Embed Size (px)
Citation preview

第二代TKI藥物用於 慢性骨髓性白血病第一線治療
亞東紀念醫院
腫瘤暨血液科
謝佩穎 醫師

認識白血病
• 白血病即是血癌
• 一種血液細胞 (紅血球、白血球、血小板)的癌症
• 依臨床及病理特徵可分為:急性、慢性
• 依細胞型態可分:淋巴性、骨髓性

慢性骨髓性白血病(CML)
• 白血病的其中一種分類
• 發生原因:血液細胞內的染色體,第9對和第22對染色體發生轉位,產生新的異常染色體。即『費城染色體』。

慢性骨髓性白血病(CML)的症狀
• 20-40% 毫無症狀 • 非特異性症狀:
– 容易倦怠 – 體重減輕 – 食慾不振、發燒
• 脾臟腫大: 腹脹、腹痛 • 抽血異常:
– 白血球過多 – 血小板過多 – 不成熟的白血球 – 可能有貧血的現象

慢性骨髓性白血病(CML)的診斷
• 抽骨髓
– 血液抹片
– 染色體分析:費城染色體 t(9;22)

慢性骨髓性白血病(CML)的 分期及治療方針
• 慢性期: 口服標靶藥物(TKI)治療為主
• 加速期: 口服標靶藥物,考慮作血液幹細胞移植
• 急性期: 化學治療合併口服標靶藥物 血液幹細胞移植

治療反應
• 完全血液緩解:血球數目和正常人無異
• 染色體緩解:費城染色體的減少或消失
– 完全染色體緩解:0%
– 主要染色體緩解:0-35%
– 沒有染色體緩解:95%以上
• 基因緩解:利用抽血分子檢驗的方法,測量異常細胞減少的程度(微量疾病)


臨床上明顯的疾病
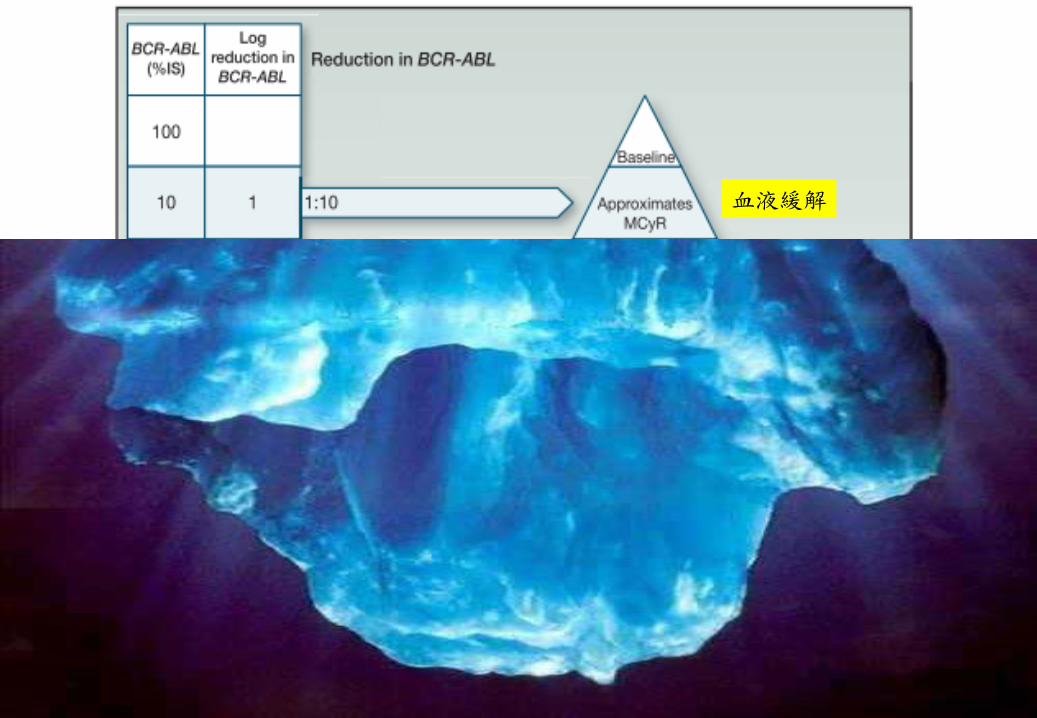
血液緩解

血液緩解
染色體的緩解

血液緩解
染色體的緩解
主要基因緩解
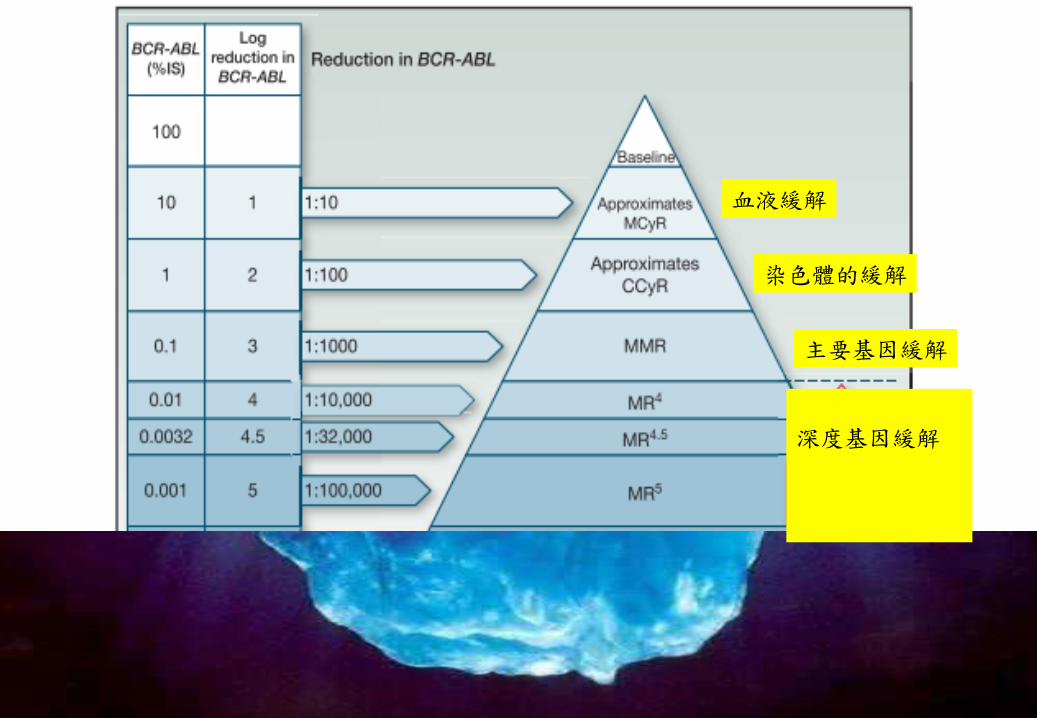
血液緩解
染色體的緩解
主要基因緩解
深度基因緩解

血液緩解
染色體的緩解
主要基因緩解
深度基因緩解
-
-
-
-
-
-

藥物治療
• 第一代藥物: 基利克
慢性骨髓性白血病(CML)的演進
基利克
第二代
骨髓移植
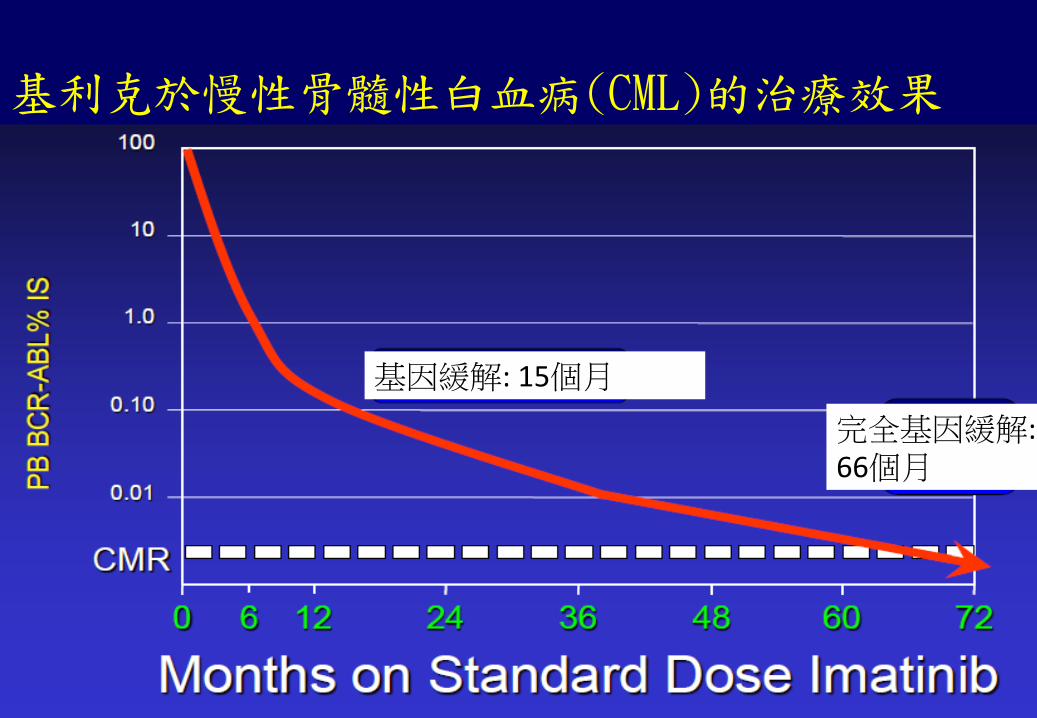
基利克於慢性骨髓性白血病(CML)的治療效果
基因緩解: 15個月
完全基因緩解: 66個月

基利克於慢性骨髓性白血病(CML)的長期追蹤
失去血液相緩解 失去基因緩解 慢性期轉加速期或急性期 死亡
慢性期轉加速期或急性期
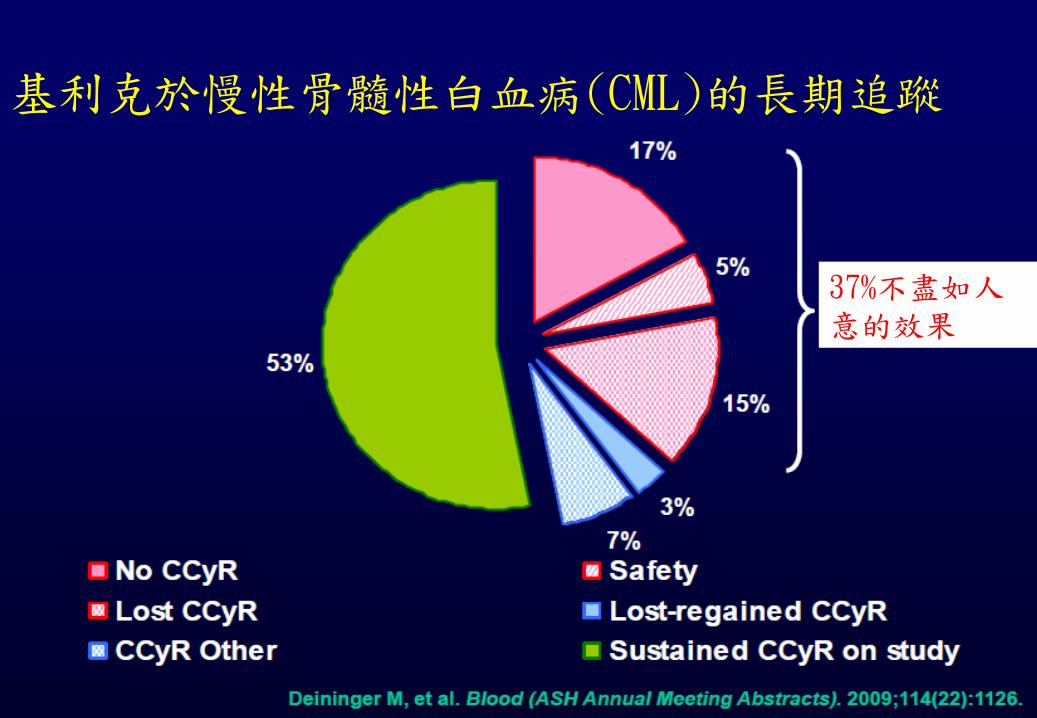
基利克於慢性骨髓性白血病(CML)的長期追蹤
37%不盡如人意的效果

進擊の TKI
泰息安
柏萊


歐洲白血病團體制定的治療指引 (針對TKI)2013:
References: 1. Baccarani M, et al. Presented at the 4th international Congress on Leukemia Lymphoma Myeloma. Istanbul, Turkey. May 22-25 2013.
時間 理想 警告 失敗
診斷時 - High risk
CCA in Ph+ -
用藥後3個月 微量疾病
RT-PCR: -1
Minor CgR to 95% Ph+
and/or > 10%
No CHR
and/or 95% Ph+
用藥後6個月 微量疾病
RT-PCR: -2
< CCgR to minor CgR
and/or > 1 – 10%
< minor CgR
and/or > 10%
用藥後12個月 微量疾病
RT-PCR: -3
> 0.1 – 1%
(CCyR, no MMR)
> 1% Ph+
and/or > 1%
(No CCyR)

泰息安使用三個月的成績
Outcome at
5 Yrs, %
Treatment BCR-ABL Level at 3 Mos P Value
≤ 1% > 1% - ≤ 10% > 10%
PFS Nilotinib* 94.6 95.3 78.3 .0010
Imatinib 95.3 98.5 80.1 < .0001
OS Nilotinib* 95.7 97.6 81.9 .0007
Imatinib 95.3 99.2 79.5 < .0001
MR4.5 Nilotinib* 70.0 52.0 8.0 .0001
Imatinib 67.0 34.0 15.0 .0016
Saglio G, et al. ASH 2013. Abstract 92.
BCR-ABL level ≤ 10%IS at 3 mos higher for nilotinib (91%) vs imatinib (67%) independent of Sokal risk score
*300 mg BID.
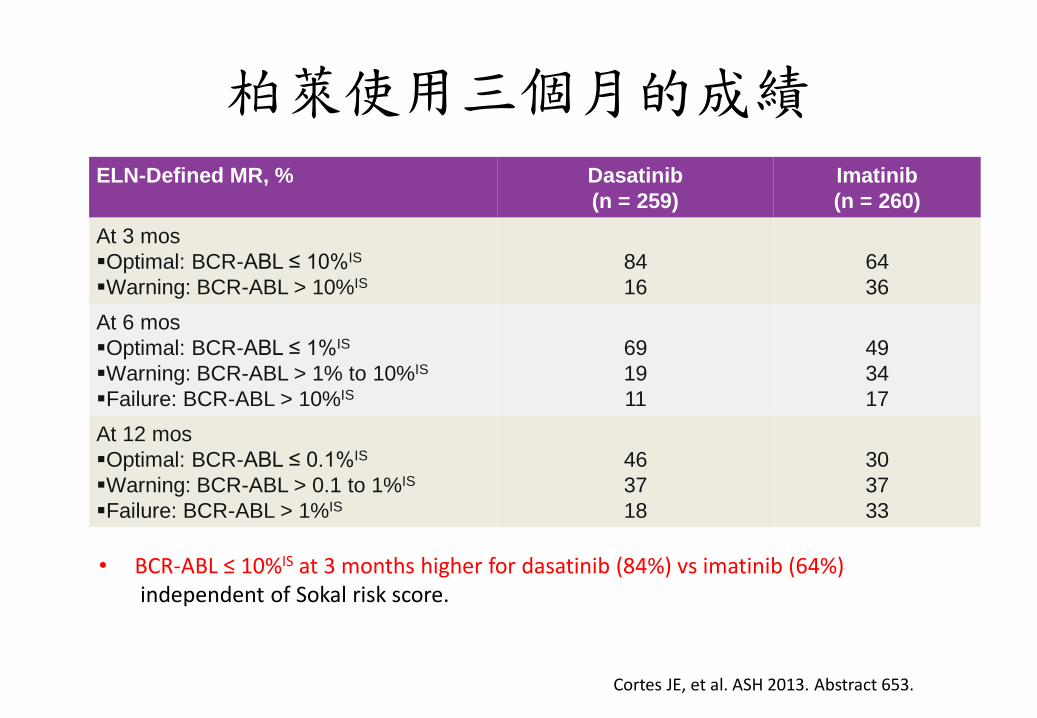
• BCR-ABL ≤ 10%IS at 3 months higher for dasatinib (84%) vs imatinib (64%) independent of Sokal risk score.
柏萊使用三個月的成績
Cortes JE, et al. ASH 2013. Abstract 653.
ELN-Defined MR, % Dasatinib
(n = 259)
Imatinib
(n = 260)
At 3 mos
Optimal: BCR-ABL ≤ 10%IS
Warning: BCR-ABL > 10%IS
84
16
64
36
At 6 mos
Optimal: BCR-ABL ≤ 1%IS
Warning: BCR-ABL > 1% to 10%IS
Failure: BCR-ABL > 10%IS
69
19
11
49
34
17
At 12 mos
Optimal: BCR-ABL ≤ 0.1%IS
Warning: BCR-ABL > 0.1 to 1%IS
Failure: BCR-ABL > 1%IS
46
37
18
30
37
33

泰息安使用後進展到加速期/急性期的比率
• Rates of progression to AP/BC were lower with nilotinib vs imatinib when including all progressions occurring on study
• 2 new cases of progression to AP/BC after discontinuation of core treatment were observed between the 4-yr analysis and the current analysis
– 1 in the imatinib arm and 1 in the nilotinib 300 mg BID arm
– BCR-ABL > 10%IS at 3 mos for both patients
Imatinib 400 mg BID (n = 283) Nilotinib 300 mg BID (n = 282)
Nilotinib 400 mg BID (n = 281)
Saglio G, et al. ASH 2013. Abstract 92.
Pat
ien
ts (
n)
Progressions of Study
7.1% 3.5% 2.1%
P = .0588 P = .0047
25
20
15
10
5
0
20
10
6 New events in Yr 5

柏萊使用後進展到加速期/急性期的比率
n =
Pat
ien
ts (
n)
On Study Including Follow-up Beyond Discontinuation (ITT)*
14 (5.4%)
8(3.1%)
12
18
Dasatinib 100 mg QD Imatinib 400 mg QD
259
260
259
260 0
5
20
10
15
Cortes JE, et al. ASH 2013. Abstract 653.
Saglio G, et al. ASH 2013. Abstract 92. Used with permission.
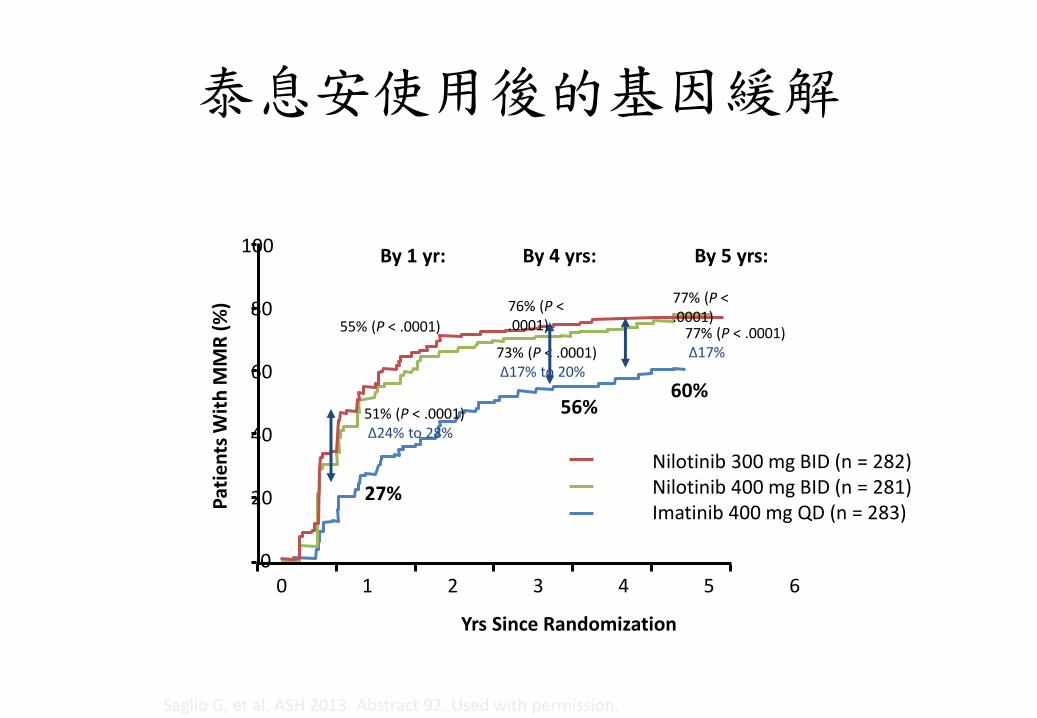
泰息安使用後的基因緩解
100
80
60
40
20
0 2 1 4 3 5 6
Yrs Since Randomization
Pat
ien
ts W
ith
MM
R (
%)
Nilotinib 300 mg BID (n = 282) Nilotinib 400 mg BID (n = 281) Imatinib 400 mg QD (n = 283)
By 1 yr: By 4 yrs:
73% (P < .0001) ∆17% to 20%
56%
27%
By 5 yrs:
77% (P < .0001) ∆17%
60% 51% (P < .0001) ∆24% to 28%
0
55% (P < .0001)
76% (P < .0001)
77% (P < .0001)

柏萊使用後的基因緩解
MMR = major molecular response, BCR-ABL ≤0.1%
MMR 4-year
cumulative rates
Hasford Risk Score
Low Intermediate High
Dasatinib 90% 70% 65%
Imatinib 69% 63% 52%
With faster and deeper responses, dasatinib maintained higher MMR rates vs imatinib at year 4 across all risk groups
Dasatinib 100 mg QD
Imatinib 400 mg QD
0 12 Months
24 36 48 60
0
20
40
60
80
100 P<0.0001
% W
ith
MM
R
46%
23%
64%
46%
69%
55%
74%
60%
76%
63%
1.6-fold higher likelihood of achieving MMR with dasatinib; HR=1.55 (1.26-1.91)

快=好?

如果都會到MMR…
• 王牌投手? • 普通投手 救援投手?

醫師我可以停藥嗎?
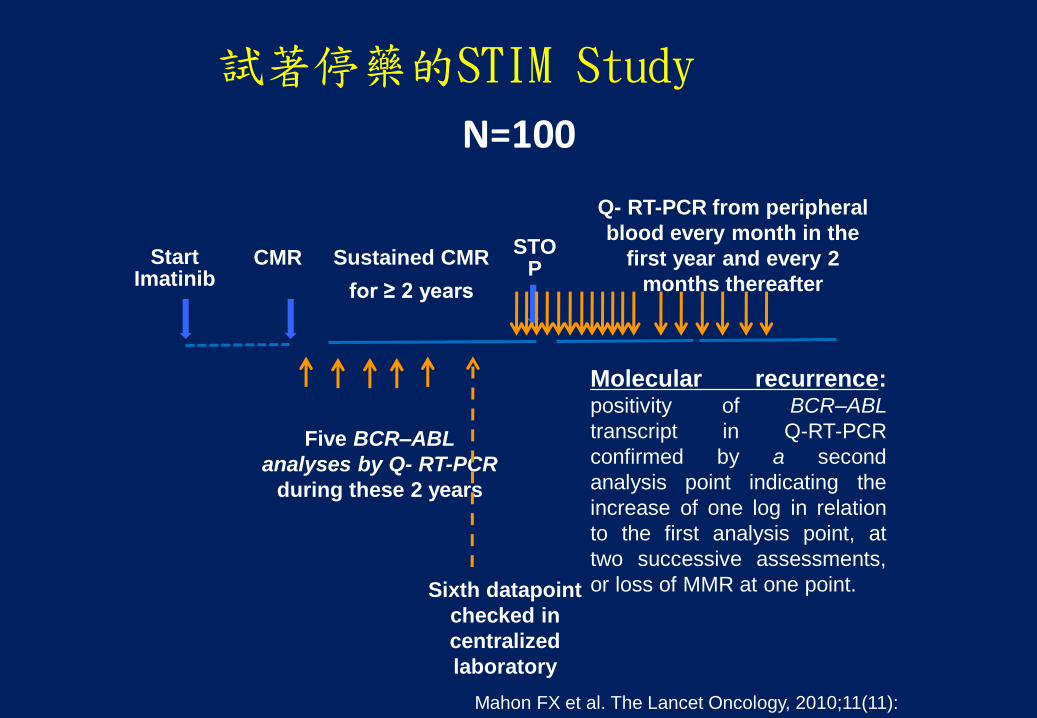
試著停藥的STIM Study
N=100
STOP
Sustained CMR
for ≥ 2 years
Start Imatinib
CMR
Q- RT-PCR from peripheral
blood every month in the
first year and every 2
months thereafter
Five BCR–ABL
analyses by Q- RT-PCR
during these 2 years
Sixth datapoint
checked in
centralized
laboratory
Mahon FX et al. The Lancet Oncology, 2010;11(11):
1029-1035.
Molecular recurrence: positivity of BCR–ABL
transcript in Q-RT-PCR
confirmed by a second
analysis point indicating the
increase of one log in relation
to the first analysis point, at
two successive assessments,
or loss of MMR at one point.

成功停藥的比率
Median follow up: 55 months (range 9-72)
Mahon et al., ASH 2013 [abstract 255]

第二代TKI的停藥試驗正在努力中…

如果你是想結婚、懷孕的女生…
現在的國際趨勢
• 利用第二代的TKI,在病患服藥的第一個月達到血液相緩解(-1 log),未來有較好的預後
• 較深較久的基因緩解率,以期能讓病患停藥

結論
• 把第二代的TKI提前到第一線使用,以目前的成績來看,不論是柏萊或泰息安,都有明顯較高的基因緩解率。
• 但長期(8~10年)的存活表現,目前尚未有結論,但極可能有較佳表現。
• 兩藥的副作用各有不同,需要在臨床上依醫師的判斷再作調整。





























