Embed Size (px)
Citation preview
COLORADO
EARLY CHILDHOOD
HEARING SCREENING
GUIDELINES
COLORADO DEPARTMENT OF EDUCATION
COLORADO DEPARTMENT OF PUBLIC HEALTH AND ENVIRONMENT
SEPTEMBER 2001 2nd Edition
The following participants are acknowledged for their work

2
in developing the original version of this manual in 1996.
Jay Tinglum Audiology Consultant Colorado Dept. of Public Health & Environment Cheryl D. Johnson Audiology Consultant Colorado Dept. of Education Beverly Bridges Nurse Denver Public Schools Child Find Jane Cotler Nurse Consultant Child Health Services Colorado Dept. of Public Health & Environment Norma Edelman Program Administrator Child Health Services Colorado Dept. of Public Health & Environment Lily Kasbaum Nurse Denver Head Start Kim Miller Audiologist Weld County BOCES Jean Schule Nurse Consultant Migrant Health Colorado Dept. of Public Health & Environment Annette Schurich Audiologist Jefferson County CCB Mary Lou Seeliger Audiologist Denver Public Schools 2001 Revisions by Cheryl D. Johnson, Senior Consultant, Colorado Department of Education, Vickie Thomson, Audiology Consultant, Colorado Department of Public Health & Environment, & Sally Specht, Regional Audiology Coordinator, Colorado Department of Public Health & Environment.
TABLE OF CONTENTS

3
I. Introduction 4 II. Recommended Early Childhood Hearing Screening Procedures 5
• History • Visual Inspection of the Ear • Audiometric Screening • Immittance
III. Methods For Audiometry and Immittance Screening 6
• Calibration 6 • Audiometric Screening Procedures 6 • Comparison of Non-Traditional Screening Procedures 8
IV. Screening Management 9
• Otoacoustic Emissions for Early Childhood Hearing Screening 9 Flowchart & Follow-up 11 • Pure Tone and Immittance Screening Flowchart & Follow-up • Audiological Evaluation Outcome 13 • Data Management 14 • General Information About Hearing Screening 15 • Personnel & Training 17
• Equipment And Calibration 17 V. Appendix 18 A. Self-Listening Check of Audiometer Function 19 B. Hearing Healthcare Associations 20
C. Colorado Audiometric Equipment Resources 21 D. Brochure for Parents: Your Child’s Hearing 22 E. Handout: Suggestions for Parents of Children with Middle Ear Problems 27 F. Sample Forms 30
Screening Permission/Release of Information Hearing History Hearing Developmental Checklist Hearing Screening – Summary (group) Hearing Screening Report & Referral (individual) Medical Referral and Response Certificate of Hearing Screening

4
I. INTRODUCTION
There are five important points that support the need for early childhood hearing screening.
♦ hearing loss is not uncommon; in fact some screening programs have shown as many as 20% of
children do not pass hearing screenings ♦ hearing loss can have a major impact on a child’s development, especially in his/her first years
of life ♦ early identification and intervention minimize the effects of hearing loss on a child's development ♦ hearing screening is the quick and efficient first step in the process of identifying normal hearing
or the need for further evaluation ♦ hearing screening may identify conditions requiring medical attention
Colorado receives federal tax dollars to carry out Public Law 102-119, the Individuals with Disabilities Education Act (IDEA). This law mandates states to identify children who have disabilities, or who have factors which may result in disabilities.
Healthy People 2000 is a set of National Health Promotion and Disease Prevention Objectives to be met by the year 2000. Objective 17.16 is to reduce the average age at which children with significant hearing impairment are identified to no more than 12 months of age.
Education 2000, a set of education-related goals, includes the objective that all children should enter school ready to learn. To meet this objective, hearing loss must be identified at an early age and an intervention and management plan must be available.
House Bill 1095-97 requires all Colorado hospitals to provide a newborn hearing screen prior to birth. Although Colorado State Law mandates the public schools have a system for routine hearing screening for children in grade levels K, 1, 2, 3, 5, 7 & 9, a gap exists in population-based hearing screening between birth and entry into school.
The purpose of these guidelines is to establish recommended early childhood hearing screening practices to be used statewide by all agencies providing services to young children. These guidelines are for screening only; they are designed to identify children who need further testing. Children with any known hearing loss must be managed by an audiologist and therefore should not be seen through a screening program.
All hearing screening programs must include regular consultation by an audiologist. Before setting up your screening program locate an audiologist who can assist in the training and coordination of the screening program as well as follow-up for children referred. Most often your school district's audiologist will be able to provide this service. Children who are difficult to screen due to age or development should be referred to the audiologist for screening.

5
II. R
ECO
MM
END
ED E
AR
LY C
HIL
DH
OO
D H
EAR
ING
SC
REE
NIN
G P
RO
CED
UR
ES
SCR
EEN
ING
C
OM
PON
ENTS
R
ECO
MM
END
ATIO
NS
REF
ERR
AL C
ON
SID
ERAT
ION
S
H
ISTO
RY
Ask
for i
nfor
mat
ion
rega
rdin
g th
e fo
llow
ing:
•
Fam
ily h
isto
ry o
f hea
ring
loss
•
Num
ber o
f epi
sode
s of
ear
infe
ctio
ns; t
ubes
or o
ther
ear
sur
gerie
s •
Prob
lem
s du
ring
preg
nanc
y or
del
iver
y •
Con
cern
s re
gard
ing
spee
ch/la
ngua
ge, d
evel
opm
enta
l del
ay
• Pr
evio
us h
earin
g sc
reen
ing
or te
stin
g
This
info
rmat
ion
shou
ld b
e pa
rt of
th
e re
ferra
l and
follo
w-u
p pr
oces
s. C
once
rns
note
d th
roug
h hi
stor
y sh
ould
incr
ease
the
impo
rtanc
e of
obt
aini
ng
audi
omet
ry a
nd im
mitt
ance
re
sults
VISU
AL
INSP
ECTI
ON
OF
THE
EAR
Look
for:
• St
ruct
ural
def
ects
•
Dra
inag
e fro
m th
e ea
r can
al
If tra
ined
in o
tosc
opy,
al
so lo
ok fo
r: •
Ear c
anal
abn
orm
aliti
es
• Fo
reig
n ob
ject
s/tu
bes
• C
ondi
tion
of th
e ty
mpa
nic
mem
bran
e
Any
conc
erns
sho
uld
be n
oted
, bu
t not
use
d to
refe
r for
med
ical
at
tent
ion
and/
or a
udio
logi
cal
atte
ntio
n if
audi
omet
ry a
nd
imm
ittan
ce s
cree
ning
s ar
e pa
ssed
.
PRO
CED
UR
ES F
OR
CH
ILD
REN
WH
O C
AN N
OT
RES
PON
D T
O C
ON
VEN
TIO
NAL
PU
RE
TON
E SC
REE
NIN
G M
ETH
OD
S
PRO
CED
UR
E FO
R C
HIL
DR
EN W
HO
R
ESPO
ND
TO
TR
ADIT
ION
AL P
UR
E TO
NE
SCR
EEN
ING
MET
HO
DS
AUD
IOM
ETR
IC
SCR
EEN
ING
Con
duct
one
or m
ore
of th
e fo
llow
ing
as a
ppro
pria
te:
• So
und
Boot
h Vi
sual
Rei
nfor
cem
ent
audi
omet
ry (V
RA)
•
Auto
mat
ed O
toac
oust
ic E
mis
sion
s Th
e fo
llow
ing
proc
edur
es a
re c
ondu
cted
onl
y up
on
reco
mm
enda
tion
of th
e au
diol
ogis
t •
Audi
tory
Bra
inst
em R
espo
nse
(ABR
/BSE
R)
• D
iagn
ostic
Oto
acou
stic
Em
issi
ons
(OAE
)
Util
izin
g co
nditi
oned
pla
y au
diom
etry
, con
duct
a
scre
enin
g ut
ilizin
g a
pure
tone
aud
iom
eter
at t
he
follo
win
g fre
quen
cies
and
dec
ibel
leve
ls: 2
0dBH
L @
100
0, 2
000
& 40
00H
z.
All f
requ
enci
es m
ust b
e he
ard
in
both
ear
s in
ord
er to
pas
s th
e pu
re to
ne s
cree
ning
.
IM
MIT
TAN
CE
PASS
: Gra
dien
t (ty
mpa
nom
etric
wid
th) v
alue
is le
ss th
an 2
00 (d
aPa
or m
mH
20)
NO
T PA
SS: G
radi
ent v
alue
is g
reat
er th
an 2
00 (d
aPa
or m
mH
20);
then
als
o re
cord
ear
can
al v
olum
e. I
f O
AE is
pre
sent
, im
mitt
ance
not
requ
ired.
[Not
e: Im
mitt
ance
scr
eeni
ng is
not
app
ropr
iate
for i
nfan
ts u
nder
6
mon
ths
of a
ge].
Ref
erra
ls d
eter
min
ed in
co
njun
ctio
n w
ith o
ther
find
ings
an
d du
ratio
n of
con
ditio
ns.
Impo
rtant
Not
es:
1. P
aren
t con
sent
sho
uld
be o
btai
ned
prio
r to
cond
uctin
g he
arin
g sc
reen
ing.
2.
Chi
ldre
n sh
ould
be
refe
rred
to a
n au
diol
ogis
t whe
n he
arin
g sc
reen
ing
resu
lts c
anno
t be
obta
ined
with
in tw
o w
eeks
of t
he in
itial
Chi
ld F
ind
scre
en.
3. A
ll ch
ildre
n, b
irth
thro
ugh
3rd
grad
e, s
houl
d ha
ve a
n an
nual
hea
ring
scre
enin
g re
gard
less
of w
heth
er o
r not
they
pas
sed
new
born
scr
eeni
ng o
r fam
ily s
tory
of h
earin
g lo
ss.
4. A
ll he
arin
g sc
reen
ing
prog
ram
s sh
ould
be
deve
lope
d an
d co
nduc
ted
in c
olla
bora
tion
with
an
audi
olog
ist.

6
III. METHODS FOR AUDIOMETRY AND IMMITANCE
SCREENING These are screening methods to identify children who need further testing. Therefore it is not appropriate to screen children who have known hearing losses monitored by an audiologist, or children who wear hearing aids. All screeners must receive appropriate training prior to conducting any of the following procedures. Calibration 1. Pure Tone Audiometers
Each time the hearing screening equipment is set up for use, the screener should listen to the equipment to make sure it is working. See Appendix A for a chart of listening check items. Place the headphones on yourself or someone else with normal hearing, and screen at 5dBHL below the level you are using for screening (20dBHL at 15dBHL at 1000, 2000, and 4000 Hz). Make sure each tone can be heard clearly and easily. Then make sure that as the volume is increased the sound becomes louder.
2. Otoacoustic Emissions (OAE) – follow the manufacturer’s instructions 3. Immittance - follow the manufacture’s instructions Audiometric Screening Procedures 1. Conventional Audiometry
The Conventional pure tone screening procedure is recommended for children who are able to respond to earphone sound presentation utilizing a pure tone audiometer. For each sound presentation children should respond by raising their hand or playing a game (block in bucket, ring on stand, peg in board). Protocol: 25 dB @ 20 dB @ 1000, 2000, & 4000 Hz. All sounds must be heard in both ears in order for a child to pass the pure tone screening.
2. Sound Booth Visual Reinforcement Audiometry (VRA):
This technique is appropriate for children who have the ability to localize to the source of sound. The child responds to the sound source by turning his/her head toward the sound source. A visual reinforcer is then presented (lighted toy or moving toy) when the child localizes to the sound source. Sound-field speakers are available with toys attached at the top that are connected to a calibrated signal generator for a variety of frequencies and intensities.
3. Automated Otoacoustic Emissions (OAE: DPOAE or TEOAE):
OAEs are sounds created in the cochlea which can be measured by a sensitive microphone placed in the ear canal. These emissions may be evoked, or enhanced by presenting an external auditory signal. Emissions are not affected by neurological involvement and can be obtained up to 6000Hz. A computer is used to record and average the emissions in response to a large number of auditory signals presented to that ear. There is a high correlation between the presence of emissions and hearing levels better than 30-35 dB. Voluntary responses from the child are not required. This procedure is monitored by an audiologist.
4. Automated Auditory Brainstem Response (ABR, AER, ERA, BAER, BSER):
This procedure measures the electrical responses of the auditory nerves to a series of clicks presented to the child through headphones. A computer averages the nerve responses measured by electrodes placed in specific locations on the head. Click stimuli are used to assess high frequency hearing ability (+/-15dB

7
of threshold); tone pips may be added to evaluate low frequency hearing. Results may be affected by neurological involvement. Voluntary responses from the child are not required. This procedure is only conducted by an audiologist. Automated ABR (AABR) is used to screen newborns or young infants.
5. Immittance
Immittance is an objective means of assessing the function of the outer and middle ear, which includes the ear canal, eardrum, the bones of the middle ear (ossicles), and the eustachian tube. This procedure gives specific information about the size of the ear canal, mobility of the eardrum, and pressure on the eardrum. Although the test does not assess the ability to hear, certain conditions of the outer and middle ear are highly correlated to hearing loss. The results may indicate the need for a direct referral for medical evaluation. Tympanograms with an abnormally wide tympanometric width have configurations with shallow, rounded peaks or are flat (no peaks). The latter are often referred to as Type B tympanograms.
A PASS is when the gradient (tympanometric width) is less than 200 (daPa or mm H20). The child does NOT PASS when the value is equal to or greater than 200 (daPa or mm H20). If NOT PASS, also record the canal volume. See Appendix D for sample tympanograms and information on how to calculate the gradient if your tympanometer doesn't calculate it automatically.

8 C
OM
PAR
ISO
N O
F N
ON
-TR
AD
ITIO
NA
L SC
REE
NIN
G P
RO
CED
UR
ES
Vi
sual
Rei
nfor
cem
ent A
udio
met
ry
Oto
acou
stic
Em
issi
ons
Bra
inSt
em
Evok
ed
Res
pons
e
Equi
pmen
t Cos
t $1
,000
$4
,000
$1
0,00
0 an
d hi
gher
Port
abili
ty
Goo
d G
ood
Mos
t diff
icul
t
Trai
ning
Nee
ds
Mod
erat
e M
oder
ate
Hig
h
Sens
itivi
ty &
Sp
ecifi
city
G
ives
an
idea
of a
ppro
xim
ate
hear
ing
leve
ls d
own
to s
oft l
evel
s at
spe
cific
fre
quen
cies
Pres
ence
of e
mis
sion
s in
dica
tes
hear
ing
bette
r tha
n 30
-35
dBH
L in
the
mid
-to h
igh
frequ
enci
es
Com
mon
ly p
rovi
des
high
fre
quen
cy (2
k-4k
Hz)
he
arin
g in
form
atio
n w
ithin
15
dB o
f thr
esho
ld
Lim
itatio
ns
Not
ear
spe
cific
; req
uire
s qu
iet r
oom
C
hild
mus
t sit
quie
tly a
nd to
lera
te a
pr
obe
in th
e ea
r can
al
May
requ
ire s
edat
ion
for
todd
lers
, res
ults
may
be
affe
cted
by
neur
olog
ical
in
volv
emen
t
9
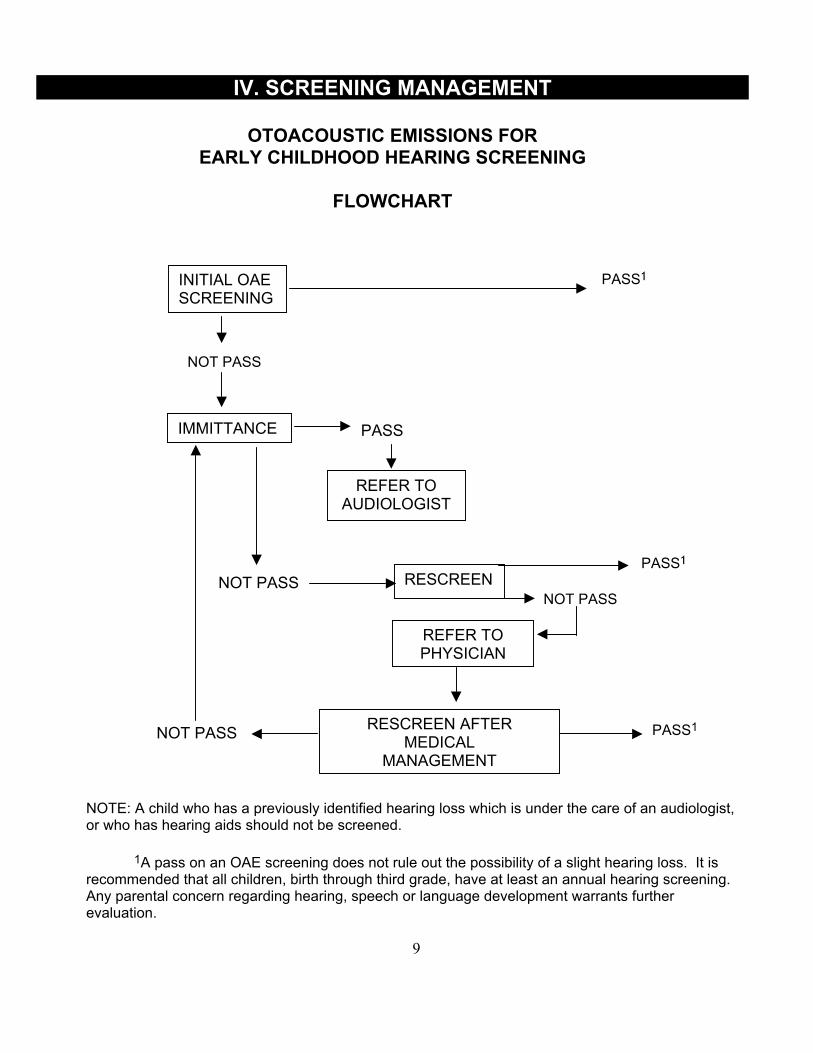
IV. SCREENING MANAGEMENT
OTOACOUSTIC EMISSIONS FOR
EARLY CHILDHOOD HEARING SCREENING
FLOWCHART
NOT PASS
NOTE: A child who has a previously identified hearing loss which is under the care of an audiologist, or who has hearing aids should not be screened.
1A pass on an OAE screening does not rule out the possibility of a slight hearing loss. It is
recommended that all children, birth through third grade, have at least an annual hearing screening. Any parental concern regarding hearing, speech or language development warrants further evaluation.
RESCREEN AFTER MEDICAL
MANAGEMENT
INITIAL OAESCREENING
PASS1
IMMITTANCE PASS
NOT PASS
REFER TO AUDIOLOGIST
RESCREEN
REFER TO PHYSICIAN
NOT PASS PASS1
NOT PASS
PASS1

10
OTOACOUSTIC EMISSIONS FOR EARLY CHILDHOOD SCREENING
FOLLOW - UP
1. All children who do not pass OAE and immittance screening should be rescreened within two to four weeks unless referred for immediate medical or audiological evaluation.
2. Children who do not pass OAE screening but do pass immittance should be referred
to an audiologist for a hearing evaluation.
3. Any concerns identified through history and/or visual inspection of the ear (structural defects, ear canal abnormalities, drainage, excessive wax) should be interpreted in conjunction with immittance and OAE screening results. If OAEs and immittance are passed, the history/visual inspection concerns may be noted but should not be considered a basis for referral. If OAEs and/or immittance are not passed, then the history/visual inspection concern should be noted with the referral. It is important that these children be seen for hearing screening annually.
4. Children with patent PE tubes should have a normal OAE response and should be
monitored according to the physician’s recommendations. Should abnormal results be obtained, refer the child to his/her physician.
RESCEENING RESULTS OUTCOME REFERRAL FOLLOW-UP
OAE - PASS
Normal None Routine annual screening
OAE – NOT PASS Tympanometry – NOT PASS
Possible abnormal middle ear function
To audiologist Monitor and refer to physician when necessary; if condition persists 3 months or more a medical referral is recommended
OAE - NOT PASS Tympanometry - PASS
Possible hearing loss
To audiologist Management based upon audiologist's recommendations

11
PURE TONE AND IMMITTANCE SCREENING
FLOWCHART
PURE TONE & IMMITTANCE PASS1 INITIAL SCREENING NOT PASS PURE TONE & IMMITTANCE PASS1
RESCREEN NOT PASS IMMITTANCE:NOT PASS REFER TO PHYSICIAN (AUDIOMETRIC: PASS OR NOT PASS) AUDIOMETRIC: NOT PASS RESCREEN AFTER (IMMITTANCE:PASS) MEDICAL MANAGEMENT REFER TO AUDIOLOGIST NOT PASS PASS1 NOTE: A child who has a previously identified hearing loss which is under the care of an audiologist, or who has hearing aids should not be screened.
1Passing a hearing screening may not rule out the possibility of a slight hearing loss or a loss
at frequencies not tested. It is recommended that all children, birth through third grade, have at least an annual hearing screening. Any parental concern regarding hearing, speech or language warrants immediate evaluation by an audiologist.

12
PURE TONE AND IMMITTANCE SCREENING
FOLLOW - UP
1. All children who do not pass audiometry and immittance screening should be rescreened within two to four weeks unless referred for immediate medical or audiological evaluation.
2. Children who do not pass the second screening should be managed according to the
follow-up recommendations in the chart below.
3. Any concerns identified through history and/or visual inspection of the ear (structural defects, ear canal abnormalities, drainage, excessive wax) should be interpreted in conjunction with immittance and audiometric screening results. If pure tones and immittance are passed, the history/visual inspection concerns may be noted but should not be considered a basis for referral. If pure tones and/or immittance are not passed, then the history/visual inspection concern should be noted with the referral. It is important that these children be seen for hearing screening annually.
RESCEENING RESULTS OUTCOME REFERRAL FOLLOW-UP
Audiometry - PASS Immittance - PASS Normal None Routine annual screening
Audiometry – PASS Immittance – NOT PASS
Possible abnormal middle ear function
To audiologist Monitor and refer to physician when necessary; if condition persists 3 months or more a medical referral is recommended
Audiometry - NOT PASS Immittance - NOT PASS
Possible abnormal middle ear function and
hearing loss
To audiologist and/or physician depending upon significance of
findings
Monitor and refer to physician when necessary; rescreen tympanometry and audiometry after medical treatment; refer back to physician if tympanometry is still abnormal
Audiometry - NOT PASS Immittance - PASS
Possible hearing loss To audiologist Management based upon audiologist's recommendations
13
AUDIOLOGICAL EVALUATION OUTCOME Following evaluation by an audiologist all children should be categorized in one of the following outcomes: Normal Hearing: Child's hearing is within a normal range. Hearing, however, should be screened annually through the third grade. Medically Significant Ear Problem: Child's hearing is within a normal range, but middle ear function is abnormal, or fluctuates frequently, due to otitis media or otitis media-related ear problems, including middle ear tubes. Hearing, and tube status, if the child has tubes, should be monitored, through screening or evaluation, at least every 6 months
Note: • three or more episodes of otitis media in a 6 month period, or • 4 or more episodes in a 12 month period, or • one episode of otitis media lasting three months or longer • are risk factors for speech, language, and learning problems.
Non-educationally Significant Hearing Loss: Child has a hearing loss that does not meet the criteria for educationally significant hearing loss (based upon Colorado Department of Education's Audiology Effectiveness Indicators for Audiology Services in the Schools). These losses are slight and typically in the high frequency range, affect only one or two frequencies, or only one ear. These losses are usually sensorineural in origin and therefore permanent. These types of losses should be monitored at least annually, through evaluation or screening, to insure their stability. Any change in hearing requires an audiological evaluation and referral to an ear specialist. Educationally Significant Hearing Loss: A hearing loss that meets one of the following criteria, as determined by an audiological evaluation: 1. An average pure-tone hearing loss in the speech range (500-2000Hz) of 2OdBHL or greater
in the better ear which is not reversible within a reasonable period of time. 2. An average high frequency, pure-tone hearing loss of 35 dBHL or greater in the better ear at
two (2) or more of the following frequencies - 2000, 3000, 4000, 6000 Hz. 3. A permanent unilateral hearing loss of 35 dBHL or greater in the speech range (500-2000
Hz). 4. Chronic otitis media (any episode lasting 3 months or longer), whether educationally
significant hearing loss is present or not, between the ages of birth and 5 years. Children who meet the educationally significant hearing loss category must be referred to the community or school district Child Find program for appropriate assessment and determination of eligibility for services.

14
DATA MANAGEMENT
Data Management is an essential component of the screening program. There must be a method for recording and tracking results that is easy to use and maintain. The following areas should be included:
• A written process for notifying parents of screening results
• Proper procedures and forms that are easy to use for referrals to the audiologist and physicians
• Parents should be able to understand these forms and how to follow through on
recommendations; translated material and/or interpreters may be required. • All forms and procedures should be developed and implemented through the
cooperative effort of the audiologist with whom you are working; the audiologist must have easy access to referral information in order to expedite follow up procedures
• Results for children who pass screening should be recorded as well as those
who do not pass; a plan to screen children who were absent is also necessary
• Work with your audiologist to develop the methods and management procedures that will work best for both of you.
INCLUDED IN THE APPENDIX ARE SOME SAMPLE FORMS TO ASSIST IN THE DEVELOPMENT OF A HEARING SCREENING PROCESS THAT IS MOST EFFECTIVE FOR YOUR AREA.
15
GENERAL INFORMATION ABOUT HEARING SCREENING
WHAT DOES IT MEAN IF A CHILD PASSES THE HEARING SCREENING? If a child has passed the screening he/she should hear at a level which is adequate for the pitches of sound which are most important for understanding what people say. Since this is a screening, it is possible for a child to occasionally pass who does have a hearing loss. The screening does not rule out a very slight hearing loss or a hearing loss in the high pitches. If a parent suspects his/her child may have a hearing problem even after the hearing screening, an evaluation by an audiologist should be recommended. Even if a child passes today, it does not mean he/she may not have a hearing problem later on. Children should have their hearing screened every year through third grade, and then at scheduled intervals as recommended through the State screening guidelines for the schools. Anytime a concern about hearing arises, another hearing screening should be done as soon as possible. WHAT DOES IT MEAN IF A CHILD NEEDS A HEARING RECHECK? This means that the child either refused the screening, did not understand, or did not respond as would be expected for his/her age. A referral does not mean the child has a hearing problem, but further testing is required to find out how well he/she hears. Since the only way to know for sure how a child hears is through hearing testing, it is recommended that follow up occur according to the procedures outlined in these guidelines. WHAT IS A IMMITANCE (Tympanometry) It is not a hearing test. Tympanometry is a method of using air pressure to move the eardrum and the bones behind the eardrum to test the function of the middle ear. The test can tell if there may be a problem such as a wax blockage in the ear canal, a hole in the eardrum, fluid behind the eardrum, or a eustachian tube problem. This test does not hurt and is not harmful. Some doctors do a similar test where they look in the ear with a light while puffing air into the ear to watch the eardrum move. If the test indicates borderline normal results, such as in a eustachian tube problem, a recheck of the tympanogram may be recommended to determine whether the ears are getting better or worse. Since the tympanogram is not a hearing test, the child could "pass" and still have a hearing problem that requires follow-up testing. WHO IS AN AUDIOLOGIST? Audiologists are hearing professionals who have at least a master's degree in audiology. Audiologists are trained to test people of all ages and abilities. There should be an audiologist working in each school district or BOCES. School audiologists are required by law to test any child (infants as well as school aged children), at no charge to families, to determine whether a hearing loss exists which might result in the child being eligible for
16
special education services. If a school district audiologist does not have the proper equipment to assess a child's hearing, as in the case of some children who are difficult to test, he/she can recommend to the family another audiologist to test the child. The audiologist may also help to find financial assistance for related hearing or medical needs. What are Otoacoustic Emissions (OAE)? OAE’s are the inner ear’s response to sound. These responses are typically present in normal hearing ears. If the child has an ear infection the OAE is usually not present. A small probe in the ear canal is used to measure the OAE. What is the Colorado Hearing Resource (CO-Hear) Coordinator? The Co-Hear Coordinator is a local professional trained to work with families who have children who are deaf or hard of hearing. The Co-Hear Coordinator assists the family in finding resources for funding, early intervention programs and parent support groups.

17
PERSONNEL AND TRAINING
1. All screening programs, including training of screeners, should be under the direction of
an audiologist.
2. While screening programs need to be flexible and adaptable to unique situations, all programs should adhere to stated protocols.
3. Individuals who will be trained to screen this age group should have broad based
knowledge and experience with early childhood development. 4. It is recommended that all screeners have initial training and annual refresher training to
maintain screening skills. Supervision of screeners by an audiologist should occur routinely.
EQUIPMENT AND CALIBRATION
1. Behavioral calibration (testing yourself) should be done at the beginning of each screening day for audiometers, VRAs and tympanometers.
2. Manually operated pure tone audiometers must meet ANSI S3.6-1969 standards. The
Owner's Manual for each piece of equipment will indicate which standards are met. Automated pure tone screening systems are typically not appropriate for use with young children. Annual professional electro-acoustic calibration is necessary.
3. Tympanometers must meet ANSI 83.39-1987, Type 4 standards. Reflectometers such as
the "Acoustic Otoscope" are not recommended. Routine calibration should occur with the system's self-calibration equipment if available. Annual calibration is necessary for equipment that does not self-calibrate. Tympanometers should be specially calibrated for use in high altitudes.
4. OAE calibration and function is available in the manufacturer's manuals.

18
V. APPENDIXES
All forms, hand-outs, or other information in this packet may be reproduced, modified, or adapted for local use.

APP
END
IX A
Self-
List
enin
g C
heck
of A
udio
met
er F
unct
ion
Au
diom
eter
Mak
e:
Mod
el:
Se
rial #
:___
____
____
____
___
D
ate
Jack
s se
ated
C
ords
ok
ay
Hea
d-ba
nd
tens
ion
Earp
hone
cu
shio
ns
okay
Dia
ls
tight
Vo
lum
e in
crea
ses
&
decr
ease
s
Pitc
h ok
ay
Tone
on
-off
okay
Tone
pr
esen
ter
inau
dibl
e
No
stat
ic
No
sign
al
cros
s-ov
er
Test
room
qu
iet
Initi
al
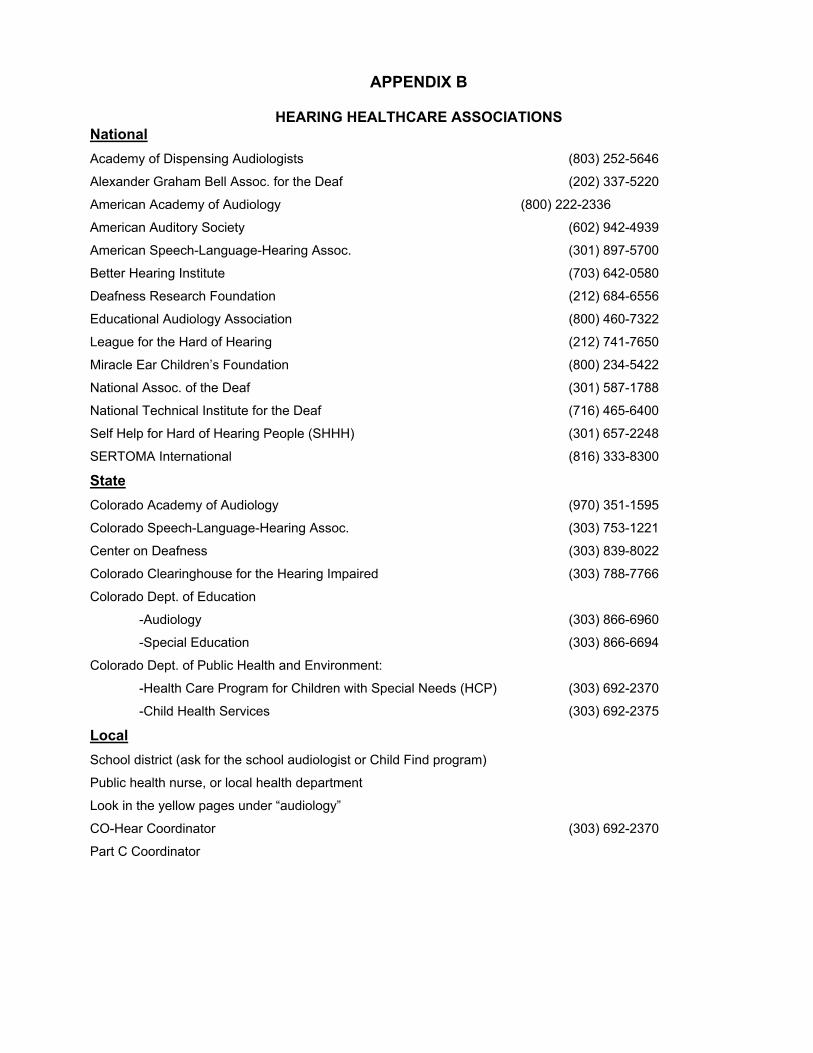
APPENDIX B
HEARING HEALTHCARE ASSOCIATIONS National Academy of Dispensing Audiologists (803) 252-5646
Alexander Graham Bell Assoc. for the Deaf (202) 337-5220
American Academy of Audiology (800) 222-2336
American Auditory Society (602) 942-4939
American Speech-Language-Hearing Assoc. (301) 897-5700
Better Hearing Institute (703) 642-0580
Deafness Research Foundation (212) 684-6556
Educational Audiology Association (800) 460-7322
League for the Hard of Hearing (212) 741-7650
Miracle Ear Children’s Foundation (800) 234-5422
National Assoc. of the Deaf (301) 587-1788
National Technical Institute for the Deaf (716) 465-6400
Self Help for Hard of Hearing People (SHHH) (301) 657-2248
SERTOMA International (816) 333-8300 State Colorado Academy of Audiology (970) 351-1595
Colorado Speech-Language-Hearing Assoc. (303) 753-1221
Center on Deafness (303) 839-8022
Colorado Clearinghouse for the Hearing Impaired (303) 788-7766
Colorado Dept. of Education
-Audiology (303) 866-6960
-Special Education (303) 866-6694
Colorado Dept. of Public Health and Environment:
-Health Care Program for Children with Special Needs (HCP) (303) 692-2370
-Child Health Services (303) 692-2375
Local School district (ask for the school audiologist or Child Find program)
Public health nurse, or local health department
Look in the yellow pages under “audiology”
CO-Hear Coordinator (303) 692-2370
Part C Coordinator

21
APPENDIX C
COLORADO AUDIOMETRIC EQUIPMENT RESOURCES MSR West, Inc. Roger Ott (303) 604-0044 P.O. Box 18176 Boulder, CO 80308 Western Acoustics Bill Van Cleave (303) 360-0575 700 Billings Aurora, CO 80011 Aurora Education Foundation (303) 344-8060 ext.365 1085 Peoria Street Aurora, CO 80011 (videotape to prepare children for traditional screening)

22
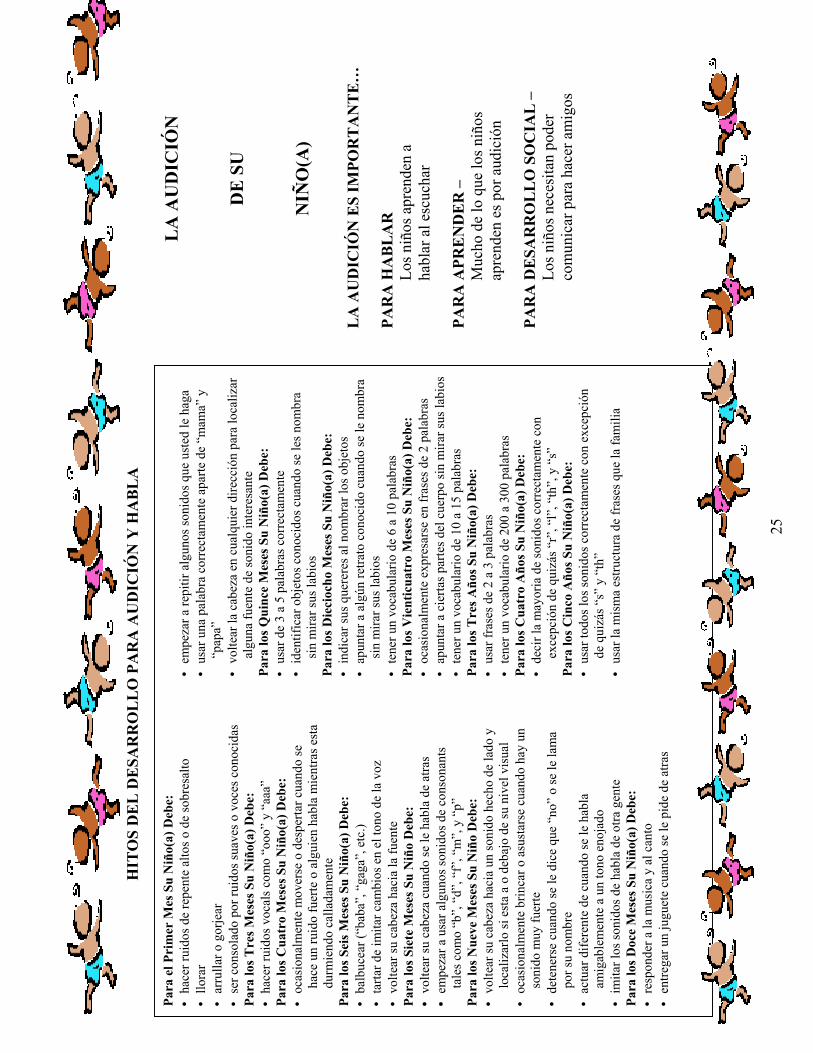
APPENDIX D
Brochure: Your Child’s Hearing “Your Child’s Hearing” is a brochure developed for parents and is provided in both English and Spanish.. It is suggested that this form be reproduced on colored paper and presented in a tri-fold format. This brochure should be given to parents at the time of screening. Additional uses include placement in physicians’ offices, health departments, daycares and preschools, Child Find offices, and any other sites where children’s health and development is addressed.

23
DEV
ELOPM
ENTA
L M
ILES
TONES
FOR
HEA
RING
& SP
EECH
By 1
Mon
th Y
our
Child
Sho
uld:
•
sta
rtle
to
loud
, sud
den
nois
es
• c
ry
• c
oo a
nd g
urgl
e •
be
com
fort
ed b
y so
ft s
ound
s an
d fa
mili
ar v
oice
s
By 3
Mon
ths
Your
Child S
hould:
•
Mak
e vo
wel s
ound
s lik
e “o
oh” a
nd “a
ah”
By 4
Mon
ths
Your
Child S
hould:
•
occ
asio
nally
sti
r or
wak
en w
hen
quie
tly
slee
ping
if
a lo
ud n
oise
i
s m
ade
or if
som
eone
tal
ks
By 6
Mon
ths
Your
Child S
hould:
•
bab
ble
(“ba
ba”,
“gag
a”, e
tc)
• t
ry t
o im
itat
e ch
ange
s in
voi
ce p
itch
•
tur
n he
ad t
owar
d so
und
sour
ce
By 7
Mon
ths
Your
child S
hould:
•
tur
n he
ad w
hen
calle
d fr
om b
ehin
d •
beg
in u
sing
som
e co
nson
ant
soun
ds s
uch
as “b
”, “d
”, “f
”, “m
”, &
“p
”
By 9
Mon
ths
Your
Child S
hould:
•
tur
n he
ad t
owar
d a
soun
d m
ade
at s
ide
and
loca
te
it if
at
eye
leve
l or
belo
w •
occ
asio
nally
jum
p or
sta
rtle
whe
n th
ere
is a
ver
y lo
ud s
ound
•
sto
p wh
en “n
o-no
” or
nam
e is
sai
d
• c
hang
e pi
tch
of h
is/h
er v
oice
•
act
dif
fere
ntly
to
frie
ndly
ver
sus
angr
y ta
lkin
g •
imit
ate
spee
ch s
ound
s of
oth
er p
eopl
e By
12
Mon
ths
Your
Child S
hould:
•
res
pond
to
mus
ic a
nd s
ingi
ng
• g
ive
a to
y wh
en a
sked
for
it f
rom
beh
ind
• b
egin
to
repe
at s
ome
of t
he s
ound
s yo
u m
ake
• u
se o
ne o
ther
wor
d co
rrec
tly
besi
des
“mam
a” a
nd
“da
da
• t
urn
head
in a
ny d
irec
tion
to
loca
te in
tere
stin
g so
und
sour
ce
By 1
5 M
onth
s Yo
ur C
hild S
hould:
•
use
3 t
o 5
word
s co
rrec
tly
• id
enti
fy f
amili
ar o
bjec
ts w
hen
nam
ed w
itho
ut
watc
hing
you
r lip
s
By 1
8 M
onth
s Yo
ur C
hild S
hould:
•
indi
cate
wan
ts b
y na
min
g ce
rtai
n ob
ject
s •
poi
nt t
o a
fam
iliar
pic
ture
whe
n na
med
wit
hout
wa
tchi
ng y
our
lips
• h
ave
a 6
to 1
0 wo
rd v
ocab
ular
y
By 2
4 M
onth
s Yo
ur C
hild S
hould:
•
occ
asio
nally
exp
ress
sel
f in
2 w
ord
sent
ence
s •
poi
nt t
o ce
rtai
n bo
dy p
arts
whe
n as
ked
with
out
watc
hing
you
r lip
s •
hav
e a
10 t
o 15
wor
d vo
cabu
lary
By 3
Yea
rs Y
our
Child
Sho
uld:
•
use
2 t
o 3
word
sen
tenc
es
• h
ave
a 20
0 to
300
wor
d vo
cabu
lary
By 4
Yea
rs Y
our
Child
Sho
uld:
•
say
mos
t so
unds
cor
rect
ly e
xcep
t pe
rhap
s “r
”, “l”
, “t
h”, a
nd “s
”
By 5
Yea
rs Y
our
Child
Sho
uld:
• •
use
all s
ound
s co
rrec
tly
exce
pt p
erha
ps “s
” and
“th”
•
use
the
sam
e se
nten
ce s
truc
ture
as
the
fam
ily
YO
UR
CHIL
D’S
HEA
RING
HEA
RING
IS I
MPO
RTANT…
FOR
SPEA
KING…
Childre
n lear
n to
spe
ak b
y lis
tening
FOR
LEARN
ING-
Muc
h of
wha
t ch
ildre
n
lea
rn is
by h
earing
FOR
SOCI
AL
GROW
TH-
Childre
n ne
ed t
o
com
mun
icat
e
to
mak
e fr
iend

24
WHY
IS I
T IM
PORT
ANT
TO H
AVE
YOUR
CHIL
D’S
HEA
RING
CHEC
KED E
VERY
YEA
R?
• H
eari
ng c
an c
hang
e •
Onl
y a
hear
ing
test
can
tel
l you
for
sur
e ho
w yo
ur
child
hea
rs
• H
eari
ng p
robl
ems
can
be r
elat
ed t
o m
edic
al
prob
lem
s •
Hea
ring
is im
port
ant
for
spee
ch, l
angu
age
deve
lopm
ent
& le
arni
ng
HOW
IS
HEA
RING
SCRE
ENED
IN
CHIL
DRE
N?
Part
1:
Aud
iom
etry
•
The
chi
ld’s
abili
ty t
o he
ar s
oft
soun
ds a
t di
ffer
ent
pitc
hes
is s
cree
ned.
•
Hea
ring
abi
lity
is d
eter
min
ed b
y ch
ecki
ng h
ow t
he
child
res
pond
s to
sou
nds
thro
ugh
head
phon
es o
r sp
eake
rs
• F
or v
ery
youn
g or
dif
ficu
lt t
o te
st c
hild
ren
othe
r te
chni
ques
may
be
used
Pa
rt 2
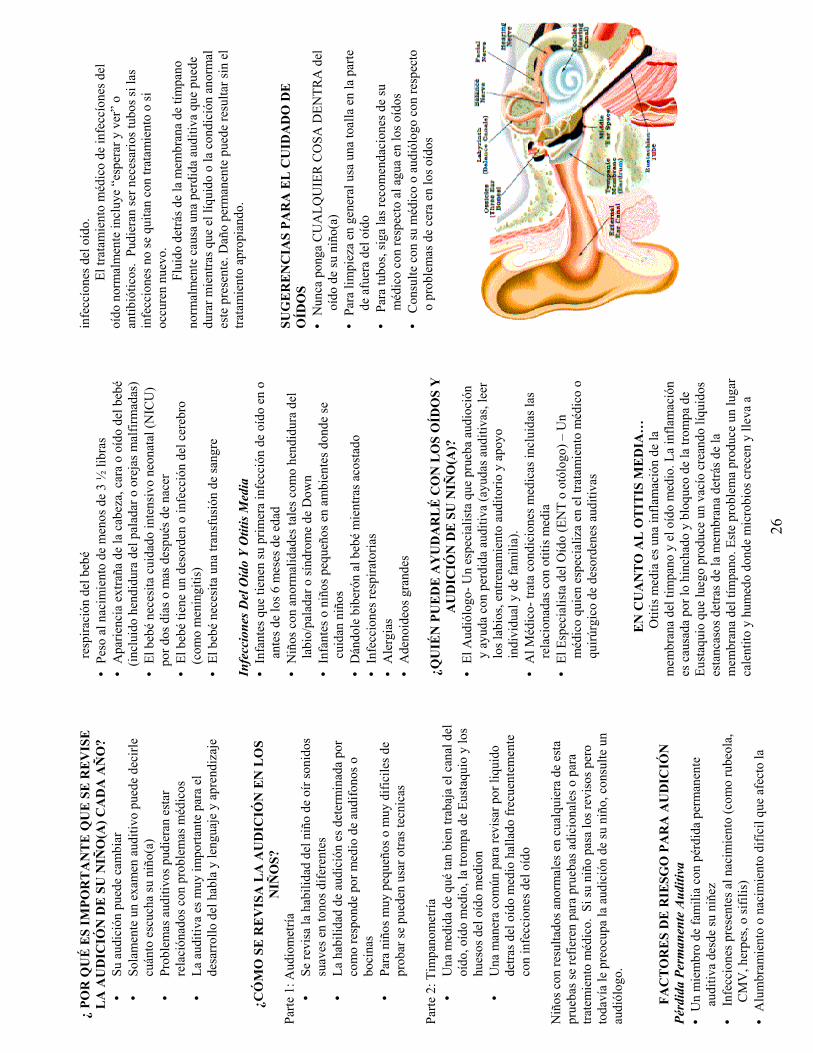
: Tym
pano
met
ry
• A
mea
sure
of
how
well
the
ear
cana
l, ea
rdru
m,
Eust
achi
an t
ube
and
mid
dle
ear
bone
s ar
e wo
rkin
g •
A c
omm
on w
ay t
o ch
eck
for
flui
d be
hind
the
ea
rdru
m f
requ
entl
y fo
und
with
ear
infe
ctio
ns
Child
ren
with
abn
orm
al r
esul
ts o
n ei
ther
of
thes
e te
sts
are
refe
rred
for
fur
ther
tes
ting
or
for
med
ical
tr
eatm
ent.
If
your
chi
ld p
asse
s th
e sc
reen
ing
and
you
still
hav
e a
conc
ern
abou
t yo
ur
child
’s he
arin
g, c
onsu
lt a
n au
diol
ogis
t.
RI
SK F
ACT
ORS
FOR
HEA
RING
Perm
anen
t Hea
ring
Los
s •
A f
amily
mem
ber
with
per
man
ent
hear
ing
loss
si
nce
child
hood
• S
erio
us in
fect
ion
pres
ent
at b
irth
(suc
h as
Ger
man
m
easl
es, C
MV,
her
pes,
or
syph
ilis)
•
Dif
ficu
lt b
irth
or
dive
rsit
y wh
ich
affe
cted
bab
y’s
brea
thin
g •
Baby
’s bi
rth
weig
ht le
ss t
han
3 lb
s
• U
nusu
al a
ppea
ranc
e of
bab
y’s h
ead,
fac
e or
ear
s (in
clud
ing
clef
t pa
late
or
mal
form
ed e
ars)
•
Bab
y re
quir
es n
eona
tal i
nten
sive
car
e (N
ICU
) for
2
days
or
mor
e fo
llowi
ng b
irth
•
Bab
y ha
s a
diso
rder
or
infe
ctio
n of
the
bra
in (s
uch
as m
enin
giti
s)
• B
aby
requ
ires
exc
hang
e bl
ood
tran
sfus
ion
Ear
Infe
ctions
& O
titis
Med
ia
• I
nfan
ts w
ho h
ave
thei
r fi
rst
ear
infe
ctio
n at
or
befo
re 6
mon
ths
of a
ge
• C
hild
ren
with
fac
ial a
bnor
mal
itie
s su
ch a
s cl
eft
lip/p
alat
e or
Dow
n Sy
ndro
me
• I
nfan
ts &
you
ng c
hild
ren
in d
ay c
are
sett
ings
•
Chi
ldre
n ex
pose
d to
cig
aret
te s
mok
e •
Bot
tle
feed
ing
when
bab
y is
lyin
g do
wn
• U
pper
res
pira
tory
infe
ctio
ns
• A
llerg
ies
• L
arge
ade
noid
s
WHO C
AN H
ELP
TAKE
CARE
OF
YOUR
CHIL
D’S
EARS
& H
EARI
NG?
•
The
Aud
iolo
gist
– A
spe
cial
ist
who
test
s he
arin
g an
d he
lps
peop
le w
ith
hear
ing
loss
(hea
ring
aid
s,
lip/s
peec
h re
adin
g, a
udit
ory
trai
ning
& in
divi
dual
&
fam
ily s
uppo
rt).
• T
he E
ar S
peci
alis
t (E
NT
otol
ogis
t) –
A p
hysi
cian
wh
o sp
ecia
lizes
in t
he m
edic
al &
sur
gica
l tre
atm
ent
of e
ar &
hea
ring
dis
orde
rs.
ABO
UT O
TIT
IS M
EDIA
…..
Oti
tis
med
ia is
an
infl
amm
atio
n of
the
eard
rum
and
the
mid
dle
ear.
The
infl
amm
atio
n is
ca
used
by
swel
ling
and
bloc
kage
of
the
eust
achi
an t
ube
that
the
n cr
eate
s a
vacu
um
resu
ltin
g in
flu
ids
pool
ing
behi
nd t
he e
ardr
um.
This
pro
blem
cre
ates
a w
arm
, wet
pla
ce w
here
ge
rms
can
thri
ve a
nd o
ften
lead
to
ear
infe
ctio
ns.
Med
ical
tre
atm
ent
of e
ar in
fect
ions
usu
ally
in
clud
es “w
atch
ing
and
wait
ing”
or
anti
biot
ics.
Tu
bes
may
be
nece
ssar
y if
the
ear
infe
ctio
ns d
o no
t cl
ear
with
tre
atm
ent
or if
the
y re
occu
r.
Flui
d be
hind
the
ear
drum
oft
en c
ause
s a
hear
ing
loss
whi
ch la
sts
as lo
ng a
s th
ere
is f
luid
or
the
abn
orm
al c
ondi
tion
is p
rese
nt.
Perm
anen
t da
mag
e ca
n re
sult
wit
hout
pro
per
trea
tmen
t.
EAR
CARE
TIP
S:
• N
ever
put
any
thin
g in
you
r ch
ild’s
ear
• Fo
r ge
nera
l cle
anin
g us
e a
wash
clo
th o
n th
e ou
ter
part
of
the
ear
• Fo
r tu
bes,
fol
low
your
phy
sici
ans
reco
mm
enda
tion
s re
gard
ing
wate
r in
the
ear
s •
Cons
ult
your
phy
sici
an o
r au
diol
ogis
t re
gard
ing
prob
lem
s of
wax
in t
he e
ars
25
HIT
OS
DE
L D
ESA
RR
OL
LO
PA
RA
AU
DIC
IÓN
Y H
AB
LA
Para
el P
rim
er M
es S
u N
iño(
a) D
ebe:
•
hac
er ru
idos
de
repe
nte
alto
s o d
e so
bres
alto
•
llor
ar
• a
rrul
lar o
gor
jear
•
ser c
onso
lado
por
ruid
os su
aves
o v
oces
con
ocid
as
Para
los T
res M
eses
Su
Niñ
o(a)
Deb
e:
• h
acer
ruid
os v
ocal
s com
o “o
oo”
y “a
aa”
Para
los C
uatr
o M
eses
Su
Niñ
o(a)
Deb
e:
• o
casi
onal
men
te m
over
se o
des
perta
r cua
ndo
se
hace
un
ruid
o fu
erte
o a
lgui
en h
abla
mie
ntra
s est
a du
rmie
ndo
calla
dam
ente
Pa
ra lo
s Sei
s Mes
es S
u N
iño(
a) D
ebe:
•
bal
buce
ar (“
baba
”, “
gaga
”, e
tc.)
• ta
rtar d
e im
itar c
ambi
os e
n el
tono
de
la v
oz
• v
olte
ar su
cab
eza
haci
a la
fuen
te
Para
los S
iete
Mes
es S
u N
iño
Deb
e:
• v
olte
ar su
cab
eza
cuan
do se
le h
abla
de
atra
s •
em
peza
r a u
sar a
lgun
os so
nido
s de
cons
onan
ts
tale
s com
o “b
”, “
d”, “
f”, “
m”,
y “
p”
Para
los N
ueve
Mes
es S
u N
iño
Deb
e:
• v
olte
ar su
cab
eza
haci
a un
soni
do h
echo
de
lado
y
loca
lizar
lo si
est
a a
o de
bajo
de
su n
ivel
vis
ual
• o
casi
onal
men
te b
rinca
r o a
sust
arse
cua
ndo
hay
un
soni
do m
uy fu
erte
•
det
ener
se c
uand
o se
le d
ice
que
“no”
o se
le la
ma
por s
u no
mbr
e •
act
uar d
ifere
nte
de c
uand
o se
le h
abla
am
igab
lem
ente
a u
n to
no e
noja
do
• im
itar l
os so
nido
s de
habl
a de
otra
gen
te
Para
los D
oce
Mes
es S
u N
iño(
a) D
ebe:
•
resp
onde
r a la
mus
ica
y al
can
to
• e
ntre
gar u
n ju
guet
e cu
ando
se le
pid
e de
atra
s
• e
mpe
zar a
repi
tir a
lgun
os so
nido
s que
ust
ed le
hag
a •
usa
r una
pal
abra
cor
rect
amen
te a
parte
de
“mam
a” y
“p
apa”
•
vol
tear
la c
abez
a en
cua
lqui
er d
irecc
ión
para
loca
lizar
al
guna
fuen
te d
e so
nido
inte
resa
nte
Para
los Q
uinc
e M
eses
Su
Niñ
o(a)
Deb
e:
• u
sar d
e 3
a 5
pala
bras
cor
rect
amen
te
• id
entif
icar
obj
etos
con
ocid
os c
uand
o se
les n
ombr
a si
n m
irar s
us la
bios
Pa
ra lo
s Die
cioc
ho M
eses
Su
Niñ
o(a)
Deb
e:
• in
dica
r sus
que
rere
s al n
ombr
ar lo
s obj
etos
•
apu
ntar
a a
lgún
retra
to c
onoc
ido
cuan
do se
le n
ombr
a si
n m
irar s
us la
bios
•
tene
r un
voca
bula
rio d
e 6
a 10
pal
abra
s Pa
ra lo
s Vie
ntic
uatr
o M
eses
Su
Niñ
o(a)
Deb
e:
• o
casi
onal
men
te e
xpre
sars
e en
fras
es d
e 2
pala
bras
•
apu
ntar
a c
ierta
s par
tes d
el c
uerp
o si
n m
irar s
us la
bios
•
tene
r un
voca
bula
rio d
e 10
a 1
5 pa
labr
as
Para
los T
res A
ños S
u N
iño(
a) D
ebe:
•
usa
r fra
ses d
e 2
a 3
pala
bras
•
tene
r un
voca
bula
rio d
e 20
0 a
300
pala
bras
Pa
ra lo
s Cua
tro
Año
s Su
Niñ
o(a)
Deb
e:
• d
ecir
la m
ayor
ia d
e so
nido
s cor
rect
amen
te c
on
exce
pció
n de
qui
zás “
r”, “
l”, “
th”,
y “
s”
Para
los C
inco
Año
s Su
Niñ
o(a)
Deb
e:
• u
sar t
odos
los s
onid
os c
orre
ctam
ente
con
exc
epci
ón
de q
uizá
s “s”
y “
th”
• u
sar l
a m
ism
a es
truct
ura
de fr
ases
que
la fa
mili
a
LA
AU
DIC
IÓN
D
E S
U
N
IÑO
(A)
LA
AU
DIC
IÓN
ES
IMPO
RT
AN
TE
…
PAR
A H
AB
LA
R
Lo
s niñ
os a
pren
den
a
habl
ar a
l esc
ucha
r PA
RA
APR
EN
DE
R –
Muc
ho d
e lo
que
los n
iños
apre
nden
es p
or a
udic
ión
PAR
A D
ESA
RR
OL
LO
SO
CIA
L –
Los n
iños
nec
esita
n po
der
co
mun
icar
par
a ha
cer a
mig
os
26
¿ PO
R Q
UÉ
ES
IMPO
RT
AN
TE
QU
E S
E R
EV
ISE
L
A A
UD
ICIÓ
N D
E S
U N
IÑO
(A) C
AD
A A
ÑO
? •
Su a
udic
ión
pued
e ca
mbi
ar
• So
lam
ente
un
exam
en a
uditi
vo p
uede
dec
irle
cuán
to e
scuc
ha su
niñ
o(a)
•
Prob
lem
as a
uditi
vos p
udie
ran
esta
r re
laci
ónad
os c
on p
robl
emas
méd
icos
•
La a
uditi
va e
s muy
impo
rtant
e pa
ra e
l de
sarr
ollo
del
hab
la y
leng
uaje
y a
pren
diza
je
¿C
ÓM
O S
E R
EV
ISA
LA
AU
DIC
IÓN
EN
LO
S N
IÑO
S?
Parte
1: A
udio
met
ría
• Se
revi
sa la
hab
ilida
d de
l niñ
o de
oír
soni
dos
suav
es e
n to
nos d
ifere
ntes
•
La h
abili
dad
de a
udic
ión
es d
eter
min
ada
por
com
o re
spon
de p
or m
edio
de
audi
fono
s o
boci
nas
• Pa
ra n
iños
muy
peq
ueño
s o m
uy d
ifici
les d
e pr
obar
se p
uede
n us
ar o
tras t
ecni
cas
Parte
2: T
impa
nom
etría
•
Una
med
ida
de q
ué ta
n bi
en tr
abaj
a el
can
al d
el
oído
, oíd
o m
edio
, la
trom
pa d
e Eu
staq
uio
y lo
s hu
esos
del
oíd
o m
edio
n •
Una
man
era
com
ún p
ara
revi
sar p
or li
quid
o de
tras d
el o
ído
med
io h
alla
do fr
ecue
ntem
ente
co
n in
fecc
ione
s del
oíd
o N
iños
con
resu
ltado
s ano
rmal
es e
n cu
alqu
iera
de
esta
pr
ueba
s se
refie
ren
para
pru
ebas
adi
cion
ales
o p
ara
trate
mie
nto
méd
ico.
Si s
u ni
ño p
asa
los r
evis
os p
ero
toda
vía
le p
reoc
upa
la a
udic
ión
de su
niñ
o, c
onsu
lte u
n au
diól
ogo.
FAC
TO
RE
S D
E R
IESG
O P
AR
A A
UD
ICIÓ
N
Pérd
ida
Perm
anen
te A
uditi
va
• U
n m
iem
bro
de fa
mili
a co
n pé
rdid
a pe
rman
ente
au
ditiv
a de
sde
su n
iňez
•
Infe
ccio
nes p
rese
ntes
al n
acim
ient
o (c
omo
rube
ola,
C
MV
, her
pes,
o si
filis
) •
Alu
mbr
amie
nto
o na
cim
ient
o di
fícil
que
afec
to la
resp
iraci
ón d
el b
ebé
• P
eso
al n
acim
ient
o de
men
os d
e 3
½ li
bras
•
Apa
rienc
ia e
xtra
ña d
e la
cab
eza,
car
a o
oído
del
beb
é
(incl
uido
hen
didu
ra d
el p
alad
ar o
ore
jas m
alfir
mad
as)
• E
l beb
é ne
cesi
ta c
uida
do in
tens
ivo
neon
atal
(NIC
U)
por d
os d
ías o
mas
des
pués
de
nace
r •
El b
ebé
tiene
un
deso
rden
o in
fecc
ión
del c
ereb
ro
(c
omo
men
ingi
tis)
• E
l beb
é ne
cesi
ta u
na tr
ansf
usió
n de
sang
re
Infe
ccio
nes D
el O
ído
Y O
titis
Med
ia
• In
fant
es q
ue ti
enen
su p
rimer
a in
fecc
ión
de o
ído
en o
an
tes d
e lo
s 6 m
eses
de
edad
•
Niñ
os c
on a
norm
alid
ades
tale
s com
o he
ndid
ura
del
labi
o/pa
lada
r o sí
ndro
me
de D
own
• In
fant
es o
niñ
os p
eque
ños e
n am
bien
tes d
onde
se
cuid
an n
iños
•
Dán
dole
bib
erón
al b
ebé
mie
ntra
s aco
stad
o •
Infe
ccio
nes r
espi
rato
rias
• A
lerg
ias
• A
deno
ideo
s gra
ndes
¿Q
UIÉ
N P
UE
DE
AY
UD
AR
LÉ
CO
N L
OS
OÍD
OS
Y
AU
DIC
IÓN
DE
SU
NIÑ
O(A
)?
• E
l Aud
iólo
go- U
n es
peci
alis
ta q
ue p
rueb
a au
dioc
ión
y ay
uda
con
perd
ida
audi
tiva
(ayu
das a
uditi
vas,
leer
lo
s lab
ios,
entre
nam
ient
o au
dito
rio y
apo
yo
indi
vidu
al y
de
fam
ilia)
. •
Al M
édic
o- tr
ata
cond
icio
nes m
edic
as in
clui
das l
as
rela
cion
adas
con
otit
is m
edia
•
El E
spec
ialis
ta d
el O
ído
(EN
T o
otól
ogo)
– U
n m
édic
o qu
ien
espe
cial
iza
en e
l tra
tam
ient
o m
édic
o o
quirú
rgic
o de
des
orde
nes a
uditi
vas
E
N C
UA
NT
O A
L O
TIT
IS M
ED
IA…
Otit
is m
edia
es u
na in
flam
ació
n de
la
mem
bran
a de
l tim
pano
y e
l oíd
o m
edio
. La
infla
mac
ión
es c
ausa
da p
or lo
hin
chad
o y
bloq
ueo
de la
trom
pa d
e Eu
staq
uio
que
lueg
o pr
oduc
e un
vac
ío c
rean
do lí
quid
os
esta
ncas
os d
etra
s de
la m
embr
ana
detrá
s de
la
mem
bran
a de
l tím
pano
. Est
e pr
oble
ma
prod
uce
un lu
gar
cale
ntito
y h
umed
o do
nde
mic
robi
os c
rece
n y
lleva
a
infe
ccío
nes d
el o
ído.
El tr
atam
ient
o m
édic
o de
infe
ccío
nes d
el
oído
nor
mal
men
te in
cluy
e “e
sper
ar y
ver
” o
antib
iótic
os.
Pudi
eran
ser n
eces
ario
s tub
os si
las
infe
ccio
nes n
o se
qui
tan
con
trata
mie
nto
o si
oc
cure
n nu
evo.
Flui
do d
etrá
s de
la m
embr
ana
de tí
mpa
no
norm
alm
ente
cau
sa u
na p
erdi
da a
uditi
va q
ue p
uede
du
rar m
ient
ras q
ue e
l líq
uido
o la
con
dici
ón a
norm
al
este
pre
sent
e. D
año
perm
anen
te p
uede
resu
ltar s
in e
l tra
tam
ient
o ap
ropi
ando
. SU
GE
RE
NC
IAS
PAR
A E
L C
UID
AD
O D
E
OÍD
OS
•
Nun
ca p
onga
CU
ALQ
UIE
R C
OSA
DEN
TRA
del
oí
do d
e su
niñ
o(a)
•
Par
a lim
piez
a en
gen
eral
usa
una
toal
la e
n la
par
te
de a
fuer
a de
l oíd
o •
Par
a tu
bos,
siga
las r
ecom
enda
cion
es d
e su
m
édic
o co
n re
spec
to a
l agu
a en
los o
ídos
•
Con
sulte
con
su m
édic
o o
audi
ólog
o co
n re
spec
to
o pr
oble
mas
de
cera
en
los o
ídos

27
Appendix E
HANDOUT:
Suggestions for Parents of Children with Middle Ear Problems
This handout is provided in English and Spanish. It may be reproduced for parents, daycare
providers, teachers, and other pertinent parties.

28
SUGGESTIONS FOR PARENTS OF CHILDREN
WITH MIDDLE EAR PROBLEMS
THE IMPORTANCE OF TALKING Talking to your child is necessary for his/her language development. Since children usually imitate what they hear, how much you talk to your child, what you say, and how you say it will affect how much and how well your child talks.
LOOK Look directly at your child’s face and wait until you have his/her attention before you begin talking.
CONTROL DISTANCE Be sure that you are close to your child when you talk (no farther than 5 feet). The younger the child, the more important it is to be close.
LOUDNESS Talk slightly louder than you normally do. Turn off the radio, TV, dishwasher, etc. to remove background noise. BE A GOOD SPEECH MODEL • Describe to your child daily activities as they occur. • Expand what your child says. For example, if your child points and says “car”, you say “Oh, you want the car.” • Add new information. You might add, “That car is little.” • Build vocabulary. Make teaching new words and concepts a natural part of every day’s activities. Use new words while shopping, taking a walk, washing dishes, etc. • Repeat your child’s words using adult pronunciation. PLAY AND TALK Set aside some times throughout each day for “play time” for just you and your child. Play can be looking at books, exploring toys, singing songs, coloring, etc. Talk to your child during these activities, keeping the conversation at his/her level. READ Begin reading to your child at a young age (under 12 months). Ask a librarian for books that are right for your child’s age. Reading can be a calming-down activity that promotes closeness between you and your child. Reading provides another opportunity to teach and review words and ideas. Some children enjoy looking at pictures in magazines and catalogs. DON’T WAIT
Your child should have the following skills by the ages listed below: 18 months: 3 word vocabulary. 2 years: 25-30 word vocabulary and several 2-word sentences. 2 ½ years: At least a 50 word vocabulary and 2-word sentences consistently.
IF YOUR CHILD DOESN’T HAVE THESE SKILLS, TELL YOUR DOCTOR. A referral to an audiologist and speech pathologist may be indicated. Hearing and language testing may lead to a better understanding of your child’s language development. Adapted from “Suggestions for Parents…”Noel Matkin, Ph.D., Professor of Audiology, University of Arizona, 1960.
Screening Children for Communication Disorders
A Project of the Robert Wood Johnson Foundation and University of Colorado Health Sciences Center

29
SUGERENCIA PARA LOS PADRES DE NIÑOS CON PROBLEMAS DEL OÍDO MEDIO
LA IMPORTANCIA DE HABLAR Hablar con su Niño/a es necessario para el desarrollo del lenguaje. Porque los niños imitan lo que oyen, lo que usted le dice a su Niño/a le afectará como habla y cuanta habla. MIRAR Mire directamente a la cara de su niño/a y espere hasta que usted tenga la atención de él/ella antes de empezar a hablar. CONTROL DE LA DISTANCIA Asegúrese de estar cerca de su Niño/a cuando le habla (no más lejos de 5 pies). Mientras mas joven es su niño/a, mas importante es estar cerca de él/ella. VOZ ALTA Hable en una voz un poco más alta de lo que usa normalmente. Apague el radio, la televisión, el lavaplatos, etc. para quitar el ruido del ambiente. SER MODELO DEL BUEN HABLA • Descríbale a su niño/a las actividades diaries cuando ocurren. • Extienda lo que dice su niño/a. Por ejemplo, si su niño/a apunta y dice “carro,” diga usted, “O, tu quieres el carro.” • Aumente o expanda las frases de su niño/a con información nueva. Tal vez usted puede anadir, “Ese carro es chiquito.” • Desarrolle más el vocabulario de su niño/a. Trate de enseñarle palabras y conceptos nuevos como parte natural de las actividades diarias. Use palabras nuevas al ir de compras, al tomar paseos, al lavar los trastes, etc. • Repita las palabras que usa su niňo/a usando pronunciación adulta. JUGAR Y HABLAR Trate de sacar tiempo durante el día solo para que usted juegue con su niño/a. Puede ser tiempo para ver libros, explorar juguetes, cantar canciones, colorear, etc. Hablele a su niño/a durante de estas actividades, manteniendo la conversación al nivel de él/ella. LEER Empiece a leerle a su niño/a cuando este chiquito (menos de 12 meses). Pídale a la bibliotecaria los libros que son apropriados para la edad de su niño/a. La lectura puede ser una actividad para calmar a su niño/a. La lectura puede ser una actividad para clamar a su niño/a y promueve una cercania entre usted y su niño/a. La lectura provee otra oportunidad para enseñarle nuevas palabras e ideas. A algunos niño les gusta ver revistas y catalogos. NO ESPERE Su niño/a debe de tener las siguientes destrezas para las edades anotadas: 18 meses: vocabulario de 3 palabras 2 años: vocabulario de 25-30 palabras y varias frases de 2-palabras. 2 ½ años: vocabulario de 50 palabras y el uso consistente de frases de 2-palabras. SI SU NIÑO/A NO TIENE ESTAS DESTREZAS, DIGALE A SU MÉDICO. Esto puede indicar que su niño/a necesita ser referido a un audiólogo o terapista del habla y lenguaje (fonoaudiólogo). Un examen para el niño/a de audición y de lenguaje le puede ayudar a entender mejor el desarrollo de lenguaje de su niño/a. Adaptado de: “Suggestions for parents…” Noel Matkin, Ph.D., Professor of Audiology, University of Arizona, 1980
EXAMINANDO A LOS NIÑOS PARA PROBLEMAS DE LA COMUNICACIÓN A Project of the Robert Wood Johnson Foundation and University of Colorado Health Sciences Center

30
APPENDIX F
SAMPLE FORMS
(It may be helpful to reproduce some of these forms on NCR paper.)

31
SCREENING PERMISSION
Annual hearing screening for all children from birth to age eight has been recommended by the Colorado Early Childhood Hearing Screening Task Force. Early identification of hearing loss and appropriate treatment greatly reduces the changes of problems later. The screening is quick, simple and harmless. I hereby consent to the provision of hearing and/or tympanometry screening for: (Full Name of Child) (Date of Birth) (Parent or Legal Guardian Signature) (Date)
RELEASE OF INFORMATION It is generally agreed that sharing information regarding the results of hearing and/or tympanometry screening with those individuals or agencies that are concerned with the child’ primary health care provider, local school district, and local public health agency. Please mark the agencies that you wish to receive the screening results. I hereby agree to have the results of hearing and/or tympanometry screening shared with the following individuals or agencies. copy to parent/legal guardian (this copy may be shared with any person or agency at the parent’s or guardian’s discretion) copy to local school district copy to local public health agency copy to primary care provider: (Full Name of Child) (Date of Birth) (Parent or Legal Guardian Signature) (Date)
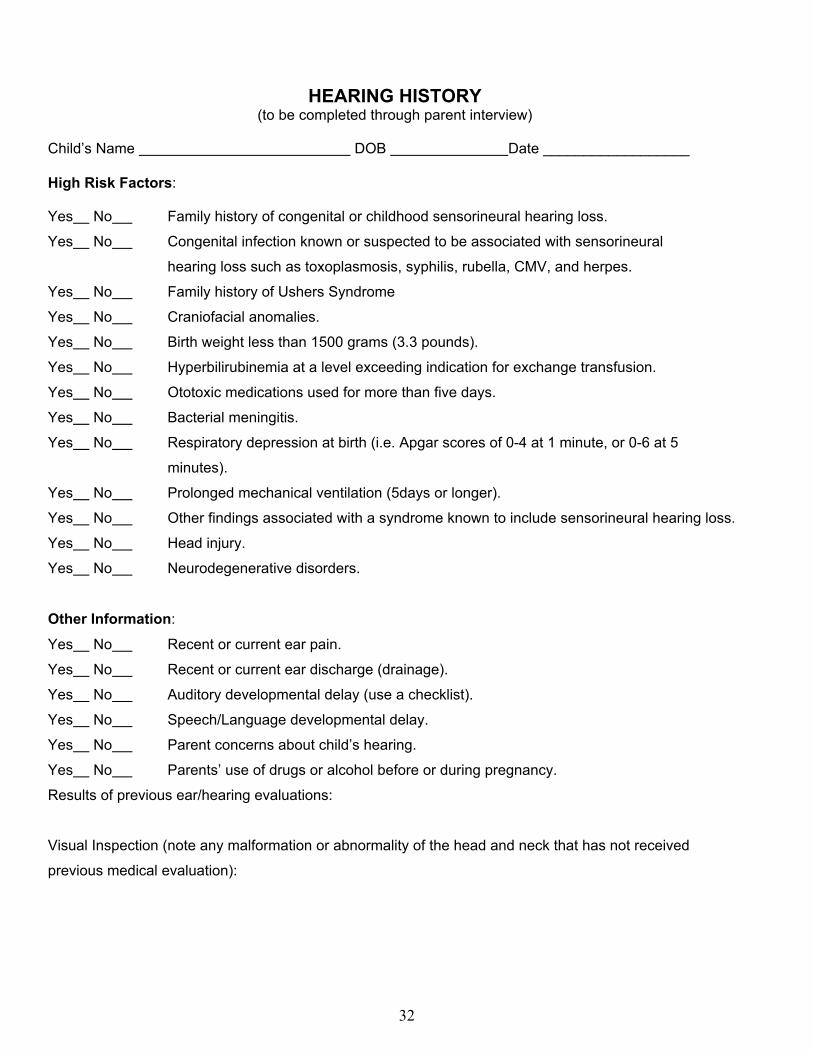
32
HEARING HISTORY (to be completed through parent interview)
Child’s Name DOB Date __________________ High Risk Factors: Yes No Family history of congenital or childhood sensorineural hearing loss.
Yes No Congenital infection known or suspected to be associated with sensorineural
hearing loss such as toxoplasmosis, syphilis, rubella, CMV, and herpes.
Yes No Family history of Ushers Syndrome
Yes No Craniofacial anomalies.
Yes No Birth weight less than 1500 grams (3.3 pounds).
Yes No Hyperbilirubinemia at a level exceeding indication for exchange transfusion.
Yes No Ototoxic medications used for more than five days.
Yes No Bacterial meningitis.
Yes No Respiratory depression at birth (i.e. Apgar scores of 0-4 at 1 minute, or 0-6 at 5
minutes).
Yes No Prolonged mechanical ventilation (5days or longer).
Yes No Other findings associated with a syndrome known to include sensorineural hearing loss.
Yes No Head injury.
Yes No Neurodegenerative disorders.
Other Information:
Yes No Recent or current ear pain.
Yes No Recent or current ear discharge (drainage).
Yes No Auditory developmental delay (use a checklist).
Yes No Speech/Language developmental delay.
Yes No Parent concerns about child’s hearing.
Yes No Parents’ use of drugs or alcohol before or during pregnancy.
Results of previous ear/hearing evaluations:
Visual Inspection (note any malformation or abnormality of the head and neck that has not received
previous medical evaluation):
33
HEARING DEVELOPMENT CHECKLIST These checklists may be used to obtain information from parents regarding developmental milestones for the auditory, language, and speech development of their child. They should not be used in place of an individually administered hearing screening. Every child should have his/her hearing screened annually. Print checklist front to back with English and Spanish on opposite sides. There is also room for you to insert your agency’s name when you reproduce these flyers.

34
DOES YOUR CHILD HAVE A HEARING LOSS?
(Two to five years checklist) Questions for parents who suspect their child has a hearing problem. Name of Child_______________________
Age_______ Today’s Date__________________
1. Does your child frequently ask you to repeat? …………………. Yes No 2. Does your child frequently request the TV or stereo be louder than others in the family? ……………………… Yes No 3. Does your child often respond to a question with an unrelated answer?………….. Yes No 4. Does your child daydream or seem inattentive?……………………… Yes No 5. Is your child a behavior problem or seem withdrawn?………………… Yes No 6. Is your child’s speech poorer than you expect for a child at this age?… Yes No 7. Does your child respond inconsistently to sound (hears it sometimes and other times does not?)……………………… Yes No 8. Does your child watch your face when you talk?……………………………. Yes No 9. Does your child speak abnormally soft or loud, or is the pitch usually high or low?…………………… Yes No 10. Does your child have lots of ear infections or cold?…………… Yes No If your answer to any of these questions is “YES”, a hearing evaluation is indicated. Remember: The earlier a hearing problem is discovered, the earlier the child can be helped. No child is ever too young to be tested.
The above checklist is provided by the New York League for the Hard of Hearing.
DOES YOUR BABY HEAR? (Birth to two years checklist)
The most important time for your baby’s learning is between birth and 3 ½ years. This is also the time your baby will learn how to communicate – first to understand what people say and then to start talking. Your baby must have normal hearing for these skills to develop adequately. As the parent, you are the best person to observe your baby’s auditory development by being alert for the following symptoms. Name of Child _________________________
Age________ Today’s Date __________________
1. Does your newborn baby startle to a loud sound or clap within 3-6 feet? …… Yes No 2. Does your three month old baby stop moving or stop crying when you call him/her or make an unfamiliar noise?….. Yes No 3. Does your fifteen month old baby turn toward you when you call his/her name from behind?………………………………. Yes No 4. Does your fifteen month old baby identify familiar objects? Does he/she repeat simple words?…………… Yes No 5. Does your two year old follow simple directions, repeat words and phrases?……………………………….. Yes No 6. Is your child disturbed by loud sounds when he’s/she’s asleep?………………. Yes No 7. Does your child turn when you call? ….. Yes No 8. Does your child pay attention to noises? Yes No 9. Does your child use gestures to communicate/point? ……………………… Yes No 10. Does your child get frequent colds or ear infections? ………………………….. Yes No If your answer to question 1-8 is “NO” or your answer to questions 9 or 10 is “YES”, a hearing evaluation is indicated. Remember: No baby is ever too young to have a hearing test. The earlier we discover the problem, the earlier we can help.
The above checklist is provided by the New York League for the Hard of Hearing.
¿OYE SU NI NIÑITO?
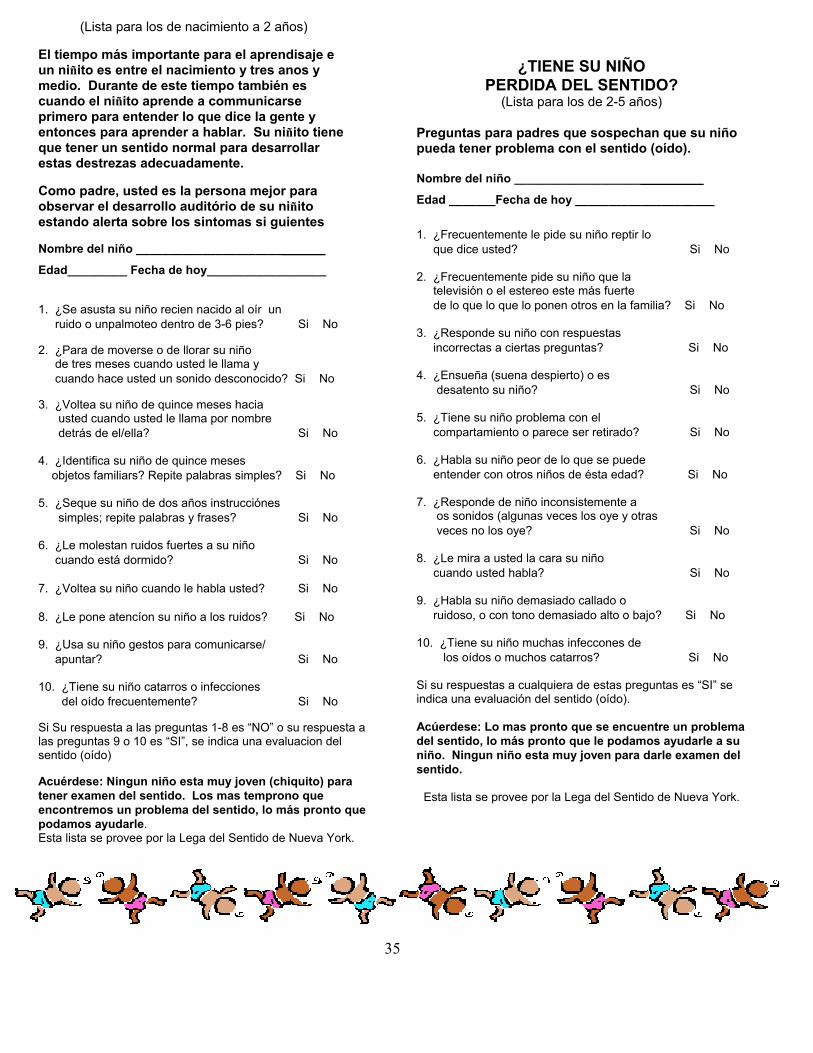
35
(Lista para los de nacimiento a 2 años) El tiempo más importante para el aprendisaje e un niñito es entre el nacimiento y tres anos y medio. Durante de este tiempo también es cuando el niñito aprende a communicarse primero para entender lo que dice la gente y entonces para aprender a hablar. Su niñito tiene que tener un sentido normal para desarrollar estas destrezas adecuadamente. Como padre, usted es la persona mejor para observar el desarrollo auditório de su niñito estando alerta sobre los sintomas si guientes Nombre del niño ______________________
Edad_________ Fecha de hoy__________________
1. ¿Se asusta su niño recien nacido al oír un ruido o unpalmoteo dentro de 3-6 pies? Si No 2. ¿Para de moverse o de llorar su niño de tres meses cuando usted le llama y cuando hace usted un sonido desconocido? Si No 3. ¿Voltea su niño de quince meses hacia usted cuando usted le llama por nombre detrás de el/ella? Si No 4. ¿Identifica su niño de quince meses objetos familiars? Repite palabras simples? Si No 5. ¿Seque su niño de dos años instrucciónes simples; repite palabras y frases? Si No 6. ¿Le molestan ruidos fuertes a su niño cuando está dormido? Si No 7. ¿Voltea su niño cuando le habla usted? Si No 8. ¿Le pone atencíon su niño a los ruidos? Si No 9. ¿Usa su niño gestos para comunicarse/ apuntar? Si No 10. ¿Tiene su niño catarros o infecciones del oído frecuentemente? Si No Si Su respuesta a las preguntas 1-8 es “NO” o su respuesta a las preguntas 9 o 10 es “SI”, se indica una evaluacion del sentido (oído) Acuérdese: Ningun niño esta muy joven (chiquito) para tener examen del sentido. Los mas temprono que encontremos un problema del sentido, lo más pronto que podamos ayudarle. Esta lista se provee por la Lega del Sentido de Nueva York.
¿TIENE SU NIÑO PERDIDA DEL SENTIDO?
(Lista para los de 2-5 años) Preguntas para padres que sospechan que su niño pueda tener problema con el sentido (oído). Nombre del niño ___________________
Edad _______Fecha de hoy _____________________ 1. ¿Frecuentemente le pide su niño reptir lo que dice usted? Si No 2. ¿Frecuentemente pide su niño que la televisión o el estereo este más fuerte de lo que lo que lo ponen otros en la familia? Si No 3. ¿Responde su niño con respuestas incorrectas a ciertas preguntas? Si No 4. ¿Ensueña (suena despierto) o es desatento su niño? Si No 5. ¿Tiene su niño problema con el compartamiento o parece ser retirado? Si No 6. ¿Habla su niño peor de lo que se puede entender con otros niños de ésta edad? Si No 7. ¿Responde de niño inconsistemente a os sonidos (algunas veces los oye y otras veces no los oye? Si No 8. ¿Le mira a usted la cara su niño cuando usted habla? Si No 9. ¿Habla su niño demasiado callado o ruidoso, o con tono demasiado alto o bajo? Si No 10. ¿Tiene su niño muchas infeccones de los oídos o muchos catarros? Si No Si su respuestas a cualquiera de estas preguntas es “SI” se indica una evaluación del sentido (oído). Acúerdese: Lo mas pronto que se encuentre un problema del sentido, lo más pronto que le podamos ayudarle a su niño. Ningun niño esta muy joven para darle examen del sentido.
Esta lista se provee por la Lega del Sentido de Nueva York.

36
HEARING SCREENING – SUMMARY FORM (group) Date: Screener:
Site:
Screening environment adequate (noise, visual distraction)? __Yes __No
List any equipment problems:
CHILD’S NAME AGE At-RISK1 AUDIO TYMP OAE RESCREEN COMMENTS
P = Pass; N = Not Pass
All Children should have their hearing screened at least annually.
1 Is the child “At-Risk” for hearing loss from history? (Yes or No)

37
HEARING SCREENING REPORT & REFERRAL
CHILD’S NAME: D.O.B. DATE: SCREENER: AGENCY
HEARING SCREENING 1000Hz 2000Hz 4000HZ
RIGHT EAR
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
LEFT EAR
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
OTOACOUSTIC EMISSIONS
PASS REFER
Right ear Left ear
TYMPANOMETRIC SCREENING VOLUME GRADIENT RESULTS
RIGHT EAR
PASS NOT PASS
LEFT EAR
PASS NOT PASS
Norms: (.4-1.occ) (less than 200) COMMENTS: FOLLOW-UP RECOMMENDATIONS: PASS (Annual Rescreen) AUDIOLOGICAL REFERRAL ( to: ) MEDICAL REFERRAL ( to: ) RESCREEN (date: ) MONITOR (date: )
Original – Child’s File Copy – Parents

38
MEDICAL REFERRAL AND RESPONSE
Dear: : This child is being referred to you for further evaluation. The following information has been gathered through recent screening. Please complete and return this form.
CHILD’S NAME: D.O.B. DATE: SCREENER: AGENCY:
HEARING SCREENING
1000Hz 2000Hz 4000HZ
RIGHT EAR
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
LEFT EAR
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
PASS (20dB) NOT PASS
OAE PASS REFER
Right ear Left ear
TYMPANOMETRIC SCREENING
VOLUME GRADIENT RESULTS RIGHT EAR
PASS NOT PASS
LEFT EAR
PASS NOT PASS
Norms: (.4-1.0cc) (less than 200 daPa) COMMENTS: MEDICAL EVALUATION OF: (child’s name) Diagnosis: Treatment Plan: Comments: Signature: Date: Return to:

Certificate for Hearing Screening
Hear! Hear! ___________________ (name of child)
Passed Hearing Screening Today
Date:______ Certified By:______________
The following procedures were used: __Tympanometry __Sound Booth VRA __Pure Tone Screening
__Otoacoustic Emissions

40
OYE! OYE! ___________________ (nombre del nino)
La Investigacíon de la Audicion
fue Logrado con Exito
Fecha:______ Certificado por:______________
Los procedimientos fueron utilizados: __Tympanometry __Sound Booth VRA __Pure tone screening
__Otoacoustic Emissions
Filename: EC Scrng Guidelines Directory: J:\Special Education\Cheryl Template: C:\Documents and Settings\macek_e\Application
Data\Microsoft\Templates\Normal.dot Title: COLORADO Subject: Author: NAHERGEN Keywords: Comments: Creation Date: 3/27/2002 12:41 PM Change Number: 2 Last Saved On: 3/27/2002 12:41 PM Last Saved By: johnson_c Total Editing Time: 0 Minutes Last Printed On: 3/27/2002 3:57 PM As of Last Complete Printing Number of Pages: 40 Number of Words: 9,312 (approx.) Number of Characters: 53,084 (approx.)