Embed Size (px)
Citation preview
Génériques et fausse innovation
exemples de l’evergreening et du spillover
COLLOQUE DE PHARMACOLOGIE
CLINIQUE GENEVE – VAUD
Nyon, jeudi 5 décembre 2013
Dr Nathalie Vernaz, MBA, PhD
Pharmacienne adjointe,
Responsable secteur Achat/Distribution1
2

Génèse du médicament
Interpharma, Le marché du médicament en Suisse.
2008
DiMasi estime le coût de la recherche à
- $802 million in 2000 par molécule, and
- $1,318 million in 2005 biologiques
DiMasi, J. A., Hansen, R. W. & Grabowski, H. G. The price of innovation: new estimates of
drug development costs. J. Health Econ. 22, 151–185 (2003).
DiMasi, J. A., Grabowski, H. G. The cost of biopharmaceutical R&D. Manage. Decis. Econ.
28, 469–479 (2007).
Pour encourager l’innovation et comme tous
les autres produits, les médicaments
sont protégés par des brevets dont la durée a
été harmonisée à 20 ans.
Brevets: critères d’éligibilité
• “non obvious”
– brevet sur la molécule et ses différentes structures chimiques, ses métabolites actifs
– le mode de synthèse,
– la forme galénique (ex: retard),
– les méthodes de traitement,
– les indications,
– le procédé de fabrication,
– association de composés, etc.
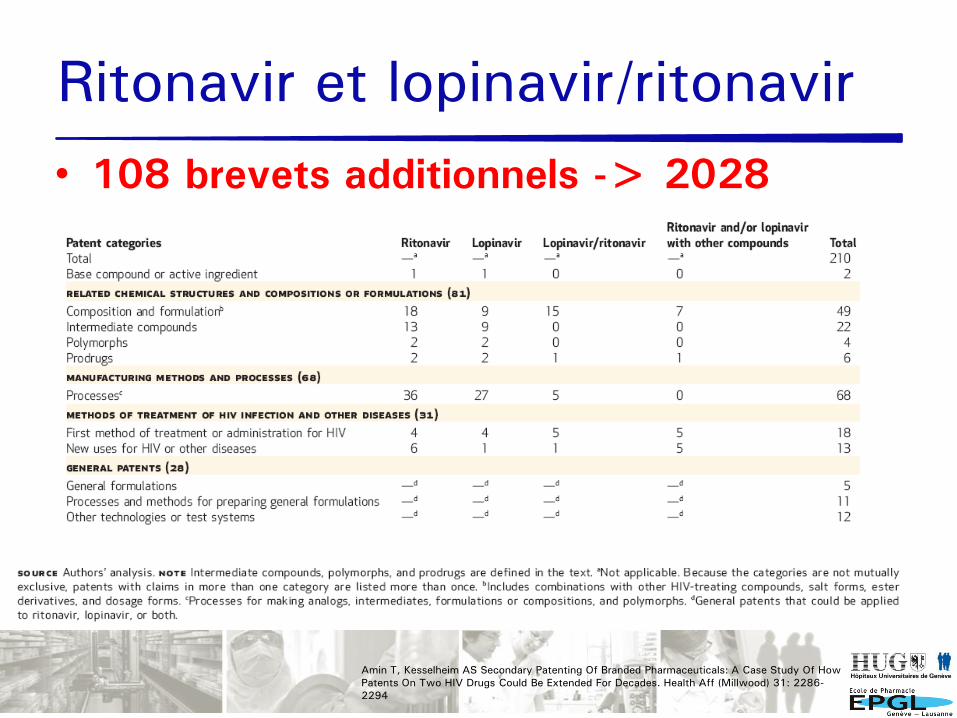
Ritonavir et lopinavir/ritonavir
• 108 brevets additionnels -> 2028
Amin T, Kesselheim AS Secondary Patenting Of Branded Pharmaceuticals: A Case Study Of How
Patents On Two HIV Drugs Could Be Extended For Decades. Health Aff (Millwood) 31: 2286-
2294

Vraie vie: eso-omeprazole
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%ja
nv.0
0
août.00
mars
.01
oct.01
mai.02
déc.0
2
juil.
03
févr.
04
sept.04
avr.
05
nov.0
5
juin
.06
janv.0
7
août.07
mars
.08
oct.08
original
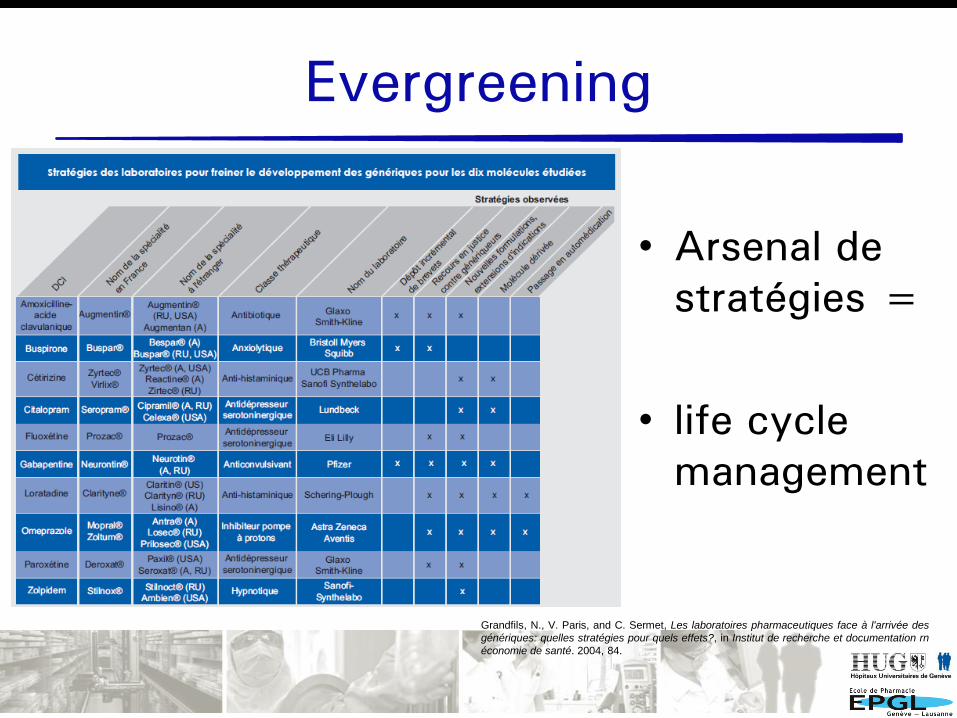
Evergreening
• Arsenal de
stratégies =
• life cycle
management
Grandfils, N., V. Paris, and C. Sermet, Les laboratoires pharmaceutiques face à l'arrivée des
génériques: quelles stratégies pour quels effets?, in Institut de recherche et documentation rn
économie de santé. 2004, 84.
Chiralité: un peu d’histoire
1
Somogyi A. BF, Foster D (2004) Inside the isomers: the tale of chiral switches. Australian
Prescriber 27: 47-49
Agranat I, Caner H, Caldwell J (2002) Putting chirality to work: the strategy of chiral
switches. Nat Rev Drug Discov 1: 753-768
Study of Praying Hands
Albrecht Dürer (1508)
Prix Nobel de chimie en 2001
« Travaux sur les réactions d'hydrogénation
catalysées par chiralité »
- William S. Knowles Saint-Louis, Missouri, USA
- Ryoji Noyori Nagoya University, Chikusa,
Nagoya, Japon,
Bénéfices cliniques attendus
• Amélioration de la sécurité– >Augmentation de l’affinité aux récepteurs
– >Diminution des effets secondaires
• Modification de la demi-vie– > dosage plus approprié
• Diminution de la variabilité interindividuelle
• Diminution de l’interraction entre médicaments
9Somogyi A. BF, Foster D (2004) Inside the isomers: the tale of
chiral switches. Australian Prescriber 27: 47-49
Bénéfices cliniques démontrés
10
Pas d’étude clinique “head to Head” ou alors
compare 40mg esomeprazole à 20 mg d’omeprazole Lind, T., et al. Aliment Pharmacol Ther, 2000. 14(7): p. 861-7.
Somogyi A. BF, Foster D (2004) Inside the isomers: the tale of chiral switches. Australian Prescriber
27: 47-49
“Need to be provided … that chiral switches have advantages for
the prescriber and the consumer”
Hughes DA, Ferner RE New drugs for old: disinvestment and NICE. Bmj 340: c572
“any resulting improvement in health outcome, is often lacking”
Svensson S, Mansfield PR (2004) Escitalopram: superior to citalopram or a chiral chimera?
Psychother Psychosom 73: 10-16.
“Methodological flaws in the trials… superiority for escitalopram
over citalopram are unwarranted”
Agranat I, Caner H, Caldwell J (2002) Putting chirality to work: the strategy of chiral switches. Nat
Rev Drug Discov 1: 753-768
“ The chiral switch is a usufull option for the owners of existing
racemate to achieve line extensions, especially if the switch can
be marketed immediately before expiry of patent on the racemate”
Evergreening strategies
11
• Breveter et mettre sur le marché des molécules légèrement modifiées
de médicaments déjà enregistrés -> à l’arrivée des génériques
- Associations de médicaments
Acide alendronique combiné au colecalciferol et alendronic acid,
simvastatin combinée à ezetimibe et simvastatin
- Analogues structurels
pregabalin et gabapentin
- Métabolites actifs
desloratadine et loratadine
- Formes retards
zolpidem retard et zolpidem
- Single enantiomer
omeprazole et esomeprazole
citalopram et escitalopram
cetirizine et levocetirizine
3 catégories de médicaments
12
• Original
• Son générique
• Son evergreening: médicament “original” sur
lequel une stratégie d’evergreening est
appliquée
• Médicaments commercialisés en même temps
• Pas au même prix
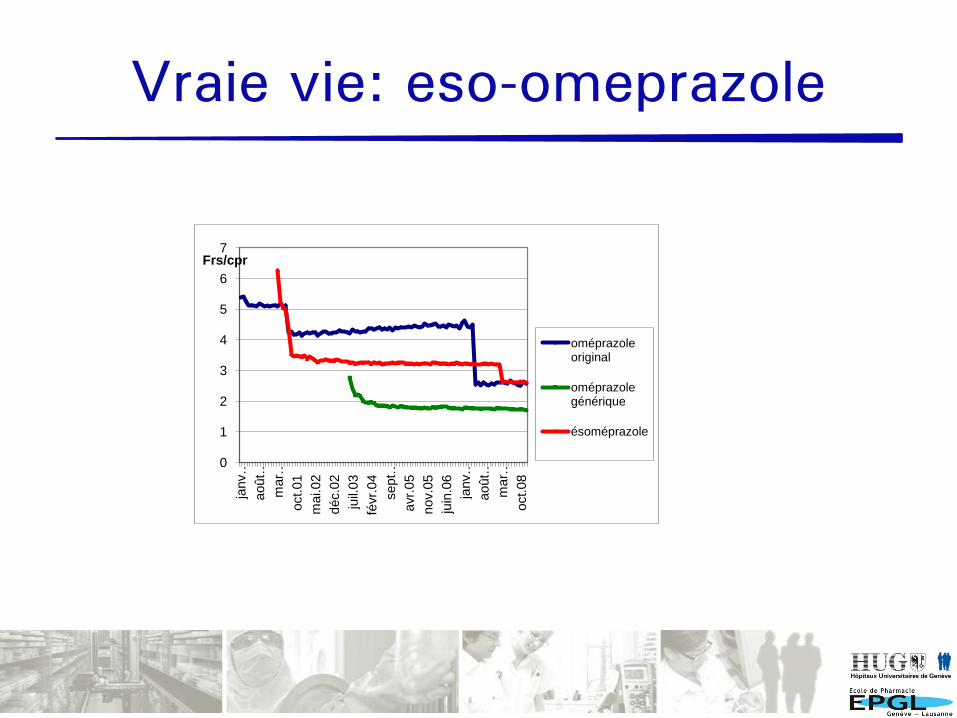
Vraie vie: eso-omeprazole
0
1
2
3
4
5
6
7ja
nv…
août…
mar…
oct.01
mai.02
déc.0
2
juil.
03
févr.
04
sept…
avr.
05
nov.0
5
juin
.06
janv…
août…
mar…
oct.08
Frs/cpr
oméprazole original
oméprazole générique
ésoméprazole
Etude: les données
14
• OFAC: intermédiaire entre les pharmacies de ville et les assurances
• Ordonnances GE (ville + HUG)
• Couvre 92% des officines
• 80% des assurés (pas Assura)
• HUG
• Janvier 2000 à décembre 2008
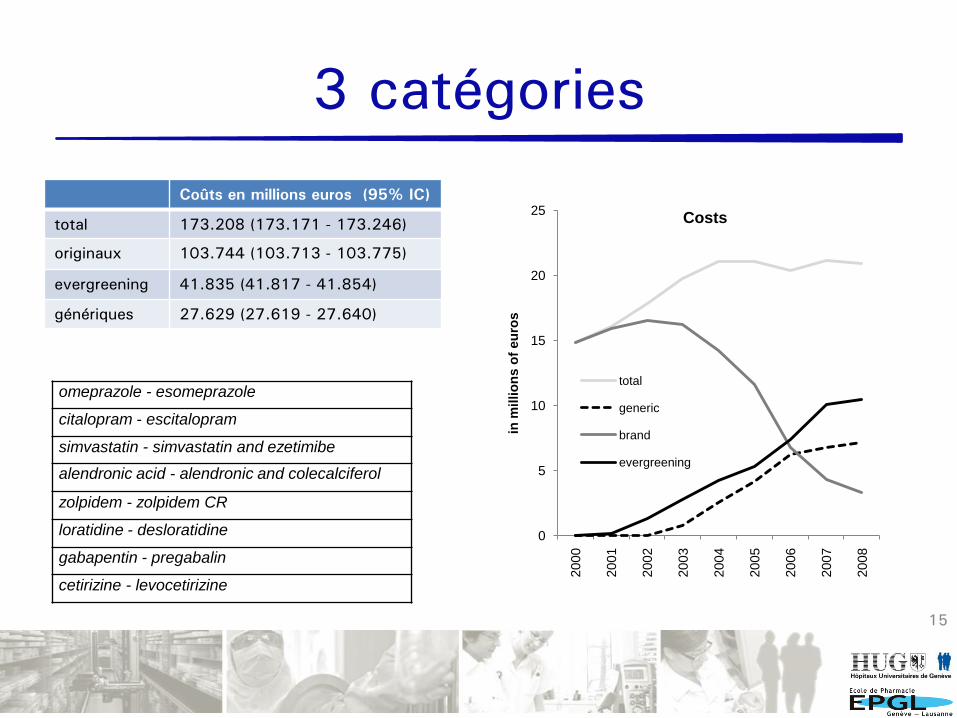
3 catégories
15
omeprazole - esomeprazole
citalopram - escitalopram
simvastatin - simvastatin and ezetimibe
alendronic acid - alendronic and colecalciferol
zolpidem - zolpidem CR
loratidine - desloratidine
gabapentin - pregabalin
cetirizine - levocetirizine
0
5
10
15
20
25
2000
2001
2002
2003
2004
2005
2006
2007
2008
in m
illio
ns o
f eu
ros
Costs
total
generic
brand
evergreening
Coûts en millions euros (95% IC)
total 173.208 (173.171 - 173.246)
originaux 103.744 (103.713 - 103.775)
evergreening 41.835 (41.817 - 41.854)
génériques 27.629 (27.619 - 27.640)
Hypothèse: « Squeezing the balloon »
16
le volume dans lequel les molécules de l'air libres de se déplacer est
réduit, elles mettent une grande énergie à traverser les frontières
la réduction financière attendue lors de l’arrivée des génériques ne serait pas aussi effective en réalité
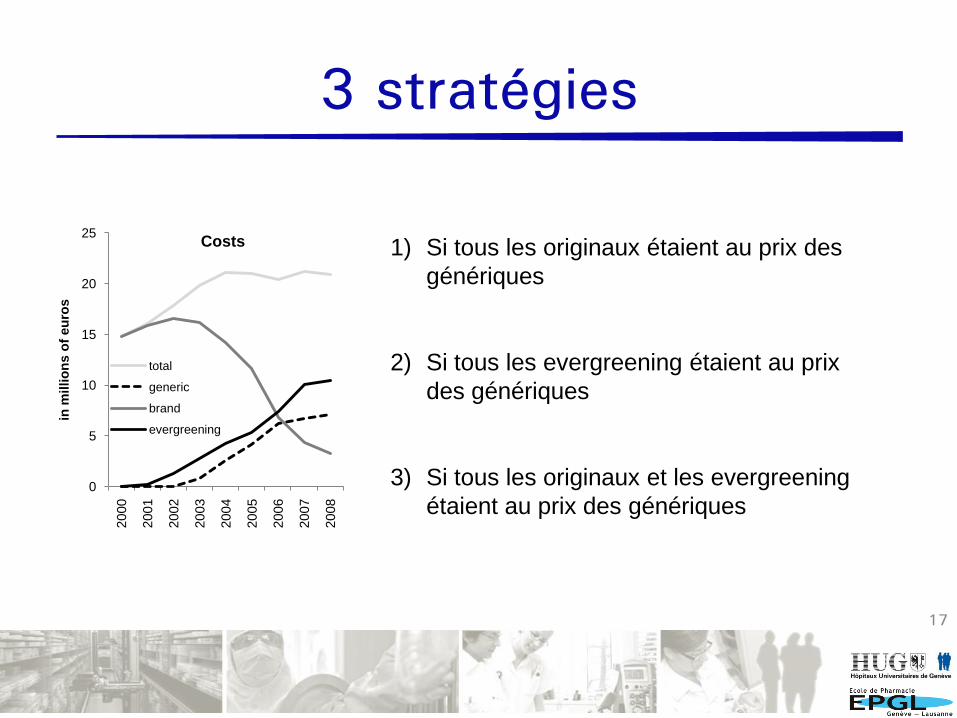
3 stratégies
17
0
5
10
15
20
25
2000
2001
2002
2003
2004
2005
2006
2007
2008
in m
illio
ns o
f eu
ros
Costs
total
generic
brand
evergreening
1) Si tous les originaux étaient au prix des
génériques
2) Si tous les evergreening étaient au prix
des génériques
3) Si tous les originaux et les evergreening
étaient au prix des génériques
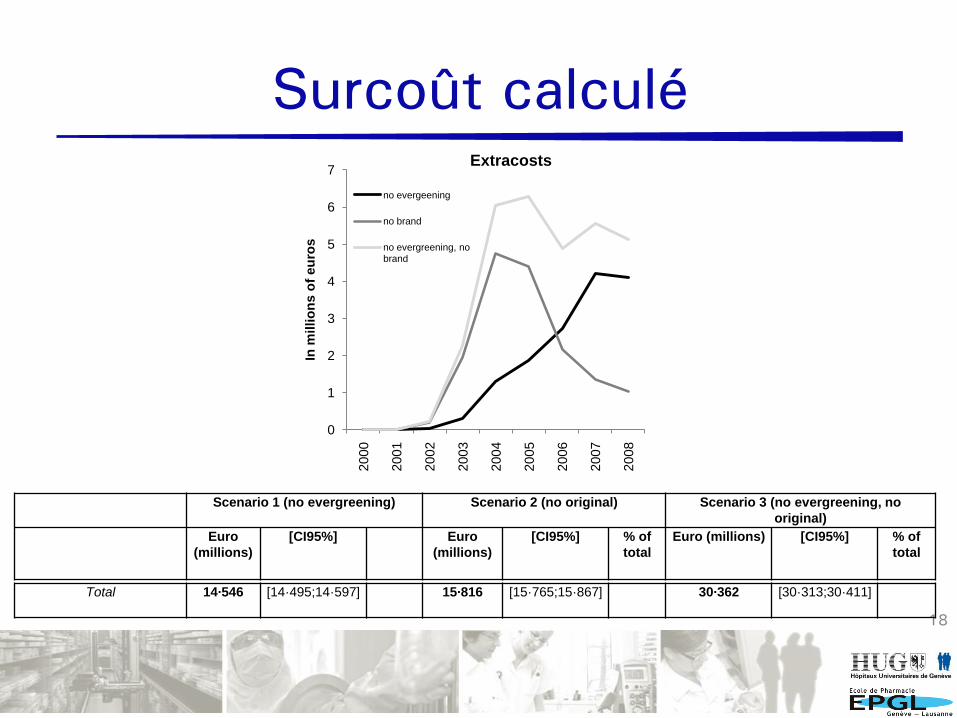
Surcoût calculé
18
0
1
2
3
4
5
6
7
2000
2001
2002
2003
2004
2005
2006
2007
2008
In m
illi
on
s o
f eu
ros
Extracosts
no evergeening
no brand
no evergreening, no brand
Scenario 1 (no evergreening) Scenario 2 (no original) Scenario 3 (no evergreening, no
original)
Euro
(millions)
[CI95%] Euro
(millions)
[CI95%] % of
total
Euro (millions) [CI95%] % of
total
Total 14·546 [14·495;14·597] 15·816 [15·765;15·867] 30·362 [30·313;30·411]

Surcoût calculé
19
Scenario 1 (no evergreening) Scenario 2 (no original) Scenario 3 (no evergreening, no
original)
Euro
(millions)
[CI95%] % of
total
Euro
(millions)
[CI95%] % of
total
Euro (millions) [CI95%] % of
total
omeprazole -
esomeprazole
5·262 [5·225;5·299] 36·2% 7294 [7·259;7·329] 46·1% 12·556 [12·521;12·591] 41·4%
citalopram - escitalopram 4·873 [4·851;4·895] 33·5% 4795 [4·773;4·817] 30·3% 9·668 [9·548;9·688] 31·8%
simvastatin - simvastatin
and ezetimibe
2·636 [2·620;2·652] 18·1% 2697 [2·679;2·715] 17·1% 5333 [5·317;5·349] 17·6%
alendronic acid -
alendronic and
colecalciferol
203 [189;217] 1·4% 199 [185;213] 1·3% 402 [388;416] 1·3%
zolpidem - zolpidem CR 64 [58;70] 0·4% 418 [412;424] 2·6% 482 [476;488] 1·6%
loratidine - desloratidine 371 [367;375] 2·6% 43 [37;49] 0·3% 414 [410;418] 1·4%
gabapentin - pregabalin 630 [612;648] 4·3% 132 [114;150] 0·8% 762 [744;780] 2·5%
cetirizine - levocetirizine 507 [501;513] 3·5% 238 [232;244] 1·5% 745 [739;751] 2·5%
Total 14·546 [14·495;14·597] 15·816 [15·765;15·867] 30·362 [30·313;30·411]
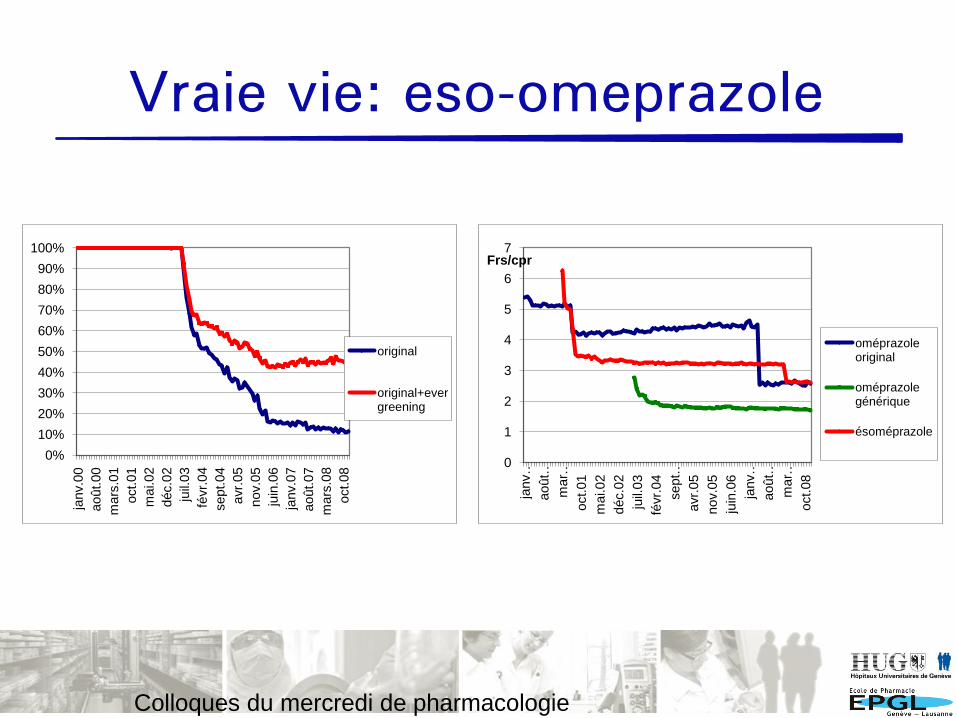
Vraie vie: eso-omeprazole
Colloques du mercredi de pharmacologie
clinique
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
janv.0
0
août.00
mars
.01
oct.01
mai.02
déc.0
2
juil.
03
févr.
04
sept.04
avr.
05
nov.0
5
juin
.06
janv.0
7
août.07
mars
.08
oct.08
original
original+evergreening
0
1
2
3
4
5
6
7
janv…
août…
mar…
oct.01
mai.02
déc.0
2
juil.
03
févr.
04
sept…
avr.
05
nov.0
5
juin
.06
janv…
août…
mar…
oct.08
Frs/cpr
oméprazole original
oméprazole générique
ésoméprazole
Spillover effect
21
Spill: renverser
over: dessus
Répercussion d’une décision-action prise dans un
environnement sur un autre environnement
Tribune de Genève, 4 mars 2011
Liste des médicaments
22
Objectif
• Hôpitaux
- minimiser coûts d’acquisition -> négociation
- limiter le nombre de médicaments
- enseignement
• Maisons pharmaceutiques:
- prescription et administration des médicaments
- Spillover effect
Hypothèse
Impact de la liste de médicaments sur les coûts en ville
Wang YR, Pauly MV (2005) Spillover effects of restrictive drug formularies: a case study of
PacifiCare in California. Am J Manag Care 11: 24–26.
≠
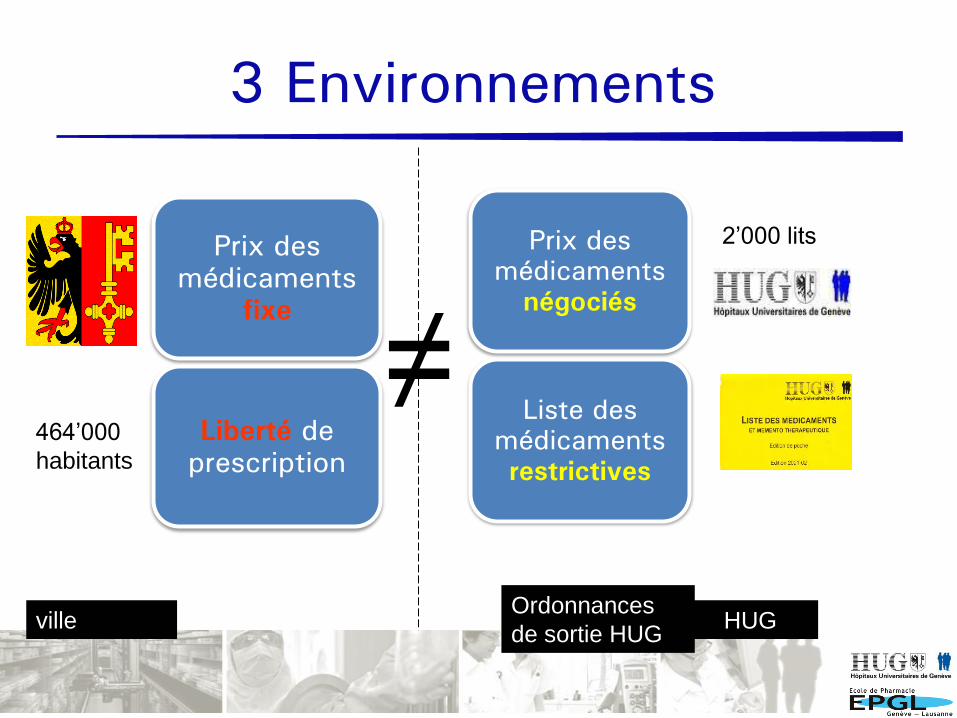
villeOrdonnances
de sortie HUG
3 Environnements
464’000
habitants
2’000 lits
HUG
Prix des
médicaments
négociés
Liste des
médicaments
restrictives
Prix des
médicaments
fixe
Liberté de
prescription
Indicateur de la prescription
24
% evergreening (DDD)
original+générique+evergreening
(DDD)
Même
échelle
Classe de
médicaments
Muijrers PE et al (2005) Fam Pract 22: 624-630
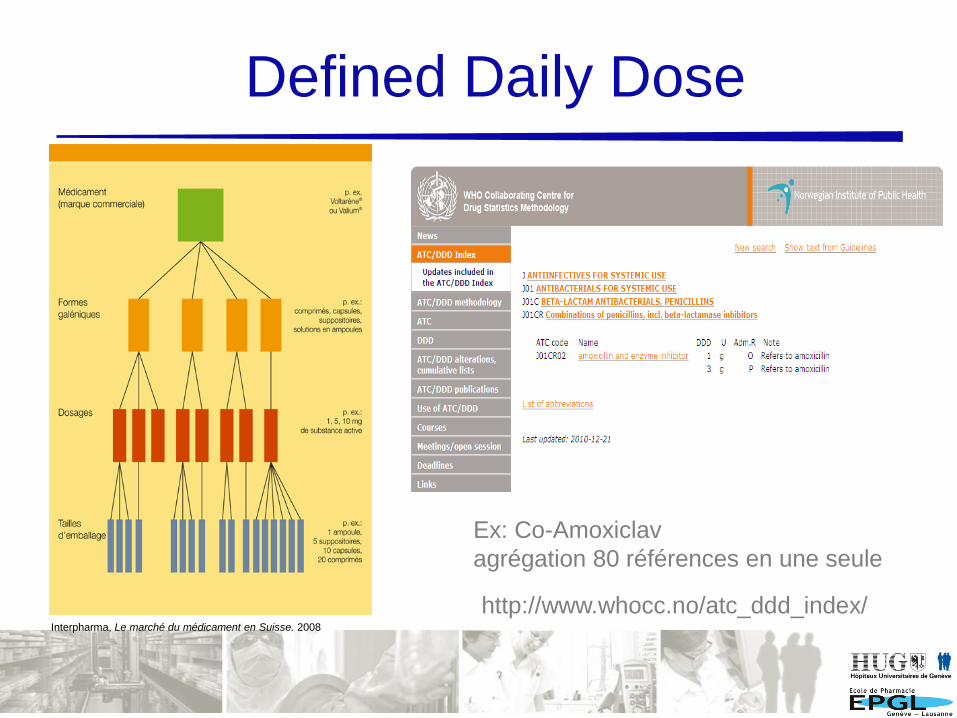
Defined Daily Dose
http://www.whocc.no/atc_ddd_index/
Ex: Co-Amoxiclav
agrégation 80 références en une seule
Interpharma, Le marché du médicament en Suisse. 2008
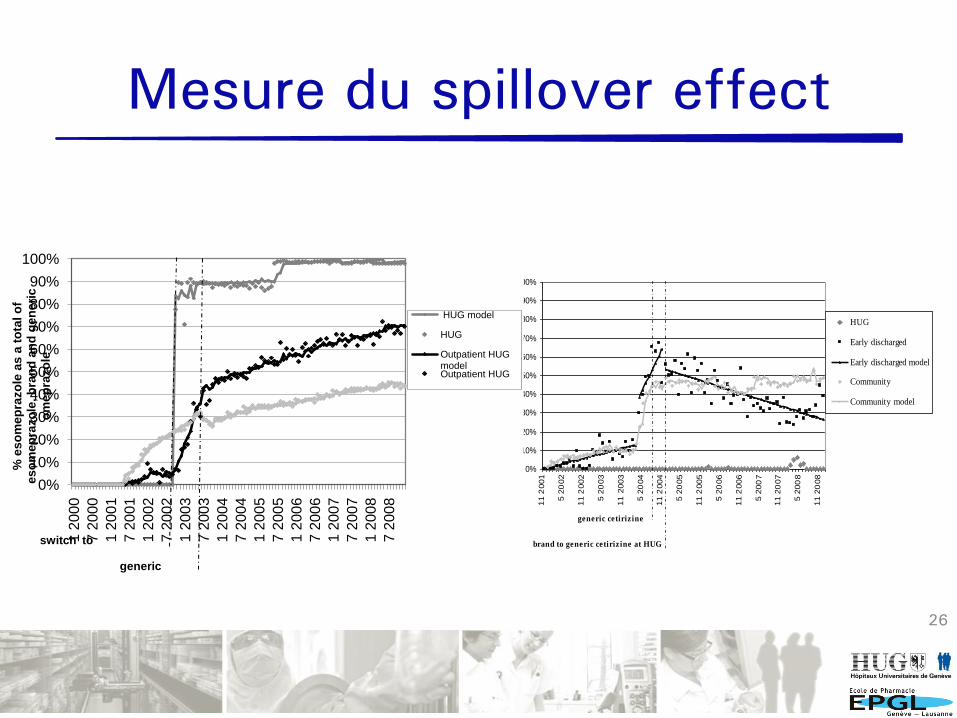
Mesure du spillover effect
26
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
11 2
001
5 2
002
11 2
002
5 2
003
1
1 2
003
5 2
004
11 2
004
5 2
005
11 2
005
5 2
006
11 2
006
5 2
00
7
11 2
007
5 2
00
8
11 2
008
% levo
ceti
rizin
e a
s a
to
tal o
f le
vo
ceti
rizin
e,
ceti
rizin
e b
ran
d a
nd
gen
eri
c a
nd
HUG
Early discharged
Early discharged model
Community
Community model
brand to generic cetiriz ine at HUG
generic cetiriz ine
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1 2
00
0
7 2
00
0
1 2
00
1
7 2
00
1
1 2
00
2
7 2
00
2
1 2
00
3
7 2
00
3
1 2
00
4
7 2
00
4
1 2
00
5
7 2
00
5
1 2
00
6
7 2
00
6
1 2
00
7
7 2
00
7
1 2
008
7 2
00
8
% e
so
me
pra
zo
le a
s a
to
tal o
f e
so
me
pra
zo
le, b
ran
d a
nd
ge
ne
ric
o
me
pra
zo
le
HUG model
HUG
Outpatient HUG modelOutpatient HUG
switch to
generic
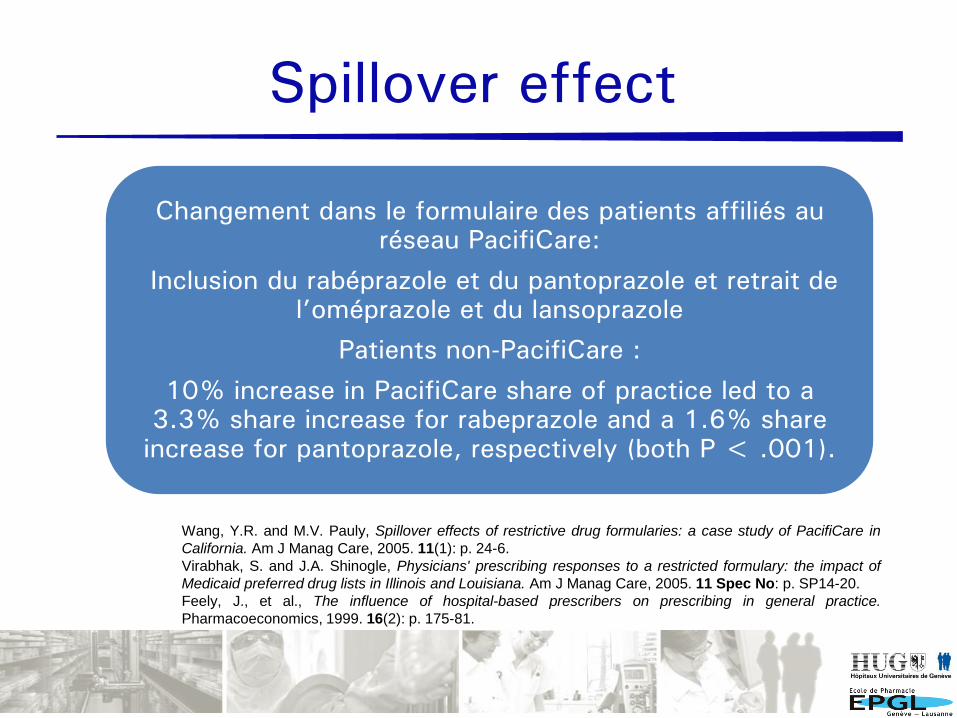
Spillover effect
Changement dans le formulaire des patients affiliés au
réseau PacifiCare:
Inclusion du rabéprazole et du pantoprazole et retrait de
l’oméprazole et du lansoprazole
Patients non-PacifiCare :
10% increase in PacifiCare share of practice led to a
3.3% share increase for rabeprazole and a 1.6% share
increase for pantoprazole, respectively (both P < .001).
Wang, Y.R. and M.V. Pauly, Spillover effects of restrictive drug formularies: a case study of PacifiCare in
California. Am J Manag Care, 2005. 11(1): p. 24-6.
Virabhak, S. and J.A. Shinogle, Physicians' prescribing responses to a restricted formulary: the impact of
Medicaid preferred drug lists in Illinois and Louisiana. Am J Manag Care, 2005. 11 Spec No: p. SP14-20.
Feely, J., et al., The influence of hospital-based prescribers on prescribing in general practice.
Pharmacoeconomics, 1999. 16(2): p. 175-81.
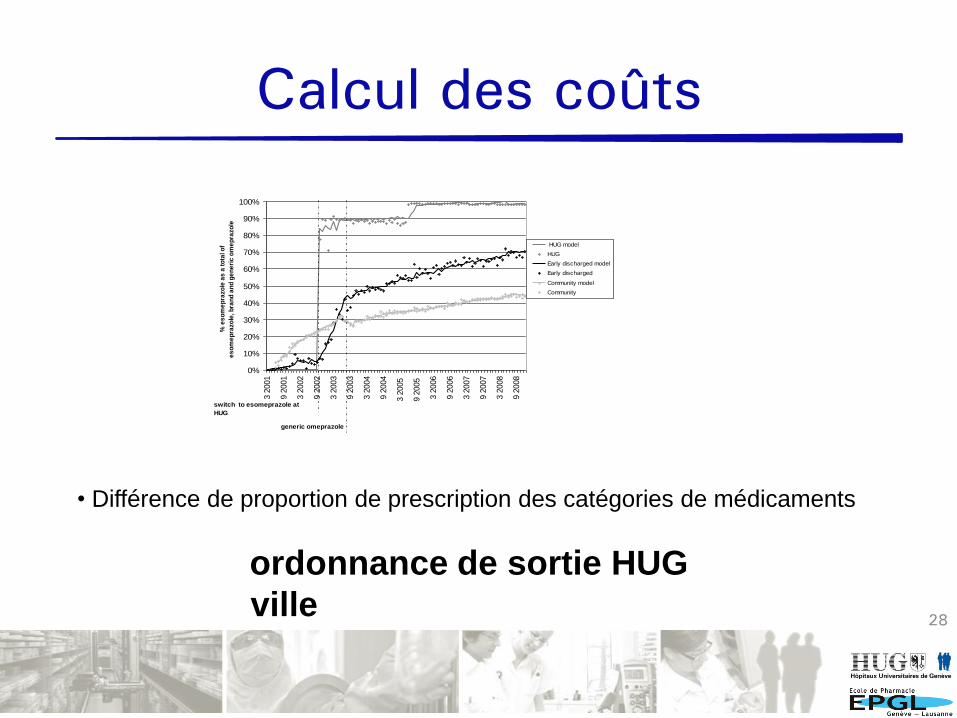
Calcul des coûts
28
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
3 2
001
9 2
001
3 2
002
9 2
002
3 2
003
9 2
003
3 2
004
9 2
004
3 2
005
9 2
005
3 2
006
9 2
006
3 2
007
9 2
007
3 2
008
9 2
008
% e
so
me
pra
zo
le a
s a
to
tal o
f
es
om
ep
razo
le, b
ran
d a
nd
ge
ne
ric
om
ep
razo
le
HUG model
HUG
Early discharged model
Early discharged
Community model
Community
switch to esomeprazole at
HUG
generic omeprazole
• Différence de proportion de prescription des catégories de médicaments
ordonnance de sortie HUG
ville
29
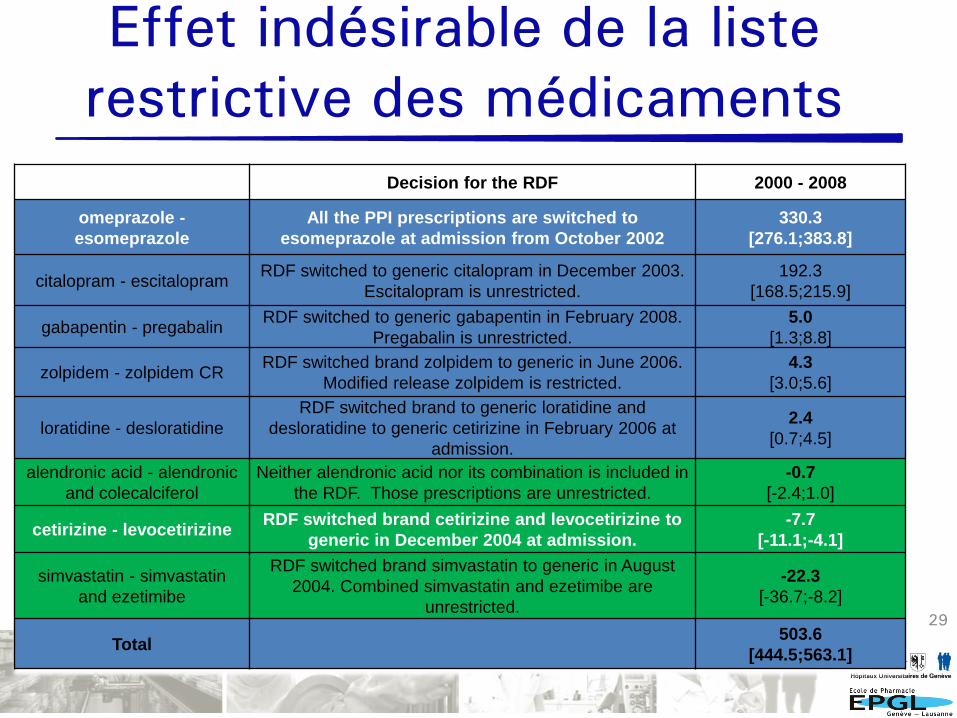
Decision for the RDF 2000 - 2008
omeprazole -
esomeprazole
All the PPI prescriptions are switched to
esomeprazole at admission from October 2002
330.3
[276.1;383.8]
citalopram - escitalopramRDF switched to generic citalopram in December 2003.
Escitalopram is unrestricted.
192.3
[168.5;215.9]
gabapentin - pregabalinRDF switched to generic gabapentin in February 2008.
Pregabalin is unrestricted.
5.0
[1.3;8.8]
zolpidem - zolpidem CRRDF switched brand zolpidem to generic in June 2006.
Modified release zolpidem is restricted.
4.3
[3.0;5.6]
loratidine - desloratidine
RDF switched brand to generic loratidine and
desloratidine to generic cetirizine in February 2006 at
admission.
2.4
[0.7;4.5]
alendronic acid - alendronic
and colecalciferol
Neither alendronic acid nor its combination is included in
the RDF. Those prescriptions are unrestricted.
-0.7
[-2.4;1.0]
cetirizine - levocetirizineRDF switched brand cetirizine and levocetirizine to
generic in December 2004 at admission.
-7.7
[-11.1;-4.1]
simvastatin - simvastatin
and ezetimibe
RDF switched brand simvastatin to generic in August
2004. Combined simvastatin and ezetimibe are
unrestricted.
-22.3
[-36.7;-8.2]
Total503.6
[444.5;563.1]
Effet indésirable de la liste
restrictive des médicaments
30
Forces et limites
Forces
• Source de l’information unique
• Longue période 9 ans
• 73% patients assurés
• Situation particulière du canton de Genève
avec un seul hôpital universitaire
Limites
• pas de différence clinique entre les 3
catégories de médicaments: même outcome
• adhérence des patients
• pas de mesure du marketing en ville
Greene JA, Kesselheim AS (2011) Why do the same drugs look different? Pills, trade dress, and
public health. N Engl J Med 365: 83–89
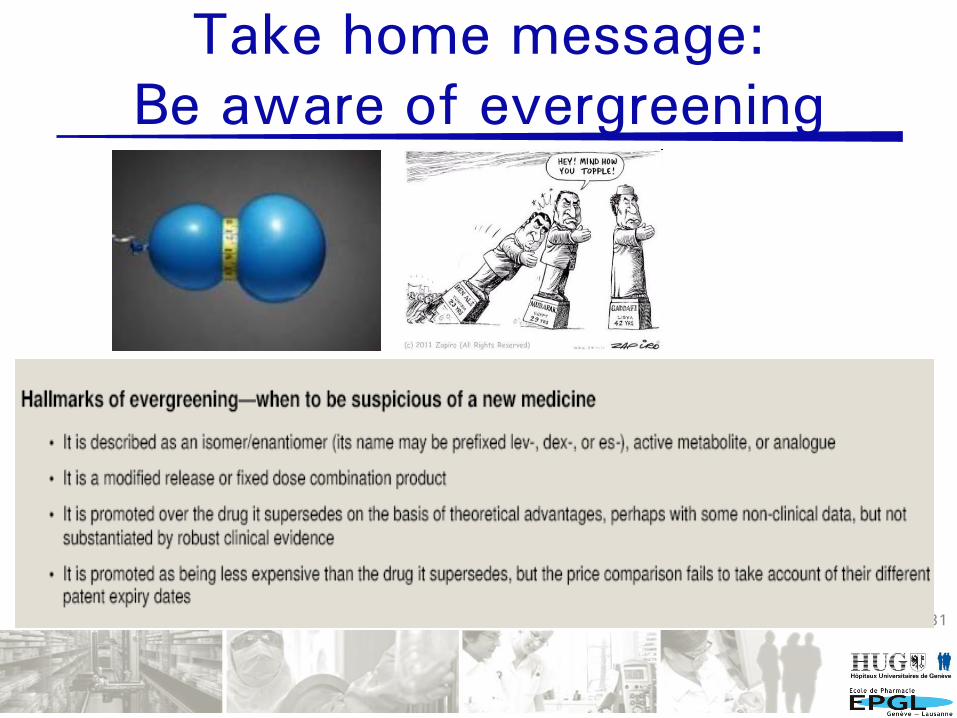
Take home message:
Be aware of evergreening
31Hitchings and all BMJ 2012; 345
Σ ε ® С ][





























