-
Common Biomechanical Deficiencies Weaknesses Inflexibilities
Postural Deficiencies
The biomechanical deficiencies are listed for precautionary
measures only so they may be identified and possibly corrected in
attempt to prevent athletic injuries during exercise or physical
activity. These deficiencies are possible risk factors for injury
and may only increase injury when combined with other risk factors.
A physician may need to establish if a biomechanical deficiency is
structural, muscular, neuromuscular, or due to some other
pathology. The corrective exercises assume deficiencies are due to
a muscular imbalance (flexibility and strength). Only a qualified
physician should diagnose and give prescription for an existing
injury. In some circumstances, an attempt to correct a
biomechanical deficiency may irritate the injury and prolong
recovery, particularly if certain therapy exercises are used
inappropriately or initiated too soon after an injury has occurred.
Even after an underlying biomechanical deficiencies has been
improved, a preexisting injury may require the attention of a
physical therapist under the advise of a physician to restore total
functionality.
Abdominal WeaknessIncreased risk of lower back injury can occur
during hip flexion, extension, stabilization and back extension
activities. Erector Spinae muscles can hyperextend lower back more
than usual if abdominal muscles are weak. The abdominal muscles
tilt the pelvis forward, improving the mechanical positioning of
the Erector Spinae, specifically when the lumbar spine becomes
straight. When abdominal strength/endurance is not adequate to
counter the pull of the antagonist Erector Spinae under load, these
low back muscles are put at a mechanical disadvantage (active
insufficiency) further placing additional stresses on these very
same lower back muscles. Iliopsoas can pull on the spine during hip
flexor activities if the abdominal muscles are weak. Risk is
compounded when abdominal weakness is combined with hip flexor
inflexibility.
Examples of affected exercises: Squat Deadlifts Military Press
(standing) Lying Leg Raise (full extension): hands may
be placed under lower portion of glutes to decrease tilt of
pelvis and subsequent hyperextension of spine.
Example preventative / corrective exercise: Crunch
1 / 16
Object 1
-
Hamstrings WeaknessIncreased risk of knee injury (instability)
occur during knee extension activities, specifically when knees are
flexed more than 90. When hip and knee are simultaneously extending
during a compound movement, hamstrings counter the anteriorly
directed forces of Quadriceps. Also see Knee Stability and Angle of
Pull for force vector explanation. Hamstrings / Quadriceps strength
ratios should be greater than 56% to 80% depending on the
population tested.
Examples of affected exercises: Squat Leg Press
Example preventative / corrective exercises: Leg Curls Straight
Leg Deadlift
Supraspinatus WeaknessIncreased risk of shoulder injury during
shoulder flexion and abduction activities, specifically when the
elbow travels below the shoulder during shoulder abduction. Risk is
compounded with a winged scapula condition. Paradoxically, avoiding
full range of motion (i.e. not initiating deltoid exercises from a
fully adducted position) may not allow the Supraspinatus to be
fully strengthened since it is more fully activated at these
initial degrees of shoulder abduction/flexion. Once an injury has
occurred, however, range of motion is typically restricted on the
shoulder press. See shoulder abduction force vector diagram.
Examples of affected exercises: Shoulder Press Upright Row
Lateral Raise
Example preventative / corrective exercises: Front Lateral Raise
Lying Lateral Raise
2 / 16
-
Infraspinatus WeaknessIncreased risk of shoulder injury occurs
during throwing and shoulder transverse flexion and transverse
adduction activities, particularly when the elbow travels behind
shoulder. Risk is compounded with a protracted shoulder girdle. The
strong stabilizing and dislocating forces of the Pectoralis Major
(Sternal and Clavical) is counteracted by the Infraspinatus, Teres
Minor, and to a lesser extent, the rear deltoid and long head of
the triceps brachii. This counter force is most crucial during:
initiation of a transverse adduction/flexion elbows behind
shoulders stabilizing force
during the end of a throwing movement high deceleration
dislocating forces required of the posterior cuff can
cause breakdown in their tendons near their humeral
attachment.
External rotation-muscular endurance / internal
rotation-muscular endurance should be greater than 70%.
Examples of affected exercises with suggestions for high risk
individuals:
Bench Press : Bring bar lower on chest, keeping elbows closer to
sides.
Chest Press : Elevate seat so elbows are closer to sides Range
of motion may need to be limited so elbows do not go behind
shoulders
Example preventative / corrective exercises: Lying External
Rotation Rows
Erector Spinae WeaknessIncreased risk of lower back injury occur
during lumbar spine extension or stabilization activities. Back
extension exercises involving complete lumbar spine range of motion
have demonstrated primarily excellent or good results for those
with chronic lower back pain. Excellent or good results by
diagnosis: 76% Mechanical / Strain, 72% Degenerative, 78% Disc
Syndrome, 75% Spondylo. In contrast, McGill condemns the use of
isolated lumbar spine exercise apparatuses and argues erector
spinae endurance is more important than strength. See Low Back
Debate.
Examples of affected exercises Straight Leg Deadlift Squat
Deadlift
Example preventative / corrective exercises: Back Extension
(novice) Cable Row (with spinal articulation) (novice to
intermediate) Stiff Leg Deadlift (advanced)
3 / 16
-
Vastus Medialis WeaknessIncreased risk of knee injury
(chondromalacia) occurs during knee extension activities. The
patella becomes laterally displaced with the pull of the vastus
lateralis. This patella tracking problem can produce wear on the
inferior patellar surface. Greater pain is usually experienced
during leg extension activities in which the knee is a greater than
a 20 to 30 degree angle. Avoiding full range of motion (i.e. not
locking out) during Quadricep exercise may not allow the Vastus
Medialis to be fully strengthened since it is more fully activated
at these final degrees of knee extension.
Examples of affected exercises: Leg Press Squat Leg
Extension
Example preventative / corrective exercises: Single Leg
Extensions (last 20 degrees of extension) Leg Press (last 20
degrees of extension)
Hip Abductor WeaknessOne hip can sag when weight is shifted to
one leg. Possible increase risk of Iliotibial band friction
syndrome (ITBFS) when combined with Gluteus Maximus and/or Tensor
Fascia Latea Inflexibility (Fredericson, et. al. 2000).
Examples of affected exercises: Lunges | Step-Ups Running |
Stair Climber | Gauntlet | Elliptical
Example preventative / corrective exercises: Lever Seated Hip
Abduction Eventually reintroduce effected exercises in a
progressive manor
4 / 16
-
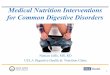
AHIP external rotators
Other Names Six Deep Lateral Rotator Hip Muscles
Heads1. Piriformis 2. Gemellus Superior 3. Obturator Internus 4.
Gemellus Inferior 5. Obturator Externus 6. Quadratus Femoris
MovementHip
External Rotation [1, 2, 3, 4, 5, 6 ] Transverse Abduction [1, 5
] Internal Rotation [1] (see comments)
AttachmentsOrigin
Sacrum Anterior [1 ] Sacrotuberous Ligament [1 ]
Ischium Posterior Portions
Ischial Spine [2 ] Ischial Tuberosity
Posterior Portion [4 ] External Border [6 ]
Obturator Foramen [5, 6 ] Ischium and Pubis
Inside Surfaces and Obturator Membrane [3 ]
5 / 16
-
Insertion
Femur Greater Trochanter
Medial Surface [2, 3, 4 ] Superior/Medial Surface [1 ] Posterior
Surface
Quadrate Tubercle [6 ] Trochanteric Fassa [5 ]
CommentsGemellus Superior [2 ] and Gemellus Inferior [4 ] also
known collectively as Gemelli. Insertion of piriformis is high up
on greater trochanter, so it assists in external rotation from
anatomical position, but when it hip is flexed, piriformis assists
in internal rotation of hip.
6 / 16
-
COMMON ORTHOPAEDIC INFLEXIBILITIESHamstrings Inflexibility
Increased risk of lower back injury during hip extension
activities when knees are straight. If hip flexion (eccentric phase
of hip extension), is inhibited by hamstrings inflexibility, the
lumbar spine may compensate by flexing more than usual. The risk of
injury is increased if the lumbar spine is not accustomed to this
movement or workload. Also see Active Insufficiency.
Examples of affected exercises: Straight Leg Deadlift Good
Morning Barbell Bent-over Row
Example assessments Active Lying Knee Extension Test Passive
Lying Leg Lift Test
Example preventative/corrective exercise: Seated Hamstrings
Stretch Lying Hamstrings Stretch
Gluteus Maximus or Adductor Magnus Inflexibility
Increased risk of lower back injury during hip extension
activities when knees are bent. After complete flexion of the hip
(eccentric phase of hip extension), the lumbar spine will flex if
movement is continued. The risk of injury is increased if the
lumbar spine is not accustomed to this movement and workload. Until
flexibility can be restored, recline leg press back support to
furthest position and base hip flexion range of motion criteria
just before hips tilt. Also see Full Squat Flexibility Q&A.
Examples of affected exercises: Leg Press Squat Single Leg
Squat
Example Assessment Deep Squat Test
Example preventative/corrective exercise:
Glute Stretch Adductor Magnus Stretch
Hip Flexor InflexibilityIncreased risk of lower back injury
during hip flexion and extension and overhead standing activities.
During
7 / 16
-
extension activities, the lower back can hyperextend more than
usual if the hip cannot fully extend. During hip flexion
activities, the Iliopsoas can hyperextend spine during hip flexor
activities. Risk is compounded when hip flexor inflexibility is
combined with abdominal weakness.
Examples of affected exercises: Military press (standing)
Decline Sit-up Lunge (rear leg) Lever Back Extension (fulcrum near
hip)
Example assessments Lunge Test Thomas Test
Example preventative/corrective exercises: Kneeling Hip Flexor
Stretch Quadriceps Stretch
Shoulder Transverse Abduction / Transverse Extension
InflexibilityTypically due to insufficient flexilibility of
pectoralis muscles. Results in decreased range of motion during
chest exercises. High risk for behind the neck exercises
particularly when combined with external shoulder rotation
inflexibility. exacerbated and often accompanied by protracted
shoulders girdle. Excluding cases with particular orthopedic
problems (e.g.: infraspinatus weakness), participants should be
encouraged to perform chest exercises through THIER full range of
motion; shoulder transverse extension / hyperextension until a
slight stretch is felt. Since the shoulder can typically
hyperextend further than it can transverse extend, the exerciser
performing a bench or chest press will be able to bring bar closer
to body when elbows are positioned closer to body (shoulders more
abducted).
Example of affected exercises: Bench Press Chest Press Chest
Flies Behind Neck Shoulder Press Rear Pull-down
Example assessment Passive Chest Flexibility Assessment
Example of preventative/corrective exercises: Straight Arm Chest
Stretch
Shoulder FlexionIn ability to raise arm forward overhead or
undue exertion required position arm in vertical position.
8 / 16
-
Examples of affected exercises:
Dumbbell Shoulder Press Cable Shoulder Press Overhead Triceps
Exercises Overhead Squat Power Clean
Example assessments Shoulder mobility (open
hands) Shoulder mobility (closed
hands) Prone Shoulder Flexion Overhead Deep Squat
Example of preventative/corrective exercises: Bent-over Lat
Stretch (on chair or bench) Wall Lat Stretch Overhead Squat
Dumbbell Shoulder Press
Shoulder External Rotation InflexibilityIncreased risk of
shoulder injury during activities involving external rotation of
the shoulder. Risk is compounded with a winged scapula condition or
kyphosis. Until full range of motion is restored, individuals with
external rotation inflexibility should be advised to perform
pull-downs and shoulder press with the bar in front of the head.
Those with more severe cases should perform overhead presses with
angled back support (eg: 100-110 incline bench).
Examples of affected exercises: Behind Neck Shoulder Press Lever
Shoulder Press (torso upright
facing away from lever) Rear Pull-down Lever Fly (on pec deck)
Overhead Squat Snatch
Example assessment Passive Shoulder External Rotation
Assessment
Example preventative/corrective exercises: Subscapularis Broom
Stick Stretch
9 / 16
-
Shoulder Internal Rotation InflexibilityIncreased risk of
shoulder injury during activities involving internal rotation of
the shoulder. When the shoulder is flexed and internally rotated,
pressure can be created between the insertion of the supraspinatus
and acromion or coracoacromial ligament. Incidentally, pain in this
position can be indicative of impingement or rotator cuff
tendinitis (Hutton & Julin 1997). Tight internal rotators can
contribute to protracted shoulders.
Examples of affected exercises: Upright Row (narrow grip)
Example assessment Passive Shoulder Internal Rotation
Assessment
Example preventative / corrective exercises: Infraspinatus Broom
Stick Stretch
Iliotibial Band TightnessIncreased risk of lateral knee injury
during knee extension activities. Iliotibial band friction syndrome
(ITBFS) is a cause of diffuse tenderness over the lateral knee.
While weight bearing during knee flexion, the Tensor Fascia Latea
contracts to assist the other hip abductors stabilize the pelvis
from lateral movement and the Gluteus Maximus extends the hip for
forward locomotion. Both the Tensor Fascia Latea and the Gluteus
Maxiums can place tension on the Iliotibial tract which produces
repetitive friction on the lateral epicondyle. Furthermore, hip
abductors weakness can exacerbate this pull on the Iliotibial tract
by allowing the hip to sag slightly when standing on a single leg,
or during locomotion (Fredericson, et. al. 2000).
Examples of affected exercises: Lunges Step-Ups
Example assessment Ober's Test
Example preventative / corrective exercises:
Tensor Fasciae Latea Stretch
Gluteus Maximus Stretch Lever Seated Hip
Abduction
Ankle Dorsiflexion InflexibilityDorsiflexion flexibility is
required during the lower phases of the squat and leg press, so
Ankle Dorsiflexion inflexibility can make it difficult to perform
squat and leg press exercises in full range of motion. If the range
of motion of the ankle is limited, hip flexion may be exaggerated
and knee flexion is often inhibited. To maintain normal range of
motion in both the hip and knee, the heel may have a tendency to
leave the
10 / 16
-
floor or platform.
Examples of affected exercises with suggestions for affected
individuals until range of motion is restored
Leg Press : place feet higher on the platform Squats : wider
stance or elevate heels slightly on board or weight plates Range of
motion may need to be restricted so heels do not raise at lower
portion of
exercise Example Assessments
Deep Squat Active Bent Knee Foot Raise Test
Example preventative / corrective exercises: Gastrocnemius
Stretch Soleus Stretch Calf Raise Calf Press
Plantar Fasciitis & Foot Dorsiflexion InflexibilityHigh
incidences of plantar flexion strength deficits and dorsiflexion
range of motion limitations are associated with Plantar Fasciitis.
Plantar Fasciitis is a common overuse syndrome occurring in runners
and walkers. This syndrome is associated with microtears in the
plantar fascia at its insertion into the calcaneus. If allowed to
progress to the point when bone spur (calcium deposit) forms on the
underside of the calcaneous (heel bone), surgery may be required.
Individuals with excessive pronation (feet rolling inward), flat
feet, or knocked knees have increased risk for plantar fasciitis.
These conditions force the plantar fascia to stretch more during
weight bearing activities placing increased pressure where it
attaches to the heel bone. High arches are also associated with
plantor faciitis.
Examples of affected exercises
Walking (particularly upon awakening) Running Jumping
Example Preventative Exercises
Seated Plantar Fasciitis Stretch Can Foot Roll
11 / 16
-
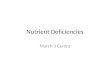
COMMON POSTURAL DEFICIENCIESStanding Postural Muscles
The diagram to the right illustrates how the body is held erect.
The thick black lines represent the principal muscles involved in
standing. The vertical dotted line indicates the center of gravity.
Note this line falls behind the axis of rotation of the hip and in
front of the knee. This renders the ligaments of the joints tense,
which are represented by dotted lines passing in front of the hip
(ilio-femoral) and behind the knee (posterior ligament).
Posterior Pelvic TiltSometimes referred to as flat back,
posterior pelvic tilt involves the reduction of the natural lumbar
curvature. This posture is characterized by the shortening of the
hip extensors (Hamstrings & Gluteus Maximus inflexibility),
tight abdominals, and lax hip flexors. Sitting on the back of the
hips may indicate a posterior pelvic tilt. It is rarely brought
about by lack of muscular strength. The posterior pelvic tilt is
less common as the anterior tilt as seen with lordosis.
Examples of affected exercises: Leg Press Squat Straight Leg
Deadlift
Example preventative / corrective exercises: Hip Flexor: Lever
Hip Flexion Hamstrings: Lying Hamstring Stretch Gluteus: Seated
Glute Stretch Abdominal: Abdominal Stretch
LordosisPelvis is positioned forward and downward. Hips are
slightly flexed and lumbar spine is excessively hyperextended. Hip
flexors, erector spinae are short. Abdominal, hamstrings, gluteus
maximus muscles may be weak. Increased risk of lower back injury
during standing or lying hip extension, flexion, or stabilization
activities, and weighted overhead activities. See abdominal
weakness and hip flexor inflexibility.
Examples of affected exercises: Squat Hack Squat , Roman Chair
Sit-up Military Press (standing)
12 / 16
-
Example preventative / corrective exercises: Hip Flexor:
Kneeling Hip Flexor Stretch Erector Spinae: Lower Back Stretch
Abdominal: Crunches Hamstrings: Leg Curl Gluteus: Seated Leg
Press
KyphosisExaggerated anterior-posterior curvature of the
vertebral column, most often involves an excessive forward bending
in the thoracic area. Kyphosis occurs in older adults, particularly
women with osteoporosis and osteoarthritis. Kyphosis is sometime
accompanied with other posterior problems such as posterior or
anterior pelvic tilt (compensates for altered line of gravity) and
protracted shoulder girdle (unrelated). Kyphosis makes it difficult
to include overhead exercises particularly when combined with a
winged scapula condition or shoulder external rotation
inflexibility.
Examples of affected exercises: Shoulder Press Seated Triceps
Extension Front Squat Overhead Squat
Corrective exercises for gravity induced kyphosis: Strengthening
of thoracic vertebral column extensors Stretching of thoracic
vertebral column flexors
Forward Head PostureAn anterior positioning of the cervical
spine is characteristic of forward head posture, or protracted
neck. Forward head posture may make it more difficult to perform
exercises with the bar in front of head or neck. Evaluate neck
position at night since elevating head too high with additional
pillows may act as a continuous neck stretch throughout the evening
exacerbating the forward head posture.
Examples of affected exercises: Shoulder Press
Corrective exercises for gravity induced kyphosis: Strengthening
of cervical vertebral column extensors
Isometric Neck Retraction Stretching of cervical vertebral
column flexors
Neck Retraction
13 / 16
-
Winged ScapulaMedial border or inferior angle of scapula
protrudes slightly from body. A winged scapula condition may be
accompanied by a protracted shoulder girdle. Risk of shoulder
injury is compounded with a supraspinatus weakness or an external
shoulder rotation inflexibility. Because of the forward tilt of the
scapula, complete flexion or external rotation of the shoulder may
be seemingly restricted. A winged scapula condition indicates a
serratus anterior weakness. The rhomboids may be weak and the
pectoralis minor may be short. A winged scapula is considered
normal posture in young children, but not older children and
adults.
Examples of affected exercises: Shoulder Press Pullovers
Pull-downs
Example preventative / corrective exercises: Incline Shoulder
Raise Cable Row Pectoralis Minor Stretch Wall Lat. Stretch
Protracted Shoulder GirdleThe shoulders are pulled forward.
Medial border of the scapula may also protrude slightly from body.
Increased risk of shoulder injury during shoulder transverse
flexion and transverse adduction activities, specifically when
elbow travels behind shoulder. Scapula protraction can also
decrease width of subacromical space, possibly increasing risk of
subacromical impingement (Solem-Bertift E, et al. 1993). In both
cases, risk of shoulder injury is compounded with a infraspinatus
weakness. Possible limited range of motion during retraction of the
shoulder girdle. A protracted shoulder girdle may be accompanied by
a winged scapula condition or transverse adduction / flexion
inflexibility. The subscapularis and Pectoralis minor and
clavicular & sternal heads of the pectoralis major muscles may
be short. The trapezius (middle fibers) and particularly the
rhomboids may be weak if the medial borders of the scapula also
protrude slightly from body.
14 / 16
-
Examples of affected exercises: Bench Press Chest Press Flies
Barbell Hack Squat Upright Row (particularly close grip) Front
Lateral Raise (with internal shoulder rotation)
Example preventative / corrective exercises: Cable Row or Lever
Row (do not hold protracted position) Doorway Modified Chest
Stretch Wall Shoulder Girdle Stretch Doorway Subscapularis Stretch
Work through full range of
motion on chest exercises just to position that
slight stretch is felt.
If lying on one's side, position upper arm under head (with or
without pillow in between) since lying on one's side with one's arm
down or in front (protracting shoulder girdle) may act as a
continuous stretch throughout the night exacerbating this
condition.
Likewise, those with a protracted shoulder girdle should avoid
stretches that protract the shoulder such as Rear Delt Stretches or
holding a protracted position during rowing resistive
exercises.
Normalizing this postural deficiency can improve mechanics of
the shoulder and provide a fuller appearance throughout the
chest.
ScoliosisMediatorial curve of the vertebral column.
Congenital scoliosis develops before birth and is caused by a
defect in the formation of the spinal column. Either parts of the
vertebrae are missing or vertebrae fail to separate, leading to
asymmetry and unequal growth of the spine. Scoliosis develops
because one side grows more than the other, causing the spine to
curve.
Degenerative scoliosis occurs in adults for two main reasons.
First, scoliosis may have started when the patient was younger
(starting as adolescent idiopathic scoliosis) and may have worsened
with increasing age. The second degenerative, or de novo, type of
scoliosis starts after 40 years old and is thought to be the result
of arthritis or degeneration of the spine, with changes in
alignment caused by degeneration of the discs and the facet joints.
Degenerative curves might also progress a few degrees per year,
particularly if the patient has osteoporosis and a sequential
collapse of the vertebrae.
In about 80% of all scoliosis cases there is no known cause.
This type of scoliosis is called idiopathic scoliosis.
15 / 16
-
Idiopathic scoliosis can be described as early onset or late
onset. It is surprisingly common although most patients need no
treatment or do not realise that they have a curved spine. Curves
measuring up to 11 are considered normal. Observation is the
mainstay of management in most patients, and bracing or plaster
casts are sometimes used. Surgery is reserved for those curves that
are symptomatic or are at high risk of becoming symptomatic because
of the size that they have reached.
The term neuromuscular scoliosis is used to describe curvature
of the spine in patients with any disorder of the neurological
system. Common categories include cerebral palsy, spina bifida,
muscular dystrophies, and spinal cord injuries. In most of these
children the unifying feature is weakness of the trunk. Nerves can
be affected from the brain (eg, cerebral palsy) down to the spinal
cord (eg, poliomyelitis). If the muscles do not work, such as in
spinal muscular atrophy or Duchenne muscular dystrophy, then
scoliosis can develop.
Patients with these conditions often develop scoliosis or
kyphosis (round back), or both. As they grow and their trunk
muscles get weaker, the spine progressively collapses, producing a
long, C-shape scoliosis. The curvature of the spine worsens during
growth spurts. These curves tend to be progressive, with the rate
of progression becoming worse during rapid growth. For children
confined to a wheelchair, progressive curves can affect the child's
ability to be seated comfortably, thereby affecting their quality
of life and function. A progressive or large curve can affect a
childs pulmonary function by leading to collapse of the torso and
raising of the diaphragm, which reduce the space for the lungs.
This reduction in space can manifest itself in recurrent pneumonia
(chest infection).
Scheuermanns kyphosis is a structural curvature of the thoracic
or thoracolumbar spine that develops before puberty and
deteriorates during adolescence. It is the second most common cause
of back pain in children and adolescents with spondylolysis (defect
in the vertebral arch) and spondylolisthesis (displacement of a
vertebra or the vertebral column in relation to the vertebrae
below).
The age at onset is about 1012 years, but a subset of patients
present in adulthood. The condition occurs in 0.4-8.3% of the
population, though its true incidence is probably underestimated
because it is often attributed to poor trunk posture. It affects
equally male and female patients.
Scoliosis can occur as part of a recognised syndrome. For
example, people diagnosed with Marfans syndrome, Rett syndrome, or
Beales syndrome are likely to develop scoliosis.
Extensive research and recent experience of certain physical and
complementary therapists supports ideas around alternative
scoliosis long-term management and possible treatment using
alternative or complementary therapies such as gentle bone setting
or other joint corrections methods. One of the examples of a safe
non-manipulative method is the Dorn Method or Dorn Therapy. Dorn
Method may be the only existing safe method suitable for
non-medical environment which does not involve any manipulations or
forced movements or use of excessive leverage in the process of
correcting alignment of any vertebral joints. It involves active
therapy and self-help routines for long-term management. Dorn
Method can potentially be taught to sensitive carers who could use
it frequently on their family members, clients or patient as
appropriate.
16 / 16
Common Biomechanical DeficienciesAbdominal WeaknessHamstrings
WeaknessSupraspinatus WeaknessInfraspinatus WeaknessErector Spinae
WeaknessVastus Medialis WeaknessHip Abductor WeaknessOther
NamesHeadsMovementAttachmentsCommentsHamstrings
InflexibilityGluteus Maximus or Adductor Magnus InflexibilityHip
Flexor InflexibilityShoulder Transverse Abduction / Transverse
Extension InflexibilityShoulder FlexionShoulder External Rotation
InflexibilityShoulder Internal RotationInflexibilityIliotibial Band
TightnessAnkle Dorsiflexion InflexibilityPlantar Fasciitis &
Foot Dorsiflexion InflexibilityStanding Postural MusclesPosterior
Pelvic TiltLordosisKyphosisForward Head PostureWinged
ScapulaProtracted Shoulder GirdleScoliosis