between 20-24 years, unmarried, no history of
alcohol consumption in the last month, smokeless form of tobacco use, tobacco use less
than 10 years, low and moderate nicotine dependence were found to be significantly
associated with abstinence. But in the multivariate analysis low and moderate nicotine
dependence was found to be the single most important predictor of abstinence.
A review of determinants of outcome in smoking cessation interventions has
shown no effect of age on cessation attempts. Most studies which have examined
socioeconomic factors found no association with outcome. But few studies found that
wealthier people and those with higher levels of education were more successful in
stopping. The evidence is strong that heavier smokers find it more difficult to quit.
Several studies also demonstrate that the chance of success in any one cessation attempt
decreases with length of time spent as a smoker. Marriage has been shown to be a
predictor of good outcome. Alcohol consumption was shown to increase the chance of
relapse. Tobacco consumption status of the peers was shown to influence the outcome.40
A longitudinal study among Danish adults showed that the successful smoking
cessation was associated with older age, high social status, spouse smoking behaviour,
low prior tobacco consumption and baseline motivation to stop smoking.45
A study which investigated the quitting behaviour among current, daily, and non
daily young adult smokers in the United States found that nicotine dependence measures

play a significant role in quitting and intention to quit among daily smokers. But socio-
demographic variables play a significant role with quitting and intention to quit among
non-daily smokers.46
This trial highlights the need for measuring the dependence, which will be helpful
in tailoring the intervention. In this study 69% of the participants had low and moderate
dependence and they require brief behavioural interventions. But 31% of the participants
belonged to the category of high and very high dependence needs intensive behavioural
and pharmacological intervention.
Timings for the delivery of intervention, alcohol consumption and heavy rural-
urban migration were found to be the major barriers while implementing this trial. Most
of the rural men go for their work at 7.30 AM and return to their home after 6.00 PM. The
intervention can be delivered as envisaged only after 7.00 PM. Adequate planning and
interaction with community volunteers should be done before organising an intervention.
In this study 69.5% of men between the age group 20-40 reported alcohol consumption in
the last month. So it was found to be very difficult to meet them during evening hours.
Heavy rural-urban migration among young men resulted in difficulty in recruitment and
follow up. Most of these migrant workers were found to be employed in urban informal
sector. Interventions targeting urban informal sector will help rural migrants to quit
tobacco.
4.1.4. Tobacco cessation in India: Time for action
Tobacco consumption in India is increasing particularly among young people.11
Smoking was estimated to cause one million deaths every year from 2010. More than
70% of deaths will occur in productive young age rather than old age.13
This poses a huge
threat to overall development by increasing the health care costs and productive life years
lost for a country which aspires to be a major economic power in the 21st century.
47

Tobacco cessation is the only practical way to prevent millions of premature mortality
and morbidity before 2050.16
This is a great opportunity for India to act decisively and
curb the tobacco epidemic. India has responded by establishing few tobacco cessation
clinics and allocating Rs.40.5 crore (nine million USD) to a tobacco control program.47
The tobacco cessation clinic reaches urban educated tobacco users, whereas 79% of
tobacco users were living in rural India. The tobacco cessation clinics delivers intensive
specialist based cessation services and scaling up this service for a diverse country like
India is going to be very difficult.25
There is not much difference between the quit rates of
this brief group intervention and tobacco cessation clinics. There is a need to introduce
and scale up tobacco cessation techniques in India, which focus on group and community
settings not just individuals.
A review of tobacco dependence treatment systems in five countries such as
Brazil, England, India, South Africa and Uruguay found that lower income countries
prioritized more intensive but low reach approaches rather than developing basic
infrastructure. Of these countries only England had a combination of approaches with
wide reach less effective interventions (Brief advice in primary care) and smaller reach
intensive specialist support. In India brief advice is not integrated within the primary
health care system.25
We have a large number of health workers in the rural areas of India
and this can be effectively utilized for such brief interventions targeting groups of
tobacco users. This has the advantage of using the existing infrastructure without any
need for additional resources.
The primary health care system in India should be sensitized and strengthened to
deliver tobacco related health education and promote tobacco cessation. This requires
participation of health care professionals of all categories at all levels of health care.
Multipurpose health workers, nurses and doctors should at the forefront to tackle this

epidemic. To achieve these they should be suitably trained and adequately motivated.
Community based cessation facilities which can be delivered by grass root health workers
should be the main model for tobacco cessation in India.8
4.2. Strengths of the study:
1. The intervention was developed based on the formative research done by Project
Quit Tobacco International(QTI)
2. The intervention focussed on both smoking and smokeless forms of tobacco
3. The study followed the standard guidelines for reporting cluster randomized trials
as recommended by CONSORT statement (Consolidated Standards for Reporting
Trials).48
4.3. Limitations of the study:
1. This trial looked at only short term outcomes due to resource constrains. Future
trials should adhere to the „Russell Standard‟ and follow up should be done at six
or twelve months.49
2. This study measured the self reported outcomes. Ideally biochemical verification
should be done at least at the six month or twelve month follow up point.49
But
SRNT (Society for Research on Nicotine and Tobacco) subcommittee on
biochemical verification recommends that for large population based trials with
low demand situations, biochemical verification is not necessary.50
3. This is an open label trial. The outcome assessor was not blinded to allocation
groups while collecting follow-up data.
4. Data analysis was done with individual as a unit of analysis. Ideally the unit of
analysis should be done at cluster level for cluster randomized trials.
5. Women and elderly were excluded from this study. In this taluk gutkha
consumption is increasing among women.

6. There is no clinical equipoise in this trial since there is enough evidence from
western countries that group intervention is more efficacious than self help
materials. Ideally the control group should have been made as „delayed
intervention control‟. Due to the lack of time and resources, a booklet was issued
to the control group as a token of participation.
7. Participation in the second session of health education program was low.
4.4. Conclusion:
1. Community based group intervention for tobacco cessation has the potential to
reach rural young men.
2. The quit rate, quit attempts and reduction of tobacco use was found to be
significantly higher in the intervention group compared to the control group at two
months.
3. Low and moderate dependence was found to be the single most important factor
which was independently associated with abstinence.
4. Timing of the intervention, alcohol consumption and heavy rural-urban migration
were found to be important barriers for conducting group intervention in rural
areas.
4.5. Recommendations:
1. Future research should provide the assessment of biochemically verified long term
quit rates.
2. The National Tobacco Control Program should focus on community based brief
group interventions to improve the access to tobacco cessation services for the
majority rural tobacco users.

3. Brief tobacco cessation interventions should be integrated within the primary
health care delivery system.
4. Tamilnadu public health department can easily integrate this intervention with
their flagship mass rural disease prevention camps conducted under the scheme
“Varummun Kaappom Thittam”.

REFERENCE:
1) World Health Organisation. WHO report on the global tobacco epidemic, 2008.
http://www.who.int/tobacco/mpower/mpower_report_full_2008.pdf (accessed 20
Feb 2010).
2) Jha P, Chaloupka FJ. Curbing the Epidemic: Governments and the Economics of
Tobacco Control. Washington, DC: The World Bank; 1999:13-20.
3) Jha P, Ranson MK, Jguyen SN, Yach D. Estimates of global and regional smoking
prevalence in 1995, by age and sex. Am J Public Health 2002; 92: 1002-1006.
4) Molarius A, Parsons RW, Dobson AJ, Evans A, Fortmann SP, Jamrozik K et al.,
and WHO MONICA Project. Trends in cigarette smoking in 36 populations from
the early 1980s to the mid-1990s: findings from the WHO MONICA Project. Am
J Public Health 2001; 91: 206-212.
5) Murray CJL, Lopez AD. Global mortality, disability, and the contribution of risk
factors: Global burden of disease study. Lancet 1997; 349: 1436-42.
6) Ezzati M, Lopez AD, Rodgers A, Hoorn SV, Murray CJL, and the comparative
risk assessment collaborating group. Selected major risk factors and global and
regional burden of disease. Lancet 2002; 360:1347-60.
7) Murray CJL, Lopez AD. Alternate projections of mortality and disability by cause
1990-2020: Global burden of disease study. Lancet 1997; 349: 1498-1504.
8) Reddy KS, Gupta PC, eds. Report on Tobacco Control in India (2004). New
Delhi, India. Ministry of Health and Family Welfare.
9) Rani M, Bonu S, Jha P, Nguyen SN, Jamjoum L. Tobacco use in India:
Prevalence and Predictors of smoking and chewing in a nationally representative
cross sectional household survey. Tob Control 2003; 12: e4.

10) International Institute for Population Sciences (IIPS) and Macro International.
2007. National Family Health Survey (NFHS-3), 2005–06: India: Volume I.
Mumbai: IIPS.
11) Thankappan, K.R., Mini, G.K., Pakhale, S., Pandey, D., Pandey, R., Jha, P.,
Gupta, P. C., Peto, R., the Million Death Study Collaborators. Case-Control Study
of Smoking and Death in India. N Engl J Med 2008; 358: 2842.
12) Press Information Bureau, Government of India. Azad Releases First Global
Adult Tobacco Survey. http://pib.nic.in/release/release.asp?relid=66419
(Accessed 21 Oct 2010).
13) Jha P, Jacob B, Gajalakshmi V, Gupta PC, Dhingra N, Kumar R et al. A
nationally representative case–control study of smoking and death in India. N
Engl J Med 2008; 358:1137-47.
14) Jindal SK, Aggarwal AN, Chaudhry K, Chhabra SK, Souza GAD, Gupta D et al.
Tobacco Smoking in India: Prevalence, Quit rates, and Respiratory Morbidity.
Indian J Chest Dis Allied Sci 2006; 48: 37-42.
15) International Institute for Population Sciences (IIPS) and Macro International,
2008. National Family Health Survey (NFHS-3), India, 2005-06: Tamil Nadu.
Mumbai: IIPS.
16) Jha P. Avoidable global cancer deaths and total deaths from smoking. Nat Rev
Cancer. 2009; 9: 655-664.
17) Jha P, Chaloupka FJ, Moore J, Gajalakshmi V, Gupta PC, Peck R et al. Tobacco
addiction. In: Jamison DT, Breman JG, Measham AR, et al., eds. Disease control

priorities in developing countries. 2nd ed. New York: Oxford University Press,
2006:869-86. http://files. dcp2.org/pdf/DCP/DCP46.pdf. (accessed 20 Feb 2010).
18) Fiore MC, Jaen CR, Baker BT, et al. Treating tobacco use and dependence:
Clinical Practice Guideline 2008 update. Rockville, MD: U.S. Department of
Health and Human Services. Public Health Service. May 2008.
19) Doll R, Peto R, Boreham J, Sutherland I. Mortality in relation to smoking: 50
years‟ observations on male British doctors. BMJ 2004; 328: 1519.
20) Gajalakshmi V, Peto R, Kanaka TS, Jha P. Smoking and mortality from
tuberculosis and other diseases in India: retrospective study of 43000 adult male
deaths and 35000 controls. Lancet 2003; 362: 507-15.
21) Rose G, Colwell L. Randomised controlled trial of anti-smoking advice: final (20
year) results. J Epidemiol Community Health. 1982; 36: 102-108.
22) John RM, Sung HY, Max W. Economic cost of tobacco use in India, 2004. Tob
Control 2009; 18: 138-143.
23) Lando HA. Reflections on 30 + years of smoking cessation research: from the
individual to the world. Drug Alcohol Rev 2006; 25: 5-14.
24) World Health Organisation. Framework Convention on Tobacco Control. http://
www.who.int/fctc/en . (accessed 28 Sep 2010).
25) Raw M, McNeill A, Murray R. Case studies of tobacco dependence treatment in
Brazil, England, India, South Africa and Uruguay. Addiction 2010; 105: 1721-
1728.
26) Nichter M, for the Project Quit Tobacco International Group. Introducing tobacco
cessation in developing countries: an overview of Project Quit Tobacco
International. Tob Control 2006; 15: 12-17.

27) Nichter M, Nichter M, Muramoto M and Project Quit Tobacco International.
Project Quit Tobacco International: Laying the groundwork for tobacco cessation
in low- and middle-income countries. Asia Pac J Public Health 2010; 22: 181S-
188S.
28) Nichter M, Nichter M, Padmavathi S, Thresia CU. Anthropological contributions
to the development of culturally appropriate tobacco cessation programs: a global
health priority. In: Hahn R, Inhorn M, editors. Anthropology and public Health:
bridging differences in culture and society. 2nd
ed. New York: Oxford University
Press; 2009.
29) Sinha DN, Singh S, Jha M, Singh M. Report on tobacco cessation through
community intervention in India 2003.
www.searo.who.int/LinkFiles/NMH_cess3.pdf (accessed 27 Sep 2010).
30) Stead LF, Lancaster T. Group behaviour therapy programs for smoking cessation.
Cochrane Database Syst Rev. 2005; 2: CD001007.
31) Perry CL, Stigler MH, Arora M, Reddy KS. Preventing tobacco use among young
people in India: Project MYTHRI. Am J Public Health 2009; 99: 899-906.
32) Prabhakaran D, Jeemon P, Goenka S, Lakshmy R, Thankappan KR, Ahmed F et
al. Impact of a Worksite Intervention Program on Cardiovascular Risk Factors: A
Demonstration Project in an Indian Industrial Population. J Am Coll of Cardiol
2009; 53: 1718-1728
33) Metha FS, Gupta MB, Pindborg JJ, Bhonsle RB, Jalnawalla PN, Sinor PN. An
intervention study of oral cancer and pre cancer in rural Indian populations: a
preliminary report. Bull World Health Organ 1982; 60: 441-446.
34) Murthy P, Saddichha S. Tobacco cessation services in India: Recent developments
and the need for expansion. Indian J Cancer 2010; 47: 69-74.

35) Ministry of Home affairs: Directorate of census operations 2001.
www.census.tn.nic.in (Accessed 15 March 2010).
36) Prochaska JO, DiClemente CC, Norcross JC. In search of how people change. Am
Psychol 1992; 47:1102-4.
37) Jhanjee S and Sethi H. The Fagerstrom Test for Nicotine Dependence in an Indian
sample of daily smokers with poly drug use. Nicotine Tob Res 2010;
doi:10.1093/ntr/ntq148.
38) Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO. The Fagerstrom test
for nicotine dependence: a revision of the Fagerstrom Tolerance Questionnaire. Br
J Addict 1991; 86:1119-27.
39) Ebbert JO, Patten CA, Schroeder DR. The Fagerstrom test for nicotine
dependence – Smokeless tobacco (FTND-ST). Addict Behav 2006 31(9): 1716–
1721.
40) Lennox AS. Determinants of outcome in smoking cessation. Br J General practice
1992; 42: 247-252.
41) Sharma I, Sarma PS, Thankappan KR. Awareness, attitude and perceived barriers
regarding implementation of the cigarettes and other tobacco products act in
Assam, India. Indian J Cancer 2010; 47: 48-53.
42) Centers for Disease Control and Prevention. Cigarette smoking among adults
United States, 1995. MMWR Morb Mortal Wkly Rep 1997; 46:1217-20.
43) Mottillo S, Filion KB, Belisle P, et al. Behavioral interventions for smoking
cessation: a meta-analysis of randomized controlled trials. Eur Heart J 2009; 30:
718–730.
44) Murthy P. Clinic based tobacco cessation programs in India: the evidence and
what it calls for. Fourteenth world congress on tobacco or health.

www.14wctoh.org/abstract/.../Hemiplenary_5_Pratima_Murthy.pdf (accessed 21
Oct 2010).
45) Osler M, Prescott E. Psychosocial, behavioural, and health determinants of
successful smoking cessation: A longitudinal study of Danish adults. Tobacco
Control 1998; 7:262–267.
46) Fagan P, Augustson E, Backinger CL, O‟Connell ME, Vollinger RE, Kaufman A,
Gibson JT. Quit attempts and intention to quit cigarette smoking among young
adults in the United States. Am J Public Health. 2007; 97: 1412–1420.
47) Reddy KS. India wakes up to the threat of Cardiovascular Diseases. J Am Coll of
Cardiol 2007; 14: 1370-1372.
48) Campbell MK, Elbourne DR, Altman DG, for the CONSORT Group. CONSORT
statement: extension to cluster randomised trials. BMJ 2004; 328: 702-708.
49) West R, Hajek P, Stead L, Stapleton J. Outcome criteria in smoking cessation
trials: proposal for a common standard. Addiction 2005; 100: 299-303.
50) SRNT Subcommittee on Biochemical Verification. Biochemical verification of
tobacco use and cessation. Nicotine Tob Res 2002; 4:149-59.

APPENDIX-I
PARTICIPANT INFORMATION SHEET
You are invited to take part in the research study: Community based group intervention
for tobacco cessation in rural Tamilnadu: A cluster randomized trial. Before you decide it
is important for you to understand why the research is being done and what it will
involve.
1. What is the purpose of the study?
I am a public health student at Achutha Menon Centre for Health Science Studies,
Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum. I am
supervised by Prof.K.R.Thankappan, Professor and Head of the Achutha Menon Centre
for Health Science Studies. The main aims of the research are:
To study the effects of group intervention and self help materials among
individuals using tobacco in rural areas.
To identify the facilitating factors, barriers and acceptance of these intervention in
rural areas
2. How your village was chosen?
The study will be conducted in Manaparai taluk, Tiruchirappalli district, Tamilnadu.
This taluk was selected because of my convenience and it is the largest taluk in the
district. Out of 97 villages twenty were selected based on their population size. These
twenty villages were divided into two groups by lottery method. One group will receive
the group intervention and the other will receive self help material like pamphlet. Lottery
method ensured that your village had an equal opportunity to be selected in either of these
groups. In each village twenty eligible individuals will be selected.
3. Why have you been chosen?
The study includes men who use any form of tobacco, living in this village and
their age should be between 20 to 40 years of age. Men who are suffering from severe
debilitating illness and who are planning to migrate in the next three months will be
excluded from the study.

4. What will happen to you if you take part in the study?
Your involvement in the study can be divided into three parts.
Baseline interview- Information regarding socio-demographic profile and tobacco
use pattern will be collected. This can take 25-30 minutes. You may even refuse
to answer any question if you are uncomfortable.
Endline survey- Two months after intervention you will be contacted again to
collect information regarding the effects of the intervention.
Intervention – If your village has come under the intervention group than you can
take part in two health education sessions conducted five weeks apart. These
sessions will last for 30 minutes. In these sessions you will be shown pictures
related to harmful effects of tobacco use, challenges in quitting tobacco and
coping skills to prevent relapse. The time and place will be fixed according to
your convenience. You will also receive self help materials like booklet at the end
of the first session.
Intervention – If your village has come under the control group you will receive
self help material regarding harmful effects of tobacco immediately after the
baseline interview.
It is up to you to decide whether or not to take part. If you do decide to take part you
will be given this information sheet to keep. You will also be asked to sign a consent
form. If you decide to take part, you are still free to withdraw from the study at any time
and without any reason.
5. Will your participation in the study be kept confidential?
All information collected during the course of this research will be kept strictly
confidential. All personal information collected will be destroyed at the end of the
research. Your personal information will not be included while writing the report. But
your privacy and confidentiality may be breached while participating in the group
intervention. The group intervention will be conducted in a closed space.

6. What will be the benefit if you participate in the study?
If you participate in this study you can quit tobacco and lead a healthy life. You will
also benefit from a physical screening examination and health advice from a doctor.
7. Who is funding the research?
I am doing this research from my own expenses.
8. What will happen to the results of the study?
The results of the study will be used in my MPH thesis. The findings will be
presented at academic and professional conferences and in academic journals. Findings
from the study will help in designing better tobacco cessation interventions in rural areas
of Tamilnadu.
Contact for further information:
Dr.M.Santhosh Kumar Dr. K. R. Thankappan
MPH Scholar Professor and Head
Mobile No. 08089393594
Achutha Menon centre for Health Science Studies, SCTIMST, Trivandrum, Kerala

APPENDIX-II
Informed consent
Good morning/afternoon/evening,
I am Dr.Santhosh Kumar, currently doing Master of Public Health (MPH) at Sree
Chitra Tirunal Institute for Medical Science and Technology, Trivandrum. I am
conducting a study on “Community based group intervention for tobacco cessation in
rural Tamilnadu: A cluster randomized trial” as a part of the requirement of this course.
The aim of the research is to study the effects of group intervention and self help material
like pamphlet among tobacco users in rural Tamilnadu.
For this study Manaparai taluk, Thiruchirappalli district, Tamilnadu has been
selected. In this taluk 20 villages has been selected based on their population size. These
twenty villages were divided into two groups by lottery method. Lottery method ensured
that your village had an equal opportunity to be in the experimental group or control
group. Ten villages will come under the group intervention arm and other ten villages
will receive self help material like booklet. In each village twenty eligible individuals will
be selected. In the group intervention arm the individuals will receive two sessions of
health education conducted five weeks apart regarding harmful effects of tobacco,
challenges in quitting tobacco and coping mechanisms. You will also receive self help
material like booklet at the end of the first session. Each health education session will last
for 30 minutes and will be conducted at a convenient place and time fixed by you. Self
help materials like booklet will be provided to individuals in the control arm free of cost.
You will be contacted again after two months at a convenient time to study the effects of
this intervention. If you participate in this study, I will help you to quit tobacco and
protect your health from the harmful effects of tobacco. While you try to quit tobacco you
may develop craving, but I will help you to overcome this problem by providing coping
skills. You will also benefit from physical examination and health advice at free of cost.
The information provided by you in the baseline and endline surveys will be kept
confidential and will be used for research purpose only. The information provided by you
will not be disclosed to anyone under any circumstances.
The participation in this study is purely voluntary. You are free to refuse to participate in
the study. You may also withdraw from the study at any time after joining.

Are you willing to participate in this study?
Yes, I am willing to participate in the above mentioned study.
No, I am not willing to participate in the above mentioned study.
Signature/Thumb impression of the participant:
Signature of the investigator:
Time of the day that is convenient for revisit:
Date: Time: Place:
In case of any queries or doubts, please contact me at the following address,
Dr.M.Santhosh Kumar, MPH scholar,
Achutha Menon Centre for Health Science Studies,
Sree Chitra Tirunal Institute for Medical Sciences and Technology,
Trivandrum.
Mobile No. 08089393594
In case if you need further clarifications about the study you can also contact
Dr. Anoopkumar Thekkuveettil,
Member Secretary,
Institutional Ethics Committee (IEC)
Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum.

APPENDIX-III
CHECK LIST – ELIGIBILITY SCREENING FORM
Inclusion criteria:
1. Age between 20 to 40 years
2. Male
3. Resident of this village
4. Current user of any tobacco products
5. Willing to participate in this study
Exclusion criteria:
1. Suffering from debilitating illness
2. Planning for migration in the next three months
Yes No
Name of the Cluster: Form No.
Date: Time:

APPENDIX-IV
Community based group intervention for tobacco cessation in rural
Tamilnadu: A cluster randomized Trial
Achutha Menon Centre for Health Science Studies
Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum,
Baseline Interview Schedule
1. Name and Address :
2. Age in completed years:
3. Marital status:
1- Unmarried 2- Currently married 3-Widower
4- Divorced 5- Separated 6-Others (Specify)___
4. How many years of schooling you have completed?
5. Total number of members in the household
Declaration: The information collected using this schedule will be kept confidential and will
be used for research purposes. Individual information will not be disclosed to anyone under
any circumstances.
Principal Investigator
Name of the Cluster: Identity No.
Interview schedule No
Researcher‟s Name:
Date: Time:

6. Occupation:
1-Government employee 2-Non-government employee 3-Self employed
4-Non-Paid 5-Student 6-Homemaker
7-Retired 8-Unemployed (able to work) 9-Unemployed (unable to work)
9-Others (specify) _____________
7. What was your total household expenditure in the last one month?
8. Religion:
1- Hindu 2-Christian 3-Muslim 4-Others (Specify) ______
9. Community:
1-FC 2-OBC 3-SC 4- Others (specify) ________
10. Did you consume any alcoholic drinks such as wine, beer, whisky, rum, brandy,
toddy or arrack in the last one month? 1-Yes 2-No
11. Do any of your family members use tobacco? 1-Yes 2-No
12. Do any of your friends use tobacco? 1-Yes 2-No
13. What forms of tobacco do you use? (Tick all that apply)
1. Cigarette 2. Bidi 3.Khaini
4.Gutkha
5. Paan masala 6. Betal quid 7. Others (Specify)_________
14. How old were you when you first started using tobacco?
15. How long did you use tobacco?

15. How do you rate your health status in general?
1. Good 2. Fair 3.Poor
16. Do you think using tobacco is harmful to health? 1-Yes 2-No
17. Did anybody advise you to quit tobacco in the last one year? 1-Yes 2-No
If Yes, Who advised you? _______________
18. Did you try to quit tobacco in the last one year? 1-Yes 2-No
19. If yes to Q18, how many attempts did you make to quit tobacco in the last one
year? (Attempt which last more than 24 hours) _______________
20. Do you wish to quit tobacco in the next one year? 1-Yes 2-No
21. How many dips do you place in your mouth per day? (Smokeless tobacco)_____
Signature of the interviewer

APPENDIX-V
Community based group intervention for tobacco cessation in rural Tamilnadu:
A cluster randomized Trial
Achutha Menon Centre for Health Science Studies
Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum, Kerala.
Interview schedule to measure outcome
1. Name: ___________________________
2. Have you ever used any form of tobacco in the last one week?
1-Yes 2-No
3. If yes to Q2, how many cigarettes/Bidis do you smoke per day? (For smokers)
a) 0
b) 1-10
c) 11-20
d) 21-30
e) 31 or more
4. If yes to Q2, how many dips do you place in your mouth per day? (For chewers)
a) 0
b) 1-10
c) 11-20
d) 21-30
e) 31 or more
5. If no to Q2, have you made any attempts to quit tobacco? (which lasts more than
24 hours)
1-Yes 2-No
6. If yes to Q5, How many attempts did you make to quit tobacco? ____________
Thank you
Name of the Cluster: Identity No.
Interview schedule No.
Researcher‟s Name:
Date: Time:

APPENDIX-VI
FAGERSTROM TEST FOR NICOTINE DEPENDECE FOR SMOKERS
A) How soon after you wake up do you smoke your first cigarette/Bidi? (Score)
a) Within 5 minutes (3)
b) 6 to 30 minutes (2)
c) 31-60 minutes (1)
d) After 60 minutes (0)
B) Do you find it difficult to refrain from smoking in places where it is forbidden?
a) Yes (1)
b) No (0)
C) Which cigarette/Bidi would you hate most to give up?
a) The first one in the morning (1)
b) All others (0)
D) How many cigarettes/bidis do you smoke?
a) 10 or less (0)
b) 11-20 (1)
c) 21-30 (2)
d) 31 or more (3)
E) Do you smoke more frequently during the first hours after waking than the rest of
the day?
a) Yes (1)
b) No (0)
F) Do you smoke if you are so ill that you are in bed most of the day?
a) Yes (1)
b) No (0)
Classification of nicotine dependence based on scores:
0-2 Very low dependence 6-7 High dependence
3-4 Low dependence 8-10 Very high dependence
5 Medium dependence

APPENDIX – VII
FAGERSTROM TEST FOR NICOTINE DEPENDENCE –SMOKELESS TOBACCO
A) How soon after you wake up to do you place your first dip? (Score)
a) Within 5 min (3)
b) 6–30 min (2)
c) 31–60 min (1)
d) After 60 min (0)
B) How often do you intentionally swallow tobacco juice?
a) Always (2)
b) Sometimes (1)
c) Never (0)
C) Which chew would you hate to give up most?
a) The first one in the morning (1)
b) Any other (0)
D) How many cans/pouches per week do you use?
a) More than 3 (2)
b) 2–3 (1)
c) 1 (0)
E) Do you chew more frequently during the first hours after awakening than during
the rest of the day?
a) Yes (1)
b) No (0)
F) Do you chew if you are so ill that you are in bed most of the day?
a) Yes (1)
b) No (0)
Classification of nicotine dependence based on scores:
0-2 Very low dependence 6-7 High dependence
3-4 Low dependence 8-10 Very high dependence
5 Medium dependence

APPENDIX – VIII
INTERVENTION TOOLS
Illness narratives
Smoking and heart attack:
Chinnasamy is a 32 year old young man. He is living in a remote village Orangur,
Cuddalore district, Tamilnadu. On one bad morning life became stand still for his whole
family and his dependents. He had severe chest pain with sweating all over his body. He
also had severe vomiting. He was absolutely found to be normal a day before he had this
problem. He has not even gone to a hospital for a head ache in the last ten years. Because
of this severe chest pain he was taken to a nearby hospital. The doctor in the hospital
examined him and told the family members that he was suffering from a massive heart
attack. He referred the patient to a private hospital in Trichy which is 150 Km from this
village. He died on the way due to heart attack.
Why he died due to heart attack in a very young age?
He started his smoking habit at the age of 14 because of the pressure from his
friends. Then onwards he started smoking 2-3 packets per day for the past 18 years. The
toxins from the smoke got deposited in his blood vessels supplying the heart muscles and
he suffered this heart attack. This is the reason for his ill fate at a very young age. The
fate doesn‟t stop with him alone; he left his young wife who was just 27 years old and a 2
year old kid.
Think what will happen to this small kid and this young widow? What will be their
future?
Who is responsible for his death?

Hans and Oral cancer:
Periyasamy is a 55 year old man. He is residing in a village Thozhudur which is
located near Perambalur. He owned a small Photostat shop and sold SIM cards and
Recharge coupons for cell phones. He was married and has three sons. He was using betel
quid and Hans for 20 years. He was advised by his doctors whenever he fell ill to quit
tobacco but he continued his habit thinking that it is not harmful to health. Five years
back he developed hardness in his right cheek. The swelling increased in size within three
months. The local doctor referred him to a dental hospital in Chennai where it was
confirmed as cancer cheek. He underwent surgery and radiotherapy. The total cost for the
treatment was around 2.5 lakhs. He had to sell his small shop to meet his medical
expenses. Even after surgery he was not able speak properly, he can drink only liquid
food. His life became miserable since his small grand daughter was not willing to come
near him because of his ugly face. He died after two years because of the spread of the
cancer. This is the tragic story of a person who used Hans.

Pictures used in this intervention:
Whether costly or cheap all are harmful to health
Source: http://www.inctr.org
Source: http://screening.iarc.fr
Betal quid
Normal teeth and smokers teeth
Source: https://online.epocrates.com/
Oral leukoplakia
Source: www.screening.iarc.fr
Oral erythroplakia
Source: http://screening.iarc.fr
Oral submucosal fibrosis
Source: www.tobaccohealthconcerns

Source: www.knowledgebase-script.com
Smoking and stroke
Source: www.1aim.net
Smoking and heart attack
Source: www.kingcounty.gov
Normal lung and smokers lung
Smoking and chronic bronchitis
Smoking and Tuberculosis
Smoking and cataract
Source: www.smoke-free.ca
Smoking and impotence
Smoking and gastric ulcer

Source: http://www.itsyourlifefoundation.org
Smoking reduces the life span
Source: WHO
Pregnancy and second hand smoke
Source: WHO
Source: www.asahikawa-med-surger
Thromboangitis obliterans