Embed Size (px)
Citation preview

Colonic Ulceration Associated with Nonsteroidal Anti-Inflammatory Drugs Report of Three Cases
Howard L. Kaufman, M.D., Andrew H. Fischer, M.D., Mitchell Carroll, M.D., James M. Becker, M.D.
From the Department of Surgery and Pathology, Carney Hospital and Boston University School of Medicine, Boston, Massachusetts
Nonsteroidal anti-inflammatory drugs (NSAIDs) are associ- ated with a variety of gastrointestinal side effects. Effects on the large intestine have been reported with increasing fre- quency. Recognition of NSMD-induced colonic lesions has been confounded by variable clinical presentations, variable pathologic findings, and unfamiliarity of this entity among clinicians. We have recently seen three cases of NSMD- induced cecal ulcerations in patients undergoing right co- lectomy. A correct preoperative diagnosis was not made in our patients, one of whom presented with an acute abdo- men and two in whom there was an inability to rule out carcinoma. The gross, radiographic, and histologic findings in each case consisted of a characteristic transverse ulcer- ation with thin diaphragm-like scarring. NSMD-induced ce- cal ulcers can have a variety of presentations to the general surgeon, are likely to be misdiagnosed preoperatively, but may be recognized based on characteristic gross features evident by radiography and colonoscopy, along with a care- ful history. Review of recent literature suggests that lapa- rotomy can be avoided when diagnosis is considered, but operation is indicated for complications, such as hemor- rhage, obstruction, or perforation, and when carcinoma cannot be adequately excluded. [Key words: Nonsteroidal anti-inflammatory agents; Colonic ulceration; Colectomy; Side effects]
Kaufman HL, Fischer AH, Carroll M, Becker JM. Colonic ulceration associated with nonsteroidal anti-inflammatory drugs: report of three cases. Dis Colon Rectum 1996;39: 705-710.
N onsteroidal anti- inflammatory agents (NSAIDs)
are a m o n g the most widely prescr ibed drugs in
the United States, with estimates of over 100 million
physician prescriptions for NSAIDs in addit ion to
more than 40 billion aspirin tablets sold o re> the -
counter each year. 1 Incidence of side effects while
taking NSAID therapy is quite high and has b e e n
repor ted to approach 70 percent w h e n patients re-
ceive long- term treatment. 2 The most frequently cited
complicat ions involve gas t roduodenal mucosa and
range f rom asymptomat ic petechiae to nonspecif ic
Present address of Dr. Fischer: Department of Pathology, Emory University-, Atlanta, Georgia 30322. Address reprint requests to Dr. Becket: Department of Surgery, Boston University School of Medicine, 88 East Newton Steer, Bos- ton, Massachusetts 02118.
gastroduodenit is and, less commonly , frank peptic
ulceration. The more severe side effects, such as hem-
orrhage and perforation, are usually associated with
advanced age and may por tend significant morbidi ty
and mortality.
The effect of NSAIDs on the small bowel has been
less well appreciated. However , several recent reports
indicate that small intestine mucosa may also be dam-
aged by NSAIDs. 3' 4 Small-bowel complicat ions range
from ulcerations and stricture formation to rarely
frank perforations. Al though the exact et iology of
these abnormalit ies is u n k n o w n , the small bowel mu-
cosa often shows a characteristic diaphragm-like
septa, which often narrows the lumen of the bowel .
The apex of these diaphragm-like strictures often con-
tains an area of ulceration with nonspecif ic acute and
chronic inflammation. 5
Al though it is generally recognized that NSAIDs can
exacerbate pre-existing inf lammatory bowel disease
(IBD), it is important to be aware that damage to
normal colonic mucosa can also occur. Nonspecific
NSAID-induced ulcerations, perforations, and charac-
teristic diaphragm-like strictures similar to those in the
small bowel are also repor ted in the colon. 6-9 Endo-
scopic, radiographic, and clinical features of NSAID-
associated colonic injury can be confused with other
colonic pathology, t~ resulting in operative interven-
t ion and co lec tomy w h e n simple cessation of drug therapy may be curative. 13
REPORT OF THREE CASES
Three patients with NSMD-associated colonic ul-
cerations were identified in a review of medical
records during a two-year period. All patients had
u n d e r g o n e co lec tomy with pathologic evaluat ion and
conf i rmed diagnoses. Characteristics of these cases
are presented herein.
705
706 KAUFMAN ETAL
Case 1
A 77-year-old white female with a history of degen- erative osteoarthritis presented with 15 days of non- radiating, right lower quadrant abdominal pain. Pa-
tient medications on admission to the hospital included salicylate and enteric-coated aspirin. In ad- dition, she had been taking indomethacin for 12
months for osteoarthritis, and this was s topped one month before presentation when a gastric ulcer was
diagnosed by endoscopy. Physical examination performed on admission re-
vealed a healthy-appearing female with minimum
right lower quadrant tenderness and the suggestion of a right lower quadrant mass on abdominal examina- tion. Stool was brown and stained positive on guiaic card testing for occult blood. Laboratory tests were remarkable for a hemoglobin of 9.5 mg/dl, and he- matocrit was 30.4 percent.
Colonoscopy was performed revealing partially ob- structing lesion in the ascending colon with friability
and ulceration. Pathologic examination of a biopsy specimen revealed ulceration with nonspecific acute and chronic inflammation and no evidence of malig-
nancy. Based on colonoscopy findings and a palpable mass in the right abdomen, a malignant tumor was suspected, and the patient underwent right colec- tomy. At laparotomy a small mass was palpable in the
cecum with some serosal adhesions. Pathologic examination of the specimen revealed
two areas of web-like transverse ulcerations involving
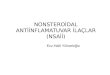
the cecum and proximal ascending colon (Fig. 1). Histology showed sharply demarcated transverse ul- cerations on the surface of the webs (Fig. 2) with
smaller, deeper ulcerations in the intervening mu- cosa. These unusual gross pathologic findings are consistent with NSAID-induced colonic ulcers. There were no granulomas, crypt abscesses, or crypt distor- tions elsewhere to suggest inflammatory bowel dis- ease, and there was no vasculitis. The patient had an uneventful recovery and had no recurrent symptoms
over a six-month period after stopping the salicylate.
Case 2
A 58-year-old male with a history of rheumatoid arthritis and osteoarthritis was admitted to the hospital with several weeks of melanotic stools. He com- plained of vague left lower quadrant pain radiating to his testicles, generalized weakness, dizziness, an- orexia, and a recent 10-pound weight loss. He re- ported using indomethacin and other NSAIDs in the
Dis Colon Rectum, June 1996
Figure 1. Gross photograph of ascending colon of Pa- tient 1 cut longitudinally through one of the transverse muscular diaphragms. The muscularis propria (black ar- rows) is thrown into a fold projecting toward the lumen. At the apex of this web is a sharply demarcated ulcer (de- lineated by white arrowheads) measuring only approxi- mately 3 mm across. The full length of this thin transverse ulceration was approximately 4 cm. Adjacent mucosa is without abnormality.
past for arthritis. Physical examination on admission revealed a pale, middle-aged male with mild left lower quadrant tenderness without masses. A rectal examination was performed, and no masses were palpable. Hemoccult of the stool was negative for
blood. The patient was found to have a hematocrit of 24
percent, and he was transfused with two units of packed red blood cells. A barium enema showed some mild diverticulosis of the left colon and a con- centric narrowing of the distal-ascending colon that
was suspicious for carcinoma (Fig. 3). Esophagogas- t roduodenoscopy was performed, and a small ante- rior wall duodenal ulcer was identified. A colonos- copy revealed few sigmoid diverticulum and an ascending colonic stricture with ulceration contained
within the strictured segment. Biopsy showed only
nonspecific ulcerations. Clinical diagnosis of a colonic malignancy was
made and a right colectomy performed. The speci- men revealed a stellate mucosal scar measuring 4 cm in diameter just distal to the ileocecal junction with
stricture formation at the ileocecal valve. A second area of ulceration measuring 5 mm was present at the appendiceal orifice, although the appendix appeared normal. Several other areas of characteristic dia- phragm-like transverse scarring were present in a pattern typical of NSAID-associated colonic ulcers at

Vol. 39, No. 6 COLONIC ULCERATION ASSOCIATED WITH NSAIDS 707
Figure 2. A histologic section stained with hematoxylin and eosin of the ulceration of Figure 1 is shown at 20• magnification. The lower-most portion of the picture shows the top of the muscular web (inner-most layer of the muscularis propria), with overlying nonspecific fibro- sis. The residual colonic mucosa at the upper left shows no evidence of previous injury, Le., there is no crypt drop-out or distortion and no regenerative change. Ulcer- ation starts abruptly and shows nonspecific features, with only mild chronic inflammation and no granulomas.
7, 10, 18, and 19 cm from the ileocecal junction. The overlying serosa showed focal adhesions. No longi- tudinal ulcerations or "cobblestone mucosa" was present, and no histologic evidence of inflammatory bowel disease or vasculitis was present.
The patient recovered from his operation and was told to stop taking indomethacin. He has remained free from further bleeding or abdominal pain for two years.
Case 3
A 63-year-old male with a 19-year history of dialysis for chronic renal failure secondary to a membranous nephropathy presented with a 12-hour history of right lower quadrant crampy abdominal pain associated with nausea and bilious vomiting. He had a history of severe shoulder and hip pain, which was diagnosed as dialysis-related amyloid arthropathy by biopsy, and
Figure 3. Barium enema of a patient on indomethacin with left lower quadrant abdominal pain and anemia. Mild sigmoid diverticulosis is present, and a narrowing, apple core-like lesion in the distal ascending colon (arrow) is identified.
he was prescribed nabumetone, a nonsteroidal anti- inflammatory agent. He was unable to tolerate this
medication and was started on double-strength tolme- tin for arthritis. He was again unable to tolerate the tolmetin because of gastrointestinal upset and
stopped taking it. His rheumatologist suggested a new NSAID called oxaprozin that he started along with misoprostol, which he was still taking on admission.
Physical examination revealed a somewhat anxious male with normal vital signs. Cardiac examination was remarkable for a soft Grade II/VI systolic ejection murmur at the apex with clear lung fields. There was right lower quadrant abdominal tenderness with lo-
calized guarding but no rebound. Rectal examination found no tenderness or masses. Stool was positive for occult blood on guiaic card testing.
The patient was admitted to the hospital and had a routine panel of blood chemistries and a plain ab- dominal roentgenogram performed. His white blood cell count was 10.5 with 5 percent eosinophilia; he- matocrit was 38.5 percent, and the remainder of lab- oratory values were normal. A computed tomography scan showed mild splenomegaly and moderate co- Ionic mucosal edema involving the mid ascending

708
colon with some narrowing of the lumen and a mild inflammatory reaction around the narrowed area. Un- able to exclude ischemic colitis, the patient was taken
to the operating room for celiotomy. At laparotomy, a walled-off area was identified
against the anterior abdominal wall on the right side.
Ascending colonic mesentery was edematous with thickened lymph nodes. The cecum appeared gray with areas at the base of the serosa that appeared nearly perforated with fibrous exudate on the surface. Vasculature was intact, and there was no evidence of
small bowel ischemia. The patient underwent an ex- tended right colectomy, and 10 cm of the terminal
ileum was also resected. Pathologic examination showed the cecum to be
sharply dilated, with serosal adhesions over the ileo- cecal junction. A small web-like area was seen in the ileal mucosa 5 cm from the ileocecal valve. The right
colon showed a sharply demarcated area of dusky discoloration, with patchy ulcerations delimited by
the ileocecal valve proximally and distally by the last of several web-like circumferential thickenings with
strictures 10 cm distal to the ileocecal valve. Histologic examination revealed transmural isch-
emic necrosis of the cecum and several transversely oriented fibromuscular web-like thickenings of the proximal ascending colon, typical of NSAID-induced
ulcerations. Ischemic necrosis ended abruptly at the site of the last fibromuscular web. The large area of contiguous involvement was unlike small vessel arte- rial occlusion, and the abrupt cut-off pattern was unlike large vessel arterial occlusion. The close asso- ciation of ischemic changes with mucosal strictures and muscular webs was most consistent with colonic
obstruction by the most distal fibromuscular web leading to cecal dilation and subsequent ischemia.
There were insignificant trace amyloid deposits seen
with Congo Red staining. The patient has s topped NSAIDs and is being
closely followed. He has not experienced any further episodes of abdominal pain or gastrointestinal upset.
D I S C U S S I O N
A possible association between NSAIDs and lower gastrointestinal (GI) ulceration has been suspected for years but has been difficult to prove. 12' 13 In 1988, Lang e t al . 14 reported a series of unusual small bowel diaphragm-like strictures that appeared to be specifi- cally associated with NSAIDs. Shortly thereafter, iden- tical diaphragm-like strictures of the right colon were
KAUFMAN ETAL Dis Colon Rectum, June 1996
associated with NSAIDs. 6-9 Currently, it is possible that these diaphragm-like webs of the small and large bowel are pathognomonic of NSAID injury. In the past two years, we have seen three patients undergo right colectomy for such NSAID-induced colonic ul- cerations. The three patients demonstrate a broad
range of clinical presentations, including hemorrhage, obstruction, and tumor. Diagnosis of NSAID-induced colonic ulcers is based on the characteristic gross appearance of the lesion, together with a history of NSAID use, and the absence of other apparent causes of cecal ulceration. The gross morphologic features that are characteristic of NSAID-induced strictures in- clude a sharply demarcated ulceration at the crest of a mucosal web with adjacent normal appearing colonic mucosa.6, 15 Webs may be difficult to detect by barium
studies, z Lesions can be easily seen by colonoscopy, 6
although it may be difficult to pass the scope beyond a tight muscular web. x6 The histologic appearance of
the web is nonspecific and consists of a thin ring of submucosal fibrosis. Associated ulcerations are also histologically nonspecific, with generally only a scant inflammatory reaction to a sharply defined ulcer. 5 Because nonspecific ulcerations may be found adja- cent to bulky rumors, malignancy may be difficult to exclude based on negative biopsy results.
Other local benign intestinal ulcerations may be attributable to various infectious etiologies, inflamma-
tory diseases, radiation injury, other drugs, and "idio- pathic" causes. 15 Important infectious causes of local
large bowel ulcerations include Campylobacter, ame- biasis, and Yersinia. In comparison with NSAID-asso- ciated ulcers, these infectious agents generally cause much more fibrosis and inflammation adjacent to the areas of ulceration, and ulcerations tend to be punc- rate or longitudinal. Ulcerations of tuberculosis tend to be transverse, and rarely circumferential, and they almost always primarily involve the small bowel. In- flammatory causes of benign focal colonic ulcerations include IBD, particularly Crohn's disease, Behget's
syndrome, and vasculitis. Crohn's disease usually demonstrates a poorly demarcated mixed longitudi- nal-transverse orientation of ulcers with a resulting cobblestone-like appearance and sharp lymphoplas- macytic infiltration of the lamina propria and deeper layers with occasional granulomas. Strictures in Crohn's disease are not as thin as diaphragms associ- ated with NSAIDs. Diaphragm-like webs have not been described in association with Behget's syn- drome; ulcers in Behget's tend to undermine deeply to the s e r o s a . 17' 18 The presence of the characteristics

Vol. 39, No. 6 COLONIC ULCERATION ASSOCIATED WITH NSAIDS 709
triad of aphthous oral ulcers, genital ulcers, and uve-
itis is important in establishing the diagnosis of Beh-
qet's syndrome. Vasculitis or ischemic colitis should
not cause sharply demarcated ulcerations. Radiation
injury can cause broad-based circumferential stric- tures and chronic ulcers. Potassium chloride-induced
ulcers are found in the small bowel and gold salts are
associated variously with colitis and discrete ulcers. 15
A careful drug history is important in evaluation of
any ulcerative condition of the bowel. It is possible that many, but not all, 19 of the remaining "idiopathic"
colonic ulcers are actually related to NSAIDs, because
most of the cases were reported before description of the characteristic diaphragm-like lesions. 2~ "Idiopath-
ic" colonic ulcers usually involve the cecum and as-
cending colon, 2~ and some have been associated with renal failure, 21 and with cytomegalovirus infection in transplant patients. 22
In addition to local ulcerations and diaphragm-like
webs, NSAIDs may lead to colitis resembling IBD or
exacerbate preexisting inflammatory bowel dis- ease.2, 11, 23-26 New onset colitis occurs rarely among
NSAID users, but as many as 10 percent of all cases of pre-existing colitis may be related to NSAIDs. 27 Mean
age appears to be in the sixth decade, and onset of
symptoms varies from a few days of treatment to years of use. 11 A possible association of NSAIDs with col-
lagenous colitis has been reported. 2 NSAID use may
also increase complications in patients with divertic- ulosis. Langman e t al. 28 found that NSAID use was
twice as common in 268 patients with diverticulosis
complicated by small or large bowel perforations or
hemorrhage than in an age-matched control group of diverticulosis patients without complications. Their
conclusion that NSAID use may cause complications
from diverticular disease has been supported by both retrospective 29 and prospective s t u d i e s 9
The mechanism of NSAID-related colonic ulcer- ation and web-like strictures is uncertain. Sharp de-
marcations together with high incidence of involve-
ment in the cecum and ascending colon suggest a
direct intraluminal effect of the drug, rather than a systemic effect. 31 In support of this, colonic compli-
cations are relatively more frequent in patients receiv-
ing slow-release formulations. 9 NSAID suppositories may also induce a local proctitis. 32, 33 The mechanism
of injury at the cellular level is obscure but may relate to disruption of a "cytoprotective effect" of prosta- glandins in the GI tract. 34' 35
Although a causal relationship be tween NSAIDs and colonic ulcerations is yet to be proven, the un-
usual pathologic findings seen in our patients seem to
be specific for NSAID-induced injury. Recognition of
NSAID-induced colonic ulcers is important because
surgery could be avoided or less radical surgery per-
formed. Treatment of NSAID colitis depends on the findings and severity of presenting s y m p t o m s Y Indi-
cations for surgical exploration or colonic resection
have not been previously described for patients with
NSMD-induced colonic ulcerations. In a recent re-
view of 40 patients with NSAID-induced colonic ul-
ceration, ten were treated with operation. The re-
mainder improved with cessation of NSAID therapy
and/or medical management , xl Patients who present
with gross perforation, hemorrhage associated with
hemodynamic instability, or those in w h o m carci-
noma cannot adequately be excluded represent clear surgical candidates. Those patients with less severe
symptoms can often be managed medically. 36 Patients
should not be placed back on NSAIDs in the future, because relapse may occur, sl None of our patients
has had recurrent ulceration during a six-month to
two-year follow-up without NSAID therapy.
NSAIDs are a widely prescribed group of drugs
used in a large variety of rheumatologic and inflam-
matory disease processes. Complications with NSAID use needs to be understood by both patient and
physician. Although upper GI effects of NSMDs are
well known, less common side effects of these agents
on the small bowel and colon have received less
attention. Despite a number of case reports in gastro-
enterology journals, the surgical literature is lacking in
reports of this problem or specific recommendat ions
for management . Our report of three patients with NSAID-induced colonic ulcerations illustrates the var-
ied clinical presentations of this entity. Recognition of
this diagnosis by surgeons, understanding the mor-
phologic features, and carefully taking a history in-
cluding specific questioning about NSAID use may
allow cessation of NSAID therapy and prevent unnec- essary operations.
REFERENCES
1. Gibson T. Nonsteroidal anti-inflammatory drugs-- another look. BrJ Rheumatol 1989;27:87-90.
2. Bjarnason I, Hayller J, Macpherson AJ, Russell AS. Side effects of nonsteroidal anti-inflammatory drugs on the small and large intestine in humans. Gastroenterology 1993; 104:1832--47.
3. Sturges HF, Krone CL. Ulcers and strictures of the jeju- num in a patient on long term indomethacin therapy. Am J Gastroenterol 1973;59:162-9.

710 KAUFMAN E T AL
4. Bjarnason I, Price AB, Zanelli G, et al. Clinico- pathological features of NSAID induced small intestinal strictures. Gastroenterology 1988;94:1070-4.
5. Levi S, de Lacey G, Price AB, Gumpel JM, Levi AJ, Bjamason I. 'Diaphragm-like' strictures of the small bowel in patients treated with nonsteroidal anti- inflammatory drugs. Br J Radiol 1990;63:186-9.
6. Whitcomb DC, Morton SP, Trellis DR, Evans BA, Becich MJ. 'Diaphragmlike' stricture of the colon during di- clofenac treatment. Arch Intern Med 1992;152:2341-3.
7. Pucius RJ, Charles AK, Adair HM, Rowe RC, HackingJC. Diaphragm-like strictures of the colon induced by non- steroidal anti-inflammatory drugs. Br J Surg 1993;80: 395-6.
8. Fellows JW, Clarke JM, Roberts PF. Non-steroidal anti- inflammatory drug-induced jejunal and colonic dia- phragm disease. Gut 1992;33:1424-6.
9. Halter F, Weber B, Huber T, Eigenmann F, Frey MP, Ruchti C. Diaphragm disease of the ascending colon: association with sustained-release diclofenac. J Clin Gastroenterol 1993;16:74-80.
10. Langman, MJ, Morgan L, Worrell A. Use of anti- inflammatory drugs by patients with small or large bowel perforation and haemorrhage. BMJ 1985;290:
347-9. 11. Gibson GR, Whitacre EB, Ricotti CA. Colitis induced by
nonsteroidat anti-inflammatory drugs. Arch Intern Med
1992;152:625-32. 12. Charuzi I, Ovnat A, Zirkin H, Peiser J, Sukenik S. Ibupro-
fen and benign cecal ulcer. J Rheumatol 1985; 12:188-9. 13. Debenham GP. Ulcer of the cecum during oxyphen-
butazone (Tandearil) therapy. Can Med Assoc J 1966;
94:1182-3. 14. LangJ, Price AB, Levi AJ, Burke M, GumpelJM, Bjarna-
son I. Diaphragm disease: pathology of disease of the small intestine induced by non-steroidal anti-inflamma- tory drugs. J Clin Pathol 1988;41:516-26.
15. Lewin KJ, Riddell RH, Weinstein WM. Miscellaneous diseases of the small and large intestines. In: Lewin KJ, Riddell RH, Weinstein WM, eds. Gastrointestinal pathol- ogy and its clinical implications. New York: Igaku- Shoin Medical Publishers, 1992:1086-151.
16. Monahan W, Starnes EC, Parker AL. Colonic strictures in a patient on long-term nonsteroidal anti-inflammatory drugs. Gastrointest Endosc 1992;38:385-6.
17. Baba S, Maruta M, Ando K, Teramoto T, Endo I. Intes- tinal Behget's disease: report of five cases. Dis Colon Rectum 1976;19:428-40.
18. Kasahara Y, Tanaka S, Nishino M, Umemnra H, Shiraha S, Kuyama T. Intestinal involvement in Behget's disease: review of 136 surgical cases in the Japanese literature. Dis Colon Rectum 1981;24:103-6.
19. Bjarnason I, Hopkinson N, Zanelli G, et al. Treatment of
Dis Colon Rectum, June 1996
non-steroidal anti-inflammatory drug induced enterop- athy. Gut 1990;31:777-80.
20. Shallman RW, Kuehner M, Williams G, Sajjad S, Sautter R. Benign cecal ulcers. Dis Colon Rectum 1985;28: 732-7.
21. Huded FV, Posner GL, Tick R. Nonspecific ulcer of the colon in a chronic hemodialysis patient. Am J Gastro- enterol 1982;77:913-6.
22. Sutherland DE, Chan FY, Foucar E, Simmons RL, Howard RJ, Najarian JS. The bleeding cecal ulcer in transplant patients. Surgery 1979;86:386-98.
23. Shanahan F, Targan S. Sulfasalazine and salicylate- induced exacerbation of ulcerative colitis. N Eng J Med 1987;317:455.
24. Schwartz HA. Lower gastrointestinal side effects of non- steroidal anti-inflammatory drugs. J Rheumatol 1981;8: 952~4.
25. Rampton DS, Sladen GE. Relapse of ulcerative procto- colitis during treatment with non-steroidal anti- inflammatory drugs. Postgrad MedJ 1981;57:297-9.
26. Kaufmann HJ, Taubin HL. Nonsteroidal anti-inflamma- tory drugs activate quiescent inflammatory bowel dis- ease. Ann Intern Med 1987;107:513-6.
27. Tanner AR, Raghunath AS. Colonic inflammation and nonsteroidal anti-inflammatory drug administration: an assessment of the frequency of the problem. Digestion 1988;41:116-20.
28. Langman MJ, Morgan L, Worrell A. Use of anti- inflammatory drugs by patients with small bowel per- foration and haemorrhage. BMJ 1985;290:347-9.
29. Corder A. Steroids, non-steroidal anti-inflammatory drugs, and serious septic complications of diverticular disease. BMJ 1987;295:1238.
30. Wilson RG, Smith AN, Macintyre, IM. Complications of diverticular disease and non-steroidal anti-inflammatory drugs: a prospective study. Br J Surg 1990;77:1103-4.
31. Huber TH, Ruchti CH, Halter F. Non-steroidal anti- inflammatory drug induced colonic strictures: a case report. Gastroenterology 1991;100:1119-22.
32. Pearson DJ, Stones NH, Bentley SJ. Proctocolitis induce by salicylate and associated with asthma and recurrent nasal polyps. BMJ 1983;287:1675.
33. Levy N, Gaspar L. Rectal bleeding and indomethacin suppositories. Lancet 1975;1:577.
34. Bjamason I, Zanelli G, Smith T, et al. Nonsteroidal antiinflammatory drug-induced intestinal inflammation in humans. Gastroenterology 1987;93:480-9.
35. Levi S, Shaw-Smith C. Non-steroidal anti-inflammatory drugs: how do they damage the gut? Br J Rheumatol
1994;33:605-12. 36. Bjarnason I, Hopkinson N, Zanelli G, et al. Treatment of
non-steroidal anti-inflammatory drug induced enterop- athy. Gut 1990;31:777-80.