Embed Size (px)
Citation preview

CNS Drugs 2004; 18 (12): 777-792LEADING ARTICLE 1172-7047/04/0012-0777/$31.00/0
© 2004 Adis Data Information BV. All rights reserved.
Combination Therapy forMultiple SclerosisThe Treatment Strategy of the Future?
Bianca Weinstock-Guttman1,2 and Rohit Bakshi3
1 Baird MS Research Center of The Jacobs Neurological Institute, Buffalo, New York, USA2 Department of Neurology, School of Medicine and Biomedical Sciences, University at Buffalo,
State University of New York, Buffalo, New York, USA3 Department of Neurology, Harvard Medical School, Brigham & Women’s Hospital, Center for
Neurological Imaging, Partners Multiple Sclerosis Center, Boston, Massachusetts, USA
Multiple sclerosis (MS) is an inflammatory autoimmune disease characterisedAbstractby demyelination and axonal loss in the CNS. Although new immunomodulatorytherapies including interferon-β and glatiramer acetate became available duringthe last decade, these therapies are only partially effective. There is a continuingneed to develop more effective treatment strategies to combat the chronic andprogressive aspects of the disease. In view of the complex pathophysiologyunderlying the MS disease process, combination therapy offers a rational thera-peutic approach. Combining immunomodulatory agents with different mechan-isms of action that promote synergistic or additive effects represents an importantobjective in MS therapeutic research. Ultimately, the optimal therapies will likelyinclude strategies that promote repair and limit tissue destruction in combinationwith anti-inflammatory interventions.
1. Introduction and Rationale for some degree of recovery; this is known as relapsing-Combination Therapy remitting (RR) MS.[1] Within 10–15 years, approxi-
mately 50% of patients enter a stage of continuousMultiple sclerosis (MS) is postulated to be a cell- progressive deterioration during which relapses be-
mediated autoimmune disease directed against mye-come less prominent; this is known as secondary-
lin components of the CNS. The last decade hasprogressive (SP) MS.[1] Fifteen percent of patients
been characterised by the discovery of effectivehave continuous neurological deterioration at onsettherapies that alter the natural history of the disease.without superimposed relapses (primary-progres-However, the available therapies are only partiallysive [PP] MS)[1] or rare superimposed subsequentbeneficial and the response to these therapies variesrelapses (progressive-relapsing [PR] MS).[1]
among patients.Recent histological studies of MS lesions indica-Clinical and immunological heterogeneity across
te that myelin destruction is also a heterogeneousMS patients may explain the existence of respondersprocess.[2] The aetiology of MS is believed to beand nonresponders to current therapies. In >80% ofimmunologically mediated and related to genetic,cases, the disease begins with acute relapses, charac-
terised by acute neurological deficits, followed by infectious and environmental influences. Figure 1

778 Weinstock-Guttman & Bakshi
Systemiccirculation
Myelindestruction
CNS
Repair
Antigen-presenting
cell
Auto-reactive
Th0
Auto-reactive
Th1
1
2 3
Th2
4VLA-4
VCAM
MMP9
85
6
IL-2IFNγTNFαLT
7
Th1
Th19
IL-10IL-4{Th2
10
B cell
MFG/micro
MFG/micro
NT3NT4/5NGFBDNF
11
T cell
Walleriandegeneration
Oligo'
Oligo
B cellactivated
{
MHC II
MHC II
MHC II7
7'
10'MFG/micro
IL-1TNFαFree radicals(nitric oxide,superoxide anion)
Blood-brainbarrier
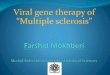
Fig. 1. The pathogenesis and treatment of multiple sclerosis. Circulating autoreactive T lymphocytes (T autoreactive noncommitted cells[Th0]) are activated by superantigens, molecular mimicry or unknown mechanisms (1). Once activated (3), these autoreactive T helper cellsubset 1 (Th1) cells traverse the blood-brain barrier and enter the CNS (4). Local antigen-presenting cells provide the signals necessary tocause activation and clonal expansion of these autoreactive T cells and the secretion of destructive proinflammatory cytokines (5,6,7). Thesecretion of cytokines, including tumour necrosis factor (TNF)-α, lymphotoxin (LT), interferon (IFN)-γ, interleukin (IL)-2 and chemokines (6),results in recruitment of circulating lymphocytes and monocytes and differentiation of recruited monocytes and tissue microglial cells intomacrophages (7). The most important mechanisms of damage to the myelin sheath (bottom figure) involve antibody binding, complementactivation, and macrophage and microglia activation, followed by myelin phagocytosis and release of toxic factors (7’). Oligodendrocyteapoptosis (Oligo’) could be a secondary phenomenon associated with this activation process or can be the primary target of the destructiveprocess, as described in certain cases of primary progressive multiple sclerosis[2] or malignant forms of relapsing-remitting disease.[4] Anti-inflammatory cytokines (IL-10, -4) produced by T helper cell subset 2 (Th2) cells (2,9), serve to inhibit the inflammatory process. Recruitmentof B-lymphocytes (10) and their transformation to plasma cells produces immunoglobulins that can cause complement-mediated demyelin-ation (bottom figure). Neurotrophic factors such as neurotrophin (NT) 3, NT 4/5, nerve growth factor (NGF) and brain-derived neurotrophicfactor (BDNF), which are produced by activated T cells, can positively influence the repair and remyelination processes (11). The putativemechanisms of action of immunotherapies can also be understood by their action on various steps in this complex cascade. IFNβ inhibitsproliferation of autoreactive T cells (3) and inhibits expression of MHC class II molecules (5,7). This results in reduced antigen presentationwithin the CNS and inhibition of matrix metalloproteases [MMPs] (5,8). This is followed by reduced migration of T cells into and through theCNS (8), as well as induction of immunosuppressive cytokines, resulting in attenuation of the inflammatory process (9). Glatiramer acetateis designed to mimic human myelin basic protein by inducing myelin-specific responses in suppressor T-lymphocytes (2), inhibiting specificeffector T-lymphocytes (3) and inducing specific immunomodulatory Th2 cells (1,2,9). The latter enter the CNS and secrete cytokines thatsuppress local inflammation through ’bystander suppression’. Natalizumab binds to α4-β1-integrin very late activation antigen 4 (VLA-4),blocking its binding to vascular cell adhesion molecule (VCAM)-1 and fibronectin receptors (4), thereby preventing leucocyte entry into theCNS (4,5). Minocycline inhibits the action of MMP-9. Since MMPs tear down the basal lamina that lines endothelial cells (8), this inhibitionprotects the integrity of the blood-brain barrier. MFG/micro = macrophage/microglia; Oligo = oligodendrocyte.
outlines the prevailing hypothesis that autoreactive metalloproteinases with disruption of the blood-T lymphocytes orchestrate a complex cascade of brain barrier and invasion of activated T cells intoevents involving the release of proinflammatory the CNS. B-lymphocytes are probably also involvedcytokines, up-regulation of adhesion molecules and
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

Combination Therapy for Multiple Sclerosis 779
in certain forms of the disease through the produc- Currently, there is no proven therapeutic combi-nation protocol for MS, although multiple phase I/IItion of autoantibodies[2,3] (figure 1).studies have tested various strategies. The beneficialSuccessful immunotherapies are able to modifyresults seen in these preliminary studies need to beparticular aspects of this autoimmune inflammatoryconfirmed in larger phase III studies. Designs forcascade (figure 1). Interferon (IFN)-β and gla-such studies must be developed, and increasinglytiramer acetate represent two important immuno-sensitive outcome measures will be required tomodulatory agents that showed a significant clinicalachieve adequate statistical power and a practicalbenefit in large clinical trials of RRMS. Unfortu-sample size. This review summarises results fromnately, these therapies are only partially effectiverecent studies using combination disease-modifyingand a search for more effective therapies is ongoing.therapies in MS.Taking into account the complex pathophysiology
of MS, combining immunomodulatory therapies2. Overview of Disease Modifying
with different mechanisms of action or developing Therapies Available forneuroprotective therapies that are additive to anti- Relapsing-Remitting Multiple Sclerosisinflammatory strategies, represent potentially syner-gistic approaches to treating the disease.
2.1 Interferon (IFN)-βThe current monotherapies approved for thetreatment of MS are only partially effective and their A summary of the effect of immunotherapies inbenefits are confined to the RR form of the disease. RRMS is presented in figure 1. Type I β-interferonsThe heterogeneous treatment responses observed have had a favourable impact on the clinical courseamong patients could be the result of multiple fac- of MS. Large phase III studies have shown thattors, including pharmacogenetic variability, a differ- long-term administration of recombinant IFNβent disease stage (RR vs PR) or heterogeneity of the reduces the number of relapses and slows progres-underlying disease process among patients with an sion of physical disability in patients withapparently similar clinical course. Most therapeutic RRMS.[5-7] Thus, IFNβ-1b (Betaseron®)1 andtrials of combination strategies are designed for IFNβ-1a (Avonex® and Rebif®) have been ap-patients with active RRMS or early SPMS when an proved by the US FDA for the treatment of RRMS.active inflammatory process is believed to be the The studies demonstrated an approximately 30%primary feature. For PPMS or later stages of SPMS reduction in exacerbation (relapse) rate in patientswhen the disease pathophysiology is probably more treated for the study duration. A significant delay indegenerative than inflammatory, other strategies the time to sustained progression in physical disabil-such as neurotrophic or neuroprotective agents will ity was seen in the IFNβ-1a (Avonex®), andprobably be necessary in addition to anti-inflamma- IFNβ-1a (Rebif®) trials.[5,7] All three of the IFNβtory therapies. therapies also showed a benefit on magnetic
resonance imaging (MRI) outcomes.Combination therapies (‘drug cocktails’) areThe biological process underlying the beneficialwidely used in chronic progressive diseases with a
effect of IFNβ therapy in MS is complex (figure 1).complex pathophysiology, such as cancer, autoim-Inhibition of proinflammatory cytokines, inductionmune diseases (e.g. lupus, rheumatoid arthritis), hy-of anti-inflammatory mediators, reduction of cellu-pertension, heart failure and liver disease. Com-lar migration and inhibition of autoreactive T cellsbined therapies should have different mechanismsare key mechanisms (figure 1).[8,9]of action, synergistic or at least additive effects, low
toxicity and the ability to be administered in a practi- The benefit of IFNβ in SPMS is limited to thecal way. initial phase of the disease when patients continue to
1 The use of trade names is for product identification purposes only and does not imply endorsement.
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

780 Weinstock-Guttman & Bakshi
experience relapses and, presumably, when in- ciated with a 29% reduction in the number of relap-flammatory processes dominate. The European ses in the treated group versus placebo.[14]
Study Group of IFNβ-1b (Betaferon®) in SPMS Glatiramer acetate is designed to mimic humanshowed a benefit in delaying the time to disability myelin basic protein and is postulated to induceprogression (p = 0.0008) and a 31% reduced relapse myelin-specific response of suppressor T-lympho-rate (p = 0.0002) in the treated group versus place- cytes and to inhibit specific effector T-lympho-bo.[10] The MRI parameters also showed a signif- cytes[15,16] (figure 1). In addition, recent studies sug-icant benefit with treatment. Unfortunately, the re- gest that treatment with glatiramer acetate can in-sults of a 3-year phase III study (SPECTRIMS [Se- duce specific immunomodulatory T helper (Th)2condary Progressive Efficacy Clinical Trial of cells; these can enter the CNS and secrete anti-Recombinant Interferon-beta-1a in MS]) of IFNβ-1a inflammatory cytokines which suppress local in-(Rebif®) in SPMS did not show a significant benefit flammation by a phenomenon known as ‘bystanderfor the primary outcome measure (time to sustained suppression’ (figure 1). Additional MRI data fromprogression of disability) versus placebo.[11] How- patients treated with glatiramer acetate were ob-ever, a treatment effect was seen on MRI lesions. tained from a multicentre study consisting of a ran-Negative results on clinical (sustained disability) domised placebo-controlled period (9 months) fol-outcomes were also obtained in the North American lowed by an open-label phase.[17] The effect onIFNβ-1b (Betaseron®) study.[12] The IFNβ-1a gadolinium-enhancing lesions in favour of the gla-(Avonex™) SPMS trial (International MS Secon- tiramer acetate-treated group was a delayed effectdary Progressive Avonex Controlled Trial [IM- that developed 6–7 months after the onset of ther-PACT]),[13] in which patients received weekly 60μg apy.intramuscular injections, showed a beneficial effect The available results are highly suggestive of afor treatment versus placebo on sustained clinical complex, different mechanism of action of gla-disability as measured by a relatively new scale, the tiramer acetate versus IFNβ. For example, IFNβ hasMS Functional Composite (MSFC) scale. While shown a more immediate and robust effect on limit-there was no treatment effect using the Extended ing gadolinium-enhancing lesions than glatiramerDisability Status Scale (EDSS), this was not the acetate.[17,18] Because of the different mechanism ofprimary outcome measure and the study was not actions of glatiramer acetate and IFNβ (figure 1),designed or powered to show such an effect. Bene- combining the two appears to be a reasonable thera-fits on MRI lesions were also evident. peutic intervention (see section 3.2.1).
The disparate results reported in these studiesprobably reflect differences in study populations. 2.3 Mitoxantrone (Novantrone®)For example, the Rebif® study[11] had far fewer
Mitoxantrone (Novantrone®) is an anthracene-relapsing patients than the Betaferon® trial[10] (48%dione cytotoxic agent with immunosuppressivevs 70%, respectively). The Rebif® study[11] also hadproperties. Based on the results of a phase III studyfewer patients who had been in a progressive phaseof 194 patients randomised to two treatment groupsof the disease for a longer period of time.(mitoxantrone 12 mg/m2 vs 5 mg/m2) and one place-bo group, mitoxantrone was approved in the US and2.2 Glatiramer Acetate (Copaxone®)Europe for the treatment of worsening RRMS and
Glatiramer acetate is the acetate salt of a mixture SPMS.[19] EDSS score was decreased from baselineof synthetic polypeptides composed of L-alanine, L- by 0.12 in the mitoxantrone 12 mg/m2 group and byglutamic acid, L-lysine and L-tyrosine. Treatment 0.23 in the mitoxantrone 5mg/m2 group, while thewith this medication consists of a daily subcutane- placebo arm showed an increase of 0.23 (p = 0.038).ous injection of glatiramer acetate 20mg. In the Both the number of relapses (p = 0.0002) and sus-pivotal phase III trial, glatiramer acetate was asso- tained progression of disability (p = 0.045) were
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

Combination Therapy for Multiple Sclerosis 781
Table I. Data available on use of combination therapies in multiple sclerosis (MS)
Agent 1 Agent 2 Type of MS Study design Clinical benefit MRI benefit(phase)
IFNβ-1a (Avonex®)[22] Glatiramer acetate (Copaxone®) RR I Trend Trend
Azathioprine (Imuran®) (three IFNβ-1a (Avonex®) RR I/II Trend NRdoses: 50, 100, 150mg)[23]
IFNβ-1a (Avonex®)[24] Azathioprine (Imuran®) 50mg RR II Ongoing OngoingPrednisone 10mg once daily
IFNβ-1a (Avonex®)[25] Methotrexate 20mg orally once RR, SP with I/II Trend Trendweekly relapses
IFNβ-1a (Avonex®)[26] Intravenous methotrexate RW I/II Trend NR
IFNβ[27] IL-2 receptor α-antibody RW I/II NS Trend(Zenapex®)
IFNβ-1a (Avonex®)[28] Cyclophosphamide (Cytoxan®) RW II Trend + Trend +
IFNβ-1b (Betaseron®)[29] Mitoxantrone (Novantrone®) RR, SP I Trend TrendIFN = interferon; IL = interleukin; MRI = magnetic resonance imaging; NR = not reported; NS = nonsignificant; RR = relapsing-remitting; RW= relapsing-worsening; SP = secondary-progressive; Trend = trend to beneficial results (phase I design study); Trend + indicatespreliminary positive results.
significantly lower in the mitoxantrone group. The lower rate of accumulation of T2 lesion load thanclinical benefit of therapy was supported by MRI controls (p = 0.025).[20] A recently completed phaseresults. Significant adverse effects related to mito- II study that evaluated the effect of mitoxantrone inxantrone therapy were nausea, hair thinning, ame- PPMS did not show clinical benefit in this group ofnorrhoea, transient leukopenia and urinary tract in- patients.[21]
fections. Because mitoxantrone is structurally relat-3. Combination Therapiesed to anthracycline agents with well established
cardiotoxicity, cardiovascular function was closelyA summary of the currently available data onmonitored during the study. No patient showed clin-
combination therapies in MS is presented in table I.ical evidence of congestive heart failure. However,It should be emphasised that many of the combina-because the cardiotoxic effect of mitoxantrone istion studies discussed below have the disadvantagedose related, long-term clinical use of this agentof lacking control groups to determine if the patientsrequires caution; the lifetime cumulative dosagewho received combination therapy would have doneshould not exceed 140 mg/m2.just as well as those left on monotherapy or those nottreated at all.2.4 Summary
The currently available disease-modifying treat- 3.1 Definition of ‘Breakthrough Disease’ments for MS are only partially effective and appearto exert their maximum benefit in reducing active Unfortunately, there are many MS patients re-inflammatory components of the disease, which ap- ceiving active monotherapy who still experiencepear to be less prominent as the disease progresses. relapses or show continuous neurological deteriora-Furthermore, no effective therapies are available for tion and progressive MRI lesions and brain atrophy.PPMS. A recent, large, 3-year, multicentre study Usually an immunological steady state associatedusing glatiramer acetate in PPMS was discontinued with a full clinical therapeutic effect is considered tobecause of projected negative results at the 2-year be reached within 6 months to 1 year in patientstimepoint. Another phase II study using 2-weekly taking IFNβ or glatiramer acetate therapy. There-intramuscular doses of IFNβ-1a (30 and 60μg) in fore, following the initiation of a monotherapy ap-PPMS showed no efficacy on sustained progression proved for MS (i.e. IFNβ or glatiramer acetate),of disability, although patients receiving 30μg had a clinical and MRI responses should be monitored
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

782 Weinstock-Guttman & Bakshi
closely (i.e. clinically every 6 months and MRI weekly group were dominated by differences in thefirst 24 weeks.probably annually). Patients experiencing clinical
and MRI activity over this period are likely to be Furthermore, the reported incidence of neutralis-experiencing incomplete therapeutic responsive- ing antibody titres ≥20IU published in large-scaleness. Another term often used to define the situation trials was substantially higher with frequent subcu-in this group of unresponsive/partially responsive taneous administration (27–38% for Betaseron® andpatients is ‘breakthrough disease’ and we will con- 13–25% for Rebif®) compared with Avonex®tinue to use this term throughout the remainder of (2–5%). Persistently high neutralising antibodythis article. While there is no accepted optimal al- levels (e.g. >20IU) have been associated with de-gorithm for managing breakthrough disease, logical creased biological efficacy on both clinical groundssteps are suggested below. (relapse rate) and MRI parameters.[32-35] To shed
more light on the controversial area of the relevanceThe first step is to increase the frequency of IFNβof neutralising antibodies, a consensus panel[34] wastherapy (i.e. switch from once a week Avonex® torecently convened on behalf of The Consortium ofthree times weekly Rebif® or every other dayMS Centers. The panel was comprised of 33 partici-Betaseron® injections). Although some data supportpants from the US, Canada, Europe and Israel. Alla short-term advantage with respect to relapses fol-persons who had published in this field and repre-lowing more frequent administration of IFNβ ther-sentatives from large academic MS programmesapy, the reported magnitude of the potential advan-were invited. Consensus statements (>70% agree-tage is small.[30,31] More importantly, the long-termment) developed from this group included: (i) thatadvantages of treatment at higher doses is unprovenhigh levels of neutralising antibodies interfere withand must be weighed against the higher incidence ofbiological activity of IFNβ; (ii) that IFNβ-1b isneutralising antibodies associated with frequent sub-more immunogenic than IFNβ-1a; (iii) that persis-cutaneous administration compared with oncetence of high levels of neutralising antibodies inweekly intramuscular dose regimens. For example,patients with active MS will eventually led to clin-in an open-label, randomised, comparative study ofical evidence of loss of efficacy; (iv) that immuno-two IFNβ-1a preparations,[30] the advantage (withgenicity of neutralising antibodies is a factor thatrespect to effects on relapse) of 44μg administeredshould be considered in the selection of initial ther-subcutaneously three times weekly (Rebif®) com-apy; and (v) that neutralising antibody positivitypared with 30μg administered intramuscularly onceshould urge the clinician to consider discontinuingweekly (Avonex®) observed during the first 24IFNβ. Further work is still required to fully evaluateweeks of therapy (75% relapse-free patients in thethe role of neutralising antibody monitoring in the44μg three times weekly group vs 63% in the 30μglong-term management of patients receiving IFNβ.once weekly group) was diminished during the
second 24 weeks of therapy (62% relapse-free pa- Switching from one monotherapy to another, fortients in the 44μg three times weekly group vs 52% example from IFNβ to glatiramer acetate, is anotherin the 30μg once weekly group). When calculating consideration that should be kept in mind in manag-the difference as annualised relapse rate per patient, ing breakthrough disease, particularly for patientsthe significant difference at 24 weeks (0.29 in the with sustained positive neutralising antibody titres44μg three times weekly group vs 0.40 in the 30μg ≥20IU. Switching from glatiramer acetate to IFNβ isonce weekly group; p = 0.022) became nonsignifi- also an option, particularly given the rapid and ro-cant at 48 weeks (0.54 in the 44μg three times bust effect of IFNβ on inflammatory activity asweekly group vs 0.64 in the 30μg once weekly measured by MRI.[18] However, combination ther-group; p = 0.093). Thus, it seems that the effects apy should be strongly considered for patients withfavouring the 44μg three times weekly subcutane- breakthrough disease who are neutralising-antibodyous group versus the 30μg intramuscularly once negative because this type is seen as a more com-
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

Combination Therapy for Multiple Sclerosis 783
plex, difficult-to-control disease stage, requiring a tained funding from the National Institutes of Healthmore active, broader therapeutic intervention. and is currently in the process of enrolling approxi-
mately 1200 patients at >70 centres.A third approach is to add immunomodulatory orcytotoxic agents shown to have a beneficial effect as
3.2.2 IFNβ and Azathioprinemonotherapy in MS to IFNβ or glatiramer acetateAzathioprine is a purine analogue with immuno-therapy. Small phase I/II combination therapy stud-
modulatory effects on both T and B cells. It has beenies (see section 3.2) have suggested a beneficialshown to be beneficial in RRMS but less efficient ineffect of certain combinations; based on these en-preventing disease progression.[39] Azathioprine cancouraging preliminary data, large clinical trials arebe considered as a therapeutic option in patientsongoing to confirm their efficacy. In the future,with RRMS who do not respond to IFNβ or gla-neurotrophic or neuroprotective agents are also like-tiramer acetate. The results of an open pilot studyly to serve as add-on therapy to anti-inflammatory(ERAZISMUS [Early Azathioprine versus Beta-agents.Interferon treatment in Multiple Sclerosis]), whichcombined azathioprine with Avonex® were present-3.2 Combination ofed at the 9th Annual Meeting of the EuropeanImmunomodulatory AgentsNeurological Society.[23] The study included 30 pa-
3.2.1 IFNβ and Glatiramer Acetate tients with RRMS who had received azathioprine forat least 6 months prior to enrolment (mean of 4IFNβ and glatiramer acetate are approved in theyears). Three different doses of azathioprine wereUS and most European and Asian countries for theassigned: 50mg, 100mg and 150mg. Patients receiv-treatment of RRMS. Therefore, combining theseing azathioprine were started on additional weeklytwo products and their different mechanisms of ac-Avonex® injections for 4 months. The study showedtion appears logical. However, although preliminarysafety and tolerability of this combination, pavingin vitro data demonstrated an additive effect of thethe way for phase III studies.two products,[36] concerns about an antagonistic
interaction were raised by supplementary data ob- Preliminary results from an ongoing study oftained in animal models.[37] More recent studies IFNβ in combination with azathioprine and low-support the notion that glatiramer acetate and IFNβ dose corticosteroids for RRMS appear promising.[24]
appear to interact antagonistically.[38] These prelim- Half of the 183 planned patients have already beeninary concerns highlight the need for well designed, enrolled. Patients were randomised into threecombination clinical studies. groups: (i) IFNβ + azathioprine 50 mg/day + predni-
sone 10mg every other day; (ii) IFNβ + azathioprineLublin et al.[22] presented preliminary results of a50 mg/day + placebo corticosteroids; or (iii) IFNβ +phase I study of 33 patients with RRMS who wereplacebo azathioprine + placebo corticosteroids. Thereceiving IFNβ–1a (Avonex®) therapy for at least 6initial results after 1 year showed a decrease inmonths. Daily glatiramer acetate injections wererelapse rate from 1.85 ± 0.53 to 0.57 ± 0.86 (p <added while Avonex® was continued. The results0.05) and a change in EDSS from 1.97 ± 0.76 to 1.78suggested that the combination was safe, and there± 0.87 in the whole group (the blinding was notwas a trend towards a decrease in mean gadolinium-broken). It will be interesting to see the full resultsenhancing lesions from 0.83 ± 2.2 at baseline to 0.44of this study when completed.± 1.0 after 6 months of combination therapy. Some
patients continued in the study for an additional 6 Another small study, using IFNβ-1b and azathio-months and showed continuing clinical and MRI prine 150 mg/day combination therapy in ten pa-stability. However, for a definite understanding of tients with SPMS who continued to have attacks orthe effects of combined therapy with IFNβ and disease progression despite IFNβ therapy, showed aglatiramer acetate, a large phase III study is re- decrease in the number of attacks and MRI lesionquired. Fortunately, such a trial has recently ob- load, although there was no benefit on clinical dis-
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

784 Weinstock-Guttman & Bakshi
ease progression.[25] The combination was generally ACT (Avonex Combination Therapy) study willwell tolerated, although strict laboratory monitoring assess the benefit of Avonex® combined with week-was recommended because lymphopenia occurred ly oral methotrexate 20mg versus three other treat-at least once in all patients. ment arms: (i) Avonex® + placebo; (ii) Avonex® +
bimonthly intravenous corticosteroids; and (iii)3.2.3 IFNβ and Methotrexate Avonex® + bimonthly intravenous corticosteroids +Methotrexate is an inhibitor of dihydrofolate re- weekly oral methotrexate. The study will enrol pa-
ductase. At high doses, methotrexate is an anti- tients with RRMS who are experiencing break-mitotic agent used in cancer chemotherapy proto- through disease as defined by continuing relapses orcols. In low doses, methotrexate is an immuno- active (enhancing) MRI lesions despite 6 months ofmodulatory and anti-inflammatory agent with inhib- Avonex® therapy.itory effects on both cell-mediated and humoral A study has been performed evaluating the com-immune mechanisms. When given in low doses bination of IFNβ with intravenous methotrexate.[26]
(7.5mg weekly), oral methotrexate has been shown The objective of this study was to assess the safetyto slow disease progression in patients with progres- and efficacy of bimonthly high-dose intravenoussive MS in a phase II study.[40,41] Potential liver methotrexate with leucovorin rescue, in combina-toxicity and bone marrow suppression related to tion with Avonex®, in patients with worsening-methotrexate necessitate monthly blood test moni- relapsing (WR) MS. The group that conducted thistoring in patients taking this agent. study had previously shown that use of intravenous
Calabresi et al.[42] recently presented the results methotrexate leads to stability in patients withof an open-label phase I/II clinical trial using a WRMS. In the current study,[26] 15 patients withcombination of Avonex® and oral methotrexate. WRMS despite receiving Avonex® for at least 6The primary aim was to determine whether weekly months were given high dose intravenous methotre-IFNβ injections in combination with weekly oral xate at 2 g/m2 followed by leucovorin rescue. Treat-methotrexate 20mg were safe and well tolerated in ment was administered bimonthly for a total of sixpatients with relapsing forms of MS. The secondary treatments. MSFC scores and the expression ofendpoints were MRI measurements, including the chemokine receptors and intracellular cytokines onnumber of gadolinium-enhancing MRI lesions after peripheral blood T lymphocytes were determined at6 months of combination therapy. Fifteen patients baseline and every 4 months during 1 year of ther-with RRMS (EDSS 0–6.5) were included in this apy. The preliminary data after 1 year of treatmentstudy; inclusion criteria included a history of clinical suggested improvement in MSFC composite scoresexacerbation after receiving Avonex® for ≥1 year (+0.34; p = 0.001) and immunological parametersand/or ≥2 gadolinium-enhancing lesions shown in (significant decreases in expression of the3-monthly baseline screening MRI scans. Patients chemokine receptors CXCR3 and CCR4 as well as awere evaluated clinically on two disability scales, decrease in secretion of proinflammatory TNF-α)the EDSS and MSFC. The study showed that pa- during the combination therapy.[43] The combinationtients remained stable or improved with significant- appears viable in active MS.ly (44%) fewer MRI gadolinium-enhancing lesions.No severe adverse effects were seen; the most com- 3.2.4 IFNβ and Glucocorticosteroidsmon adverse effect was nausea (which affected 80% There is a general consensus that intravenousof patients). In summary, the combination of administration of glucocorticosteroids (usuallyAvonex® and methotrexate appears to be safe over a methylprednisolone 500–1000mg daily for 3–56-month period; initial results suggesting efficacy days) shortens the duration of acute relapses.[44,45]
need to be extended in phase III studies. There is also evidence that similar efficacy can beBased on these results, a large, multicentre, com- achieved with oral administration of glucocorticos-
bination therapy study was recently launched. The teroids.[46] High-dose intravenous corticosteroids
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

Combination Therapy for Multiple Sclerosis 785
can also delay the development of clinically definite (ICAM).[50] Furthermore, addition of prednisoneMS for 2 years following the first attack of optic therapy antagonised the beneficial effect of IFNβ onneuritis.[47] The role of long-term corticosteroid ad- up-regulation of IL-10 and soluble CD95 (alsoministration in the prevention of MS disease pro- known as Fas, a transmembrane molecule that in-gression is still uncertain. A phase II, double-blind duces programmed cell death). These findings em-study comparing the tolerability and efficacy of two phasise the complexity of using combination immu-doses of intravenous methylprednisolone in patients notherapies and the importance of evaluating their inwith relapsing-progressive MS (RPMS) [including vivo effects in well controlled, clinical studies.RRMS patients with incomplete recovery and earlySPMS with still superimposed relapses] found no 3.2.5 Intravenous Immunoglobulinsignificant benefit of treatment for patients who
Intravenous immunoglobulin has been used ef-experienced sustained progression of disability.fectively in various immune-mediated neurologicalHowever, a significant beneficial treatment effectdiseases (e.g. inflammatory demyelinating polyneu-was seen for the preplanned secondary outcome, aropathy, myasthenia gravis and myositis) but itsLog Rank comparison of the survival curves ofvalue in MS is uncertain. Potential immunother-6-month sustained progression of disability in theapeutic mechanisms of action of intravenous immu-two groups (p = 0.003).[48] This finding provided thenoglobulin include blocking the macrophage Fc re-rationale for evaluating the combination of bimonth-ceptor, anti-idiotypic effects and reduction of endo-ly intravenous methylprednisolone with Avonex®thelial cell activation and super-antigen neutralisingversus bimonthly intravenous methylprednisolone,antibodies. Intravenous immunoglobulin also pro-Avonex® and methotrexate in patients with break-motes remyelination in virus-induced experimentalthrough disease (see also section 3.2.3).encephalomyelitis. An Austrian group investigated
A recent randomised, controlled, single-blind, the efficacy of intravenous immunoglobulin5-year, phase II clinical trial of intravenous methyl- (0.15–0.2 g/kg once monthly vs placebo) for 2 yearsprednisolone in patients with RRMS demonstrated and found that treatment with intravenous immu-that long-term administration of high doses of corti- noglobulin therapy led to a decreased EDSS disabil-costeroids may limit clinical and MRI markers of ity score while disability increased in the placebodisease progression.[49] The study compared regular group (–0.23 vs 0.12, respectively; p = 0.008).[51]
pulses of intravenous methylprednisolone (1 g/day Intravenous immunoglobulin therapy was also asso-for 5 days with an oral prednisone taper) given every ciated with a robust reduction in relapse rate versus4 months for 3 years and then every 6 months for the placebo. MRI data from a double-blind, crossoversubsequent 2 years versus intravenous methyl- study of intravenous immunoglobulin (1 g/kg/dayprednisolone only for relapses. Pulses of intrave- for 2 days, monthly for 6 months) in patients withnous methylprednisolone slowed development of T1 RRMS showed fewer enhancing lesions during in-black holes, the rate of whole-brain atrophy and the travenous immunoglobulin treatment compareddevelopment of sustained physical disability. How- with placebo (p = 0.03).[52] There were also moreever, there was no significant difference between patients free of exacerbations in the intravenoustreatment arms in the T2 lesion volume or annual immunoglobulin group than in the placebo group (prelapse rate. = 0.02). However, >50% of patients treated with
intravenous immunoglobulin reported adverseAnother recent article that analysed the effect ofevents (e.g. headache, nausea and skin reactions).IFNβ therapy alone versus a combination of IFNβThese studies suggest that intravenous immu-and prednisone showed that combined therapy didnoglobulin may be partially effective in patientsnot significantly enhance the inhibitory effects ofwith RRMS, although the ideal dose for MS needs toIFNβ on the pro-inflammatory cytokines TNFα,be determined.IL-12, IL-2R and intercellular adhesion molecule
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

786 Weinstock-Guttman & Bakshi
There are no data available on intravenous immu- development of new MRI gadolinium-enhancing le-noglobulin combined with IFNβ or glatiramer ace- sions.[54] In addition, an open-label safety and phar-tate, although in practice, combinations that include macokinetic drug interaction study of a single intra-a monthly infusion of immunoglobulin 0.2–0.4 g/kg venous infusion of natalizumab either 3 or 6 mg/kgare used extensively with anecdotal benefits. Well was conducted in 38 patients with RRMS who weredesigned studies of combination therapies that in- receiving weekly intramuscular Avonex® for atclude intravenous immunoglobulin are warranted; least 3 months.[55] The results indicated that thehowever, the high cost and limited availability of the combination was safe and well tolerated. Based onlatter may become disadvantageous. these preliminary data, a large phase III, combina-
tion study of IFNβ-1a (Avonex®) weekly combined3.3 Combination of a Broad Immunotherapy with monthly intravenous natalizumab (300mg) haswith a More Specific Agent been initiated. Enrolment of 1200 patients with
RRMS who continue to experience relapses despite3.3.1 Avonex® and Natalizumab (Antegren®) at least 1 year of Avonex® therapy has been com-Natalizumab is a recombinant humanised anti- pleted and results are expected in 2005.
α4-integrin antibody that is produced in NSO mu-3.3.2 IFNβ and Daclizumab (Zenapax®)
rine myeloma cells.[53] The α4 integrins are heter-Ten MS patients with an incomplete response toodimeric receptors consisting of an α4 subunit and
IFNβ based on clinical and MRI parameters wereeither a β1 or β7 subunit. Both types of integrin areenrolled in a recent study.[27] Baseline monthly MRIinvolved in leucocyte migration across vascular en-findings over 4 months and immunological para-dothelium and contribute to cell activation and sur-meters were compared with data obtained after 9vival within parenchyma. Natalizumab binds to themonths of combination therapy with IFNβ andα4 subunit of α4-β1-integrin very late activationdaclizumab (IL-2 antibody therapy). The combina-antigen 4 (VLA-4) and α4-β7-integrin on leuco-tion was well tolerated and led to a >50% additionalcytes and blocks the interaction of these integrinsreduction in MRI contrast-enhancing lesions in thewith their ligands (vascular cell adhesion moleculemajority of patients. The therapy did not cause gen-[VCAM] and mucosal addressin cell adhesion mole-eral immunosuppression, nor did it significantly de-cule-1 [MadCAM-1], respectively).[53] Some ofcrease the response of peripheral blood T-lympho-these molecules, such as MadCAM-1, are specificcytes to strong polyclonal stimuli or recall antigens.for the gastrointestinal endothelium. The ability ofDaclizumab appears a promising component ofactivated leucocytes to cross the blood-brain barriercombination therapy for unresponsive active MSand infiltrate the brain parenchyma is considered anpatients although there is no clear data to showimportant step in MS lesion formation. Traffickingwhether the benefits observed should be attributedof leucocytes across the blood-brain barrier involvesto daclizumab alone or to the combination withinteraction of the cell adhesion molecule α4 integrinIFNβ.(which is expressed on lymphocytes and mono-
cytes) with its counter-receptor VCAM-1 in brain 3.3.3 Anti-Matrix Metalloproteinasesendothelial cells and with fibronectin in the extracel- Matrix metalloproteinases (MMPs) are extracel-lular matrix[53] (figure 1). Blockade of these cell- lular matrix remodelling proteases that are impor-adhesion interactions is assumed to inhibit or pre- tant in normal development, angiogenesis, woundvent leucocyte entry into the CNS and limit subse- repair and a wide range of pathological processes.[56]
quent leucocyte activation.[53] MMPs can injure the basal lamina that lines theA phase II study of 213 patients with RRMS and blood vessels, creating deficiencies in the blood-
relapsing SPMS showed that monthly intravenous brain barrier (figure 1). In MS, there is an increasednatalizumab (3 and 6 mg/kg) infused for 6 months production of MMP-9 (also known as gelatinase B),was well tolerated and reduced relapses and the which was recently shown to proteolytically cleave
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

Combination Therapy for Multiple Sclerosis 787
IFNβ, damaging its bioactivity and hence counter- nous methylprednisolone in patients who did notacting its antiviral and immunomodulatory ef- respond to standard IFNβ therapy was recently com-fects.[57] When given in high doses, minocycline, a pleted and presented in preliminary form.[28] Fifty-synthetic analogue of tetracycline used to treat mi- nine patients who developed breakthrough diseasecrobial infections such as acne vulgaris, has been while on IFNβ therapy for at least 1 year wereshown to inhibit potently MMP-9 and MMP-2, re- randomised to either six 1-monthly doses of cyclo-sulting in decreases in MMP activity and levels.[58,59] phosphamide (800 mg/m2) plus intravenous methyl-Treatment with minocycline has also shown a bene- prednisolone or to intravenous methylprednisoloneficial effect in an animal model of MS.[58] These data alone. All patients continued with weekly IFNβprovide a cost-effective, novel mechanism and ratio- injections. Preliminary data suggested that cyclo-nale for treatment of MS with minocycline or other phosphamide infusions were well tolerated and re-gelatinase B inhibitors, alone or in combination with duced the number of gadolinium-enhancing MRIIFNβ. lesions compared with treatment with intravenous
methylprednisolone alone. Pulse cyclophosphamide3.3.4 Phosphodiesterase Inhibition
therapy also decreased clinical disease activity. AtTreatment with the combination of IFNβ-1b
the time of analysis, most of the patients had com-(Betaseron®) and the phosphodiesterase inhibitor
pleted 2 years of follow-up. Baseline gadolinium-pentoxifylline (800mg twice daily) was associated
enhancing MRI status (enhancing vs non-enhanc-with a decrease in adverse events on initiation of
ing) predicted treatment response. A total of 26% ofIFNβ therapy and a beneficial synergistic immuno-
patients receiving cyclophosphamide experiencedlogical effect (decrease in TNFα). These findings
treatment failure, compared with 52% of those re-suggest that this combination may be useful.[60]
ceiving intravenous methylprednisolone alone (p =3.3.5 β2-Adrenergic Agents 0.03). Although the combination of cyclophospha-Other therapies that can be considered as candi- mide and Avonex® appeared to be superior to the
dates for add-on therapy in the treatment of MS combination of intravenous methylprednisolone andinclude β2-adrenoceptor agonists (salbutamol).[61] Avonex® in this study, a treatment period for cyclo-
phosphamide longer than the 6-month protocol is3.4 IFNα and Broad Action probably necessary, especially for patients with theImmunosuppressive Chemotherapies most active disease and continuing gadolinium en-
hancement despite continuous IFNβ therapy.The use of cyclophosphamide, an alkylating
Additional preliminary data from a randomised,agent with potent cytotoxic and immunosuppressivecontrolled study of IFNβ-1a (Avonex®) in combina-effects, for MS has been studied in controlled,tion with either weekly oral cyclophosphamideunblinded trials using intravenous high doses as an(150–200 mg/m2) or placebo in a group of 24 pa-induction therapy or as repeated cycles; these regi-tients with breakthrough disease showed that oralmens have shown benefit in patients with SPMS incyclophosphamide was well tolerated.[67] Oversome[62,63] but not all studies.[64] Cyclophosphamideshort-term follow-up (9 months), patients receivinghas multiple adverse effects, including leucopenia,cyclophosphamide fared better, remaining clinicallymyocarditis, haemorrhagic cystitis and alopecia.stable while the Avonex® monotherapy group con-Therefore, treatment with cyclophosphamide is con-tinued to deteriorate slowly; however, the differencesidered for patients with active disease that has notdid not reach significance.responded to less toxic therapies or which has a
rapidly progressive course.[65,66]3.4.2 IFNβ and Mitoxantrone (Novantrone®)
3.4.1 IFNβ and Cyclophosphamide A small cohort of ten patients with RRMS orA controlled trial of Avonex® combined with six SPMS who had responded incompletely response to
1-monthly cycles of cyclophosphamide or intrave- IFNβ therapy (Betaseron®) was started on an open-
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

788 Weinstock-Guttman & Bakshi
label trial of Betaseron® combined with monthly group receiving lofepramine and phenylalanine. Inmitoxantrone (5 mg/m2).[29] Within 6 months, there another study, treatment with lofepramine and phe-was a decrease in the number of gadolinium-enhanc- nylalanine alone was associated with certain benefi-ing lesions on MRI and in the number of relapses. cial effects on MRI parameters in a small number ofNo severe adverse effects of treatment were seen MS patients compared with placebo.[70] Althoughand the combination appeared safe and beneficial; the cyanocobalamin, lofepramine and phenylalaninehowever, larger long-term studies are required combination may have certain benefits in patientsbefore a final conclusion can be drawn. with MS, additional data demonstrating efficacy
will be necessary before large scale clinical trialsAlthough preliminary data[28,29,65,67] on globallycan be considered.immunosuppressive (chemotherapeutic) agents in
patients with MS with very active disease looks4.2 Complementary andencouraging, it is important to keep in mind thatAlternative Interventionsevolving reports suggest that the process of remye-
lination requires inflammatory T cells and that An increasing number of MS patients use a varie-chronic aggressive nonspecific immunosuppression ty of complementary and alternative interventionmay have undesirable effects on subsequent tissue therapies including oral strategies (herbs, vitamins,repair.[68] The balance between the detrimental in- dietary changes, etc.), alternative medical systemsflammatory effect of T cells versus their influence (acupuncture, homeopathy), relaxation methods andon repair and remyelination is unknown, and there- biofeedback. Rigorous studies of the safety and effi-fore more sensitive and specific methods are neces- cacy of these interventions are therefore necessary.sary to evaluate treatment effects in this complex In addition, the interaction between well accepteddisease. MS disease-modifying therapies and these remedies
are not known. Among the various alternative thera-4. Other Combination Therapiespies, dietary interventions promoting a decrease insaturated fats using unsaturated fatty acid supple-
4.1 Cyanocobalamin (Vitamin B12), mentation have been most closely studied.Lofepramine and Phenylalanine (‘The Cari
4.2.1 Low-Fat Diet with Omega-3 SupplementationLoder Regime’)There is an increasing body of evidence sug-
In a randomised, placebo-controlled, exploratory gesting that there are interactions between thestudy, 138 patients with MS were randomised to immune system and dietary factors although thesereceive intramuscular cyanocobalamin (vitamin relationships are complex.[71] The anti-inflammatoryB12) 1mg weekly with either lofepramine 70mg and paradigm previously described[72,73] in the context ofphenylalanine 500mg twice daily or matching place- dietary lipid modification in a variety of autoim-bo tablets for 24 weeks.[69] This regimen was similar mune diseases suggests an active influence on theto the one promoted by Cari Loder and may be immune system. The best known diet in the contexthelpful by increasing noradrenaline levels. An in- of MS is the low-fat ‘Swank diet’, which has beencrease in noradrenaline levels can be obtained by shown to decrease the number and severity of relap-combining lofepramine, a noradrenaline reuptake ses in RRMS.[74] Additional studies in MS haveinhibitor, with phenylalanine, a precursor of norad- suggested a possible benefit from a low-fat dietrenaline. However, there is no compelling in vitro or supplemented with omega-6 and omega-3 essentialin vivo evidence to support the rationale for this fatty acids.[75] Recently, our group showed in astrategy. In the study referred to above,[69] patients 1-year, phase I/II, randomised, single-blind, control-improved by two points on the Guy’s neurological led study that combining a low-fat diet study anddisability scale after starting cyanocobalamin, and supplemental omega-3 polyunsaturated fatty acidsan additional benefit of 0.6 points was seen in the with long-term IFNβ or glatiramer acetate therapy
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

Combination Therapy for Multiple Sclerosis 789
was well tolerated and may have additive disease- therapeutic value in the treatment of inflammatorymodifying effects compared with standard therapy diseases.[79] Another active line of investigation sug-in patients with RRMS.[76] gests that abnormal iron deposition occurs in the
grey matter of patients with MS.[80] It is not as yet5. Future Candidates for clear whether this iron deposition is an epiphenome-Combination Therapies non or contributes directly to the pathogenesis of
MS through the generation of free radicals, lipidperoxidation and neurotoxicity. Antioxidants in5.1 Infectious Disease Agentscombination with anti-inflammatory interventions(Antiviral, Antibacterial)initiated early in the course of MS represent poten-
Several authorities believe that MS is related to tially appealing therapeutic strategies yet to be test-ongoing or reactivated infection, with several poss- ed.ible microorganisms having been suggested as re-sponsible. Recent studies have implicated both 5.3 Hormonal TherapyHerpes viruses (e.g. human herpes virus [HHV]-6,
Preliminary data using the pregnancy sex hor-Epstein-Barr virus) and the obligate intracellularmone estriol succinate in RRMS showed beneficialbacterium Chlamydia pneumonia in the aetiology ofimmunological and MRI effects.[81] Further largerMS.[77] However, the cause-and-effect relationshipstudies are underway. Combination of hormonalbetween infectious agents and MS pathophysiologytherapy with one of the proven beneficial monother-is not clear.[77] Accumulated diagnostic and epide-apies in MS may be a consideration for future pilotmiological data are compatible with a role for thetrials.Herpes viruses as cofactors rather than aetiological
agents, and recent studies showing early neuronal5.4 Statins
damage in MS patients focus attention on the neuro-trophic α-herpes viruses. Antiviral treatment trials The HMG-CoA reductase inhibitors, or ‘statins’,using safe and effective drugs such as valaciclovir, are orally active cholesterol-lowering drugs that arealone or in combination with proven beneficial ther- relatively well tolerated and have immuno-apies (IFNβ, glatiramer acetate), offer a platform for modulatory effects independent of their cholesterol-testing hypotheses concerning viral involvement in reducing properties.[82,83] A growing body of evi-MS, although preliminary data have been disap- dence indicates that statins also have anti-inflamma-pointing.[78] Phase II studies with anti-chlamydial tory and neuroprotective properties that may be ben-antibacterial combination therapies are underway. eficial in the treatment of patients with MS.[82,83]
Several immunomodulatory properties of statins5.2 Antioxidants may account for beneficial clinical effects such as
decreased leucocyte migration into the CNS, inhibi-The hallmark of brain inflammation is the activa-tion of major histocompatibility complex class IItion of glial cells, especially microglia that produceand costimulatory signals required for activation ofa variety of proinflammatory and neurotoxic sub-proinflammatory T cells, induction of a Th2 pheno-stances, including cytokines and free radicals suchtype in T cells and decreasing the expression ofas nitric oxide and superoxide. It has been suggestednitric oxide and TNFα.[82-84] Statins appear to be athat excessive production of nitric oxide contributesreasonable candidate for future combination trialsto neurodegeneration.[79] Therefore, one potentialwith the available immunomodulatory agents.target for therapeutic intervention that provides
neuroprotection is modulation of pathways asso-5.5 Neurotrophic or Neuroprotective Factors
ciated with nitric oxide generation. The opioid re-ceptor antagonist naloxone and (more particularly) Enhancing myelin repair remains an importantits non-opioid enantiomer (+)-naloxone may be of therapeutic goal in the treatment of MS. The emerg-
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

790 Weinstock-Guttman & Bakshi
2. Lucchinetti C, Bruck W, Parisi J, et al. Heterogeneity ofing heterogeneity of pathology within MS lesions,multiple sclerosis lesions: implications for the pathogenesis of
particularly with respect to variable oligodendrocyte demyelination. Ann Neurol 2000; 47: 707-173. Lucchinetti CF, Mandler RN, McGavern D, et al. A role forsurvival, suggests that therapeutic strategies may
humoral mechanisms in the pathogenesis of Devic’s neuromy-need to be tailored to patient or disease subtypes.[2]elitis optica. Brain 2002; 125: 1450-61
A number of therapeutic strategies have been pro- 4. Barnett MH, Prineas JW. Relapsing remitting multiple sclerosis:pathology of the newly forming lesion. Brain 2004; 55: 458-68posed to enhance myelin repair in the CNS: these
5. IFNB Multiple Sclerosis Study Group. Interferon beta-1b isinclude cell transplantation, growth factors and anti- effective in relapsing-remitting multiple sclerosis: I. Clinical
results of a multicenter, randomized, double blind, placebo-body therapy, each of which has a different effect oncontrolled trial. Neurology 1993; 43 (4): 655-61the cascade of events involved in demyelination and
6. Jacobs LD, Cookfair DL, Rudick RA, et al. Intramuscularaxonal loss. Of these, antibody therapy is the most interferon beta-1a for disease progression in relapsing multiple
sclerosis. Ann Neurol 1996; 39: 285-94amenable to immediate application in patients but a7. PRISMS (Prevention of Relapses and Disability by Interferon β-combination of therapeutic approaches may be re- 1a Subcutaneously in Multiple Sclerosis) Study Group. Ran-
domized double-blind placebo-controlled study of interferonquired ultimately.[85]
β-1a in relapsing/remitting multiple sclerosis. Lancet 1998;352: 1498-504
6. Conclusion 8. Weinstock-Guttman B, Ransohoff RM, Kinkel RP, et al. Theinterferons: biological effects mechanisms of action, and use inmultiple sclerosis. Ann Neurol 1995; 37: 7-15MS is a treatable disease but it is still not curable.
9. Yong VW, Chabot S, Stuve O, et al. Interferon beta in theCurrent therapies are mainly effective as prophylax-treatment of multiple sclerosis: mechanism of action. Neuro-
is in the RR stage of the disease, while the more logy 1998; 51: 682-910. European Study Group on Interferon β-1b in Secondary Pro-aggressive therapies that appear to have benefit in
gressive MS. Placebo-controlled multicentre randomised trialthe progressive stage of the disease are of only of interferon β-1b in treatment of secondary progressive multi-
ple sclerosis. Lancet 1998; 352: 1491-7limited benefit and have significant toxicity. Cur-11. Secondary Progressive Efficacy Clinical trial of Recombinantrently, off-label recommendations for combination
Interferon-beta-1a in MS (SPECTRIMS) Study Group. Ran-therapy are individualised by the general neurolo- domized controlled trial of recombinant interferon beta-1a in
secondary progressive MS: clinical results. Neurology 2001;gist, often in consultation with an MS specialist.56: 1496-504
However, the benefits or otherwise of these com- 12. Goodkin DE, the North American Study Group on Interferonbeta-1b in Secondary Progressive MS. Interferon beta-1b inbined interventions should be determined in well-secondary progressive MS: clinical and MRI results of a 3-yeardesigned, controlled studies. Research in the field ofrandomized controlled trial [abstract]. Late Breaking News.
MS continues to advance towards a better under- Presented at the 52nd annual meeting of the American Acade-my of Neurology; 2000 Apr 29-May 6, San Diegostanding of the disease process and the development
13. Cohen JA, Cutter GR, Fischer JS, et al. Benefit of interferonof more efficient therapeutic interventions. beta-1a on MSFC progression in secondary progressive MS.Neurology 2002; 59: 679-87
14. Johnson KP, Brooks BR, Cohen JA, et al. Copolymer 1 reducesAcknowledgementsrelapse rate and improves disability in relapsing-remittingmultiple sclerosis: results of a phase III multicenter, double-This review has been supported in part by research grantsblind, placebo-controlled trial. Neurology 1995; 45: 1268-76
from the National Institutes of Health (NIH-NINDS 1 K23 15. Chen M, Gran B, Costello K, et al. Glatiramer acetate induces aNS42379-01, R. Bakshi), National Multiple Sclerosis Society Th2-biased response and crossreactivity with myelin basic(RG 3258A2/1, both authors) and National Science Founda- protein in patients with MS. Mult Scler 2001; 7: 209-19
16. Dhib-Jalbut S. Sustained immunological effects of glatiramertion (DBI-0234895, both authors). Dr Weinstock-Guttmanacetate in patients with multiple sclerosis treated for over 6has received research grants from Biogen and Serono/Im-years. J Neurol Sci 2002; 201: 71-7munex and honoraria from Biogen and Teva Neuroscience.
17. Comi G, Filippi M, Wolinsky JS. European/Canadian multicen-Dr Bakshi is a member of the speaker’s bureau of Biogen and ter, double-blind, randomized, placebo-controlled study of thehas received honoraria from Teva Neuroscience. We thank effects of glatiramer acetate on magnetic resonance imaging:Colleen Hogan for the production of figure 1. measured disease activity and burden in patients with relapsing
multiple sclerosis. European/Canadian Glatiramer AcetateStudy Group. Ann Neurol 2001; 49: 290-7
References 18. Calabresi PA, Stone LA, Bash CN, et al. Interferon beta results1. Lublin FD, Reingold SC. Defining the clinical course of multi- in immediate reduction of contrast-enhanced MRI lesions in
ple sclerosis: results of an international survey. Neurology multiple sclerosis patients followed by weekly MRI. Neuro-1996; 46: 907-11 logy 1997; 48: 1446-8
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

Combination Therapy for Multiple Sclerosis 791
19. Hartung HP, Gonsette R, Konig N, and the MIMS-Study Group, tients with relapsing remitting multiple sclerosis. Lancet 2003;et al. Mitoxantrone in progressive multiple sclerosis: a place- 302: 1184-91bo-controlled, double-blind, randomized, multicenter trial. 36. Milo R, Panitch H. Additive effects of copolymer-1 and inter-Lancet 2002; 360: 2018-25 feron beta-1b on the immune response to myelin basic protein.
J Neuroimmunol 1995; 61: 185-9320. Leary SM, Miller DH, Stevenson VL, et al. Interferon beta-1ain primary progressive MS: an exploratory, randomized, con- 37. Brod SA, Lindsey JW, Wolinsky JS. Combination therapy withtrolled trial. Neurology 2003; 60: 44-51 glatiramer acetate (copolymer-1) and a type I interferon (IFN-
alpha) does not improve experimental autoimmune encephalo-21. Kita M, Cohen JA, Rox R, et al. A phase II trial of mitoxantronemyelitis. Ann Neurol 2000; 47: 127-31in patients with primary progressive MS [abstract]. Neurology
2004; 62: A99 38. Zang Y, Hong J, Robinson R, et al. Immune regulatory proper-ties and interactions of copolymer I and beta-interferon 1a in22. Lublin F, Cutter G, Elfont R, et al. A trial to assess the safety ofMS. J Neuroimmunol 2003; 137 (1-2): 144-53combining therapy with interferon beta-1a and glatiramer ace-
tate in patients with relapsing MS [abstract]. Neurology 2001; 39. Yudkin PL, Ellison GW, Ghezzi A, et al. Overview of azathio-56 Suppl. 3: A148 prine treatment in multiple sclerosis. Lancet 1991; 38: 1051-5
23. Moreau T, Blanc S, Riche G, et al. ERAZISMUS: Early 40. Goodkin DE, Rudick RA, VanderBrug Medendorp S, et al.Azathioprine versus Beta-Interferon treatment in Multiple Low dose (7.5mg) oral methotrexate reduces the rate of pro-Sclerosis: results of a pilot study [abstract]. The 9th Annual gression in chronic progressive multiple sclerosis. Ann NeurolMeeting of the European Neurological Society; Milan 1999 1995; 37: 30-40Jun 5-9, 143 41. Goodkin DE, Rudick RA, VanderBrug Medendorp S. Low-dose
oral methotrexate in chronic progressive multiple sclerosis:24. Havrdova E, Ticha V, Novakova I, et al. Intramuscular inter-analysis of serial MRIs. Neurology 1996; 47: 1153-7feron beta-1a in combination with azathioprine and low-dose
steroids for relapsing-remitting multiple sclerosis: design and 42. Calabresi PA, Wilterdink JL, Rogg JM, et al. An open-labelpreliminary results of a two-year double-blind, randomized, trial of combination therapy with interferon beta-1a and oralplacebo-controlled study [abstract]. Neurology 2001; 56 Sup- methotrexate in MS. Neurology 2002; 58: 314-7pl. 3: A356 43. Rowe VD, Dressman LA, Wang D, et al. High dose intravenous
25. Fernandez O, Guerro M, Mayorga C, et al. Combination therapy methotrexate in MS patients worsening despite Avonex ther-with interferon beta-1b and azathioprine in secondary progres- apy: final results [abstract]. Neurology 2004; 62: A260sive MS: a 2 year pilot study. J Neurol 2002; 249: 1058-62 44. Durelli L, Cocito D, Riccio A. High dose intravenous methyl-
26. Rowe VD, Wang D, John HA, et al. Rescue therapy with high prednisolone in the treatment of multiple sclerosis: clinical-dose intravenous methotrexate in MS patients worsening de- immunologic correlations. Neurology 1986; 36: 238-43spite Avonex therapy [abstract]. Neurology 2003; 60 Suppl. 1: 45. Andersson PB, Goodkin DE. Glucocorticosteroid therapy forA149 multiple sclerosis: a critical review. J Neurol Sci 1998; 160:
27. Bielekova B, Reichert-Scrivner S, Wuerfel J, et al. Combina- 16-25tion therapy of MS patients with incomplete response to inter- 46. Barnes D, Hughes RAC, Morris R, et al. Randomized trial offeron-beta with humanized antibody against the interleukin-2 oral and intravenous methylprednisolone in acute relapses ofreceptor alpha chain [abstract]. Mult Scler 2002; 8 Suppl. 1: S4 multiple sclerosis. Lancet 1997; 349: 902-6
28. Smith DR, Weinstock-Guttman B, Cohen JA, et al. Blinded 47. Beck RW, Cleary PA, Trobe J, et al. The effect of corticoster-randomized trial of pulse cyclophosphamide in IFN beta resis- oids for acute optic neuritis on the subsequent development oftant active MS [abstract]. Neurology 2003; 60 Suppl. 1: A84 multiple sclerosis. N Engl J Med 1993; 329: 1764-9
29. Jeffrey DR, Durden DD, Burdette JH. Pilot trial of IFN beta-1b 48. Goodkin DE, Kinkel RP, Weinstock-Guttman B, et al. A phaseand mitoxantrone in multiple sclerosis using monthly gadolini- II study of IV methylprednisolone in secondary-progressiveum enhanced MRI [abstract]. Neurology 2001; 56 Suppl. 3: multiple sclerosis. Neurology 1998; 51: 239-45A353 49. Zivadinov R, Rudick RA, De Masi R, et al. Effects of IV
30. Panitch H, Goodin DS, Francis G, et al. Randomized, compara- methylprednisolone on brain atrophy in relapsing-remittingtive study of interferon beta-1a treatment regimens in MS; the MS. Neurology 2001; 57: 1239-47EVIDENCE Trial. Neurology 2002; 359: 1453-60 50. Salama HH, Kolar OJ, Zang YC, et al. Effects of combination
31. Durelli L, Verdun E, Barbero P, et al. Every other day inter- therapy of beta-interferon 1a and prednisone on serum immu-feron beta-1b versus once-weekly interferon beta-1a for multi- nologic markers in patients with multiple sclerosis. Mult Sclerple sclerosis; results of a 2-year prospective randomized multi- 2003; 9: 28-31center study (INCOMIN). Lancet 2002; 359: 1453-60 51. Fazekas F, Deisenhammer F, Strasser FS, et al. Randomised
32. IFNB Multiple Sclerosis Study Group and the University of placebo-controlled trial of monthly intravenous immunoglobu-British Columbia MS/MRI Analysis Group. Neutralizing anti- lin therapy in relapsing-remitting multiple sclerosis. Austrianbodies during treatment of multiple sclerosis with interferon Immunoglobulin in Multiple Sclerosis Study Group. Lancetbeta-1b: experience during the first 3 years. Neurology 1996; 1997; 349: 589-9347: 889-94 52. Sorensen PS, Wanscher B, Jensen CV, et al. Intravenous
33. The PRISMS Study Group and the University of British Colum- immunoglobulin G reduces MRI activity in relapsing multiplebia MS/MRI Analysis Group. PRISMS-4: long-term efficacy sclerosis. Neurology 1998; 50: 1273-81of interferon beta-1a in relapsing MS. Neurology 2001; 56: 53. Archelos JJ, Previtali SC, Hartung HP. The role of integrins in1628-36 immune-mediated diseases of the nervous system. Trends
34. Pachner AR. Anti-IFNB antibodies in IFNB-treated MS pa- Neurosci 1999; 22: 30-8tients. Neurology 2003; 61 Suppl. 5: S1-5 54. Miller DH, Khan OA, Sheremata WA, et al. A controlled trial
35. Sorensen PS, Ross C, Clemmesen KM, et al. Clinical impor- of natalizumab for relapsing multiple sclerosis. N Engl J Medtance of neutralizing antibodies against interferon beta in pa- 2003; 348: 15-23
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)

792 Weinstock-Guttman & Bakshi
55. Vollmer TL, Phillips JT, Goodman AD, et al. An open-label 71. Calder PC. Fat chance of immunomodulation. Trends Immunolsafety and drug interaction study of natalizumab in combina- Today 1998; 19: 244-7tion with interferon beta (Avonex. Mult Scler. In press 2004
72. Thies F, Nebe-von-Caron G, Powell JR, et al. Dietary supple-56. Rosenberg GA. Matrix metalloproteinases and neuroinflamma- mentation with gamma linolenic acid or fish oil decreases T-
tion in multiple sclerosis. Neuroscientist 2002; 8: 586-95 lymphocyte proliferation in healthy older humans. J Nutr2001; 131 (7): 1918-2757. Nelissen I, Martens E, Van Den Steen PE, et al. Gelatinase B/
matrix metalloproteinase-9 cleaves interferon-β and is a target 73. James MJ, Gibson RA, Cleland LG. Dietary polyunsaturatedfor immunotherapy. Brain 2003; 126: 1371-81 fatty acids and inflammatory mediator production. Am J Clin
Nutr 2000; 71 (1): 343-348S58. Brundula V, Rewcastle NB, Metz LM, et al. Targeting leuko-cyte MMPs and transmigration; Minocycline as a potential 74. Swank RL, Dugan BB. Effect of low saturated fat diet in earlytherapy for multiple sclerosis. Brain 2002; 125: 1297-308 and late cases of multiple sclerosis. Lancet 1990; 336: 37-9
59. Popovic N, Schubart A, Goetz BD, et al. Inhibition of autoim- 75. Dworkin RH, Bates D, Millar JHD, et al. Linoleic acid andmune encephalomyelitis by a tetracycline. Ann Neurol 2002; multiple sclerosis: a reanalysis of three double-blind trials.51: 215-23 Neurology 1984; 34: 1441-5
60. Weber F, Polak T, Gunther A, et al. Synergistic immuno- 76. Weinstock-Guttman B, Baier M, Feichter J, et al. A randomizedmodulatory effects of interferon-beta1b and the phosphodies- study of low fat diet with omega-3 fatty acids supplementationterase inhibitor pentoxifylline in patients with relapsing-remit-
in patients with RRMS [abstract]. Neurology 2003; 60 Suppl.ting multiple sclerosis. Ann Neurol 1998; 44: 27-341: A151
61. Makhlouf K, Weiner HL, Khoury SJ. Potential of beta-2-adre-77. Swanborg RH, Whittum-Hudson JA, Hudson AP. Humannoceptor agonist as add-on therapy for multiple sclerosis:
herpes virus 6 and chlamydia pneumoniae as etiologic agentsfocus on salbutamol (albuterol). CNS Drugs 2002; 16: 1-8in MS: a critical review. Microbes Infect 2002; 4: 1327-33
62. Hauser SL, Dawson DM, Lehrich JR, et al. Intensive immuno-78. Lycke J, Svennerholm B, Hjelmquist E, et al. Acyclovir treat-suppression in progressive multiple sclerosis; a randomized,
ment of RRMS: a randomized, placebo-controlled, double-three arm study of high-dose intravenous cyclophosphamide,blind study. J Neurol 1996; 243: 214-24plasma exchange and ACTH. N Engl J Med 1983; 308: 173-80
79. Liu B, Gao H. Role of nitric oxide in inflammation-mediated63. Weiner HL, Mackin GA, Orav EJ, et al. Intermittent cyclophos-neurodegeneration. Ann N Y Acad Sci 2002; 962: 318-31phamide pulse therapy in progressive multiple sclerosis: final
report of the Northeast Cooperative Multiple Sclerosis Treat- 80. Bakshi R, Benedict RHB, Bermel RA, et al. T2 hypointensity inment Group. Neurology 1993; 43: 910-8
the deep gray matter of patients with multiple sclerosis: aquantitative magnetic resonance imaging study. Arch Neurol64. The Canadian Cooperative Multiple Sclerosis Group. The Cana-
dian cooperative trial of cyclophosphamide and plasma ex- 2002; 59: 62-8change in progressive multiple sclerosis. Lancet 1991; 337:
81. Sicotte NL, Liva SM, Klutch R, et al. Treatment of multiple441-6sclerosis with pregnancy hormone estriol. Ann Neurol 2002;
65. Weinstock-Guttman B, Kinkel RP, Cohen JA, et al. Treatment 52: 421-8of fulminant multiple sclerosis with intravenous cyclophos-
82. Stuve O, Prod’homme T, Slavin A, et al. Statins and theirphamide. Neurologist 1997; 3: 178-85potential targets in multiple sclerosis therapy. Expert Opin
66. Gobbini MI, Smith ME, Richert ND, et al. Effect of open-label Ther Targets 2003; 7: 613-22pulse cyclophosphamide therapy on MRI measures of disease
83. Stuve O, Youssef S, Steinman L, et al. Statins as potentialactivity in five patients with refractory relapsing-remittingtherapeutic agents in neuroinflammatory disorders. Curr Opinmultiple sclerosis. J Neuroimmunol 1999; 99: 142-9Neurol 2003; 16: 393-401
67. Kaufman M, Norton HJ, Sonnefeld G. A randomized controlled84. Youssef S, Stuve O, Patarroyo JC, et al. The HMG-CoAsafety trial of IFN beta 1-a and oral cyclophosphamide in MS.
reductase inhibitor, atorvastatin, promotes a Th2 bias andInt J MS Care 2002; 4 (4): 174-82reverses paralysis in central nervous system autoimmune dis-
68. Bieber AJ, Kerr S, Rodriguez M. Efficient central nervousease. Nature 2002; 420: 39-40
system remyelination requires T cells. Ann Neurol 2003; 53:680-4 85. Colman D, Lubetzki C, Reingold S. Multiple paths, towards
repair in MS. Trends Neurosci 2003; 26: 59-6169. Wade DT, Young CA, Chaudhuri KR, et al. A randomizedplacebo controlled exploratory study of Vit B12, lofepramineand L-phenylalanine (the “Cari Loder regime”) in the treat-
Correspondence and offprints: Dr Bianca Weinstock-ment of MS. J Neurol Neurosurg Psychiatry 2002; 73: 246-9Guttman, The Jacobs Neurological Institute, 100 High70. Puri BK, Bydder GM, Chaudhuri KR, et al. MRI changes in MSStreet, Suite E-2, Buffalo, NY 14203, USA.following treatment with lofepramine and L-phenylalanine.
Neuroreport 2001; 12: 1821-4 E-mail: [email protected]
© 2004 Adis Data Information BV. All rights reserved. CNS Drugs 2004; 18 (12)