Embed Size (px)
Citation preview
Gastro Highlights 2012in honour of
Prof Dr Michael Fried Sept 8th 2012
Eamonn M M Quigley MD FRCP FACP FACG FRCPIAlimentary Pharmabiotic Centre
Department of MedicineUniversity College Cork
CorkIreland
Colonic Motility Disorders: what have we learned over the past 20 years?

Michael Fried; a
Global PerspectiveChair, Guidelines and Publications WGO
Member Executive Committee and Governing Council

Michael Fried: a Global Perspective
Guidelines with Cascades
• Acute Diarrhea (UPDATED)• Colorectal Cancer Screening• Constipation (UPDATED)• Endoscope Disinfection (UPDATED)• Esophageal Varices• Helicobacter pylori in developing countries
(UPDATED)• Hepatitis B• HCC: a global perspective• IBD: a global perspective• IBS: a global perspective• NAFLD-NASH• Obesity (UPDATED)• Radiation protection in the endoscopy suite

Michael Fried: a Global Perspective
• Translated into multiple languages
• Published on line and in J Clin Gastro and elsewhere
• No 1 reason for web site hits
• Exponential rise in down-loads
• Have been used by national societies as their guidelines
• Ever-increasing citations
Guidelines
• Asymptomatic Gallstone Disease• Celiac Disease• Diverticular Disease• Dysphagia• Management of Acute Viral Hepatitis• Management of Strongyloidiasis• Needlestick injury and accidental exposure to blood
• Osteoporosis• Probiotics and Prebiotics(UPDATED)

Michael Fried: a Global Perspective
• Numerous related publications in high-impact journals


Congratulations and
a very big thank you from WGO

Colonic Motility Disorders
•Motility of the Colon
•Diverticular disease
•IBS
•Constipation
•The microbiota

Colorectal Motility

Colon
• Changes in tone– Right colon– Serves to accommodate
• Segmenting contractions– Throughout the colon
• Power contractions (High Amplitude Propagating Contractions, HAPCs)– Propulsive along the colon

80 mmHg
8 cm/sec 2 cm/sec
30 sec
High Amplitude Propagated Contractions (HAPCs)

HAPC

Defecation
• Pelvic floor musculature and the puborectalis relaxes to straighten out the anal canal
• External sphincter relaxes
• Internal sphincter relaxes
• Diaphragm and abdominal wall muscles contract

Contracted Puborectalis Increases Ano-Rectal Angle
Relaxed Puborectalis Decreases Ano-Rectal Angle

Diverticula – easy to find but difficult to incriminate!

Burden of Disease
*Kang JY, et al. Aliment Pharmacol Ther 2003;17:1189-1195
• Inpatient admissions UK 1989-2000*

Perforated Diverticular Disease
Humes DJ, et al. Gastroenterology 2009;136:1198-1205.
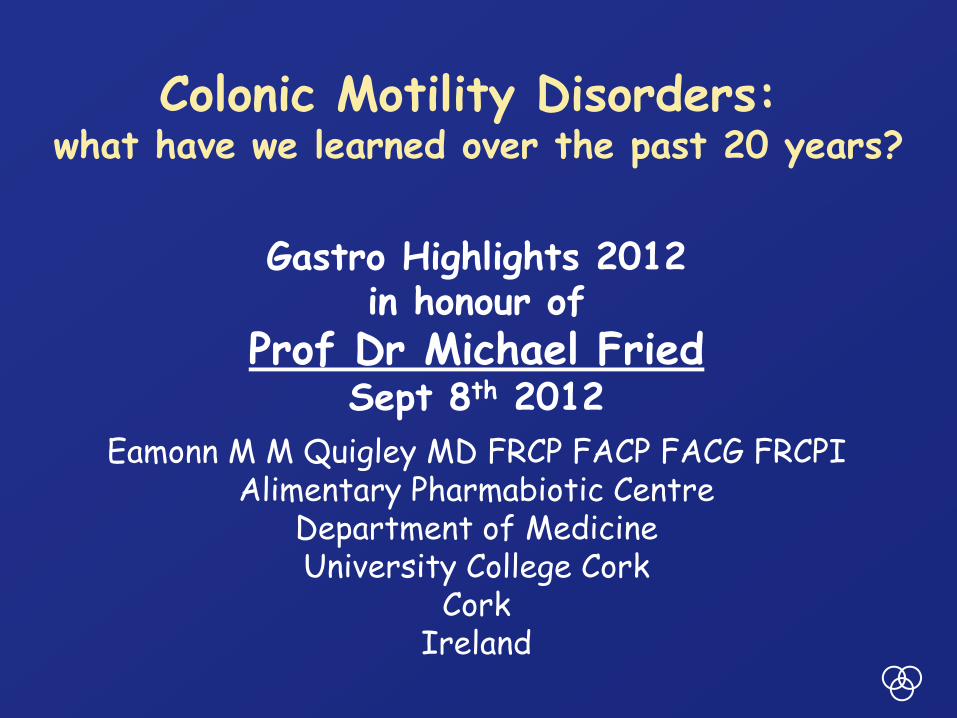
Design Findings Comments RefCase control study: 100 (symptomatic) DD cases vs 80 age and sex matched controls
Dietary fiber intake higher amongst controls
Participants hospitalized due to diverticulosis; symptoms may have influenced diet
Manousos et al
Prevalence of DD in 189 non-vegetarians vs 55 vegetarians
Diverticular disease was higher in the non-vegetarians
"A potential confounder is a possible causative effect for meat”
Gear et al
Case control study:40 (symptomatic) DD vs 80 age/sex matched controls
Dietary fiber intake higher amongst controls
Symptoms may have influenced their diet
Brodribb et al
43 881 US men aged 40-75 followed over 6 years
Dietary fiber intake lower in cases
Presence of DD not defined at outset; cannot rule out effects of DD on dietary choices
Aldoori et al
Case control study:86 right-sided DD cases and 106 controls
No relationship between DD and fiber consumption
May indicate different etiology or right-sided DD has fewer effects ondiet
Lin et al
Commane DM, et al. World J Gastroenterol 2009;28:2479-88.

What happens to diverticulitis?• < 10% require surgery on first admission
• 15-25% develop complications leading to surgery.
• Among those managed conservatively recurrence rate: 7-45%.
PLACEBO (n=41)
5-ASA (n=40)
5-ASA + Probiotic
(n=36)Withdrew due to surgery
1 (2.4%) 2 (5.0%) 0 (0%)
Recurrent Diverticulitis
8 (20%) 5 (12.5%) 4 (11.8%)
Stollman N, et al. Am J Gastroenterol 2010;105:S139.

Stollman N, et al. Am J Gastroenterol 2010;105:S139.
Persistent Symptoms
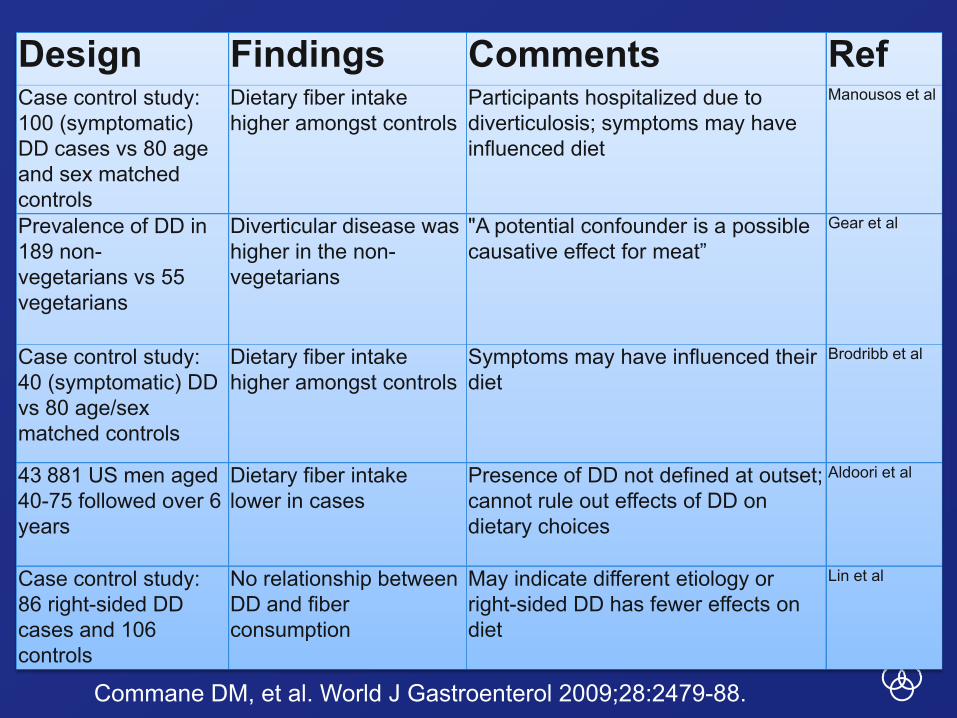
Painful Diverticular Disease
• 170 patients with diverticula on BE followed from 1999-2006– 34% recurrent abdo pain
• Median of 3.5 days per month• Median duration 1 hour
– Predictors of recurrent pain• History of acute diverticulitis• High score on HAD scale
• 51/261 with diverticula on BE had episodes of prolonged pain lasting on average 3 days– Recurrence rate 71% for those treated with an antibiotic
vs 34% not
Humes DJ, et al. Br J Surg 2008;95:195-198.Simpson J, et al. Eur J Gastroenterol Hepatol 2003;15:1005-10.
Irritable Bowel Syndrome(IBS)
The Traditional View• A “nuisance” rather than a syndrome
• Not a “real” entity but brought on by stress or anxiety
• Main issue is to exclude important “real/organic” disease
• Does not merit serious scientific investigation
• No worthwhile treatments

Irritable Bowel Syndrome(IBS)
A Changed Perspective
• Common world wide
• Can be disabling
• Varying phenotype
• Etiology unclear but gut-brain axis thought to play a pivotal role and new avenues being explored
• Therapeutic options remain limited, but considerable progress and interest

Quigley E al. J Clin Gastro 2012

Do we investigate too much?Radiation exposure in GI disorders
Desmond et al, Clin Gastroenterol Hepatol 2011

Do we investigate too much?Radiation exposure in GI disorders
Desmond et al, Clin Gastroenterol Hepatol 2011

Variable Spontaneous abortion, n
Crude OR (95% CI), abortion
Adjusted OR (95%
CI), abortion
Ectopic pregnancy,
n
Crude OR (95% CI), ectopic
pregnancy
Adjusted OR (95%
CI), ectopic
pregnancy
No IBS 12,041 Reference Reference 1,296 Reference ReferenceIBS but no depression/anxiety
3,593 1.26(1.21, 1.31)
1.21(1.16, 1.26)
453 1.42(1.26, 1.61)
1.35(1.19, 1.52)
IBS and depression anxiety
1,803 1.40(1.32, 1.48)
1.26(1.19, 1.34)
254 1.74(1.50, 2.01)
1.51(1.30, 1.74)
IBS and Pregnancy Outcome
Khashan et al, Clin Gastroenterol Hepatol 2012 (in press)

IBS Pathophysiology
• Heredity; nature vs nurture
• Dysmotility, “spasm”
• Visceral Hypersensitivity
• Altered CNS perception of visceral events
• Psychopathology
• Infection/Inflammation
• Altered Microbiota

What factors precipitate symptoms in IBS?
•Food
•Stress
•Menstrual cycle (females)

Why does food provoke symptoms in IBS?
•Dietary components– Tryptophan
•Depletion/augmentation can influence anxiety and GI symptoms in IBS
•Food allergy•Food intolerance
– Gluten– FODMAPs
•Interaction with the gut flora

Evidence for a role for the Microbiota in IBS
• Direct evidence of an altered gut flora:– Post-Infectious IBS (PI-IBS)– Small Intestinal Bacterial Overgrowth (SIBO)– Altered Colonic Flora
• Evidence of physiological effects of an altered flora:– Changes in stool volume/consistency
•Bile salt deconjugation– Alterations in gas volume/composition
•Fermentation– Food-microbiota interactions
• Mediator of pro-inflammatory state
• Therapeutic impact of altering flora

Evidence for a role for the Microbiota in IBS
• Direct evidence of an altered gut flora:– Post-Infectious IBS (PI-IBS)

Post-Infectious IBS
• 10-14% incidence following confirmed bacterial gastroenteritis
Dunlop, et al. 2003. Mearin, et al. 2005.
•Risk factors– Female– Severe illness– Pre-morbid psyche
• Depression– Persistent inflammation
• EC cells• T lymphocytes
Dunlop, et al. 2003.
300
200
100
0PI-IBS Patient
ControlsVolunteers
Lamina
Prop
ria
TLy
mph
ocyt
es P
er h
pf
**
75
50
25
0PI-IBS Patient
ControlsVolunteers
EC C
ells P
er h
pf
**
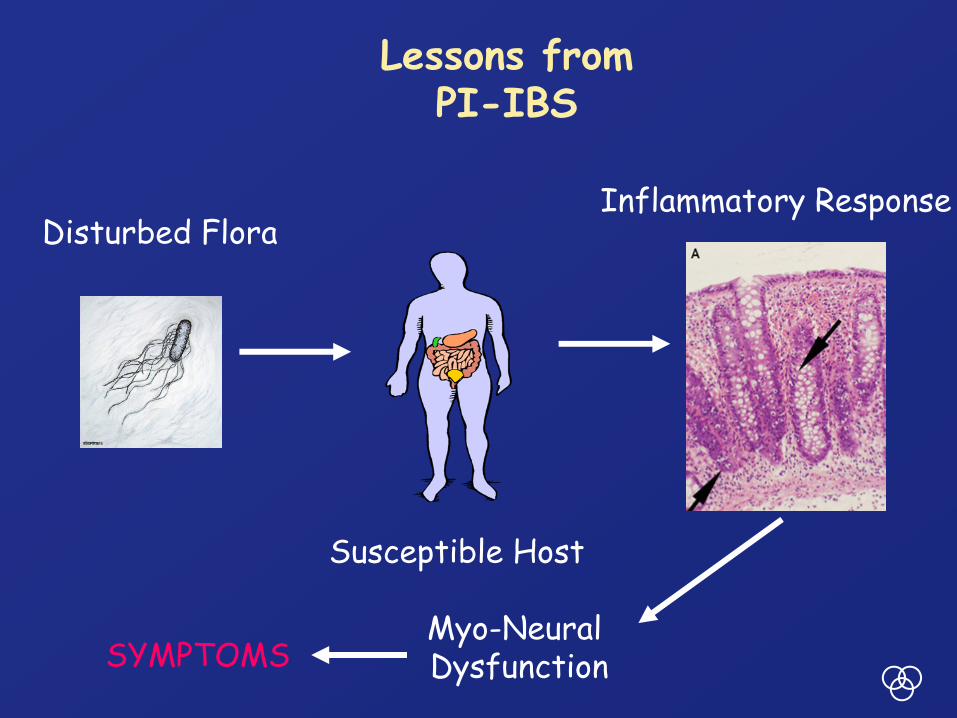
Lessons from PI-IBS
Disturbed Flora
Susceptible Host
Inflammatory Response
Myo-Neural DysfunctionSYMPTOMS

Evidence for a role for the Microbiota in IBS
• Direct evidence of an altered gut flora:– Altered Colonic Flora

% s
imila
rity
0
1 0
2 0
3 0
4 0
5 0
6 0
7 0
8 0
9 0
1 0 0
H e a l t h y
I B S
Variability in Flora
Codling et al, 2010

Large overlap in the two populations
IBS, in generalHigh-throughput Sequencing of the Microbiota
Jeffery et al, Gut 2011

Correlation-based clustering of subjects by microbiota composition
Two IBS specific clusters Jeffery et al, Gut 2011

Revised Groupings
The two IBS specific clusters are similar
Jeffery et al, Gut 2011

Clinical Associations
Jeffery et al, Gut 2011

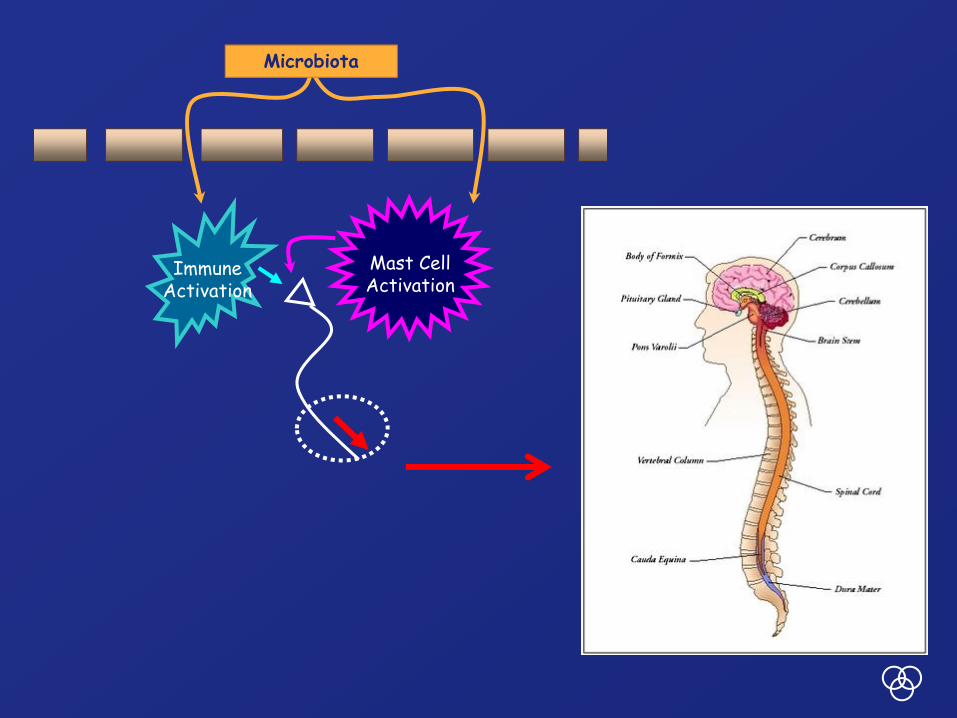
ImmuneActivation
Mast CellActivation
Luminal FactorsMicrobiota
A New Paradigm
Gut Barrier
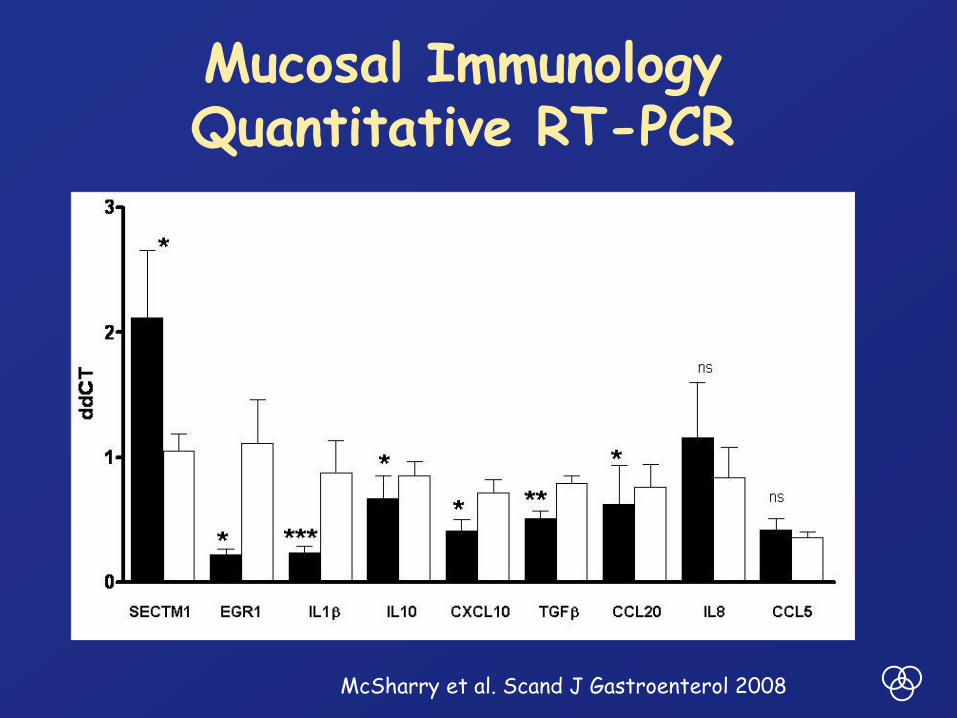
Mucosal Immunology Quantitative RT-PCR
IBSControls
McSharry et al. Scand J Gastroenterol 2008
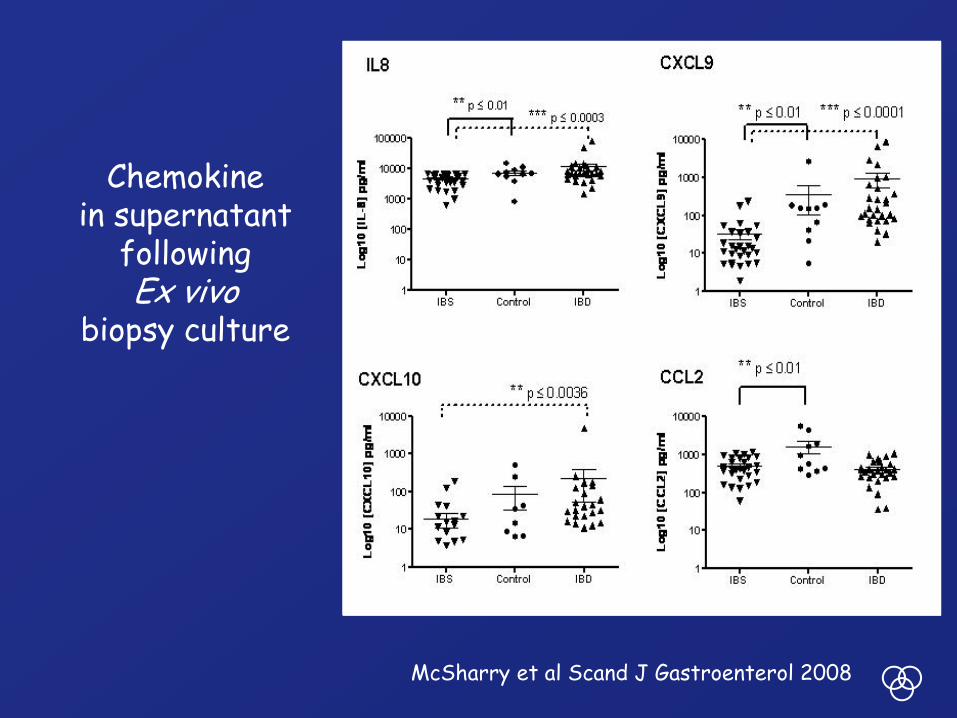
Chemokinein supernatant
followingEx vivo
biopsy culture
McSharry et al Scand J Gastroenterol 2008

McSharry et al. Scand J Gastroenterol 2008

Healthy IBS
CD3
CD4
CD8
T-Cell Subsets in the colonic mucosa

IP-10 (CXCL10)
IFNγ
Moloney et al, DDW 2012

Mucosal Compartment
• Increased mast cellsGuilarte et al, 2007
• More degranulating mast cells
Barbara et el, 2004
• Increased proteasesCenac 2007, Barbara 2008

A
Involved in crosstalk between mast cells and regulatory T cells.Induces release of histamine, proteases and IL-6 from mast cells
Effects on permeabilityInduces the expression of regulatory cytokines, such as IL-10
Beltran et al, DDW 2012

Early Life Events, Childhood Trauma, Visceral Hypersensitivity and IBS
Craig et al, DDW 2011

Early-Life Dysbiosis -Adult Visceral Hypersensitivity
O’Mahony et al DDW 2009

4 weeks 8 weeks
Microbiota at 4 and 8 weeks
4 weeks 8 weeks

Vehicl
e
10mg/kg
30mg/kg
100m
g/kg
0
20
40
60
*
***
Pres
sure
of d
iste
nsio
n (m
mH
g)
Vehicl
e
10mg/kg
30mg/kg
100m
g/kg
0
5
10
15
***
No
of p
ain
beha
viou
rs
Response to Colo-Rectal Distension at 9-12 weeks
Disruption of the Microbiota in early life leadsto a permanent change in enteric neurophysiology

Gut-Brain AxisCentral
Processing &Perception
Abnormal reflexesDisturbed perceptionAutonomic dysfunctionAberrant activation
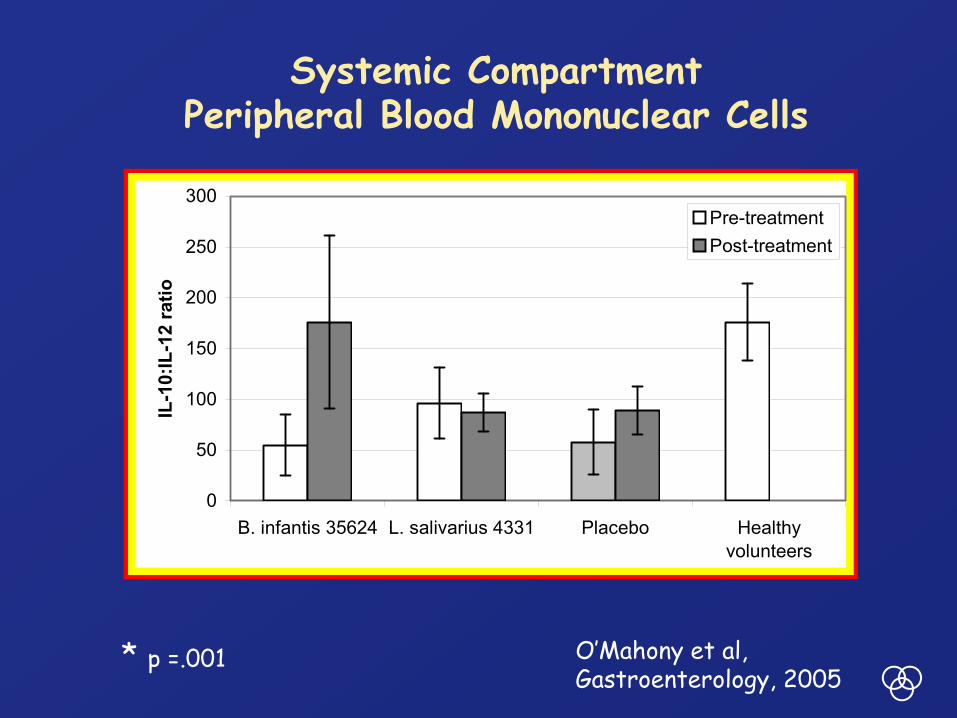
0
50
100
150
200
250
300
B. infantis 35624 L. salivarius 4331 Placebo Healthyvolunteers
IL-1
0:IL
-12
ratio
Pre-treatmentPost-treatment
* p =.001
*
O’Mahony et al, Gastroenterology, 2005
Systemic CompartmentPeripheral Blood Mononuclear Cells

Systemic Immune Compartment in IBSSerum Cytokines
Dinan, et al. Gastroenterology. 2006.
* IL-6
IBS Controls
6
5
4
3
2
1
0
IL-6
(pg/
ml)
* sIL-6r
IBS Controls0
50000
100000
150000
sIL-
6r

IL-1β
Control IBS0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5 p = 0.3433
IL-1
β (p
g/m
l)
IL-6
Control IBS0
1
2
3
4
5
6
7p = 0.0068
**
IL-6
(pg/
ml)
IL-8
Control IBS0
5
10
15
20p = 0.0036
**
IL-8
(pg/
ml)
IL-10
Control IBS0
25
50
75
100 p = 0.0971
IL-1
0 (p
g/m
l)
“Pure”IBS
Scully et al, Am J Gastroenterol 2010

IL-12
Control IBS0
102030405060708090
100110
p = 0.2406
IL-1
2 (p
g/m
l)
IL-13
Control IBS0
25
50
75
100
125p = 0.1903
IL-1
3 (p
g/m
l)
TNFα
Control IBS0123456789
10111213 p = 0.56
TNF α
IFNγ
Control IBS0.02.55.07.5
10.012.515.017.520.022.5 p = 0.4692
IFN
γ (p
g/m
l)
“Pure”IBS
Scully et al, Am J Gastroenterol 2010

Extra-Intestinal Features of IBS(CFS, Fibromyalgia, PMS)
Scully et al, Am J Gastroenterol 2010

Extra-Intestinal Features of IBS(CFS, Fibromyalgia, PMS)
Scully et al, Am J Gastroenterol 2010

Microbiota(Dysbiosis)
Mucosa(Immune Dysfunction)
DysmotilityVisceral Hypersensitivity
Gut-Brain Axis Dysfunction
Immune Activation
Beyond the Gut?
IL6, IL8
IL1β, TNFα

Does this mean anything?

0.2
ratio
10 mins
HealthyPlasma (1:250)
IBSPlasma (1:250)
A
B
C
Healthy plasma
IBSplasma
-0.050
-0.025
0.000
0.025
0.050
0.075
0.100
0.125 ***
∆R
atio
IBS-AIBS-C IBS-D
0.4
ratio
10 minHlthy IBS-A IBS-C IBS-D
0.000
0.025
0.050
0.075
*
*
∆R
atio
p=0.06
Does this mean anything?
O’Malley et al, DDW 2011

ACTH Response to CRH
-15 0 15 30 45 60 90 1200
10
20
30Healthy subjectsIBS
** **
Time (min)
AC
TH(n
g/l)
Significant correlation between the ACTH response (ΔACTH)
and IL-6 levels (r= 0.61, df=40, p<0.05).Dinan et al, Gastroenterology 2006

Is IBS a form of IBD?

Controls IBS0
25
50
75100
125
150
175
200
Cal
prot
ectin
(mg/
kg s
tool
)
Keohane et al, Am J Gastroenterol 2010

CD + IBS (n=37) CD – IBS (n=25) p value
Age (years) 42 (21-65) 38.3 (20- 67) 0.30
Females/males 22/15 10/14 0.25
Duration of disease (range) 11.2 yrs (2-30) 11 yrs (1-30) 0.97
Surgery 67% 56% 0.15
Smokers 27% 8% 0.0008
Medications
5-ASA 62.2% 52% 0.2
Sulfasalazine 0% 4% 0.13
Steroids 0 0 ns
AZA/6MP 32% 37.8% 0.55
No meds 13.5% 20% 0.35
CDAI (mean +/- SD) 53.4 +/- 31.3 35.6 +/- 35.6 * 0.04
How about IBS symptoms in IBD?
Keohane et al, Am J Gastroenterol 2010

CD + IBS (n=37) CD – IBS (n=25) p value
Age (years) 42 (21-65) 38.3 (20- 67) 0.30
Females/males 22/15 10/14 0.25
Duration of disease (range) 11.2 yrs (2-30) 11 yrs (1-30) 0.97
Surgery 67% 56% 0.15
Smokers 27% 8% 0.0008
Medications
5-ASA 62.2% 52% 0.2
Sulfasalazine 0% 4% 0.13
Steroids 0 0 ns
AZA/6MP 32% 37.8% 0.55
No meds 13.5% 20% 0.35
CDAI (mean +/- SD) 53.4 +/- 31.3 35.6 +/- 35.6 * 0.04
How about IBS symptoms in IBD?
Keohane et al, Am J Gastroenterol 2010

p=0.01
CD+IBS CD-IBS Controls0
100
200
300
400
500
Cal
prot
ectin
(mg/
kg s
tool
, mea
n +
SE)
Crohn’s Disease
Keohane et al, Am J Gastroenterol 2010

UC + IBS UC - IBS Controls0
100
200
300
400
500
600
700
800
Cal
prot
ectin
(mg/
kg s
tool
, mea
n +
SE)
Ulcerative Colitis
Keohane et al, Am J Gastroenterol 2010
ImmuneActivation
Mast CellActivation
Microbiota

What is the Evidence for a Microbiome-Gut-Brain Axis?

A Probiotic can Reduce Stress Response
Bravo et al,PNAS 2011
Associated with altered levels of GABA in the brainEffects abolished by vagotomy

What is the Evidence for a role for the Microbiome-Gut-Brain
Axis in IBS?

Can we link the microbiota and inflammation in IBS?
• Anti-Flagellin antibodies (but not ANCA or ASCA)
• Increased levels of β-defensin
• Toll-like receptor (TLR) activation

TLR’s in IBS
0
1
2
3
TLR3
ddct
HC IBS
TLR7
HC IBS
ddct
P<0.0001
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0
1
2
3
4
5
6
TLR8dd
ct
HC IBS
P=0.0019
0123456789 TLR4
ddct
HC IBS
P<0.0001

ImmuneActivation
Mast CellActivation
Microbiota
The Microbiota-Gut-Brain Axis
GutBarrier
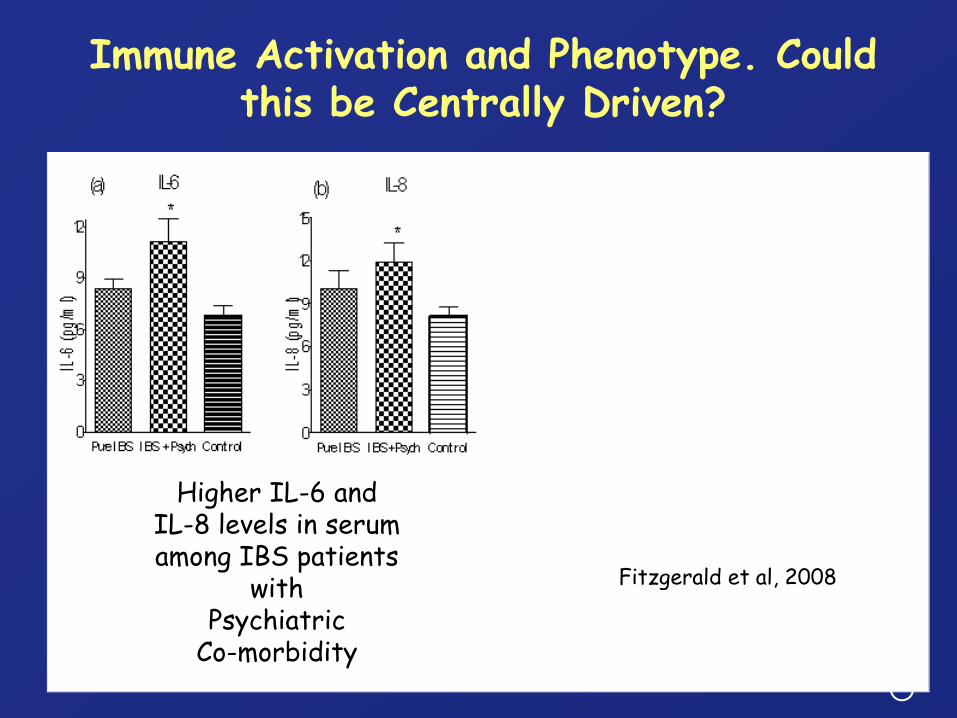
Higher IL-6 and IL-8 levels in serumamong IBS patients
with Psychiatric
Co-morbidity
Fitzgerald et al, 2008
Immune Activation and Phenotype. Could this be Centrally Driven?

Craig et al, DDW 2012
Co-morbid Depression/Anxiety and IL-6 in IBS

Classical Approach to Constipation
Constipation
Colon TransitEvacuation
Delayed TransitNormal Evacuation
SLOW TRANSIT CONSTIPATION Normal TransitImpaired Evacuation
DEFECATORY DYSFUNCTIONDelayed Transit
Normal EvacuationIBS

Diagnostic tools for chronic constipation
Medical history
• Nature of symptoms- Duration of
constipation- Description of stool
movements• Frequency• Formation
• Current medications, including:- OTC laxatives- Prescription
agents• Health conditions
Rectal examination
• Perianal excoriation• Skin tags, hemorrhoids• Anocutaneous reflex• Anal fissure• Prolapse• Rectocele• Sphincter resting tone
Diagnostic testing
• Colonic transit• Balloon expulsion• Anorectal manometry• Dynamic pelvic
magnetic resonance imaging
• Defecography
Eoff JC, Lembo AJ. J Manag Care Pharm 2008;14:1–15
OTC: Over-the-counter

New Approaches
• Pro-secretory agents
• Prokinetics/Enterokinetics

Linaclotide
Binds to GC-C receptors on enterocytes
Elevation of CGMP levels: increase in anion efflux fluid secretion
Linaclotide:Increases intestinal secretionAccelerates intestinal transit Ameliorates visceral
hypersensitivity
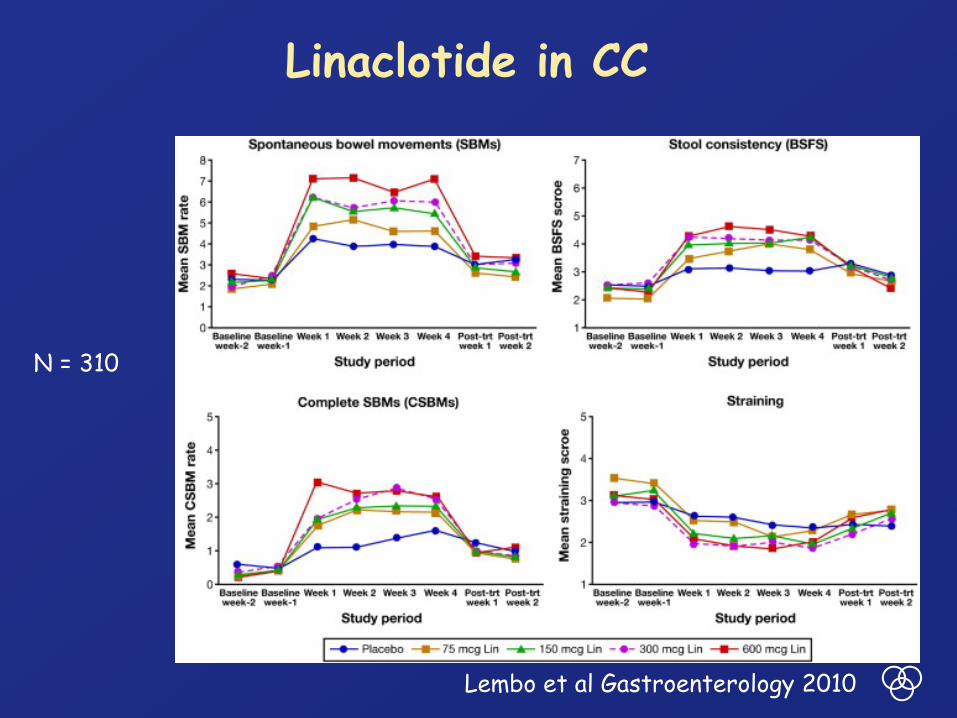
Linaclotide in CC
Lembo et al Gastroenterology 2010
N = 310

Prucalopride
Quigley et al, APT 2009

Quigley et al, APT 2009

Quigley et al, APT 2009

Other approaches
Antibiotics*Rifaximin and methanogenic flora
Probiotics**Bifidobacterium lactis
Ileal Bile Acid Transporter Inhibitor A3309***Biofeedback and other behavioral approaches for “outlet” constipationSpinal stimulationSurgery
*Chmielewska and Szajewska, WJ Gastroenterol2010
**Quigley, Best Pract Clin Res Gastroenterol 2011***Simren et al, APT 2011

A3309 Phase IIB Study• A minimally absorbed
ileal bile acid transporter (IBAT) inhibitor
• 190 patients with CC (IBS and dysynergic defecation excluded)
• Primary outcome: change from baseline in number of spontaneous bowel movements per week
• Also saw improvements in stool consistency, CSBMs and bloating
Treatment Change from baseline in
weekly SBMsPlacebo 1.7
A3309 5 mg 2.5A3309 10 mg 4A3309 15 mg 5.4
• Lowered total and LDL Cholesterol
• Increased bile acid synthesis• Troublesome cramps and
diarrhea with 15 mg dose
Chey et al, Am J Gastroenterol 2011;106:1803-12

Sacral Nerve Stimulation



Summary
• Colonic motility remains poorly understood
• Diverticular disease represents a growing but relatively ignored public health issue
• IBS, a variable amalgam of common gastrointestinal symptoms, is an important global issue
• Alterations in the microbiota or in microbiota-host interactions could explain some symptoms in IBS or lead to immune activation which could, in turn, influence local and central pathways
• New therapeutic avenues are opening in IBS and chronic constipation

Supported by: Science Foundation Ireland, HRB, EU, Wellcome Trust, Enterprise Ireland, Higher Education Authority
Students, Trainees, Post-Docs, Scientists:• Clare O’Leary • Rodrigo Quera• John Keohane• Ahmed Abu-Shanab• Morcos Ashraf• Alan Desmond • Sebastian McWilliams• Katie Walsh• OJ O’Connor • Orla Craig • Zaid Heetun• Marianne Fraher • Paul Scully• Ian Jeffery• John McSharry• Caroll Beltran• Ger Clarke• Ger Moloney• Clare Codling• Declan McKernan• Peter Fitzgerald
Co-PI’s in APC:Gerald FitzgeraldMichael MaherPaul O’TooleJulian MarchesiKen NallySylvia MelgarLiam O’MahonyBeth BrintPaul RossCatherine StantonJohn CryanTed DinanNiall HylandSiobhain O’MahonyMichael MolloyDouwe van SinderenCharles Daly
Alimentary Health:Barry KielyEileen MurphyJenny RoperEileen MurphyCarmel Wycherly
COLONISTGeraldine GreelyAnne O’Neill
CUH/MUHPaula O’LearySeamus O’MahonyOrla CrosbieAli KhashanLouise KennyMartin BuckleyJane McCarthy
Director of APC and Chair, Dept of MedicineFergus Shanahan

![WallFlex Colonic Stent - Boston Scientific- US · WallFlex ™ Colonic Stent Visualization Expertise in combining stent materials has resulted ... (BTS). “The WallFlex™ [Colonic]](https://img.dokumen.tips/doc/110x75/5ae601bc7f8b9a8b2b8ca931/wallflex-colonic-stent-boston-scientific-us-colonic-stent-visualization-expertise.jpg)