Embed Size (px)
Citation preview
RETIRED
Special Article
CME Practice parameter Neuroimagingof the neonate
Report of the Quality Standards Subcommittee of theAmerican Academy of Neurology and the Practice
Committee of the Child Neurology SocietyLR Ment MD HS Bada MD P Barnes MD PE Grant MD D Hirtz MD LA Papile MD
J PintondashMartin PhD M Rivkin MD and TL Slovis MD
Article abstractmdashObjective The authors reviewed available evidence on neonatal neuroimaging strategies for evaluatingboth very low birth weight preterm infants and encephalopathic term neonates Imaging for the preterm neonate Routinescreening cranial ultrasonography (US) should be performed on all infants of 30 weeksrsquo gestation once between 7 and 14days of age and should be optimally repeated between 36 and 40 weeksrsquo postmenstrual age This strategy detects lesionssuch as intraventricular hemorrhage which influences clinical care and those such as periventricular leukomalacia andlow-pressure ventriculomegaly which provide information about long-term neurodevelopmental outcome There is insuf-ficient evidence for routine MRI of all very low birth weight preterm infants with abnormal results of cranial US Imagingfor the term infant Noncontrast CT should be performed to detect hemorrhagic lesions in the encephalopathic term infantwith a history of birth trauma low hematocrit or coagulopathy If CT findings are inconclusive MRI should be performedbetween days 2 and 8 to assess the location and extent of injury The pattern of injury identified with conventional MRImay provide diagnostic and prognostic information for term infants with evidence of encephalopathy In particular basalganglia and thalamic lesions detected by conventional MRI are associated with poor neurodevelopmental outcomeDiffusion-weighted imaging may allow earlier detection of these cerebral injuries Recommendations US plays an estab-lished role in the management of preterm neonates of 30 weeksrsquo gestation US also provides valuable prognosticinformation when the infant reaches 40 weeksrsquo postmenstrual age For encephalopathic term infants early CT should beused to exclude hemorrhage MRI should be performed later in the first postnatal week to establish the pattern of injuryand predict neurologic outcome
NEUROLOGY 2002581726ndash1738
Despite the development of sophisticated care tech-niques the incidence of neurodevelopmental disabilityamong the survivors of newborn intensive care re-mains high1-4 As newborn special care enters its fifthdecade survival rates for both severely compromised
term infants and very low birth weight (VLBW) pre-term (PT) infants have increased56 However the inci-dence of cerebral palsy (CP) has not changed duringthe past 10 years the number of children with school-based problems is on the rise and the population ofinfants at risk for disability is increasing7-13 Becausethe clinical evaluation of these infants may not provideeither adequate diagnostic or prognostic informationneuroimaging is frequently used14-16
Additional material related to this article can be found on the NeurologyWeb site Go to wwwneurologyorg and scroll down the Table of Con-tents for the June 25 issue to find the title link for this article
This statement has been endorsed by the American Academy of Pediatrics the American Society of Pediatric Neuroradiology and the Society for PediatricRadiologyApproved by the AAN Quality Standards Subcommittee December 8 2001 Approved by the AAN Practice Committee January 28 2002 Approved by theAAN Board of Directors February 23 2002 Approved by the CNS Practice Committee January 30 2002From the Departments of Pediatrics and Neurology (Dr Ment) Yale University School of Medicine New Haven CT Department of Pediatrics (Dr Bada)Department of Radiology (Dr Barnes) Stanford University School of Medicine Stanford CA Departments of Radiology (Dr Grant) and Neurology (DrRivkin) Harvard University School of Medicine Boston MA Clinical Trials Section National Institute of Neurological Disorders and Stroke (Dr Hirtz)Bethesda MD Department of Pediatrics (Dr Papile) University of New Mexico Health Science Center Albuquerque Schools of Nursing and Medicine (DrPintondashMartin) University of Pennsylvania Philadelphia and Department of Radiology (Dr Slovis) Wayne State University School of Medicine Detroit MIAddress correspondence and reprint requests to the American Academy of Neurology 1080 Montreal Avenue St Paul MN 55116
1726 Copyright copy 2002 by AAN Enterprises Inc
RETIRED
RETIRED
Neuroimaging plays two important roles 1) diag-nosis of brain injury in the newborn at risk so thatappropriate medical management can be providedand 2) detection of those lesions associated withlong-term neurodevelopmental disability Currentlycranial ultrasonography (US) CT and MRI are themost available means for these tasks
Goals The Quality Standards Subcommittee of theAmerican Academy of Neurology and the PracticeCommittee of the Child Neurology Society seek todevelop scientifically sound clinically relevant prac-tice parameters for physicians for diagnostic proce-dures treatment modalities and clinical disordersPractice parameters are strategies for patient man-agement that might include diagnosis symptomtreatment or procedure evaluation They make spe-cific recommendations based on the analysis of evi-dence in the published literature
This practice parameter provides recommenda-tions in response to questions regarding brain imag-ing of PT and term infants For PT infants which PTinfants should undergo routine screening US Whenshould these studies be performed Do abnormalitiesshown by neonatal US require follow-up MRI Whatis the ability of US to accurately predict long-termneurodevelopmental outcome for this patient popula-tion For term infants which imaging strategies areable to provide clinically important information forinfants with neonatal encephalopathy Can MRI pro-vide prognostic information for these infants
Description of the process The committee con-sisted of neonatologists pediatric neurologists peri-natal epidemiologists and neonatal radiologistsselected by five professional organizations (see theelectronic version of this article for appendix 1 atwwwneurologyorg) we evaluated the quality of theevidence from the published literature Evidence re-viewed for this parameter was identified through lit-erature searches using MEDLINE and EMBASE forthe years 1990 to 2000 and CURRENT CONTENTSfor 2000 This literature search was updated in June2001 Relevant articles were chosen from theEnglish-language literature using the followingsearch terms neonate infant brain cerebral MRIMRS diffusion-weighted imaging (DWI) diffusiontensor imaging US echoencephalography Dopplerultrasonography cranial axial tomography near-infrared spectroscopy SPECT germinal matrix hem-orrhage intraventricular hemorrhage (IVH)periventricular leukomalacia (PVL) stroke ische-mia ventriculomegaly and echodensity Becauseneonatal practices and imaging strategies havechanged over the past decade1217-21 we reviewed onlythose references from 1990 onward
This search produced 1320 citations fromwhich 90 met the predefined inclusion criteria origi-nal clinical articles published since 1990 review ar-ticles and reports of meta-analyses
Each of the selected articles was reviewed ab-
stracted and classified (appendix 2) by at least tworeviewers Abstracted data included patient numbermean birth weight (BW) mean gestational age (GA)age at the time of the neuroimaging study primaryneuroimaging measure primary and secondary out-come measures and timing of subject selection (pro-spective retrospective case-control or case seriesstudy) We also noted both inclusion and exclusioncriteria for patient selection and description of theneuroimaging strategy in addition to the results ofthe given study
The strength of the evidence for each relevant ar-ticle was ranked using the defined criteria shown inappendix 2 Recommendations were derived based onthe strength of the evidence and stratified (level AB C or U) as shown in appendix 3
For the purposes of this practice parameter ascreening neuroimaging study was defined as onethat is routinely applied to identify infants at suffi-cient risk of a specific disorder who would benefitfrom further investigation or direct action but whohave no specific neurologic signs or symptoms re-quiring medical attention (eg infants born before28 weeks of gestation)
Neuroimaging strategies Although neuroimag-ing has proven to be extremely helpful for the assess-ment of injury to the PT brain and may provideuseful information for evaluating the infant withneonatal encephalopathy there are significant prob-lems associated with imaging of the critically ill in-fant142223 These include the choice of imagingtechnique the timing of the imaging study and re-gional variations in maturation of the developingbrain Further transporting acutely ill neonatesmany of whom require ventilatory assistance multi-ple indwelling catheters infusions vasopressor sup-port and warming lights represents a majorchallenge
Currently US CT and MRI represent the majorimaging modalities most widely available for evalu-ating critically ill infants
VLBW PT infants Birth weight (BW) remainsone of the most important predictors of infant mor-tality and morbidity VLBW infants (BW 1500grams) now represent 145 of all live births in theUnited States5624 In addition the survival rates forthis population are steadily increasing In contrastthe handicap rates for surviving infantsmdashparticu-larly those with the lowest BWmdashare high At 8 yearsof age 50 of children with BW of 1000 gramsare educated in special education classrooms or re-source rooms 20 have repeated a grade in schooland 10 to 15 have spastic motor handicaps1913
Hemorrhage hypoxia and ischemia are the majorcauses of injury to the PT brain and multiple studiesover the past decade have used neuroimaging tech-niques to assess these injuries24-28
US screening of the VLBW PT infant Althoughcranial US of VLBW PT infants is routinely performed
June (2 of 2) 2002 NEUROLOGY 58 1727
RETIRED
RETIRED
in newborn intensive care units the target popula-tions number of examinations and timing of thesestudies vary widely Further different institutions usedifferent systems of nomenclature to describe IVHwhite matter injury and ventriculomegaly the threemajor findings for the PT infant For this parameterthe grading system for IVH of Papile et al29 will beused (table 1) In addition because there is controversysurrounding the meaning of the periventricularechodensities routinely reported in US studies of PTinfants2830-32 injury to the PT white matter will includeonly periventricular cystic lesions114115 There is a con-sensus in the field that the degree of ventriculomegaly(see table 1) predicts long-term neurodevelopmentaloutcome for PT infants studied at or near term3334
Correlation of US findings with neuropathologicdata Before reviewing data pertinent to the prac-tice parameter questions the committee reviewedthe evidence correlating clinical US findings withneuropathologic data In four class II studies35-38
reporting results of a total of 87 autopsies per-formed on PT infants US was 76 to 100 accu-rate in detecting grade 1 lesions of 5 mm andgrade 3 and grade 4 hemorrhages (see the elec-tronic version of this article for table 4 at wwwneurologyorg) Detection of grade 2 hemorrhageswas much less accurate
Correlation of US findings of cystic PVL with neu-ropathologic data was evaluated in three class IIstudies38-40 Each study found 100 correlation be-tween US findings and neuropathologic data
Which PT infants should undergo routine screen-ing cranial US Evidence Seven class II studiesevaluated the need for screening cranial US in lowBW PT infants25272841-44 Review of these studies (ta-
ble 2 see the electronic version of this article fortable 5 at wwwneurologyorg) suggests that al-though cranial US of 12 to 51 of infants with BWof 1500 grams or GA of 33 weeks shows someabnormalities in the first 2 weeks of life major USabnormalities such as grades 3 and 4 IVH or bilat-eral cystic PVL occur in 20 of infants Further-more more severe abnormalities occur in thoseinfants with the lowest BW
Because infants with grades 3 and 4 IVH are atconsiderable risk for metabolic abnormalities post-hemorrhagic hydrocephalus and its sequelae (egapnea and obtundation) such a US finding would inall likelihood alter the infantrsquos care and thus wasconsidered clinically significant16 In addition cysticPVL and ventriculomegaly are risk factors for CPThese US findings might not only provide criticalprognostic information but also influence long-termcare strategies Therefore it is important to deter-mine which infants are at high risk for grades 3 and4 IVH cystic PVL andor ventriculomegaly
In only four studies the data were presented byspecific GA andor BW groups25284143 In these stud-ies grades 3 and 4 IVH was noted in 11 of infantswith BW of 1000 grams and in 5 of infants withBW of 1000 to 1250 grams when infants were com-pared by GA groups 16 of those with GA of 25weeks and 1 to 2 of infants with GA of 25 weekshad grades 3 and 4 IVH (see the electronic version ofthis article for table 5 at wwwneurologyorg) Like-wise cystic PVL was noted in 5 to 26 of infantsweighing 1000 grams compared with 1 to 5 ofinfants with BW of 1000 grams Ventriculomegalywas described in 5 to 7 of infants weighing1000 gramsConclusions Twelve percent to 51of infants with BW of 1500 grams andor GA of 33weeks have cranial US abnormalities (class II evi-dence) However major abnormalities such as grades3 and 4 IVH cystic PVL and ventriculomegalywhich might alter treatment or provide prognosticinformation are considerably more common (20ndash25) in infants with GA of 30 weeks
Recommendations (level B) Close to 25 of in-fants with GA of 30 weeks have significant cranialUS abnormalities that trigger important changes inacute and long-term care Therefore routine screen-ing cranial US should be performed on all infantswith GA of 30 weeks
When should screening cranial US be performedEvidence Multiple class II studies performed be-fore 1990 suggested that 90 of all IVH cases inVLBW PT infants were detected during postnataldays 4 to 545-48
Data from recent class II studies are shown intable 2 (see the electronic version of this article fortable 6 at wwwneurologyorg) In one study28 248infants with BW of 1500 grams underwent regularUS at predefined times (1ndash5 days 10ndash14 days 28days and term) Approximately 65 of IVH caseswere detected within the first week The other cases
Table 1 Classification of cranial ultrasound findings for thepreterm infant
Classification Findings
Intraventricular Grade 1 Germinal matrix hemorrhage
hemorrhage Grade 2 Blood within the ventricularsystem but not distending it
Grade 3 Intraventricular hemorrhagewith ventricular dilatation
Grade 4 Parenchymal involvement
Preterm whitematter injurydagger
Cysticlesions
Periventricular
VentriculomegalyDagger Mild 05ndash10 cmsect
Moderate 10ndash15 cmsect
Severe 15 cmsect
Reference 30daggerReferences 29 31ndash35DaggerReferences 36 37sect Measurements at the midbody of the lateral ventricle on sagit-
tal scan
1728 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
occurred in the second and third postnatal weeksand one infant developed severe IVH after postnatalday 28 When BW was 1000 grams severe IVHwas detected in 10 (77) of 13 infants on days 1 to 513 (100) of 13 cases of severe IVH were detected onday 28
In a study designed to assess changes in USfindings across time42 144 infants with BW of1500 grams or GA of 33 weeks underwent USbetween days 1 and 7 and then between days 10and 14 Fifteen infants (10) had significantchanges in US findings from the first to the secondscan Thirteen infants whose first US showed nor-mal results or grades 1 and 2 IVH were found tohave major abnormalities (ie grades 3 and 4 IVHandor PVL) at the time of the second scan Fortwo infants US findings changed from a majorabnormality during the first US (ie PVL) to eithernormal results or a minor abnormality (ie grade 2IVH) during the second US
Cystic PVL has been detected in infants withoutprevious US abnormalities as late as postnatal day104274344 In one report28 cystic PVL and ventriculo-megaly were found in 8 (3) of 256 neonates afterpreviously normal US findings For infants weighing1000 grams 3 (50) of 6 cases of PVL were notedat 36 to 40 weeksrsquo postmenstrual age
Conclusions The timing at which US can detectinjury in the developing brain may be changingGrades 3 and 4 IVH which may alter medical man-agement and prognostic information may be de-tected as late as the third postnatal week CysticPVL and ventriculomegaly which may alter progno-
sis and treatment programs may be first seen by USat term Furthermore these lesions may be detectedin many infants after previously normal US findings
Recommendation (level B) Screening cranial USshould be performed on all infants with GA of 30weeks at 7 to 14 days of age and should be optimallyrepeated at 36 to 40 weeksrsquo postmenstrual age Thisrecommendation is designed to detect both clinicallyunsuspected IVH which may require additional clin-ical andor radiologic monitoring and changes inmanagement plans and evidence for PVL andorventriculomegaly which are useful for prognosis andbest seen when the infants are examined at term
Do abnormalities of screening cranial US for thePT infant require follow-up MRI either to obtain in-formation for patient management or to provide long-term prognostic data Evidence Three recentclass II studies (see the electronic version of thisarticle for table 7 at wwwneurologyorg) comparedresults of cranial US and MRI performed during thenewborn period for PT infants264950 Maalouf et al26
performed paired MRI and US studies on the sameday for 32 infants with GA of 30 weeks US accu-rately detected the presence of germinal matrixIVH and parenchymal hemorrhage confirmed byMRI (positive predictive values of 08 085 and 096respectively) However in this study and others4950
white matter injury detected by MRI was less wellpredicted by US (sensitivity of 056ndash089) Addi-tional information provided by MRI included depic-tion of hemorrhagic lesions in 64 of infants andmore numerous or extensive cysts in infants with
Table 2 Incidence and timing of ultrasound abnormalities in preterm infants
Referenceno Class Inclusion criteria
USabnormalitiesincidence ()
Major abnormalitiesincidence ()
No () ofmajor
abnormalities
Incidence of majorabnormalities by
GA or BW
Timing of majorabnormalitiesincidence ()
41 II BW 1500 g GA34 wk
IVH 50250 (20) Grades 3 and 4 IVH13250 (5)
13 (5) GA of 25 wk 957(16) GA of 25wk 4193 (2)
42 II BW 1500 g 33wk
IVH andor PVL245338 (43)
Grades 3 and 4 IVHandor cystic PVL75338 (22)
75 (22) d 1ndash3 2775 (36)d 4ndash7 3675 (48)d 8ndash14 1275 (16)
43 II BW 1500 g PVL 14115 (12) BW of 1000 g1246 (26)
wk 1 614 (43)wk 3ndash15 814 (57)
25 II GA 32 wk BW1500 g or GA37 wk withventilator
IVH 106800(13)
Grades 2ndash4 IVH51800 (6)
51 (6) GA of 30 wk 46364 (13) GA of30 wk 5436 (1)
27 II GA 33 wk PVL 26172 (15) wk 1 1926 (73)wk 2ndash7 726 (27)
44 II GA 36 wk PVL 1153 (21) wk 1 1011 (91)wk 2 111 (9)
28 II BW 1500 g IVH PVL andorVM 161317(51)
Grades 3 and 4 IVHPVL andor VM40317 (13)
40 (126) BW of 1000 g13114 (114) BWof 1000 g 4203 (2)
BW of 1000 gwk 1 (52) wk 2(12) wk 4 (16)term (20)
BW birth weight GA gestational age wk week IVH intraventricular hemorrhage PVL periventricular leukomalacia VM ventriculomegalyd day
June (2 of 2) 2002 NEUROLOGY 58 1729
RETIRED
RETIRED
PVL diagnosed by US50 To date there has not beencorrelation with neurodevelopmental follow-up
Conclusions Compared with US performed onthe same day MRI of PT neonates detects morewhite matter abnormalities in the first week of lifemore hemorrhagic lesions and more numerous orextensive cysts There are insufficient data fromfollow-up studies to indicate whether these addi-tional findings provide more information about theneurodevelopmental prognosis
Recommendation (level C) Currently availabledata from class II studies do not provide sufficientevidence that routine MRI should be performed onall VLBW PT infants for whom results of screeningcranial US are abnormal
What is the ability of neonatal cranial US to pre-dict long-term neurodevelopmental outcome forVLBW PT infants Evidence VLBW PT infantsare at high risk for neurodevelopmental handicapDepending on the GA of the cohort and the year ofbirth the previously reported incidence of mentalretardation andor CP among PT infants rangedfrom 7 to almost 50145152 Further the timing ofcranial US used to predict outcome in the reportedliterature varied from the first 2 weeks of lifethrough term For this reason the lesions reportedand the predictive values for these lesions were diffi-cult to compare Finally in several studies childrendeemed excessively impaired were omitted from thefollow-up assessments and in many the outcomemeasures were reported in broad categories There-fore it was difficult to assess the nature of CP ormental retardation across cohorts
Only reports containing the following data wereincluded GA andor BW of the study populationpostmenstrual age of the ldquopredictorrdquo US when re-corded neurodevelopmental follow-up rate age atassessment and outcome variables
The six class II studies3453-57 (see the electronicversion of this article for table 8 at wwwneurologyorg) compared US findings with the incidence of CPfor almost 2250 VLBW PT children at ages 2 to 9years Significant associations between grade 4 IVHPVL andor ventriculomegaly and CP were noted inall six studies In the largest of these studies58 bothgrade 4 IVH and PVL were associated with CP (oddsratio [OR] 154 95 CI 76ndash311) any grade IVHalone was also associated with CP (OR 314 95 CI15ndash65) Similar data were available from one classIII study and three class IV studies (see the elec-tronic version of this article for table 8 atwwwneurologyorg)59-62
When the same groups from class II and class IIIstudies53-5557-596364 assessed the correlation of neona-tal US findings with the developmental quotientgrade 4 IVH and moderate to severe ventriculo-megaly were strongly associated with the risk ofmental retardation at 2 to 9 years of age (see theelectronic version of this article for table 8 at wwwneurologyorg) In these prospective studies OR
ranged from 997 to 190 In addition Whitaker etal65 demonstrated that for infants with BW of 500 to2000 grams who had grade 4 IVH andor moderateto severe ventriculomegaly the OR for the develop-ment of any neuropsychiatric disorder at the age 6years was 44
Conclusions Grades 3 and 4 IVH cystic PVLand moderate to severe ventriculomegaly determinedby US have all been shown to be significantly associ-ated with CP at 2 to 9 years of age in VLBW PTinfants (class II evidence) In addition class II evi-dence grade 4 IVH and ventriculomegaly have beensignificantly associated with mental retardation andneuropsychiatric disorders at the same time pointsThe OR which vary depending on the populationunder study the lesion and the outcome measureall indicate at least a 10-fold elevation in the risk ofadverse outcome for VLBW PT infants with US evi-dence of grades 3 and 4 IVH cystic PVL and moder-ate to severe ventriculomegaly
Recommendation (level A) For VLBW PT in-fants US should be used to predict long-term neuro-developmental outcome The findings of grades 3 and4 IVH periventricular cystic lesions and moderateto severe ventriculomegaly are all associated withadverse outcome
Term infants with neonatal encephalopathyClinical examination of the term infant with signsand symptoms of neonatal encephalopathy is oftenunable to determine the severity or extent of cerebraldamage and frequently provides little informationregarding the etiology of the insult Although numer-ous reports suggest that hypoxicndashischemic encepha-lopathy (HIE) is a common cause of neonatalencephalopathy the differential diagnosis of thiscondition is extensive including a spectrum of ab-normalities ranging from infectious to metabolic ab-normalities and congenital malformations6667 Evenin those infants with documented HIE the clinicalpresentation may vary widely68 Of those neonateswith moderate to severe HIE almost one-quarterhave mental retardation seizures and CP andpromising intervention strategies are now becomingavailable69-71 Therefore for diagnostic and prognos-tic reasons early assessment and diagnosis of in-fants with neonatal encephalopathy is important
For the definition of neonatal encephalopathy thecommittee used the criteria set forth by the Ameri-can Academy of Pediatrics and the American Collegeof Obstetricians and Gynecologists in Guidelines forPrenatal Care72 For results of a study to be rated asclass I evidence infants described therein must meetall of the following conditions
1 Profound metabolic or mixed acidemia (pH 700[umbilical cord artery blood sample if obtained])
2 Apgar score of 0 to 3 for 5 minutes3 Neonatal neurologic manifestations (eg seizures
coma or hypotonia)4 Multisystem organ dysfunction (eg cardiovascu-
1730 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
lar gastrointestinal hematologic pulmonary orrenal system)
Although these criteria were originally developedfor those infants thought to have HIE they also de-scribe any infant who requires immediate neonatalevaluationmdashboth to determine the underlying causeof encephalopathy and to provide therapeutic inter-ventions when available677374 Studies in which theentry criteria of the infants evaluated were less rig-orously defined received lower classification levelsthan did those in which infants met these conditions
Which neonatal neuroimaging strategies can detectcerebral abnormalities that may affect the immediateand long-term management of the infant with neona-tal encephalopathy Evidence One study dis-cussed gray-scale US of the infant with neonatalencephalopathy75 A second study compared findings ofgray-scale US and Doppler US with outcome76 and athird study compared results of gray-scale US andDoppler US with somatosensory evoked potentials vi-sual evoked potentials and results of the cerebral func-tion monitoring77 A fourth study compared findings ofgray-scale US Doppler US and CT78 Three otherstudies compared results of gray-scale US and MRI forinfants with neonatal encephalopathy79-81 Four studiesreported CT findings for these infants82-85
Gray-scale US Doppler US and studies compar-ing US with CT andor MRI In one class IIIstudy75 (see the electronic version of this article fortable 9 at wwwneurologyorg) US was performed on104 encephalopathic term neonates and 70 controlterm neonates on the first postnatal day A diffuseincrease in echogenicity of the cerebral parenchymaand slit-like ventricles were significantly more com-mon in infants with encephalopathy than in controls(39 versus 1 [p 0001] and 44 versus 9 [p 000l] respectively) but the investigators found nocorrelation between US findings on the first postna-tal day and neurodevelopmental status at 1 year ofage Similar results were noted in a class II studyevaluating term infants with neonatal encephalopa-thy on the first postnatal day76
In the same class II study76 analysis of simulta-neous Doppler US demonstrated resistive indices (re-sistive index peak systolic velocity minus enddiastolic velocity divided by peak systolic velocity) of060 for all children with adverse neurodevelop-mental outcome In another class II study78 gray-scale US Doppler US and CT were performed oninfants with neonatal encephalopathy (see the elec-tronic version of this article for table 9 at wwwneurologyorg) Gray-scale US was not predictive ofoutcome but a resistive index of 05 in the middlecerebral artery was associated with adverse neurode-velopmental outcome at 1 to 2 years (sensitivity82 specificity 89) In addition CT demonstrat-ing generalized decreased density had 91 sensitiv-ity and 100 specificity for adverse outcomes
Three studies compared early US and MRI studiesfor infants with neonatal encephalopathy (see the
electronic version of this article for table 9 atwwwneurologyorg)79-81 An abnormal MRI signal inthe basal ganglia in association with an abnormalUS result for the basal ganglia was most frequentlyassociated with an adverse neurodevelopmental out-come including CP seizures and developmental de-lay at 1 year of age while normal findings of US andCT or US and MRI had low negative predictivevalues
Conclusions Seven studies (classes II and III)assessed the role of gray-scale US in the diagnosis ofterm infants with neonatal encephalopathy Al-though gray-scale US can be easily performed at thebedside there are little data to support the use ofthis modality in imaging of the encephalopathic termneonate However two class II studies of Doppler USsuggested that resistive indices of 05ndash06 are con-sistent with the diagnosis of HIE
CT studies CT can be performed rapidly andwithout sedation of the neonate Four studies usedCT to evaluate term infants with neonatal encepha-lopathy One study84 reported basal ganglia changesa second study82 reported both basal ganglia and tha-lamic changes Two studies8385 used CT to detect in-tracranial hemorrhages in infants with signs andsymptoms of neonatal encephalopathy who also hadlow hematocrit or evidence of coagulopathy in bothstudies detection of intracranial hemorrhages al-tered clinical care
Conclusions One class II study and three classIV studies assessed the value of CT for encephalo-pathic term neonates Two studies suggested thatlow attenuation in the basal ganglia andor thalamiindicates severe injury consistent with HIE Theother two studies demonstrated that CT plays a rolein the detection of hemorrhagic lesions
MRI studies Two studies (see the electronic ver-sion of this article for table 9 at wwwneurologyorg)compared MRI findings with neuropathologic datafor infants with neonatal encephalopathy believedattributable to HIE8687 In the larger study87 imag-ing data were compared with results of neuropatho-logic analyses of the posterior limb of the internalcapsule thalamus parietal cortex hippocampusand medulla The posterior limb of the internal cap-sule was the most reliable region analyzed andagreement of MRI findings was similar to thatachieved by two pathologists reviewing the histologicsections ( 066) In this study the MRI abnormal-ity was predictive of the pathologic abnormality witha sensitivity of 070 and a positive predictive value of10 The predictive value of a single MRI abnormal-ity was 079 (95 CI 061ndash096)
In eight class II studies (see the electronic versionof this article for table 9 at wwwneurologyorg)288-94
conventional T1- and T2-weighted MRI studies wereperformed for a total of 272 term neonates most ofwhom were clinically suspected of having neonatalencephalopathy secondary to hypoxicndashischemic in-jury Scans were obtained at ages ranging from 1 to30 postnatal days and the mean age range was 2 to
June (2 of 2) 2002 NEUROLOGY 58 1731
RETIRED
RETIRED
8 days Three patterns of injury were detected byMRI 1) injury to the thalami andor posteriorndashlateral putamen with involvement of the subcorticalwhite matter in the most severe injuries 2) injury tothe parasagittal gray matter and subcortical whitematter posteriorly typically more than anteriorlyand 3) focal or multifocal injury Thalamic and basalganglia damage was the most common abnormalityreported This pattern of injury was detected in al-most 40 of infants and represented over one-half ofall abnormalities (see the electronic version of thisarticle for table 10 at wwwneurologyorg) In oneclass III study95 abnormal T1-weighted imagesshowing hyperintensities in a characteristic distribu-tion were demonstrated as early as 3 days after theinjury abnormal T2-weighted images showing hy-pointensities were demonstrated by 6 to 7 days
Conclusions Results of class II studies indicatethat characteristic MR patterns of cerebral injurycan be detected using conventional T1- and T2-weighted imaging sequences performed at mean agesof 2 to 8 days for encephalopathic term infants
Diffusion weighted imaging Studies of adult ar-terial infarcts have shown that DWI signal changesoccur within minutes of symptom onset and hoursbefore changes become apparent on T1- or T2-weighted images96 In one class II study86 and fourclass III studies97-100 that investigated the use of DWIin the evaluation of term neonates (see the electronicversion of this article for table 11 at wwwneurologyorg) entrance criteria were not stated in enough de-tail to determine which infants met strict criteria foracute neonatal encephalopathy and neonates withfocal seizures were also included MR studies wereperformed a mean of 2 to 4 days after birth and DWIfindings were compared with those of standard MRIsequences Abnormal DWI results were reported fortwo-thirds of infants For 7 to 58 of infants withabnormal DWI findings T2- andor T1-weighted im-ages were also abnormal Abnormal DWI results andnormal T1- andor T2- weighted images typically oc-curred when imaging was performed earlier than day 2of life or when there was diffuse white matter involve-ment Robertson et al99 described one patient for whomall imaging sequences including DWI and T1- and T2-weighted imaging sequences were normal when per-formed at 13 hours despite development of DWI andT1- and T2-weighted imaging abnormalities by 5 daysRobertson et al also described one other patient forwhom DWI results were normal at 8 days when T1-and T2-weighted images were abnormal this de-creased sensitivity of DWI in the subacute to chronicphase has also been noted for the adult populationsuggesting that the maximum sensitivity of DWI isbetween 2 and 8 days
Conclusions Findings of one class II study andfour class III studies suggest that DWI can provideevidence of cerebral injury before conventional MRItechniques for term infants with neonatal encepha-lopathy However DWI results may be negative if it
is performed earlier than 24 hours of life or laterthan 8 days of life
Proton MRS A number of investigators have ex-plored the utility of 1H-MRS and 31P-MRS at fieldstrengths of 15 T but the recommendations forthis parameter will be limited to 1H-MRS at 15 Tbecause this is the equipment most commonly avail-able for neonatal imaging All of the studies thatevaluated 1H-MRS at 15 T used single-voxel pointresolved spectroscopy (PRESS) or stimulate echo ac-quisition mode (STEAM) MRS although mutivoxelchemical shift imaging (CSI) allows high resolutionevaluation of larger regions of tissue there are nodata at this time that assess the role of this modalityin perinatal brain injury
In a number of class II studies (see the electronicversion of this article for table 12 at wwwneurologyorg) echo times of 136 msec and 272 msec were pre-ferred over the shorter echo times of 36 msec becauseof the higher SD of metabolite concentrations mea-sured at these shorter echo times2093 An echo time of136 msec has the additional advantage of an invertedlactate peak making distinction from lipids (which canresonate in the same region) more accurate
One class II study101 used MRS at 15 T within thefirst 18 hours in 31 cases of suspected HIE and in 7matched controls Lactatecreatine ratios rangedfrom 0 to 06 (median 005) for the seven controls Incontrast the investigators demonstrated lactatecreatine ratios of 10 for 10 (32) of the 31 infantswith suspected HIE In three additional class IIstudies93102103 proton MRS of the basal gangliawas performed within the first 2 weeks of life on 77infants with neonatal encephalopathy ElevatedlactateN-acetylaspartate ratios were the most con-sistent findings although elevated lactatecreatineand lactatecholine ratios were also reported for in-fants with suspected neonatal encephalopathy
Conclusions Data from class II studies suggestthat MRS can play an important role in the assess-ment of encephalopathic term infants Lactatecreat-ine ratios of 1 in the first 18 hours are morecommon in those infants with later neurologic find-ings consistent with HIE Elevated lactateNAA lac-tatecreatine and lactatecholine ratios in the first 2postnatal weeks are more common in infants withsuspected neonatal encephalopathy than in age-matched controls
Recommendations for diagnostic assessment1 For infants with a history of neonatal encepha-
lopathy significant birth trauma and evidence forlow hematocrit or coagulopathy
a Noncontrast CT should be performed to look forhemorrhage (level B)
b If the CT findings cannot explain the clinicalstatus of the neonate MRI should be performed (lev-el A)
2 For other neonates with acute encephalopathya MRI should be performed between days 2 and 8
of life (level A)1732 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
RETIRED
Neuroimaging plays two important roles 1) diag-nosis of brain injury in the newborn at risk so thatappropriate medical management can be providedand 2) detection of those lesions associated withlong-term neurodevelopmental disability Currentlycranial ultrasonography (US) CT and MRI are themost available means for these tasks
Goals The Quality Standards Subcommittee of theAmerican Academy of Neurology and the PracticeCommittee of the Child Neurology Society seek todevelop scientifically sound clinically relevant prac-tice parameters for physicians for diagnostic proce-dures treatment modalities and clinical disordersPractice parameters are strategies for patient man-agement that might include diagnosis symptomtreatment or procedure evaluation They make spe-cific recommendations based on the analysis of evi-dence in the published literature
This practice parameter provides recommenda-tions in response to questions regarding brain imag-ing of PT and term infants For PT infants which PTinfants should undergo routine screening US Whenshould these studies be performed Do abnormalitiesshown by neonatal US require follow-up MRI Whatis the ability of US to accurately predict long-termneurodevelopmental outcome for this patient popula-tion For term infants which imaging strategies areable to provide clinically important information forinfants with neonatal encephalopathy Can MRI pro-vide prognostic information for these infants
Description of the process The committee con-sisted of neonatologists pediatric neurologists peri-natal epidemiologists and neonatal radiologistsselected by five professional organizations (see theelectronic version of this article for appendix 1 atwwwneurologyorg) we evaluated the quality of theevidence from the published literature Evidence re-viewed for this parameter was identified through lit-erature searches using MEDLINE and EMBASE forthe years 1990 to 2000 and CURRENT CONTENTSfor 2000 This literature search was updated in June2001 Relevant articles were chosen from theEnglish-language literature using the followingsearch terms neonate infant brain cerebral MRIMRS diffusion-weighted imaging (DWI) diffusiontensor imaging US echoencephalography Dopplerultrasonography cranial axial tomography near-infrared spectroscopy SPECT germinal matrix hem-orrhage intraventricular hemorrhage (IVH)periventricular leukomalacia (PVL) stroke ische-mia ventriculomegaly and echodensity Becauseneonatal practices and imaging strategies havechanged over the past decade1217-21 we reviewed onlythose references from 1990 onward
This search produced 1320 citations fromwhich 90 met the predefined inclusion criteria origi-nal clinical articles published since 1990 review ar-ticles and reports of meta-analyses
Each of the selected articles was reviewed ab-
stracted and classified (appendix 2) by at least tworeviewers Abstracted data included patient numbermean birth weight (BW) mean gestational age (GA)age at the time of the neuroimaging study primaryneuroimaging measure primary and secondary out-come measures and timing of subject selection (pro-spective retrospective case-control or case seriesstudy) We also noted both inclusion and exclusioncriteria for patient selection and description of theneuroimaging strategy in addition to the results ofthe given study
The strength of the evidence for each relevant ar-ticle was ranked using the defined criteria shown inappendix 2 Recommendations were derived based onthe strength of the evidence and stratified (level AB C or U) as shown in appendix 3
For the purposes of this practice parameter ascreening neuroimaging study was defined as onethat is routinely applied to identify infants at suffi-cient risk of a specific disorder who would benefitfrom further investigation or direct action but whohave no specific neurologic signs or symptoms re-quiring medical attention (eg infants born before28 weeks of gestation)
Neuroimaging strategies Although neuroimag-ing has proven to be extremely helpful for the assess-ment of injury to the PT brain and may provideuseful information for evaluating the infant withneonatal encephalopathy there are significant prob-lems associated with imaging of the critically ill in-fant142223 These include the choice of imagingtechnique the timing of the imaging study and re-gional variations in maturation of the developingbrain Further transporting acutely ill neonatesmany of whom require ventilatory assistance multi-ple indwelling catheters infusions vasopressor sup-port and warming lights represents a majorchallenge
Currently US CT and MRI represent the majorimaging modalities most widely available for evalu-ating critically ill infants
VLBW PT infants Birth weight (BW) remainsone of the most important predictors of infant mor-tality and morbidity VLBW infants (BW 1500grams) now represent 145 of all live births in theUnited States5624 In addition the survival rates forthis population are steadily increasing In contrastthe handicap rates for surviving infantsmdashparticu-larly those with the lowest BWmdashare high At 8 yearsof age 50 of children with BW of 1000 gramsare educated in special education classrooms or re-source rooms 20 have repeated a grade in schooland 10 to 15 have spastic motor handicaps1913
Hemorrhage hypoxia and ischemia are the majorcauses of injury to the PT brain and multiple studiesover the past decade have used neuroimaging tech-niques to assess these injuries24-28
US screening of the VLBW PT infant Althoughcranial US of VLBW PT infants is routinely performed
June (2 of 2) 2002 NEUROLOGY 58 1727
RETIRED
RETIRED
in newborn intensive care units the target popula-tions number of examinations and timing of thesestudies vary widely Further different institutions usedifferent systems of nomenclature to describe IVHwhite matter injury and ventriculomegaly the threemajor findings for the PT infant For this parameterthe grading system for IVH of Papile et al29 will beused (table 1) In addition because there is controversysurrounding the meaning of the periventricularechodensities routinely reported in US studies of PTinfants2830-32 injury to the PT white matter will includeonly periventricular cystic lesions114115 There is a con-sensus in the field that the degree of ventriculomegaly(see table 1) predicts long-term neurodevelopmentaloutcome for PT infants studied at or near term3334
Correlation of US findings with neuropathologicdata Before reviewing data pertinent to the prac-tice parameter questions the committee reviewedthe evidence correlating clinical US findings withneuropathologic data In four class II studies35-38
reporting results of a total of 87 autopsies per-formed on PT infants US was 76 to 100 accu-rate in detecting grade 1 lesions of 5 mm andgrade 3 and grade 4 hemorrhages (see the elec-tronic version of this article for table 4 at wwwneurologyorg) Detection of grade 2 hemorrhageswas much less accurate
Correlation of US findings of cystic PVL with neu-ropathologic data was evaluated in three class IIstudies38-40 Each study found 100 correlation be-tween US findings and neuropathologic data
Which PT infants should undergo routine screen-ing cranial US Evidence Seven class II studiesevaluated the need for screening cranial US in lowBW PT infants25272841-44 Review of these studies (ta-
ble 2 see the electronic version of this article fortable 5 at wwwneurologyorg) suggests that al-though cranial US of 12 to 51 of infants with BWof 1500 grams or GA of 33 weeks shows someabnormalities in the first 2 weeks of life major USabnormalities such as grades 3 and 4 IVH or bilat-eral cystic PVL occur in 20 of infants Further-more more severe abnormalities occur in thoseinfants with the lowest BW
Because infants with grades 3 and 4 IVH are atconsiderable risk for metabolic abnormalities post-hemorrhagic hydrocephalus and its sequelae (egapnea and obtundation) such a US finding would inall likelihood alter the infantrsquos care and thus wasconsidered clinically significant16 In addition cysticPVL and ventriculomegaly are risk factors for CPThese US findings might not only provide criticalprognostic information but also influence long-termcare strategies Therefore it is important to deter-mine which infants are at high risk for grades 3 and4 IVH cystic PVL andor ventriculomegaly
In only four studies the data were presented byspecific GA andor BW groups25284143 In these stud-ies grades 3 and 4 IVH was noted in 11 of infantswith BW of 1000 grams and in 5 of infants withBW of 1000 to 1250 grams when infants were com-pared by GA groups 16 of those with GA of 25weeks and 1 to 2 of infants with GA of 25 weekshad grades 3 and 4 IVH (see the electronic version ofthis article for table 5 at wwwneurologyorg) Like-wise cystic PVL was noted in 5 to 26 of infantsweighing 1000 grams compared with 1 to 5 ofinfants with BW of 1000 grams Ventriculomegalywas described in 5 to 7 of infants weighing1000 gramsConclusions Twelve percent to 51of infants with BW of 1500 grams andor GA of 33weeks have cranial US abnormalities (class II evi-dence) However major abnormalities such as grades3 and 4 IVH cystic PVL and ventriculomegalywhich might alter treatment or provide prognosticinformation are considerably more common (20ndash25) in infants with GA of 30 weeks
Recommendations (level B) Close to 25 of in-fants with GA of 30 weeks have significant cranialUS abnormalities that trigger important changes inacute and long-term care Therefore routine screen-ing cranial US should be performed on all infantswith GA of 30 weeks
When should screening cranial US be performedEvidence Multiple class II studies performed be-fore 1990 suggested that 90 of all IVH cases inVLBW PT infants were detected during postnataldays 4 to 545-48
Data from recent class II studies are shown intable 2 (see the electronic version of this article fortable 6 at wwwneurologyorg) In one study28 248infants with BW of 1500 grams underwent regularUS at predefined times (1ndash5 days 10ndash14 days 28days and term) Approximately 65 of IVH caseswere detected within the first week The other cases
Table 1 Classification of cranial ultrasound findings for thepreterm infant
Classification Findings
Intraventricular Grade 1 Germinal matrix hemorrhage
hemorrhage Grade 2 Blood within the ventricularsystem but not distending it
Grade 3 Intraventricular hemorrhagewith ventricular dilatation
Grade 4 Parenchymal involvement
Preterm whitematter injurydagger
Cysticlesions
Periventricular
VentriculomegalyDagger Mild 05ndash10 cmsect
Moderate 10ndash15 cmsect
Severe 15 cmsect
Reference 30daggerReferences 29 31ndash35DaggerReferences 36 37sect Measurements at the midbody of the lateral ventricle on sagit-
tal scan
1728 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
occurred in the second and third postnatal weeksand one infant developed severe IVH after postnatalday 28 When BW was 1000 grams severe IVHwas detected in 10 (77) of 13 infants on days 1 to 513 (100) of 13 cases of severe IVH were detected onday 28
In a study designed to assess changes in USfindings across time42 144 infants with BW of1500 grams or GA of 33 weeks underwent USbetween days 1 and 7 and then between days 10and 14 Fifteen infants (10) had significantchanges in US findings from the first to the secondscan Thirteen infants whose first US showed nor-mal results or grades 1 and 2 IVH were found tohave major abnormalities (ie grades 3 and 4 IVHandor PVL) at the time of the second scan Fortwo infants US findings changed from a majorabnormality during the first US (ie PVL) to eithernormal results or a minor abnormality (ie grade 2IVH) during the second US
Cystic PVL has been detected in infants withoutprevious US abnormalities as late as postnatal day104274344 In one report28 cystic PVL and ventriculo-megaly were found in 8 (3) of 256 neonates afterpreviously normal US findings For infants weighing1000 grams 3 (50) of 6 cases of PVL were notedat 36 to 40 weeksrsquo postmenstrual age
Conclusions The timing at which US can detectinjury in the developing brain may be changingGrades 3 and 4 IVH which may alter medical man-agement and prognostic information may be de-tected as late as the third postnatal week CysticPVL and ventriculomegaly which may alter progno-
sis and treatment programs may be first seen by USat term Furthermore these lesions may be detectedin many infants after previously normal US findings
Recommendation (level B) Screening cranial USshould be performed on all infants with GA of 30weeks at 7 to 14 days of age and should be optimallyrepeated at 36 to 40 weeksrsquo postmenstrual age Thisrecommendation is designed to detect both clinicallyunsuspected IVH which may require additional clin-ical andor radiologic monitoring and changes inmanagement plans and evidence for PVL andorventriculomegaly which are useful for prognosis andbest seen when the infants are examined at term
Do abnormalities of screening cranial US for thePT infant require follow-up MRI either to obtain in-formation for patient management or to provide long-term prognostic data Evidence Three recentclass II studies (see the electronic version of thisarticle for table 7 at wwwneurologyorg) comparedresults of cranial US and MRI performed during thenewborn period for PT infants264950 Maalouf et al26
performed paired MRI and US studies on the sameday for 32 infants with GA of 30 weeks US accu-rately detected the presence of germinal matrixIVH and parenchymal hemorrhage confirmed byMRI (positive predictive values of 08 085 and 096respectively) However in this study and others4950
white matter injury detected by MRI was less wellpredicted by US (sensitivity of 056ndash089) Addi-tional information provided by MRI included depic-tion of hemorrhagic lesions in 64 of infants andmore numerous or extensive cysts in infants with
Table 2 Incidence and timing of ultrasound abnormalities in preterm infants
Referenceno Class Inclusion criteria
USabnormalitiesincidence ()
Major abnormalitiesincidence ()
No () ofmajor
abnormalities
Incidence of majorabnormalities by
GA or BW
Timing of majorabnormalitiesincidence ()
41 II BW 1500 g GA34 wk
IVH 50250 (20) Grades 3 and 4 IVH13250 (5)
13 (5) GA of 25 wk 957(16) GA of 25wk 4193 (2)
42 II BW 1500 g 33wk
IVH andor PVL245338 (43)
Grades 3 and 4 IVHandor cystic PVL75338 (22)
75 (22) d 1ndash3 2775 (36)d 4ndash7 3675 (48)d 8ndash14 1275 (16)
43 II BW 1500 g PVL 14115 (12) BW of 1000 g1246 (26)
wk 1 614 (43)wk 3ndash15 814 (57)
25 II GA 32 wk BW1500 g or GA37 wk withventilator
IVH 106800(13)
Grades 2ndash4 IVH51800 (6)
51 (6) GA of 30 wk 46364 (13) GA of30 wk 5436 (1)
27 II GA 33 wk PVL 26172 (15) wk 1 1926 (73)wk 2ndash7 726 (27)
44 II GA 36 wk PVL 1153 (21) wk 1 1011 (91)wk 2 111 (9)
28 II BW 1500 g IVH PVL andorVM 161317(51)
Grades 3 and 4 IVHPVL andor VM40317 (13)
40 (126) BW of 1000 g13114 (114) BWof 1000 g 4203 (2)
BW of 1000 gwk 1 (52) wk 2(12) wk 4 (16)term (20)
BW birth weight GA gestational age wk week IVH intraventricular hemorrhage PVL periventricular leukomalacia VM ventriculomegalyd day
June (2 of 2) 2002 NEUROLOGY 58 1729
RETIRED
RETIRED
PVL diagnosed by US50 To date there has not beencorrelation with neurodevelopmental follow-up
Conclusions Compared with US performed onthe same day MRI of PT neonates detects morewhite matter abnormalities in the first week of lifemore hemorrhagic lesions and more numerous orextensive cysts There are insufficient data fromfollow-up studies to indicate whether these addi-tional findings provide more information about theneurodevelopmental prognosis
Recommendation (level C) Currently availabledata from class II studies do not provide sufficientevidence that routine MRI should be performed onall VLBW PT infants for whom results of screeningcranial US are abnormal
What is the ability of neonatal cranial US to pre-dict long-term neurodevelopmental outcome forVLBW PT infants Evidence VLBW PT infantsare at high risk for neurodevelopmental handicapDepending on the GA of the cohort and the year ofbirth the previously reported incidence of mentalretardation andor CP among PT infants rangedfrom 7 to almost 50145152 Further the timing ofcranial US used to predict outcome in the reportedliterature varied from the first 2 weeks of lifethrough term For this reason the lesions reportedand the predictive values for these lesions were diffi-cult to compare Finally in several studies childrendeemed excessively impaired were omitted from thefollow-up assessments and in many the outcomemeasures were reported in broad categories There-fore it was difficult to assess the nature of CP ormental retardation across cohorts
Only reports containing the following data wereincluded GA andor BW of the study populationpostmenstrual age of the ldquopredictorrdquo US when re-corded neurodevelopmental follow-up rate age atassessment and outcome variables
The six class II studies3453-57 (see the electronicversion of this article for table 8 at wwwneurologyorg) compared US findings with the incidence of CPfor almost 2250 VLBW PT children at ages 2 to 9years Significant associations between grade 4 IVHPVL andor ventriculomegaly and CP were noted inall six studies In the largest of these studies58 bothgrade 4 IVH and PVL were associated with CP (oddsratio [OR] 154 95 CI 76ndash311) any grade IVHalone was also associated with CP (OR 314 95 CI15ndash65) Similar data were available from one classIII study and three class IV studies (see the elec-tronic version of this article for table 8 atwwwneurologyorg)59-62
When the same groups from class II and class IIIstudies53-5557-596364 assessed the correlation of neona-tal US findings with the developmental quotientgrade 4 IVH and moderate to severe ventriculo-megaly were strongly associated with the risk ofmental retardation at 2 to 9 years of age (see theelectronic version of this article for table 8 at wwwneurologyorg) In these prospective studies OR
ranged from 997 to 190 In addition Whitaker etal65 demonstrated that for infants with BW of 500 to2000 grams who had grade 4 IVH andor moderateto severe ventriculomegaly the OR for the develop-ment of any neuropsychiatric disorder at the age 6years was 44
Conclusions Grades 3 and 4 IVH cystic PVLand moderate to severe ventriculomegaly determinedby US have all been shown to be significantly associ-ated with CP at 2 to 9 years of age in VLBW PTinfants (class II evidence) In addition class II evi-dence grade 4 IVH and ventriculomegaly have beensignificantly associated with mental retardation andneuropsychiatric disorders at the same time pointsThe OR which vary depending on the populationunder study the lesion and the outcome measureall indicate at least a 10-fold elevation in the risk ofadverse outcome for VLBW PT infants with US evi-dence of grades 3 and 4 IVH cystic PVL and moder-ate to severe ventriculomegaly
Recommendation (level A) For VLBW PT in-fants US should be used to predict long-term neuro-developmental outcome The findings of grades 3 and4 IVH periventricular cystic lesions and moderateto severe ventriculomegaly are all associated withadverse outcome
Term infants with neonatal encephalopathyClinical examination of the term infant with signsand symptoms of neonatal encephalopathy is oftenunable to determine the severity or extent of cerebraldamage and frequently provides little informationregarding the etiology of the insult Although numer-ous reports suggest that hypoxicndashischemic encepha-lopathy (HIE) is a common cause of neonatalencephalopathy the differential diagnosis of thiscondition is extensive including a spectrum of ab-normalities ranging from infectious to metabolic ab-normalities and congenital malformations6667 Evenin those infants with documented HIE the clinicalpresentation may vary widely68 Of those neonateswith moderate to severe HIE almost one-quarterhave mental retardation seizures and CP andpromising intervention strategies are now becomingavailable69-71 Therefore for diagnostic and prognos-tic reasons early assessment and diagnosis of in-fants with neonatal encephalopathy is important
For the definition of neonatal encephalopathy thecommittee used the criteria set forth by the Ameri-can Academy of Pediatrics and the American Collegeof Obstetricians and Gynecologists in Guidelines forPrenatal Care72 For results of a study to be rated asclass I evidence infants described therein must meetall of the following conditions
1 Profound metabolic or mixed acidemia (pH 700[umbilical cord artery blood sample if obtained])
2 Apgar score of 0 to 3 for 5 minutes3 Neonatal neurologic manifestations (eg seizures
coma or hypotonia)4 Multisystem organ dysfunction (eg cardiovascu-
1730 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
lar gastrointestinal hematologic pulmonary orrenal system)
Although these criteria were originally developedfor those infants thought to have HIE they also de-scribe any infant who requires immediate neonatalevaluationmdashboth to determine the underlying causeof encephalopathy and to provide therapeutic inter-ventions when available677374 Studies in which theentry criteria of the infants evaluated were less rig-orously defined received lower classification levelsthan did those in which infants met these conditions
Which neonatal neuroimaging strategies can detectcerebral abnormalities that may affect the immediateand long-term management of the infant with neona-tal encephalopathy Evidence One study dis-cussed gray-scale US of the infant with neonatalencephalopathy75 A second study compared findings ofgray-scale US and Doppler US with outcome76 and athird study compared results of gray-scale US andDoppler US with somatosensory evoked potentials vi-sual evoked potentials and results of the cerebral func-tion monitoring77 A fourth study compared findings ofgray-scale US Doppler US and CT78 Three otherstudies compared results of gray-scale US and MRI forinfants with neonatal encephalopathy79-81 Four studiesreported CT findings for these infants82-85
Gray-scale US Doppler US and studies compar-ing US with CT andor MRI In one class IIIstudy75 (see the electronic version of this article fortable 9 at wwwneurologyorg) US was performed on104 encephalopathic term neonates and 70 controlterm neonates on the first postnatal day A diffuseincrease in echogenicity of the cerebral parenchymaand slit-like ventricles were significantly more com-mon in infants with encephalopathy than in controls(39 versus 1 [p 0001] and 44 versus 9 [p 000l] respectively) but the investigators found nocorrelation between US findings on the first postna-tal day and neurodevelopmental status at 1 year ofage Similar results were noted in a class II studyevaluating term infants with neonatal encephalopa-thy on the first postnatal day76
In the same class II study76 analysis of simulta-neous Doppler US demonstrated resistive indices (re-sistive index peak systolic velocity minus enddiastolic velocity divided by peak systolic velocity) of060 for all children with adverse neurodevelop-mental outcome In another class II study78 gray-scale US Doppler US and CT were performed oninfants with neonatal encephalopathy (see the elec-tronic version of this article for table 9 at wwwneurologyorg) Gray-scale US was not predictive ofoutcome but a resistive index of 05 in the middlecerebral artery was associated with adverse neurode-velopmental outcome at 1 to 2 years (sensitivity82 specificity 89) In addition CT demonstrat-ing generalized decreased density had 91 sensitiv-ity and 100 specificity for adverse outcomes
Three studies compared early US and MRI studiesfor infants with neonatal encephalopathy (see the
electronic version of this article for table 9 atwwwneurologyorg)79-81 An abnormal MRI signal inthe basal ganglia in association with an abnormalUS result for the basal ganglia was most frequentlyassociated with an adverse neurodevelopmental out-come including CP seizures and developmental de-lay at 1 year of age while normal findings of US andCT or US and MRI had low negative predictivevalues
Conclusions Seven studies (classes II and III)assessed the role of gray-scale US in the diagnosis ofterm infants with neonatal encephalopathy Al-though gray-scale US can be easily performed at thebedside there are little data to support the use ofthis modality in imaging of the encephalopathic termneonate However two class II studies of Doppler USsuggested that resistive indices of 05ndash06 are con-sistent with the diagnosis of HIE
CT studies CT can be performed rapidly andwithout sedation of the neonate Four studies usedCT to evaluate term infants with neonatal encepha-lopathy One study84 reported basal ganglia changesa second study82 reported both basal ganglia and tha-lamic changes Two studies8385 used CT to detect in-tracranial hemorrhages in infants with signs andsymptoms of neonatal encephalopathy who also hadlow hematocrit or evidence of coagulopathy in bothstudies detection of intracranial hemorrhages al-tered clinical care
Conclusions One class II study and three classIV studies assessed the value of CT for encephalo-pathic term neonates Two studies suggested thatlow attenuation in the basal ganglia andor thalamiindicates severe injury consistent with HIE Theother two studies demonstrated that CT plays a rolein the detection of hemorrhagic lesions
MRI studies Two studies (see the electronic ver-sion of this article for table 9 at wwwneurologyorg)compared MRI findings with neuropathologic datafor infants with neonatal encephalopathy believedattributable to HIE8687 In the larger study87 imag-ing data were compared with results of neuropatho-logic analyses of the posterior limb of the internalcapsule thalamus parietal cortex hippocampusand medulla The posterior limb of the internal cap-sule was the most reliable region analyzed andagreement of MRI findings was similar to thatachieved by two pathologists reviewing the histologicsections ( 066) In this study the MRI abnormal-ity was predictive of the pathologic abnormality witha sensitivity of 070 and a positive predictive value of10 The predictive value of a single MRI abnormal-ity was 079 (95 CI 061ndash096)
In eight class II studies (see the electronic versionof this article for table 9 at wwwneurologyorg)288-94
conventional T1- and T2-weighted MRI studies wereperformed for a total of 272 term neonates most ofwhom were clinically suspected of having neonatalencephalopathy secondary to hypoxicndashischemic in-jury Scans were obtained at ages ranging from 1 to30 postnatal days and the mean age range was 2 to
June (2 of 2) 2002 NEUROLOGY 58 1731
RETIRED
RETIRED
8 days Three patterns of injury were detected byMRI 1) injury to the thalami andor posteriorndashlateral putamen with involvement of the subcorticalwhite matter in the most severe injuries 2) injury tothe parasagittal gray matter and subcortical whitematter posteriorly typically more than anteriorlyand 3) focal or multifocal injury Thalamic and basalganglia damage was the most common abnormalityreported This pattern of injury was detected in al-most 40 of infants and represented over one-half ofall abnormalities (see the electronic version of thisarticle for table 10 at wwwneurologyorg) In oneclass III study95 abnormal T1-weighted imagesshowing hyperintensities in a characteristic distribu-tion were demonstrated as early as 3 days after theinjury abnormal T2-weighted images showing hy-pointensities were demonstrated by 6 to 7 days
Conclusions Results of class II studies indicatethat characteristic MR patterns of cerebral injurycan be detected using conventional T1- and T2-weighted imaging sequences performed at mean agesof 2 to 8 days for encephalopathic term infants
Diffusion weighted imaging Studies of adult ar-terial infarcts have shown that DWI signal changesoccur within minutes of symptom onset and hoursbefore changes become apparent on T1- or T2-weighted images96 In one class II study86 and fourclass III studies97-100 that investigated the use of DWIin the evaluation of term neonates (see the electronicversion of this article for table 11 at wwwneurologyorg) entrance criteria were not stated in enough de-tail to determine which infants met strict criteria foracute neonatal encephalopathy and neonates withfocal seizures were also included MR studies wereperformed a mean of 2 to 4 days after birth and DWIfindings were compared with those of standard MRIsequences Abnormal DWI results were reported fortwo-thirds of infants For 7 to 58 of infants withabnormal DWI findings T2- andor T1-weighted im-ages were also abnormal Abnormal DWI results andnormal T1- andor T2- weighted images typically oc-curred when imaging was performed earlier than day 2of life or when there was diffuse white matter involve-ment Robertson et al99 described one patient for whomall imaging sequences including DWI and T1- and T2-weighted imaging sequences were normal when per-formed at 13 hours despite development of DWI andT1- and T2-weighted imaging abnormalities by 5 daysRobertson et al also described one other patient forwhom DWI results were normal at 8 days when T1-and T2-weighted images were abnormal this de-creased sensitivity of DWI in the subacute to chronicphase has also been noted for the adult populationsuggesting that the maximum sensitivity of DWI isbetween 2 and 8 days
Conclusions Findings of one class II study andfour class III studies suggest that DWI can provideevidence of cerebral injury before conventional MRItechniques for term infants with neonatal encepha-lopathy However DWI results may be negative if it
is performed earlier than 24 hours of life or laterthan 8 days of life
Proton MRS A number of investigators have ex-plored the utility of 1H-MRS and 31P-MRS at fieldstrengths of 15 T but the recommendations forthis parameter will be limited to 1H-MRS at 15 Tbecause this is the equipment most commonly avail-able for neonatal imaging All of the studies thatevaluated 1H-MRS at 15 T used single-voxel pointresolved spectroscopy (PRESS) or stimulate echo ac-quisition mode (STEAM) MRS although mutivoxelchemical shift imaging (CSI) allows high resolutionevaluation of larger regions of tissue there are nodata at this time that assess the role of this modalityin perinatal brain injury
In a number of class II studies (see the electronicversion of this article for table 12 at wwwneurologyorg) echo times of 136 msec and 272 msec were pre-ferred over the shorter echo times of 36 msec becauseof the higher SD of metabolite concentrations mea-sured at these shorter echo times2093 An echo time of136 msec has the additional advantage of an invertedlactate peak making distinction from lipids (which canresonate in the same region) more accurate
One class II study101 used MRS at 15 T within thefirst 18 hours in 31 cases of suspected HIE and in 7matched controls Lactatecreatine ratios rangedfrom 0 to 06 (median 005) for the seven controls Incontrast the investigators demonstrated lactatecreatine ratios of 10 for 10 (32) of the 31 infantswith suspected HIE In three additional class IIstudies93102103 proton MRS of the basal gangliawas performed within the first 2 weeks of life on 77infants with neonatal encephalopathy ElevatedlactateN-acetylaspartate ratios were the most con-sistent findings although elevated lactatecreatineand lactatecholine ratios were also reported for in-fants with suspected neonatal encephalopathy
Conclusions Data from class II studies suggestthat MRS can play an important role in the assess-ment of encephalopathic term infants Lactatecreat-ine ratios of 1 in the first 18 hours are morecommon in those infants with later neurologic find-ings consistent with HIE Elevated lactateNAA lac-tatecreatine and lactatecholine ratios in the first 2postnatal weeks are more common in infants withsuspected neonatal encephalopathy than in age-matched controls
Recommendations for diagnostic assessment1 For infants with a history of neonatal encepha-
lopathy significant birth trauma and evidence forlow hematocrit or coagulopathy
a Noncontrast CT should be performed to look forhemorrhage (level B)
b If the CT findings cannot explain the clinicalstatus of the neonate MRI should be performed (lev-el A)
2 For other neonates with acute encephalopathya MRI should be performed between days 2 and 8
of life (level A)1732 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

RETIRED
in newborn intensive care units the target popula-tions number of examinations and timing of thesestudies vary widely Further different institutions usedifferent systems of nomenclature to describe IVHwhite matter injury and ventriculomegaly the threemajor findings for the PT infant For this parameterthe grading system for IVH of Papile et al29 will beused (table 1) In addition because there is controversysurrounding the meaning of the periventricularechodensities routinely reported in US studies of PTinfants2830-32 injury to the PT white matter will includeonly periventricular cystic lesions114115 There is a con-sensus in the field that the degree of ventriculomegaly(see table 1) predicts long-term neurodevelopmentaloutcome for PT infants studied at or near term3334
Correlation of US findings with neuropathologicdata Before reviewing data pertinent to the prac-tice parameter questions the committee reviewedthe evidence correlating clinical US findings withneuropathologic data In four class II studies35-38
reporting results of a total of 87 autopsies per-formed on PT infants US was 76 to 100 accu-rate in detecting grade 1 lesions of 5 mm andgrade 3 and grade 4 hemorrhages (see the elec-tronic version of this article for table 4 at wwwneurologyorg) Detection of grade 2 hemorrhageswas much less accurate
Correlation of US findings of cystic PVL with neu-ropathologic data was evaluated in three class IIstudies38-40 Each study found 100 correlation be-tween US findings and neuropathologic data
Which PT infants should undergo routine screen-ing cranial US Evidence Seven class II studiesevaluated the need for screening cranial US in lowBW PT infants25272841-44 Review of these studies (ta-
ble 2 see the electronic version of this article fortable 5 at wwwneurologyorg) suggests that al-though cranial US of 12 to 51 of infants with BWof 1500 grams or GA of 33 weeks shows someabnormalities in the first 2 weeks of life major USabnormalities such as grades 3 and 4 IVH or bilat-eral cystic PVL occur in 20 of infants Further-more more severe abnormalities occur in thoseinfants with the lowest BW
Because infants with grades 3 and 4 IVH are atconsiderable risk for metabolic abnormalities post-hemorrhagic hydrocephalus and its sequelae (egapnea and obtundation) such a US finding would inall likelihood alter the infantrsquos care and thus wasconsidered clinically significant16 In addition cysticPVL and ventriculomegaly are risk factors for CPThese US findings might not only provide criticalprognostic information but also influence long-termcare strategies Therefore it is important to deter-mine which infants are at high risk for grades 3 and4 IVH cystic PVL andor ventriculomegaly
In only four studies the data were presented byspecific GA andor BW groups25284143 In these stud-ies grades 3 and 4 IVH was noted in 11 of infantswith BW of 1000 grams and in 5 of infants withBW of 1000 to 1250 grams when infants were com-pared by GA groups 16 of those with GA of 25weeks and 1 to 2 of infants with GA of 25 weekshad grades 3 and 4 IVH (see the electronic version ofthis article for table 5 at wwwneurologyorg) Like-wise cystic PVL was noted in 5 to 26 of infantsweighing 1000 grams compared with 1 to 5 ofinfants with BW of 1000 grams Ventriculomegalywas described in 5 to 7 of infants weighing1000 gramsConclusions Twelve percent to 51of infants with BW of 1500 grams andor GA of 33weeks have cranial US abnormalities (class II evi-dence) However major abnormalities such as grades3 and 4 IVH cystic PVL and ventriculomegalywhich might alter treatment or provide prognosticinformation are considerably more common (20ndash25) in infants with GA of 30 weeks
Recommendations (level B) Close to 25 of in-fants with GA of 30 weeks have significant cranialUS abnormalities that trigger important changes inacute and long-term care Therefore routine screen-ing cranial US should be performed on all infantswith GA of 30 weeks
When should screening cranial US be performedEvidence Multiple class II studies performed be-fore 1990 suggested that 90 of all IVH cases inVLBW PT infants were detected during postnataldays 4 to 545-48
Data from recent class II studies are shown intable 2 (see the electronic version of this article fortable 6 at wwwneurologyorg) In one study28 248infants with BW of 1500 grams underwent regularUS at predefined times (1ndash5 days 10ndash14 days 28days and term) Approximately 65 of IVH caseswere detected within the first week The other cases
Table 1 Classification of cranial ultrasound findings for thepreterm infant
Classification Findings
Intraventricular Grade 1 Germinal matrix hemorrhage
hemorrhage Grade 2 Blood within the ventricularsystem but not distending it
Grade 3 Intraventricular hemorrhagewith ventricular dilatation
Grade 4 Parenchymal involvement
Preterm whitematter injurydagger
Cysticlesions
Periventricular
VentriculomegalyDagger Mild 05ndash10 cmsect
Moderate 10ndash15 cmsect
Severe 15 cmsect
Reference 30daggerReferences 29 31ndash35DaggerReferences 36 37sect Measurements at the midbody of the lateral ventricle on sagit-
tal scan
1728 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
occurred in the second and third postnatal weeksand one infant developed severe IVH after postnatalday 28 When BW was 1000 grams severe IVHwas detected in 10 (77) of 13 infants on days 1 to 513 (100) of 13 cases of severe IVH were detected onday 28
In a study designed to assess changes in USfindings across time42 144 infants with BW of1500 grams or GA of 33 weeks underwent USbetween days 1 and 7 and then between days 10and 14 Fifteen infants (10) had significantchanges in US findings from the first to the secondscan Thirteen infants whose first US showed nor-mal results or grades 1 and 2 IVH were found tohave major abnormalities (ie grades 3 and 4 IVHandor PVL) at the time of the second scan Fortwo infants US findings changed from a majorabnormality during the first US (ie PVL) to eithernormal results or a minor abnormality (ie grade 2IVH) during the second US
Cystic PVL has been detected in infants withoutprevious US abnormalities as late as postnatal day104274344 In one report28 cystic PVL and ventriculo-megaly were found in 8 (3) of 256 neonates afterpreviously normal US findings For infants weighing1000 grams 3 (50) of 6 cases of PVL were notedat 36 to 40 weeksrsquo postmenstrual age
Conclusions The timing at which US can detectinjury in the developing brain may be changingGrades 3 and 4 IVH which may alter medical man-agement and prognostic information may be de-tected as late as the third postnatal week CysticPVL and ventriculomegaly which may alter progno-
sis and treatment programs may be first seen by USat term Furthermore these lesions may be detectedin many infants after previously normal US findings
Recommendation (level B) Screening cranial USshould be performed on all infants with GA of 30weeks at 7 to 14 days of age and should be optimallyrepeated at 36 to 40 weeksrsquo postmenstrual age Thisrecommendation is designed to detect both clinicallyunsuspected IVH which may require additional clin-ical andor radiologic monitoring and changes inmanagement plans and evidence for PVL andorventriculomegaly which are useful for prognosis andbest seen when the infants are examined at term
Do abnormalities of screening cranial US for thePT infant require follow-up MRI either to obtain in-formation for patient management or to provide long-term prognostic data Evidence Three recentclass II studies (see the electronic version of thisarticle for table 7 at wwwneurologyorg) comparedresults of cranial US and MRI performed during thenewborn period for PT infants264950 Maalouf et al26
performed paired MRI and US studies on the sameday for 32 infants with GA of 30 weeks US accu-rately detected the presence of germinal matrixIVH and parenchymal hemorrhage confirmed byMRI (positive predictive values of 08 085 and 096respectively) However in this study and others4950
white matter injury detected by MRI was less wellpredicted by US (sensitivity of 056ndash089) Addi-tional information provided by MRI included depic-tion of hemorrhagic lesions in 64 of infants andmore numerous or extensive cysts in infants with
Table 2 Incidence and timing of ultrasound abnormalities in preterm infants
Referenceno Class Inclusion criteria
USabnormalitiesincidence ()
Major abnormalitiesincidence ()
No () ofmajor
abnormalities
Incidence of majorabnormalities by
GA or BW
Timing of majorabnormalitiesincidence ()
41 II BW 1500 g GA34 wk
IVH 50250 (20) Grades 3 and 4 IVH13250 (5)
13 (5) GA of 25 wk 957(16) GA of 25wk 4193 (2)
42 II BW 1500 g 33wk
IVH andor PVL245338 (43)
Grades 3 and 4 IVHandor cystic PVL75338 (22)
75 (22) d 1ndash3 2775 (36)d 4ndash7 3675 (48)d 8ndash14 1275 (16)
43 II BW 1500 g PVL 14115 (12) BW of 1000 g1246 (26)
wk 1 614 (43)wk 3ndash15 814 (57)
25 II GA 32 wk BW1500 g or GA37 wk withventilator
IVH 106800(13)
Grades 2ndash4 IVH51800 (6)
51 (6) GA of 30 wk 46364 (13) GA of30 wk 5436 (1)
27 II GA 33 wk PVL 26172 (15) wk 1 1926 (73)wk 2ndash7 726 (27)
44 II GA 36 wk PVL 1153 (21) wk 1 1011 (91)wk 2 111 (9)
28 II BW 1500 g IVH PVL andorVM 161317(51)
Grades 3 and 4 IVHPVL andor VM40317 (13)
40 (126) BW of 1000 g13114 (114) BWof 1000 g 4203 (2)
BW of 1000 gwk 1 (52) wk 2(12) wk 4 (16)term (20)
BW birth weight GA gestational age wk week IVH intraventricular hemorrhage PVL periventricular leukomalacia VM ventriculomegalyd day
June (2 of 2) 2002 NEUROLOGY 58 1729
RETIRED
RETIRED
PVL diagnosed by US50 To date there has not beencorrelation with neurodevelopmental follow-up
Conclusions Compared with US performed onthe same day MRI of PT neonates detects morewhite matter abnormalities in the first week of lifemore hemorrhagic lesions and more numerous orextensive cysts There are insufficient data fromfollow-up studies to indicate whether these addi-tional findings provide more information about theneurodevelopmental prognosis
Recommendation (level C) Currently availabledata from class II studies do not provide sufficientevidence that routine MRI should be performed onall VLBW PT infants for whom results of screeningcranial US are abnormal
What is the ability of neonatal cranial US to pre-dict long-term neurodevelopmental outcome forVLBW PT infants Evidence VLBW PT infantsare at high risk for neurodevelopmental handicapDepending on the GA of the cohort and the year ofbirth the previously reported incidence of mentalretardation andor CP among PT infants rangedfrom 7 to almost 50145152 Further the timing ofcranial US used to predict outcome in the reportedliterature varied from the first 2 weeks of lifethrough term For this reason the lesions reportedand the predictive values for these lesions were diffi-cult to compare Finally in several studies childrendeemed excessively impaired were omitted from thefollow-up assessments and in many the outcomemeasures were reported in broad categories There-fore it was difficult to assess the nature of CP ormental retardation across cohorts
Only reports containing the following data wereincluded GA andor BW of the study populationpostmenstrual age of the ldquopredictorrdquo US when re-corded neurodevelopmental follow-up rate age atassessment and outcome variables
The six class II studies3453-57 (see the electronicversion of this article for table 8 at wwwneurologyorg) compared US findings with the incidence of CPfor almost 2250 VLBW PT children at ages 2 to 9years Significant associations between grade 4 IVHPVL andor ventriculomegaly and CP were noted inall six studies In the largest of these studies58 bothgrade 4 IVH and PVL were associated with CP (oddsratio [OR] 154 95 CI 76ndash311) any grade IVHalone was also associated with CP (OR 314 95 CI15ndash65) Similar data were available from one classIII study and three class IV studies (see the elec-tronic version of this article for table 8 atwwwneurologyorg)59-62
When the same groups from class II and class IIIstudies53-5557-596364 assessed the correlation of neona-tal US findings with the developmental quotientgrade 4 IVH and moderate to severe ventriculo-megaly were strongly associated with the risk ofmental retardation at 2 to 9 years of age (see theelectronic version of this article for table 8 at wwwneurologyorg) In these prospective studies OR
ranged from 997 to 190 In addition Whitaker etal65 demonstrated that for infants with BW of 500 to2000 grams who had grade 4 IVH andor moderateto severe ventriculomegaly the OR for the develop-ment of any neuropsychiatric disorder at the age 6years was 44
Conclusions Grades 3 and 4 IVH cystic PVLand moderate to severe ventriculomegaly determinedby US have all been shown to be significantly associ-ated with CP at 2 to 9 years of age in VLBW PTinfants (class II evidence) In addition class II evi-dence grade 4 IVH and ventriculomegaly have beensignificantly associated with mental retardation andneuropsychiatric disorders at the same time pointsThe OR which vary depending on the populationunder study the lesion and the outcome measureall indicate at least a 10-fold elevation in the risk ofadverse outcome for VLBW PT infants with US evi-dence of grades 3 and 4 IVH cystic PVL and moder-ate to severe ventriculomegaly
Recommendation (level A) For VLBW PT in-fants US should be used to predict long-term neuro-developmental outcome The findings of grades 3 and4 IVH periventricular cystic lesions and moderateto severe ventriculomegaly are all associated withadverse outcome
Term infants with neonatal encephalopathyClinical examination of the term infant with signsand symptoms of neonatal encephalopathy is oftenunable to determine the severity or extent of cerebraldamage and frequently provides little informationregarding the etiology of the insult Although numer-ous reports suggest that hypoxicndashischemic encepha-lopathy (HIE) is a common cause of neonatalencephalopathy the differential diagnosis of thiscondition is extensive including a spectrum of ab-normalities ranging from infectious to metabolic ab-normalities and congenital malformations6667 Evenin those infants with documented HIE the clinicalpresentation may vary widely68 Of those neonateswith moderate to severe HIE almost one-quarterhave mental retardation seizures and CP andpromising intervention strategies are now becomingavailable69-71 Therefore for diagnostic and prognos-tic reasons early assessment and diagnosis of in-fants with neonatal encephalopathy is important
For the definition of neonatal encephalopathy thecommittee used the criteria set forth by the Ameri-can Academy of Pediatrics and the American Collegeof Obstetricians and Gynecologists in Guidelines forPrenatal Care72 For results of a study to be rated asclass I evidence infants described therein must meetall of the following conditions
1 Profound metabolic or mixed acidemia (pH 700[umbilical cord artery blood sample if obtained])
2 Apgar score of 0 to 3 for 5 minutes3 Neonatal neurologic manifestations (eg seizures
coma or hypotonia)4 Multisystem organ dysfunction (eg cardiovascu-
1730 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
lar gastrointestinal hematologic pulmonary orrenal system)
Although these criteria were originally developedfor those infants thought to have HIE they also de-scribe any infant who requires immediate neonatalevaluationmdashboth to determine the underlying causeof encephalopathy and to provide therapeutic inter-ventions when available677374 Studies in which theentry criteria of the infants evaluated were less rig-orously defined received lower classification levelsthan did those in which infants met these conditions
Which neonatal neuroimaging strategies can detectcerebral abnormalities that may affect the immediateand long-term management of the infant with neona-tal encephalopathy Evidence One study dis-cussed gray-scale US of the infant with neonatalencephalopathy75 A second study compared findings ofgray-scale US and Doppler US with outcome76 and athird study compared results of gray-scale US andDoppler US with somatosensory evoked potentials vi-sual evoked potentials and results of the cerebral func-tion monitoring77 A fourth study compared findings ofgray-scale US Doppler US and CT78 Three otherstudies compared results of gray-scale US and MRI forinfants with neonatal encephalopathy79-81 Four studiesreported CT findings for these infants82-85
Gray-scale US Doppler US and studies compar-ing US with CT andor MRI In one class IIIstudy75 (see the electronic version of this article fortable 9 at wwwneurologyorg) US was performed on104 encephalopathic term neonates and 70 controlterm neonates on the first postnatal day A diffuseincrease in echogenicity of the cerebral parenchymaand slit-like ventricles were significantly more com-mon in infants with encephalopathy than in controls(39 versus 1 [p 0001] and 44 versus 9 [p 000l] respectively) but the investigators found nocorrelation between US findings on the first postna-tal day and neurodevelopmental status at 1 year ofage Similar results were noted in a class II studyevaluating term infants with neonatal encephalopa-thy on the first postnatal day76
In the same class II study76 analysis of simulta-neous Doppler US demonstrated resistive indices (re-sistive index peak systolic velocity minus enddiastolic velocity divided by peak systolic velocity) of060 for all children with adverse neurodevelop-mental outcome In another class II study78 gray-scale US Doppler US and CT were performed oninfants with neonatal encephalopathy (see the elec-tronic version of this article for table 9 at wwwneurologyorg) Gray-scale US was not predictive ofoutcome but a resistive index of 05 in the middlecerebral artery was associated with adverse neurode-velopmental outcome at 1 to 2 years (sensitivity82 specificity 89) In addition CT demonstrat-ing generalized decreased density had 91 sensitiv-ity and 100 specificity for adverse outcomes
Three studies compared early US and MRI studiesfor infants with neonatal encephalopathy (see the
electronic version of this article for table 9 atwwwneurologyorg)79-81 An abnormal MRI signal inthe basal ganglia in association with an abnormalUS result for the basal ganglia was most frequentlyassociated with an adverse neurodevelopmental out-come including CP seizures and developmental de-lay at 1 year of age while normal findings of US andCT or US and MRI had low negative predictivevalues
Conclusions Seven studies (classes II and III)assessed the role of gray-scale US in the diagnosis ofterm infants with neonatal encephalopathy Al-though gray-scale US can be easily performed at thebedside there are little data to support the use ofthis modality in imaging of the encephalopathic termneonate However two class II studies of Doppler USsuggested that resistive indices of 05ndash06 are con-sistent with the diagnosis of HIE
CT studies CT can be performed rapidly andwithout sedation of the neonate Four studies usedCT to evaluate term infants with neonatal encepha-lopathy One study84 reported basal ganglia changesa second study82 reported both basal ganglia and tha-lamic changes Two studies8385 used CT to detect in-tracranial hemorrhages in infants with signs andsymptoms of neonatal encephalopathy who also hadlow hematocrit or evidence of coagulopathy in bothstudies detection of intracranial hemorrhages al-tered clinical care
Conclusions One class II study and three classIV studies assessed the value of CT for encephalo-pathic term neonates Two studies suggested thatlow attenuation in the basal ganglia andor thalamiindicates severe injury consistent with HIE Theother two studies demonstrated that CT plays a rolein the detection of hemorrhagic lesions
MRI studies Two studies (see the electronic ver-sion of this article for table 9 at wwwneurologyorg)compared MRI findings with neuropathologic datafor infants with neonatal encephalopathy believedattributable to HIE8687 In the larger study87 imag-ing data were compared with results of neuropatho-logic analyses of the posterior limb of the internalcapsule thalamus parietal cortex hippocampusand medulla The posterior limb of the internal cap-sule was the most reliable region analyzed andagreement of MRI findings was similar to thatachieved by two pathologists reviewing the histologicsections ( 066) In this study the MRI abnormal-ity was predictive of the pathologic abnormality witha sensitivity of 070 and a positive predictive value of10 The predictive value of a single MRI abnormal-ity was 079 (95 CI 061ndash096)
In eight class II studies (see the electronic versionof this article for table 9 at wwwneurologyorg)288-94
conventional T1- and T2-weighted MRI studies wereperformed for a total of 272 term neonates most ofwhom were clinically suspected of having neonatalencephalopathy secondary to hypoxicndashischemic in-jury Scans were obtained at ages ranging from 1 to30 postnatal days and the mean age range was 2 to
June (2 of 2) 2002 NEUROLOGY 58 1731
RETIRED
RETIRED
8 days Three patterns of injury were detected byMRI 1) injury to the thalami andor posteriorndashlateral putamen with involvement of the subcorticalwhite matter in the most severe injuries 2) injury tothe parasagittal gray matter and subcortical whitematter posteriorly typically more than anteriorlyand 3) focal or multifocal injury Thalamic and basalganglia damage was the most common abnormalityreported This pattern of injury was detected in al-most 40 of infants and represented over one-half ofall abnormalities (see the electronic version of thisarticle for table 10 at wwwneurologyorg) In oneclass III study95 abnormal T1-weighted imagesshowing hyperintensities in a characteristic distribu-tion were demonstrated as early as 3 days after theinjury abnormal T2-weighted images showing hy-pointensities were demonstrated by 6 to 7 days
Conclusions Results of class II studies indicatethat characteristic MR patterns of cerebral injurycan be detected using conventional T1- and T2-weighted imaging sequences performed at mean agesof 2 to 8 days for encephalopathic term infants
Diffusion weighted imaging Studies of adult ar-terial infarcts have shown that DWI signal changesoccur within minutes of symptom onset and hoursbefore changes become apparent on T1- or T2-weighted images96 In one class II study86 and fourclass III studies97-100 that investigated the use of DWIin the evaluation of term neonates (see the electronicversion of this article for table 11 at wwwneurologyorg) entrance criteria were not stated in enough de-tail to determine which infants met strict criteria foracute neonatal encephalopathy and neonates withfocal seizures were also included MR studies wereperformed a mean of 2 to 4 days after birth and DWIfindings were compared with those of standard MRIsequences Abnormal DWI results were reported fortwo-thirds of infants For 7 to 58 of infants withabnormal DWI findings T2- andor T1-weighted im-ages were also abnormal Abnormal DWI results andnormal T1- andor T2- weighted images typically oc-curred when imaging was performed earlier than day 2of life or when there was diffuse white matter involve-ment Robertson et al99 described one patient for whomall imaging sequences including DWI and T1- and T2-weighted imaging sequences were normal when per-formed at 13 hours despite development of DWI andT1- and T2-weighted imaging abnormalities by 5 daysRobertson et al also described one other patient forwhom DWI results were normal at 8 days when T1-and T2-weighted images were abnormal this de-creased sensitivity of DWI in the subacute to chronicphase has also been noted for the adult populationsuggesting that the maximum sensitivity of DWI isbetween 2 and 8 days
Conclusions Findings of one class II study andfour class III studies suggest that DWI can provideevidence of cerebral injury before conventional MRItechniques for term infants with neonatal encepha-lopathy However DWI results may be negative if it
is performed earlier than 24 hours of life or laterthan 8 days of life
Proton MRS A number of investigators have ex-plored the utility of 1H-MRS and 31P-MRS at fieldstrengths of 15 T but the recommendations forthis parameter will be limited to 1H-MRS at 15 Tbecause this is the equipment most commonly avail-able for neonatal imaging All of the studies thatevaluated 1H-MRS at 15 T used single-voxel pointresolved spectroscopy (PRESS) or stimulate echo ac-quisition mode (STEAM) MRS although mutivoxelchemical shift imaging (CSI) allows high resolutionevaluation of larger regions of tissue there are nodata at this time that assess the role of this modalityin perinatal brain injury
In a number of class II studies (see the electronicversion of this article for table 12 at wwwneurologyorg) echo times of 136 msec and 272 msec were pre-ferred over the shorter echo times of 36 msec becauseof the higher SD of metabolite concentrations mea-sured at these shorter echo times2093 An echo time of136 msec has the additional advantage of an invertedlactate peak making distinction from lipids (which canresonate in the same region) more accurate
One class II study101 used MRS at 15 T within thefirst 18 hours in 31 cases of suspected HIE and in 7matched controls Lactatecreatine ratios rangedfrom 0 to 06 (median 005) for the seven controls Incontrast the investigators demonstrated lactatecreatine ratios of 10 for 10 (32) of the 31 infantswith suspected HIE In three additional class IIstudies93102103 proton MRS of the basal gangliawas performed within the first 2 weeks of life on 77infants with neonatal encephalopathy ElevatedlactateN-acetylaspartate ratios were the most con-sistent findings although elevated lactatecreatineand lactatecholine ratios were also reported for in-fants with suspected neonatal encephalopathy
Conclusions Data from class II studies suggestthat MRS can play an important role in the assess-ment of encephalopathic term infants Lactatecreat-ine ratios of 1 in the first 18 hours are morecommon in those infants with later neurologic find-ings consistent with HIE Elevated lactateNAA lac-tatecreatine and lactatecholine ratios in the first 2postnatal weeks are more common in infants withsuspected neonatal encephalopathy than in age-matched controls
Recommendations for diagnostic assessment1 For infants with a history of neonatal encepha-
lopathy significant birth trauma and evidence forlow hematocrit or coagulopathy
a Noncontrast CT should be performed to look forhemorrhage (level B)
b If the CT findings cannot explain the clinicalstatus of the neonate MRI should be performed (lev-el A)
2 For other neonates with acute encephalopathya MRI should be performed between days 2 and 8
of life (level A)1732 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
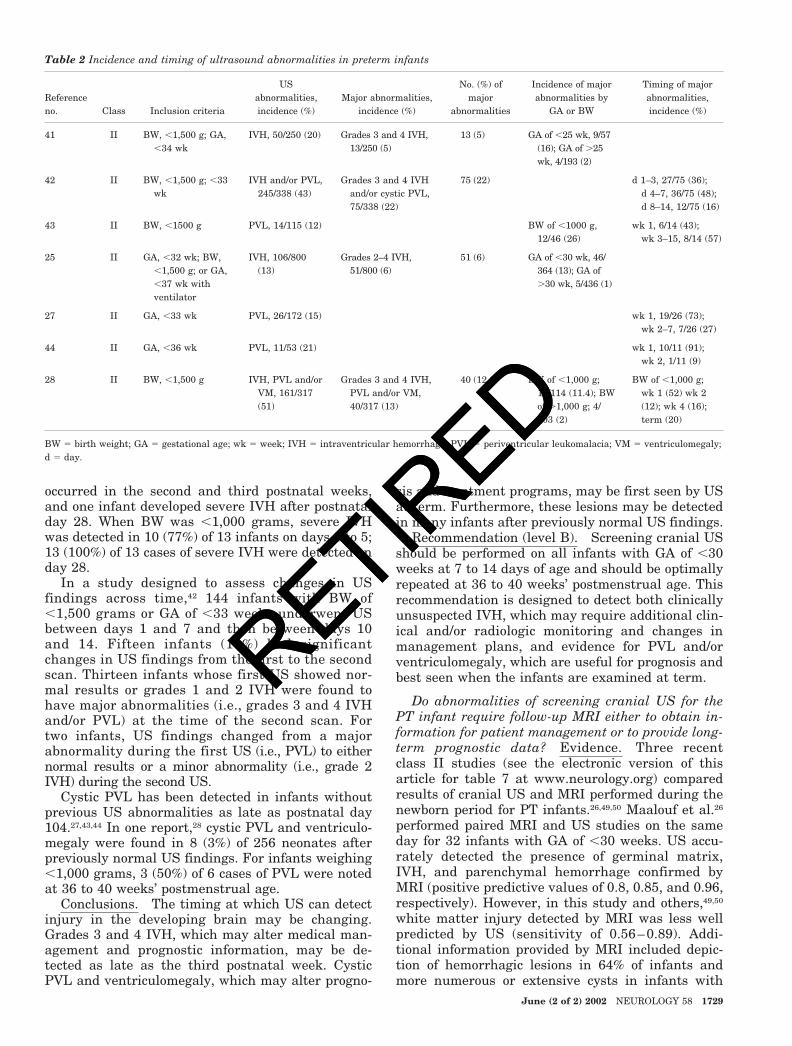
RETIRED
occurred in the second and third postnatal weeksand one infant developed severe IVH after postnatalday 28 When BW was 1000 grams severe IVHwas detected in 10 (77) of 13 infants on days 1 to 513 (100) of 13 cases of severe IVH were detected onday 28
In a study designed to assess changes in USfindings across time42 144 infants with BW of1500 grams or GA of 33 weeks underwent USbetween days 1 and 7 and then between days 10and 14 Fifteen infants (10) had significantchanges in US findings from the first to the secondscan Thirteen infants whose first US showed nor-mal results or grades 1 and 2 IVH were found tohave major abnormalities (ie grades 3 and 4 IVHandor PVL) at the time of the second scan Fortwo infants US findings changed from a majorabnormality during the first US (ie PVL) to eithernormal results or a minor abnormality (ie grade 2IVH) during the second US
Cystic PVL has been detected in infants withoutprevious US abnormalities as late as postnatal day104274344 In one report28 cystic PVL and ventriculo-megaly were found in 8 (3) of 256 neonates afterpreviously normal US findings For infants weighing1000 grams 3 (50) of 6 cases of PVL were notedat 36 to 40 weeksrsquo postmenstrual age
Conclusions The timing at which US can detectinjury in the developing brain may be changingGrades 3 and 4 IVH which may alter medical man-agement and prognostic information may be de-tected as late as the third postnatal week CysticPVL and ventriculomegaly which may alter progno-
sis and treatment programs may be first seen by USat term Furthermore these lesions may be detectedin many infants after previously normal US findings
Recommendation (level B) Screening cranial USshould be performed on all infants with GA of 30weeks at 7 to 14 days of age and should be optimallyrepeated at 36 to 40 weeksrsquo postmenstrual age Thisrecommendation is designed to detect both clinicallyunsuspected IVH which may require additional clin-ical andor radiologic monitoring and changes inmanagement plans and evidence for PVL andorventriculomegaly which are useful for prognosis andbest seen when the infants are examined at term
Do abnormalities of screening cranial US for thePT infant require follow-up MRI either to obtain in-formation for patient management or to provide long-term prognostic data Evidence Three recentclass II studies (see the electronic version of thisarticle for table 7 at wwwneurologyorg) comparedresults of cranial US and MRI performed during thenewborn period for PT infants264950 Maalouf et al26
performed paired MRI and US studies on the sameday for 32 infants with GA of 30 weeks US accu-rately detected the presence of germinal matrixIVH and parenchymal hemorrhage confirmed byMRI (positive predictive values of 08 085 and 096respectively) However in this study and others4950
white matter injury detected by MRI was less wellpredicted by US (sensitivity of 056ndash089) Addi-tional information provided by MRI included depic-tion of hemorrhagic lesions in 64 of infants andmore numerous or extensive cysts in infants with
Table 2 Incidence and timing of ultrasound abnormalities in preterm infants
Referenceno Class Inclusion criteria
USabnormalitiesincidence ()
Major abnormalitiesincidence ()
No () ofmajor
abnormalities
Incidence of majorabnormalities by
GA or BW
Timing of majorabnormalitiesincidence ()
41 II BW 1500 g GA34 wk
IVH 50250 (20) Grades 3 and 4 IVH13250 (5)
13 (5) GA of 25 wk 957(16) GA of 25wk 4193 (2)
42 II BW 1500 g 33wk
IVH andor PVL245338 (43)
Grades 3 and 4 IVHandor cystic PVL75338 (22)
75 (22) d 1ndash3 2775 (36)d 4ndash7 3675 (48)d 8ndash14 1275 (16)
43 II BW 1500 g PVL 14115 (12) BW of 1000 g1246 (26)
wk 1 614 (43)wk 3ndash15 814 (57)
25 II GA 32 wk BW1500 g or GA37 wk withventilator
IVH 106800(13)
Grades 2ndash4 IVH51800 (6)
51 (6) GA of 30 wk 46364 (13) GA of30 wk 5436 (1)
27 II GA 33 wk PVL 26172 (15) wk 1 1926 (73)wk 2ndash7 726 (27)
44 II GA 36 wk PVL 1153 (21) wk 1 1011 (91)wk 2 111 (9)
28 II BW 1500 g IVH PVL andorVM 161317(51)
Grades 3 and 4 IVHPVL andor VM40317 (13)
40 (126) BW of 1000 g13114 (114) BWof 1000 g 4203 (2)
BW of 1000 gwk 1 (52) wk 2(12) wk 4 (16)term (20)
BW birth weight GA gestational age wk week IVH intraventricular hemorrhage PVL periventricular leukomalacia VM ventriculomegalyd day
June (2 of 2) 2002 NEUROLOGY 58 1729
RETIRED
RETIRED
PVL diagnosed by US50 To date there has not beencorrelation with neurodevelopmental follow-up
Conclusions Compared with US performed onthe same day MRI of PT neonates detects morewhite matter abnormalities in the first week of lifemore hemorrhagic lesions and more numerous orextensive cysts There are insufficient data fromfollow-up studies to indicate whether these addi-tional findings provide more information about theneurodevelopmental prognosis
Recommendation (level C) Currently availabledata from class II studies do not provide sufficientevidence that routine MRI should be performed onall VLBW PT infants for whom results of screeningcranial US are abnormal
What is the ability of neonatal cranial US to pre-dict long-term neurodevelopmental outcome forVLBW PT infants Evidence VLBW PT infantsare at high risk for neurodevelopmental handicapDepending on the GA of the cohort and the year ofbirth the previously reported incidence of mentalretardation andor CP among PT infants rangedfrom 7 to almost 50145152 Further the timing ofcranial US used to predict outcome in the reportedliterature varied from the first 2 weeks of lifethrough term For this reason the lesions reportedand the predictive values for these lesions were diffi-cult to compare Finally in several studies childrendeemed excessively impaired were omitted from thefollow-up assessments and in many the outcomemeasures were reported in broad categories There-fore it was difficult to assess the nature of CP ormental retardation across cohorts
Only reports containing the following data wereincluded GA andor BW of the study populationpostmenstrual age of the ldquopredictorrdquo US when re-corded neurodevelopmental follow-up rate age atassessment and outcome variables
The six class II studies3453-57 (see the electronicversion of this article for table 8 at wwwneurologyorg) compared US findings with the incidence of CPfor almost 2250 VLBW PT children at ages 2 to 9years Significant associations between grade 4 IVHPVL andor ventriculomegaly and CP were noted inall six studies In the largest of these studies58 bothgrade 4 IVH and PVL were associated with CP (oddsratio [OR] 154 95 CI 76ndash311) any grade IVHalone was also associated with CP (OR 314 95 CI15ndash65) Similar data were available from one classIII study and three class IV studies (see the elec-tronic version of this article for table 8 atwwwneurologyorg)59-62
When the same groups from class II and class IIIstudies53-5557-596364 assessed the correlation of neona-tal US findings with the developmental quotientgrade 4 IVH and moderate to severe ventriculo-megaly were strongly associated with the risk ofmental retardation at 2 to 9 years of age (see theelectronic version of this article for table 8 at wwwneurologyorg) In these prospective studies OR
ranged from 997 to 190 In addition Whitaker etal65 demonstrated that for infants with BW of 500 to2000 grams who had grade 4 IVH andor moderateto severe ventriculomegaly the OR for the develop-ment of any neuropsychiatric disorder at the age 6years was 44
Conclusions Grades 3 and 4 IVH cystic PVLand moderate to severe ventriculomegaly determinedby US have all been shown to be significantly associ-ated with CP at 2 to 9 years of age in VLBW PTinfants (class II evidence) In addition class II evi-dence grade 4 IVH and ventriculomegaly have beensignificantly associated with mental retardation andneuropsychiatric disorders at the same time pointsThe OR which vary depending on the populationunder study the lesion and the outcome measureall indicate at least a 10-fold elevation in the risk ofadverse outcome for VLBW PT infants with US evi-dence of grades 3 and 4 IVH cystic PVL and moder-ate to severe ventriculomegaly
Recommendation (level A) For VLBW PT in-fants US should be used to predict long-term neuro-developmental outcome The findings of grades 3 and4 IVH periventricular cystic lesions and moderateto severe ventriculomegaly are all associated withadverse outcome
Term infants with neonatal encephalopathyClinical examination of the term infant with signsand symptoms of neonatal encephalopathy is oftenunable to determine the severity or extent of cerebraldamage and frequently provides little informationregarding the etiology of the insult Although numer-ous reports suggest that hypoxicndashischemic encepha-lopathy (HIE) is a common cause of neonatalencephalopathy the differential diagnosis of thiscondition is extensive including a spectrum of ab-normalities ranging from infectious to metabolic ab-normalities and congenital malformations6667 Evenin those infants with documented HIE the clinicalpresentation may vary widely68 Of those neonateswith moderate to severe HIE almost one-quarterhave mental retardation seizures and CP andpromising intervention strategies are now becomingavailable69-71 Therefore for diagnostic and prognos-tic reasons early assessment and diagnosis of in-fants with neonatal encephalopathy is important
For the definition of neonatal encephalopathy thecommittee used the criteria set forth by the Ameri-can Academy of Pediatrics and the American Collegeof Obstetricians and Gynecologists in Guidelines forPrenatal Care72 For results of a study to be rated asclass I evidence infants described therein must meetall of the following conditions
1 Profound metabolic or mixed acidemia (pH 700[umbilical cord artery blood sample if obtained])
2 Apgar score of 0 to 3 for 5 minutes3 Neonatal neurologic manifestations (eg seizures
coma or hypotonia)4 Multisystem organ dysfunction (eg cardiovascu-
1730 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
lar gastrointestinal hematologic pulmonary orrenal system)
Although these criteria were originally developedfor those infants thought to have HIE they also de-scribe any infant who requires immediate neonatalevaluationmdashboth to determine the underlying causeof encephalopathy and to provide therapeutic inter-ventions when available677374 Studies in which theentry criteria of the infants evaluated were less rig-orously defined received lower classification levelsthan did those in which infants met these conditions
Which neonatal neuroimaging strategies can detectcerebral abnormalities that may affect the immediateand long-term management of the infant with neona-tal encephalopathy Evidence One study dis-cussed gray-scale US of the infant with neonatalencephalopathy75 A second study compared findings ofgray-scale US and Doppler US with outcome76 and athird study compared results of gray-scale US andDoppler US with somatosensory evoked potentials vi-sual evoked potentials and results of the cerebral func-tion monitoring77 A fourth study compared findings ofgray-scale US Doppler US and CT78 Three otherstudies compared results of gray-scale US and MRI forinfants with neonatal encephalopathy79-81 Four studiesreported CT findings for these infants82-85
Gray-scale US Doppler US and studies compar-ing US with CT andor MRI In one class IIIstudy75 (see the electronic version of this article fortable 9 at wwwneurologyorg) US was performed on104 encephalopathic term neonates and 70 controlterm neonates on the first postnatal day A diffuseincrease in echogenicity of the cerebral parenchymaand slit-like ventricles were significantly more com-mon in infants with encephalopathy than in controls(39 versus 1 [p 0001] and 44 versus 9 [p 000l] respectively) but the investigators found nocorrelation between US findings on the first postna-tal day and neurodevelopmental status at 1 year ofage Similar results were noted in a class II studyevaluating term infants with neonatal encephalopa-thy on the first postnatal day76
In the same class II study76 analysis of simulta-neous Doppler US demonstrated resistive indices (re-sistive index peak systolic velocity minus enddiastolic velocity divided by peak systolic velocity) of060 for all children with adverse neurodevelop-mental outcome In another class II study78 gray-scale US Doppler US and CT were performed oninfants with neonatal encephalopathy (see the elec-tronic version of this article for table 9 at wwwneurologyorg) Gray-scale US was not predictive ofoutcome but a resistive index of 05 in the middlecerebral artery was associated with adverse neurode-velopmental outcome at 1 to 2 years (sensitivity82 specificity 89) In addition CT demonstrat-ing generalized decreased density had 91 sensitiv-ity and 100 specificity for adverse outcomes
Three studies compared early US and MRI studiesfor infants with neonatal encephalopathy (see the
electronic version of this article for table 9 atwwwneurologyorg)79-81 An abnormal MRI signal inthe basal ganglia in association with an abnormalUS result for the basal ganglia was most frequentlyassociated with an adverse neurodevelopmental out-come including CP seizures and developmental de-lay at 1 year of age while normal findings of US andCT or US and MRI had low negative predictivevalues
Conclusions Seven studies (classes II and III)assessed the role of gray-scale US in the diagnosis ofterm infants with neonatal encephalopathy Al-though gray-scale US can be easily performed at thebedside there are little data to support the use ofthis modality in imaging of the encephalopathic termneonate However two class II studies of Doppler USsuggested that resistive indices of 05ndash06 are con-sistent with the diagnosis of HIE
CT studies CT can be performed rapidly andwithout sedation of the neonate Four studies usedCT to evaluate term infants with neonatal encepha-lopathy One study84 reported basal ganglia changesa second study82 reported both basal ganglia and tha-lamic changes Two studies8385 used CT to detect in-tracranial hemorrhages in infants with signs andsymptoms of neonatal encephalopathy who also hadlow hematocrit or evidence of coagulopathy in bothstudies detection of intracranial hemorrhages al-tered clinical care
Conclusions One class II study and three classIV studies assessed the value of CT for encephalo-pathic term neonates Two studies suggested thatlow attenuation in the basal ganglia andor thalamiindicates severe injury consistent with HIE Theother two studies demonstrated that CT plays a rolein the detection of hemorrhagic lesions
MRI studies Two studies (see the electronic ver-sion of this article for table 9 at wwwneurologyorg)compared MRI findings with neuropathologic datafor infants with neonatal encephalopathy believedattributable to HIE8687 In the larger study87 imag-ing data were compared with results of neuropatho-logic analyses of the posterior limb of the internalcapsule thalamus parietal cortex hippocampusand medulla The posterior limb of the internal cap-sule was the most reliable region analyzed andagreement of MRI findings was similar to thatachieved by two pathologists reviewing the histologicsections ( 066) In this study the MRI abnormal-ity was predictive of the pathologic abnormality witha sensitivity of 070 and a positive predictive value of10 The predictive value of a single MRI abnormal-ity was 079 (95 CI 061ndash096)
In eight class II studies (see the electronic versionof this article for table 9 at wwwneurologyorg)288-94
conventional T1- and T2-weighted MRI studies wereperformed for a total of 272 term neonates most ofwhom were clinically suspected of having neonatalencephalopathy secondary to hypoxicndashischemic in-jury Scans were obtained at ages ranging from 1 to30 postnatal days and the mean age range was 2 to
June (2 of 2) 2002 NEUROLOGY 58 1731
RETIRED
RETIRED
8 days Three patterns of injury were detected byMRI 1) injury to the thalami andor posteriorndashlateral putamen with involvement of the subcorticalwhite matter in the most severe injuries 2) injury tothe parasagittal gray matter and subcortical whitematter posteriorly typically more than anteriorlyand 3) focal or multifocal injury Thalamic and basalganglia damage was the most common abnormalityreported This pattern of injury was detected in al-most 40 of infants and represented over one-half ofall abnormalities (see the electronic version of thisarticle for table 10 at wwwneurologyorg) In oneclass III study95 abnormal T1-weighted imagesshowing hyperintensities in a characteristic distribu-tion were demonstrated as early as 3 days after theinjury abnormal T2-weighted images showing hy-pointensities were demonstrated by 6 to 7 days
Conclusions Results of class II studies indicatethat characteristic MR patterns of cerebral injurycan be detected using conventional T1- and T2-weighted imaging sequences performed at mean agesof 2 to 8 days for encephalopathic term infants
Diffusion weighted imaging Studies of adult ar-terial infarcts have shown that DWI signal changesoccur within minutes of symptom onset and hoursbefore changes become apparent on T1- or T2-weighted images96 In one class II study86 and fourclass III studies97-100 that investigated the use of DWIin the evaluation of term neonates (see the electronicversion of this article for table 11 at wwwneurologyorg) entrance criteria were not stated in enough de-tail to determine which infants met strict criteria foracute neonatal encephalopathy and neonates withfocal seizures were also included MR studies wereperformed a mean of 2 to 4 days after birth and DWIfindings were compared with those of standard MRIsequences Abnormal DWI results were reported fortwo-thirds of infants For 7 to 58 of infants withabnormal DWI findings T2- andor T1-weighted im-ages were also abnormal Abnormal DWI results andnormal T1- andor T2- weighted images typically oc-curred when imaging was performed earlier than day 2of life or when there was diffuse white matter involve-ment Robertson et al99 described one patient for whomall imaging sequences including DWI and T1- and T2-weighted imaging sequences were normal when per-formed at 13 hours despite development of DWI andT1- and T2-weighted imaging abnormalities by 5 daysRobertson et al also described one other patient forwhom DWI results were normal at 8 days when T1-and T2-weighted images were abnormal this de-creased sensitivity of DWI in the subacute to chronicphase has also been noted for the adult populationsuggesting that the maximum sensitivity of DWI isbetween 2 and 8 days
Conclusions Findings of one class II study andfour class III studies suggest that DWI can provideevidence of cerebral injury before conventional MRItechniques for term infants with neonatal encepha-lopathy However DWI results may be negative if it
is performed earlier than 24 hours of life or laterthan 8 days of life
Proton MRS A number of investigators have ex-plored the utility of 1H-MRS and 31P-MRS at fieldstrengths of 15 T but the recommendations forthis parameter will be limited to 1H-MRS at 15 Tbecause this is the equipment most commonly avail-able for neonatal imaging All of the studies thatevaluated 1H-MRS at 15 T used single-voxel pointresolved spectroscopy (PRESS) or stimulate echo ac-quisition mode (STEAM) MRS although mutivoxelchemical shift imaging (CSI) allows high resolutionevaluation of larger regions of tissue there are nodata at this time that assess the role of this modalityin perinatal brain injury
In a number of class II studies (see the electronicversion of this article for table 12 at wwwneurologyorg) echo times of 136 msec and 272 msec were pre-ferred over the shorter echo times of 36 msec becauseof the higher SD of metabolite concentrations mea-sured at these shorter echo times2093 An echo time of136 msec has the additional advantage of an invertedlactate peak making distinction from lipids (which canresonate in the same region) more accurate
One class II study101 used MRS at 15 T within thefirst 18 hours in 31 cases of suspected HIE and in 7matched controls Lactatecreatine ratios rangedfrom 0 to 06 (median 005) for the seven controls Incontrast the investigators demonstrated lactatecreatine ratios of 10 for 10 (32) of the 31 infantswith suspected HIE In three additional class IIstudies93102103 proton MRS of the basal gangliawas performed within the first 2 weeks of life on 77infants with neonatal encephalopathy ElevatedlactateN-acetylaspartate ratios were the most con-sistent findings although elevated lactatecreatineand lactatecholine ratios were also reported for in-fants with suspected neonatal encephalopathy
Conclusions Data from class II studies suggestthat MRS can play an important role in the assess-ment of encephalopathic term infants Lactatecreat-ine ratios of 1 in the first 18 hours are morecommon in those infants with later neurologic find-ings consistent with HIE Elevated lactateNAA lac-tatecreatine and lactatecholine ratios in the first 2postnatal weeks are more common in infants withsuspected neonatal encephalopathy than in age-matched controls
Recommendations for diagnostic assessment1 For infants with a history of neonatal encepha-
lopathy significant birth trauma and evidence forlow hematocrit or coagulopathy
a Noncontrast CT should be performed to look forhemorrhage (level B)
b If the CT findings cannot explain the clinicalstatus of the neonate MRI should be performed (lev-el A)
2 For other neonates with acute encephalopathya MRI should be performed between days 2 and 8
of life (level A)1732 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
RETIRED
PVL diagnosed by US50 To date there has not beencorrelation with neurodevelopmental follow-up
Conclusions Compared with US performed onthe same day MRI of PT neonates detects morewhite matter abnormalities in the first week of lifemore hemorrhagic lesions and more numerous orextensive cysts There are insufficient data fromfollow-up studies to indicate whether these addi-tional findings provide more information about theneurodevelopmental prognosis
Recommendation (level C) Currently availabledata from class II studies do not provide sufficientevidence that routine MRI should be performed onall VLBW PT infants for whom results of screeningcranial US are abnormal
What is the ability of neonatal cranial US to pre-dict long-term neurodevelopmental outcome forVLBW PT infants Evidence VLBW PT infantsare at high risk for neurodevelopmental handicapDepending on the GA of the cohort and the year ofbirth the previously reported incidence of mentalretardation andor CP among PT infants rangedfrom 7 to almost 50145152 Further the timing ofcranial US used to predict outcome in the reportedliterature varied from the first 2 weeks of lifethrough term For this reason the lesions reportedand the predictive values for these lesions were diffi-cult to compare Finally in several studies childrendeemed excessively impaired were omitted from thefollow-up assessments and in many the outcomemeasures were reported in broad categories There-fore it was difficult to assess the nature of CP ormental retardation across cohorts
Only reports containing the following data wereincluded GA andor BW of the study populationpostmenstrual age of the ldquopredictorrdquo US when re-corded neurodevelopmental follow-up rate age atassessment and outcome variables
The six class II studies3453-57 (see the electronicversion of this article for table 8 at wwwneurologyorg) compared US findings with the incidence of CPfor almost 2250 VLBW PT children at ages 2 to 9years Significant associations between grade 4 IVHPVL andor ventriculomegaly and CP were noted inall six studies In the largest of these studies58 bothgrade 4 IVH and PVL were associated with CP (oddsratio [OR] 154 95 CI 76ndash311) any grade IVHalone was also associated with CP (OR 314 95 CI15ndash65) Similar data were available from one classIII study and three class IV studies (see the elec-tronic version of this article for table 8 atwwwneurologyorg)59-62
When the same groups from class II and class IIIstudies53-5557-596364 assessed the correlation of neona-tal US findings with the developmental quotientgrade 4 IVH and moderate to severe ventriculo-megaly were strongly associated with the risk ofmental retardation at 2 to 9 years of age (see theelectronic version of this article for table 8 at wwwneurologyorg) In these prospective studies OR
ranged from 997 to 190 In addition Whitaker etal65 demonstrated that for infants with BW of 500 to2000 grams who had grade 4 IVH andor moderateto severe ventriculomegaly the OR for the develop-ment of any neuropsychiatric disorder at the age 6years was 44
Conclusions Grades 3 and 4 IVH cystic PVLand moderate to severe ventriculomegaly determinedby US have all been shown to be significantly associ-ated with CP at 2 to 9 years of age in VLBW PTinfants (class II evidence) In addition class II evi-dence grade 4 IVH and ventriculomegaly have beensignificantly associated with mental retardation andneuropsychiatric disorders at the same time pointsThe OR which vary depending on the populationunder study the lesion and the outcome measureall indicate at least a 10-fold elevation in the risk ofadverse outcome for VLBW PT infants with US evi-dence of grades 3 and 4 IVH cystic PVL and moder-ate to severe ventriculomegaly
Recommendation (level A) For VLBW PT in-fants US should be used to predict long-term neuro-developmental outcome The findings of grades 3 and4 IVH periventricular cystic lesions and moderateto severe ventriculomegaly are all associated withadverse outcome
Term infants with neonatal encephalopathyClinical examination of the term infant with signsand symptoms of neonatal encephalopathy is oftenunable to determine the severity or extent of cerebraldamage and frequently provides little informationregarding the etiology of the insult Although numer-ous reports suggest that hypoxicndashischemic encepha-lopathy (HIE) is a common cause of neonatalencephalopathy the differential diagnosis of thiscondition is extensive including a spectrum of ab-normalities ranging from infectious to metabolic ab-normalities and congenital malformations6667 Evenin those infants with documented HIE the clinicalpresentation may vary widely68 Of those neonateswith moderate to severe HIE almost one-quarterhave mental retardation seizures and CP andpromising intervention strategies are now becomingavailable69-71 Therefore for diagnostic and prognos-tic reasons early assessment and diagnosis of in-fants with neonatal encephalopathy is important
For the definition of neonatal encephalopathy thecommittee used the criteria set forth by the Ameri-can Academy of Pediatrics and the American Collegeof Obstetricians and Gynecologists in Guidelines forPrenatal Care72 For results of a study to be rated asclass I evidence infants described therein must meetall of the following conditions
1 Profound metabolic or mixed acidemia (pH 700[umbilical cord artery blood sample if obtained])
2 Apgar score of 0 to 3 for 5 minutes3 Neonatal neurologic manifestations (eg seizures
coma or hypotonia)4 Multisystem organ dysfunction (eg cardiovascu-
1730 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
lar gastrointestinal hematologic pulmonary orrenal system)
Although these criteria were originally developedfor those infants thought to have HIE they also de-scribe any infant who requires immediate neonatalevaluationmdashboth to determine the underlying causeof encephalopathy and to provide therapeutic inter-ventions when available677374 Studies in which theentry criteria of the infants evaluated were less rig-orously defined received lower classification levelsthan did those in which infants met these conditions
Which neonatal neuroimaging strategies can detectcerebral abnormalities that may affect the immediateand long-term management of the infant with neona-tal encephalopathy Evidence One study dis-cussed gray-scale US of the infant with neonatalencephalopathy75 A second study compared findings ofgray-scale US and Doppler US with outcome76 and athird study compared results of gray-scale US andDoppler US with somatosensory evoked potentials vi-sual evoked potentials and results of the cerebral func-tion monitoring77 A fourth study compared findings ofgray-scale US Doppler US and CT78 Three otherstudies compared results of gray-scale US and MRI forinfants with neonatal encephalopathy79-81 Four studiesreported CT findings for these infants82-85
Gray-scale US Doppler US and studies compar-ing US with CT andor MRI In one class IIIstudy75 (see the electronic version of this article fortable 9 at wwwneurologyorg) US was performed on104 encephalopathic term neonates and 70 controlterm neonates on the first postnatal day A diffuseincrease in echogenicity of the cerebral parenchymaand slit-like ventricles were significantly more com-mon in infants with encephalopathy than in controls(39 versus 1 [p 0001] and 44 versus 9 [p 000l] respectively) but the investigators found nocorrelation between US findings on the first postna-tal day and neurodevelopmental status at 1 year ofage Similar results were noted in a class II studyevaluating term infants with neonatal encephalopa-thy on the first postnatal day76
In the same class II study76 analysis of simulta-neous Doppler US demonstrated resistive indices (re-sistive index peak systolic velocity minus enddiastolic velocity divided by peak systolic velocity) of060 for all children with adverse neurodevelop-mental outcome In another class II study78 gray-scale US Doppler US and CT were performed oninfants with neonatal encephalopathy (see the elec-tronic version of this article for table 9 at wwwneurologyorg) Gray-scale US was not predictive ofoutcome but a resistive index of 05 in the middlecerebral artery was associated with adverse neurode-velopmental outcome at 1 to 2 years (sensitivity82 specificity 89) In addition CT demonstrat-ing generalized decreased density had 91 sensitiv-ity and 100 specificity for adverse outcomes
Three studies compared early US and MRI studiesfor infants with neonatal encephalopathy (see the
electronic version of this article for table 9 atwwwneurologyorg)79-81 An abnormal MRI signal inthe basal ganglia in association with an abnormalUS result for the basal ganglia was most frequentlyassociated with an adverse neurodevelopmental out-come including CP seizures and developmental de-lay at 1 year of age while normal findings of US andCT or US and MRI had low negative predictivevalues
Conclusions Seven studies (classes II and III)assessed the role of gray-scale US in the diagnosis ofterm infants with neonatal encephalopathy Al-though gray-scale US can be easily performed at thebedside there are little data to support the use ofthis modality in imaging of the encephalopathic termneonate However two class II studies of Doppler USsuggested that resistive indices of 05ndash06 are con-sistent with the diagnosis of HIE
CT studies CT can be performed rapidly andwithout sedation of the neonate Four studies usedCT to evaluate term infants with neonatal encepha-lopathy One study84 reported basal ganglia changesa second study82 reported both basal ganglia and tha-lamic changes Two studies8385 used CT to detect in-tracranial hemorrhages in infants with signs andsymptoms of neonatal encephalopathy who also hadlow hematocrit or evidence of coagulopathy in bothstudies detection of intracranial hemorrhages al-tered clinical care
Conclusions One class II study and three classIV studies assessed the value of CT for encephalo-pathic term neonates Two studies suggested thatlow attenuation in the basal ganglia andor thalamiindicates severe injury consistent with HIE Theother two studies demonstrated that CT plays a rolein the detection of hemorrhagic lesions
MRI studies Two studies (see the electronic ver-sion of this article for table 9 at wwwneurologyorg)compared MRI findings with neuropathologic datafor infants with neonatal encephalopathy believedattributable to HIE8687 In the larger study87 imag-ing data were compared with results of neuropatho-logic analyses of the posterior limb of the internalcapsule thalamus parietal cortex hippocampusand medulla The posterior limb of the internal cap-sule was the most reliable region analyzed andagreement of MRI findings was similar to thatachieved by two pathologists reviewing the histologicsections ( 066) In this study the MRI abnormal-ity was predictive of the pathologic abnormality witha sensitivity of 070 and a positive predictive value of10 The predictive value of a single MRI abnormal-ity was 079 (95 CI 061ndash096)
In eight class II studies (see the electronic versionof this article for table 9 at wwwneurologyorg)288-94
conventional T1- and T2-weighted MRI studies wereperformed for a total of 272 term neonates most ofwhom were clinically suspected of having neonatalencephalopathy secondary to hypoxicndashischemic in-jury Scans were obtained at ages ranging from 1 to30 postnatal days and the mean age range was 2 to
June (2 of 2) 2002 NEUROLOGY 58 1731
RETIRED
RETIRED
8 days Three patterns of injury were detected byMRI 1) injury to the thalami andor posteriorndashlateral putamen with involvement of the subcorticalwhite matter in the most severe injuries 2) injury tothe parasagittal gray matter and subcortical whitematter posteriorly typically more than anteriorlyand 3) focal or multifocal injury Thalamic and basalganglia damage was the most common abnormalityreported This pattern of injury was detected in al-most 40 of infants and represented over one-half ofall abnormalities (see the electronic version of thisarticle for table 10 at wwwneurologyorg) In oneclass III study95 abnormal T1-weighted imagesshowing hyperintensities in a characteristic distribu-tion were demonstrated as early as 3 days after theinjury abnormal T2-weighted images showing hy-pointensities were demonstrated by 6 to 7 days
Conclusions Results of class II studies indicatethat characteristic MR patterns of cerebral injurycan be detected using conventional T1- and T2-weighted imaging sequences performed at mean agesof 2 to 8 days for encephalopathic term infants
Diffusion weighted imaging Studies of adult ar-terial infarcts have shown that DWI signal changesoccur within minutes of symptom onset and hoursbefore changes become apparent on T1- or T2-weighted images96 In one class II study86 and fourclass III studies97-100 that investigated the use of DWIin the evaluation of term neonates (see the electronicversion of this article for table 11 at wwwneurologyorg) entrance criteria were not stated in enough de-tail to determine which infants met strict criteria foracute neonatal encephalopathy and neonates withfocal seizures were also included MR studies wereperformed a mean of 2 to 4 days after birth and DWIfindings were compared with those of standard MRIsequences Abnormal DWI results were reported fortwo-thirds of infants For 7 to 58 of infants withabnormal DWI findings T2- andor T1-weighted im-ages were also abnormal Abnormal DWI results andnormal T1- andor T2- weighted images typically oc-curred when imaging was performed earlier than day 2of life or when there was diffuse white matter involve-ment Robertson et al99 described one patient for whomall imaging sequences including DWI and T1- and T2-weighted imaging sequences were normal when per-formed at 13 hours despite development of DWI andT1- and T2-weighted imaging abnormalities by 5 daysRobertson et al also described one other patient forwhom DWI results were normal at 8 days when T1-and T2-weighted images were abnormal this de-creased sensitivity of DWI in the subacute to chronicphase has also been noted for the adult populationsuggesting that the maximum sensitivity of DWI isbetween 2 and 8 days
Conclusions Findings of one class II study andfour class III studies suggest that DWI can provideevidence of cerebral injury before conventional MRItechniques for term infants with neonatal encepha-lopathy However DWI results may be negative if it
is performed earlier than 24 hours of life or laterthan 8 days of life
Proton MRS A number of investigators have ex-plored the utility of 1H-MRS and 31P-MRS at fieldstrengths of 15 T but the recommendations forthis parameter will be limited to 1H-MRS at 15 Tbecause this is the equipment most commonly avail-able for neonatal imaging All of the studies thatevaluated 1H-MRS at 15 T used single-voxel pointresolved spectroscopy (PRESS) or stimulate echo ac-quisition mode (STEAM) MRS although mutivoxelchemical shift imaging (CSI) allows high resolutionevaluation of larger regions of tissue there are nodata at this time that assess the role of this modalityin perinatal brain injury
In a number of class II studies (see the electronicversion of this article for table 12 at wwwneurologyorg) echo times of 136 msec and 272 msec were pre-ferred over the shorter echo times of 36 msec becauseof the higher SD of metabolite concentrations mea-sured at these shorter echo times2093 An echo time of136 msec has the additional advantage of an invertedlactate peak making distinction from lipids (which canresonate in the same region) more accurate
One class II study101 used MRS at 15 T within thefirst 18 hours in 31 cases of suspected HIE and in 7matched controls Lactatecreatine ratios rangedfrom 0 to 06 (median 005) for the seven controls Incontrast the investigators demonstrated lactatecreatine ratios of 10 for 10 (32) of the 31 infantswith suspected HIE In three additional class IIstudies93102103 proton MRS of the basal gangliawas performed within the first 2 weeks of life on 77infants with neonatal encephalopathy ElevatedlactateN-acetylaspartate ratios were the most con-sistent findings although elevated lactatecreatineand lactatecholine ratios were also reported for in-fants with suspected neonatal encephalopathy
Conclusions Data from class II studies suggestthat MRS can play an important role in the assess-ment of encephalopathic term infants Lactatecreat-ine ratios of 1 in the first 18 hours are morecommon in those infants with later neurologic find-ings consistent with HIE Elevated lactateNAA lac-tatecreatine and lactatecholine ratios in the first 2postnatal weeks are more common in infants withsuspected neonatal encephalopathy than in age-matched controls
Recommendations for diagnostic assessment1 For infants with a history of neonatal encepha-
lopathy significant birth trauma and evidence forlow hematocrit or coagulopathy
a Noncontrast CT should be performed to look forhemorrhage (level B)
b If the CT findings cannot explain the clinicalstatus of the neonate MRI should be performed (lev-el A)
2 For other neonates with acute encephalopathya MRI should be performed between days 2 and 8
of life (level A)1732 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
RETIRED
lar gastrointestinal hematologic pulmonary orrenal system)
Although these criteria were originally developedfor those infants thought to have HIE they also de-scribe any infant who requires immediate neonatalevaluationmdashboth to determine the underlying causeof encephalopathy and to provide therapeutic inter-ventions when available677374 Studies in which theentry criteria of the infants evaluated were less rig-orously defined received lower classification levelsthan did those in which infants met these conditions
Which neonatal neuroimaging strategies can detectcerebral abnormalities that may affect the immediateand long-term management of the infant with neona-tal encephalopathy Evidence One study dis-cussed gray-scale US of the infant with neonatalencephalopathy75 A second study compared findings ofgray-scale US and Doppler US with outcome76 and athird study compared results of gray-scale US andDoppler US with somatosensory evoked potentials vi-sual evoked potentials and results of the cerebral func-tion monitoring77 A fourth study compared findings ofgray-scale US Doppler US and CT78 Three otherstudies compared results of gray-scale US and MRI forinfants with neonatal encephalopathy79-81 Four studiesreported CT findings for these infants82-85
Gray-scale US Doppler US and studies compar-ing US with CT andor MRI In one class IIIstudy75 (see the electronic version of this article fortable 9 at wwwneurologyorg) US was performed on104 encephalopathic term neonates and 70 controlterm neonates on the first postnatal day A diffuseincrease in echogenicity of the cerebral parenchymaand slit-like ventricles were significantly more com-mon in infants with encephalopathy than in controls(39 versus 1 [p 0001] and 44 versus 9 [p 000l] respectively) but the investigators found nocorrelation between US findings on the first postna-tal day and neurodevelopmental status at 1 year ofage Similar results were noted in a class II studyevaluating term infants with neonatal encephalopa-thy on the first postnatal day76
In the same class II study76 analysis of simulta-neous Doppler US demonstrated resistive indices (re-sistive index peak systolic velocity minus enddiastolic velocity divided by peak systolic velocity) of060 for all children with adverse neurodevelop-mental outcome In another class II study78 gray-scale US Doppler US and CT were performed oninfants with neonatal encephalopathy (see the elec-tronic version of this article for table 9 at wwwneurologyorg) Gray-scale US was not predictive ofoutcome but a resistive index of 05 in the middlecerebral artery was associated with adverse neurode-velopmental outcome at 1 to 2 years (sensitivity82 specificity 89) In addition CT demonstrat-ing generalized decreased density had 91 sensitiv-ity and 100 specificity for adverse outcomes
Three studies compared early US and MRI studiesfor infants with neonatal encephalopathy (see the
electronic version of this article for table 9 atwwwneurologyorg)79-81 An abnormal MRI signal inthe basal ganglia in association with an abnormalUS result for the basal ganglia was most frequentlyassociated with an adverse neurodevelopmental out-come including CP seizures and developmental de-lay at 1 year of age while normal findings of US andCT or US and MRI had low negative predictivevalues
Conclusions Seven studies (classes II and III)assessed the role of gray-scale US in the diagnosis ofterm infants with neonatal encephalopathy Al-though gray-scale US can be easily performed at thebedside there are little data to support the use ofthis modality in imaging of the encephalopathic termneonate However two class II studies of Doppler USsuggested that resistive indices of 05ndash06 are con-sistent with the diagnosis of HIE
CT studies CT can be performed rapidly andwithout sedation of the neonate Four studies usedCT to evaluate term infants with neonatal encepha-lopathy One study84 reported basal ganglia changesa second study82 reported both basal ganglia and tha-lamic changes Two studies8385 used CT to detect in-tracranial hemorrhages in infants with signs andsymptoms of neonatal encephalopathy who also hadlow hematocrit or evidence of coagulopathy in bothstudies detection of intracranial hemorrhages al-tered clinical care
Conclusions One class II study and three classIV studies assessed the value of CT for encephalo-pathic term neonates Two studies suggested thatlow attenuation in the basal ganglia andor thalamiindicates severe injury consistent with HIE Theother two studies demonstrated that CT plays a rolein the detection of hemorrhagic lesions
MRI studies Two studies (see the electronic ver-sion of this article for table 9 at wwwneurologyorg)compared MRI findings with neuropathologic datafor infants with neonatal encephalopathy believedattributable to HIE8687 In the larger study87 imag-ing data were compared with results of neuropatho-logic analyses of the posterior limb of the internalcapsule thalamus parietal cortex hippocampusand medulla The posterior limb of the internal cap-sule was the most reliable region analyzed andagreement of MRI findings was similar to thatachieved by two pathologists reviewing the histologicsections ( 066) In this study the MRI abnormal-ity was predictive of the pathologic abnormality witha sensitivity of 070 and a positive predictive value of10 The predictive value of a single MRI abnormal-ity was 079 (95 CI 061ndash096)
In eight class II studies (see the electronic versionof this article for table 9 at wwwneurologyorg)288-94
conventional T1- and T2-weighted MRI studies wereperformed for a total of 272 term neonates most ofwhom were clinically suspected of having neonatalencephalopathy secondary to hypoxicndashischemic in-jury Scans were obtained at ages ranging from 1 to30 postnatal days and the mean age range was 2 to
June (2 of 2) 2002 NEUROLOGY 58 1731
RETIRED
RETIRED
8 days Three patterns of injury were detected byMRI 1) injury to the thalami andor posteriorndashlateral putamen with involvement of the subcorticalwhite matter in the most severe injuries 2) injury tothe parasagittal gray matter and subcortical whitematter posteriorly typically more than anteriorlyand 3) focal or multifocal injury Thalamic and basalganglia damage was the most common abnormalityreported This pattern of injury was detected in al-most 40 of infants and represented over one-half ofall abnormalities (see the electronic version of thisarticle for table 10 at wwwneurologyorg) In oneclass III study95 abnormal T1-weighted imagesshowing hyperintensities in a characteristic distribu-tion were demonstrated as early as 3 days after theinjury abnormal T2-weighted images showing hy-pointensities were demonstrated by 6 to 7 days
Conclusions Results of class II studies indicatethat characteristic MR patterns of cerebral injurycan be detected using conventional T1- and T2-weighted imaging sequences performed at mean agesof 2 to 8 days for encephalopathic term infants
Diffusion weighted imaging Studies of adult ar-terial infarcts have shown that DWI signal changesoccur within minutes of symptom onset and hoursbefore changes become apparent on T1- or T2-weighted images96 In one class II study86 and fourclass III studies97-100 that investigated the use of DWIin the evaluation of term neonates (see the electronicversion of this article for table 11 at wwwneurologyorg) entrance criteria were not stated in enough de-tail to determine which infants met strict criteria foracute neonatal encephalopathy and neonates withfocal seizures were also included MR studies wereperformed a mean of 2 to 4 days after birth and DWIfindings were compared with those of standard MRIsequences Abnormal DWI results were reported fortwo-thirds of infants For 7 to 58 of infants withabnormal DWI findings T2- andor T1-weighted im-ages were also abnormal Abnormal DWI results andnormal T1- andor T2- weighted images typically oc-curred when imaging was performed earlier than day 2of life or when there was diffuse white matter involve-ment Robertson et al99 described one patient for whomall imaging sequences including DWI and T1- and T2-weighted imaging sequences were normal when per-formed at 13 hours despite development of DWI andT1- and T2-weighted imaging abnormalities by 5 daysRobertson et al also described one other patient forwhom DWI results were normal at 8 days when T1-and T2-weighted images were abnormal this de-creased sensitivity of DWI in the subacute to chronicphase has also been noted for the adult populationsuggesting that the maximum sensitivity of DWI isbetween 2 and 8 days
Conclusions Findings of one class II study andfour class III studies suggest that DWI can provideevidence of cerebral injury before conventional MRItechniques for term infants with neonatal encepha-lopathy However DWI results may be negative if it
is performed earlier than 24 hours of life or laterthan 8 days of life
Proton MRS A number of investigators have ex-plored the utility of 1H-MRS and 31P-MRS at fieldstrengths of 15 T but the recommendations forthis parameter will be limited to 1H-MRS at 15 Tbecause this is the equipment most commonly avail-able for neonatal imaging All of the studies thatevaluated 1H-MRS at 15 T used single-voxel pointresolved spectroscopy (PRESS) or stimulate echo ac-quisition mode (STEAM) MRS although mutivoxelchemical shift imaging (CSI) allows high resolutionevaluation of larger regions of tissue there are nodata at this time that assess the role of this modalityin perinatal brain injury
In a number of class II studies (see the electronicversion of this article for table 12 at wwwneurologyorg) echo times of 136 msec and 272 msec were pre-ferred over the shorter echo times of 36 msec becauseof the higher SD of metabolite concentrations mea-sured at these shorter echo times2093 An echo time of136 msec has the additional advantage of an invertedlactate peak making distinction from lipids (which canresonate in the same region) more accurate
One class II study101 used MRS at 15 T within thefirst 18 hours in 31 cases of suspected HIE and in 7matched controls Lactatecreatine ratios rangedfrom 0 to 06 (median 005) for the seven controls Incontrast the investigators demonstrated lactatecreatine ratios of 10 for 10 (32) of the 31 infantswith suspected HIE In three additional class IIstudies93102103 proton MRS of the basal gangliawas performed within the first 2 weeks of life on 77infants with neonatal encephalopathy ElevatedlactateN-acetylaspartate ratios were the most con-sistent findings although elevated lactatecreatineand lactatecholine ratios were also reported for in-fants with suspected neonatal encephalopathy
Conclusions Data from class II studies suggestthat MRS can play an important role in the assess-ment of encephalopathic term infants Lactatecreat-ine ratios of 1 in the first 18 hours are morecommon in those infants with later neurologic find-ings consistent with HIE Elevated lactateNAA lac-tatecreatine and lactatecholine ratios in the first 2postnatal weeks are more common in infants withsuspected neonatal encephalopathy than in age-matched controls
Recommendations for diagnostic assessment1 For infants with a history of neonatal encepha-
lopathy significant birth trauma and evidence forlow hematocrit or coagulopathy
a Noncontrast CT should be performed to look forhemorrhage (level B)
b If the CT findings cannot explain the clinicalstatus of the neonate MRI should be performed (lev-el A)
2 For other neonates with acute encephalopathya MRI should be performed between days 2 and 8
of life (level A)1732 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

RETIRED
8 days Three patterns of injury were detected byMRI 1) injury to the thalami andor posteriorndashlateral putamen with involvement of the subcorticalwhite matter in the most severe injuries 2) injury tothe parasagittal gray matter and subcortical whitematter posteriorly typically more than anteriorlyand 3) focal or multifocal injury Thalamic and basalganglia damage was the most common abnormalityreported This pattern of injury was detected in al-most 40 of infants and represented over one-half ofall abnormalities (see the electronic version of thisarticle for table 10 at wwwneurologyorg) In oneclass III study95 abnormal T1-weighted imagesshowing hyperintensities in a characteristic distribu-tion were demonstrated as early as 3 days after theinjury abnormal T2-weighted images showing hy-pointensities were demonstrated by 6 to 7 days
Conclusions Results of class II studies indicatethat characteristic MR patterns of cerebral injurycan be detected using conventional T1- and T2-weighted imaging sequences performed at mean agesof 2 to 8 days for encephalopathic term infants
Diffusion weighted imaging Studies of adult ar-terial infarcts have shown that DWI signal changesoccur within minutes of symptom onset and hoursbefore changes become apparent on T1- or T2-weighted images96 In one class II study86 and fourclass III studies97-100 that investigated the use of DWIin the evaluation of term neonates (see the electronicversion of this article for table 11 at wwwneurologyorg) entrance criteria were not stated in enough de-tail to determine which infants met strict criteria foracute neonatal encephalopathy and neonates withfocal seizures were also included MR studies wereperformed a mean of 2 to 4 days after birth and DWIfindings were compared with those of standard MRIsequences Abnormal DWI results were reported fortwo-thirds of infants For 7 to 58 of infants withabnormal DWI findings T2- andor T1-weighted im-ages were also abnormal Abnormal DWI results andnormal T1- andor T2- weighted images typically oc-curred when imaging was performed earlier than day 2of life or when there was diffuse white matter involve-ment Robertson et al99 described one patient for whomall imaging sequences including DWI and T1- and T2-weighted imaging sequences were normal when per-formed at 13 hours despite development of DWI andT1- and T2-weighted imaging abnormalities by 5 daysRobertson et al also described one other patient forwhom DWI results were normal at 8 days when T1-and T2-weighted images were abnormal this de-creased sensitivity of DWI in the subacute to chronicphase has also been noted for the adult populationsuggesting that the maximum sensitivity of DWI isbetween 2 and 8 days
Conclusions Findings of one class II study andfour class III studies suggest that DWI can provideevidence of cerebral injury before conventional MRItechniques for term infants with neonatal encepha-lopathy However DWI results may be negative if it
is performed earlier than 24 hours of life or laterthan 8 days of life
Proton MRS A number of investigators have ex-plored the utility of 1H-MRS and 31P-MRS at fieldstrengths of 15 T but the recommendations forthis parameter will be limited to 1H-MRS at 15 Tbecause this is the equipment most commonly avail-able for neonatal imaging All of the studies thatevaluated 1H-MRS at 15 T used single-voxel pointresolved spectroscopy (PRESS) or stimulate echo ac-quisition mode (STEAM) MRS although mutivoxelchemical shift imaging (CSI) allows high resolutionevaluation of larger regions of tissue there are nodata at this time that assess the role of this modalityin perinatal brain injury
In a number of class II studies (see the electronicversion of this article for table 12 at wwwneurologyorg) echo times of 136 msec and 272 msec were pre-ferred over the shorter echo times of 36 msec becauseof the higher SD of metabolite concentrations mea-sured at these shorter echo times2093 An echo time of136 msec has the additional advantage of an invertedlactate peak making distinction from lipids (which canresonate in the same region) more accurate
One class II study101 used MRS at 15 T within thefirst 18 hours in 31 cases of suspected HIE and in 7matched controls Lactatecreatine ratios rangedfrom 0 to 06 (median 005) for the seven controls Incontrast the investigators demonstrated lactatecreatine ratios of 10 for 10 (32) of the 31 infantswith suspected HIE In three additional class IIstudies93102103 proton MRS of the basal gangliawas performed within the first 2 weeks of life on 77infants with neonatal encephalopathy ElevatedlactateN-acetylaspartate ratios were the most con-sistent findings although elevated lactatecreatineand lactatecholine ratios were also reported for in-fants with suspected neonatal encephalopathy
Conclusions Data from class II studies suggestthat MRS can play an important role in the assess-ment of encephalopathic term infants Lactatecreat-ine ratios of 1 in the first 18 hours are morecommon in those infants with later neurologic find-ings consistent with HIE Elevated lactateNAA lac-tatecreatine and lactatecholine ratios in the first 2postnatal weeks are more common in infants withsuspected neonatal encephalopathy than in age-matched controls
Recommendations for diagnostic assessment1 For infants with a history of neonatal encepha-
lopathy significant birth trauma and evidence forlow hematocrit or coagulopathy
a Noncontrast CT should be performed to look forhemorrhage (level B)
b If the CT findings cannot explain the clinicalstatus of the neonate MRI should be performed (lev-el A)
2 For other neonates with acute encephalopathya MRI should be performed between days 2 and 8
of life (level A)1732 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

RETIRED
b If single-voxel MRS is available MRI shouldinclude MRS (level B)
c At the time of MRI DWI should also be per-formed if this modality is available (level C)
d CT should be performed only if MRI is notavailable or if the neonate is too unstable for MRI(level A)
Can MRI provide prognostic data for term infantswith neonatal encephalopathy Evidence Eightclass II studies (table 3 see the electronic version ofthis article for table 9 at wwwneurologyorg) assessedthe ability of conventional MRI performed between 2and 8 days of age to predict neurodevelopmental hand-icap at postnatal ages of 12 to 24 months288-94 Al-though results of several studies suggested thatabnormalities of the cerebral white matter are asso-ciated with adverse outcome in term infants withneonatal encephalopathy 50 to 94 of infants withchanges in the basal ganglia developed CP mentalretardation and seizures at 1 to 2 years of age2889194
Barkovich et al89 correlated cognitive and motor out-come with timing of conventional MRI Proton den-sity MRI scans correlated best during the first 3postnatal days proton density and T1-weighted im-
ages correlated best during the first 7 postnataldays and T2-weighted images correlated best after 7to 8 postnatal days Overall proton density imagesduring the first 7 postnatal days were the best pre-dictor of outcome in this study
Similarly three studies using DWI (table 3 seethe electronic version of this article for table 11 atwwwneurologyorg) performed at a mean age of 2days in neonatal encephalopathy demonstrated a sig-nificantly elevated risk of adverse neurologic out-come although the small sample sizes makepredictions unreliable97-99
Finally review of the class II studies using protonMRS (table 3 see the electronic version of this articlefor table 12 at wwwneurologyorg) within the first11 days of life demonstrated that lactatecreatine ra-tios of 10 and elevated lactateNAA or lactatecholine ratios were highly predictive of adverseneurodevelopmental outcome at 1 to 2 years ofage93101-103 Infants with lactatecreatine ratios of10 were found to have adverse neurodevelopmen-tal outcome at 1 year of age (OR 132 sensitivity66 specificity 95 positive predictive value 86negative predictive value 88)101 Similarly ele-
Table 3 MRI studies of term neonatal encephalopathy
Referenceno Class Number Follow-up Predictor study Time study Outcome measures Age Data
88 II 15 1515 MRI newborn CP 1 yr only BG predict CP (33)
102 II 31 3131 MRS newborn CP MR 1 yr BG lacCHO amp lacNAAassociated with MR andor CP p 0003 for all
90 II 25 2525 MRI 7 days DQ 1 yr 66 N MRImdashNormal 12abn BGmdash1212 MRCP
117 III 16 1616 MRS d 18 exam 1 yr no significant differences
101 II 31 HIEamp 7N
3131 MRS newborn CP MR 1 yr if Laccreat 10 OR 132sens 66 spec 95
97 II 26 26 DWI newborn exam 6 mo abn DWI 1012 abnexamN DWI 1214 Nexam
98 II 4 4 of 4 DWI d 2 exam 3ndash21 mo abn DWI 44 abn exam
91 II 43 4343 MRI d 6 MR CP abn BG predict CP or MRp 001
2 II 52 5252 MRI d 8ndash30 head growth 1 yr N MRI 1112 N outcomeabn WM 55 abnoutcomeabn BG 57 abnoutcome
93 II 21 1818survivors
3 deaths
MRIMRS d 8 outcome 2 yrs N MRI 89 N abn MRI511 abn abn BGMRI47 abn LacNAA assocwith outcome p 005
99 II 43 4343 MRS 1 mo outcome 1 yr laccreat predict outcomep 0001
94 II 75 7375 MRI d 1ndash17 DQ 1 yr abn BG sens 90 spec100
104 II 18 HIEamp 3 N
1414survivors
4 deaths
MRI d 6 outcome 1ndash2 yrs LacNAA predict outcomep 005
June (2 of 2) 2002 NEUROLOGY 58 1733
RETIRED
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
RETIRED
vated lactateNAA and lactatecholine or lactatecreatine ratios in the region of the basal gangliawere significantly associated with CP and mentalretardation (p 0001 for all studies)102103 In an-other report abnormalities of NAAcreatine NAAcholine and cholinecreatine ratios in the occipitalgrayparietal white matter regions were predictive ofadverse outcome at a mean age of 15 months ininfants with HIE104 Positive predictive values forabnormal neurodevelopmental outcome based onthese metabolites were 064 068 and 075 for val-ues 2 SD from those of controls
Conclusions Class II MRI studies demonstratedthat the incidence of neurodevelopmental handicapamong those infants with abnormalities of the thal-ami and basal ganglia at mean postnatal ages of 2 to8 days is significant at 1 to 2 years of age Limitedand predominantly class III DWI evidence demon-strates abnormalities in infants with neonatal en-cephalopathy at a time when results of conventionalMRI are normal Class II studies of proton MRSperformed within the first 8 postnatal days also sug-gest good to excellent predictive values for this mea-sure for neurodevelopmental outcome at 1 to 2 yearsof age
Recommendation MRI should be performedwithin the first 2 to 8 days of life to provide predic-tive data for neurodevelopmental outcome in en-cephalopathic term infants (level A) DWI (level C)and MRS (level B) when available should also beperformed within the first 2 to 8 days to provideadditional prognostic data concerning neurodevelop-mental outcome
Future directions As the number of infantscared for in neonatal intensive care units grows andsurvival statistics steadily increase neuroimaginghas become critical technology Imaging of the devel-oping brain is no longer a research goal it has be-come clinically relevant Neuroimaging can providediagnostic information but also data used for clinicaldecision making as well as information on treatmentefficacy and prognosis This becomes particularly im-portant in the anticipation of potential preventiveprotective and rehabilitative strategies for the man-agement of critically ill newborn infants
Several ongoing clinical trials are assessing theimpact of neuroprotective strategies on long-termneurodevelopmental outcome105 For these studiesneuroimaging is criticalmdashnot only to provide diag-nostic entry criteria but also to assess the effect ofthe intervention and to provide prognostic neurologicinformation
Two sets of difficulties must be overcome to morefully incorporate neuroimaging into the newborn in-tensive care unit MRI holds great promise howeverthis imaging modality and others that may be soondeveloped must become more infant friendly andimaging strategies should be developed to providemaximum information in minimum time This wouldinclude the following improved magnet technology
that would allow easy placement of affordable MRIdevices in newborn intensive care units softwareand hardware advances that would minimize imag-ing time and allow DWI andor MRS sequences to beeasily performed on critically ill neonates and MRI-compatible devices that improve our ability to moni-tor and maintain critically ill neonates Further it isimportant that results of these imaging studies in-cluding processed DWI and MRI data be availableimmediately for viewing by all involved specialties
To provide more accurate information these MRtechniques must be optimized and standardized interms of types of sequence parameters for each im-aging sequence regions of brain evaluated and tim-ing of evaluations Prospective imaging studies withcentralized blinded readers and well-defined cohortsof infants and matched controls should be performedto determine accurate diagnostic criteria Similarlyprognostic data can be determined only from blindedstandardized follow-up assessments of all infants im-aged by the modality under study
Although there is some recent control data onDWI for neonates106107 the numbers of patients stud-ied are small There is also a strong need for MRScontrol data for neonates For both of these modali-ties serial studies are generally lacking and theimpact of timing of the study and regional variationon its result remains unknown For example al-though elevated lactateNAA lactatecreatine andlactatecholine ratios are reported to be more com-mon for infants with suspected HIE more studiesare required to determine the upper limits of theseratios for the normal population at various postnatalages and to determine the sensitivity specificity andpredictive values of these ratios Studies are alsoneeded to determine not only the optimal timing ofDWI and MRS evaluation for term infants with neo-natal encephalopathy but also the optimal region forinvestigation for MRS Long-term follow-up data onthe disability rate are of critical importance Controldata timing studies neuropathologic correlationsand ultimately outcome assessments are also neededbefore MRI becomes the standard of care for theVLBW PT neonate MRS and DWI for this age grouphave the potential to provide much needed informa-tion concerning the timing of white matter injury inthe developing brain and may lead to injury-specificinterventions108
Preliminary studies suggest that the more aggres-sive and timely use of advanced structural and func-tional prenatal imaging techniques to detect andcharacterize abnormalities may allow intervention toprevent postnatal neurologic morbidity and mortali-ty109110 Prenatal imaging may provide informationfor consideration of corrective prenatal surgical ormedical interventions where appropriate and can as-sist with the planning of surgical or medical inter-ventions in the intrapartum and postpartum periodsTherefore studies that correlate prenatal US andMRI findings with results of postnatal neuroimagingand outcome are needed
1734 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

RETIRED
Near infrared spectroscopy nuclear medicine(SPECT and PET) and fMRI are other major imag-ing technologies not discussed in this parameter be-cause of lack of data these technologies are underevaluation for use in the assessment of the develop-ing brain111-115 The challenge is to develop and im-plement effective applications of these advancedneuroimaging techniques and to perform studiesevaluating their diagnostic and predictive ability Asevidence becomes available116 it must be reviewed ona regular basis and the practice parameter must bemodified accordingly
Disclaimer This statement is provided as an edu-cational service of the American Academy of Neurol-ogy and the Child Neurology Society It is based onan assessment of current scientific and clinical infor-mation It is not intended to include all possibleproper methods of care for a particular neurologicproblem or all legitimate criteria for choosing to usea specific procedure Neither is it intended to excludeany reasonable alternative methodologies TheAmerican Academy of Neurology and the Child Neu-rology Society recognize that specific patient care de-cisions are the prerogative of the family and thephysician caring for the patient
Appendix 1Professional Organizations Represented American Academy of
Pediatrics American Academy of Neurology American Society ofPediatric Neuroradiology Child Neurology Society Society for Pe-diatric Radiology
AAN Quality Standards Subcommittee Members Gary Frank-lin MD MPH (Co-Chair) Catherine Zahn MD (Co-Chair) MiltonAlter MD PhD (ex-officio) Stephen Ashwal MD Rose M DotsonMD Richard M Dubinsky MD Jacqueline French MD Gary HFriday MD Michael Glantz MD Gary Gronseth MD DeborahHirtz MD (facilitator) Robert G Miller MD David J ThurmanMD MPH and William Weiner MD
CNS Practice Committee Members Carmela Tardo MD(Chair) Bruce Cohen MD (Vice-Chair) Elias Chalhub MD RoyElterman MD Murray Engel MD Bhuwan P Garg MD BrianGrabert MD Annette Grefe MD Michael Goldstein MD DavidGriesemer MD Betty Koo MD Edward Kovnar MD Leslie AnneMorrison MD Colette Parker MD Ben Renfroe MD AnthonyRiela MD Michael Shevell MD Shlomo Shinnar MD GeraldSilverboard MD Russell Snyder MD Dean Timmns MD GregYim MD Mary Anne Whelan MD
Appendix 2
Definitions for classification of diagnostic evidence
Class I Evidence provided by a prospective study in a broadspectrum of persons with the suspected condition using a ldquogoldstandardrdquo for case definition where test is applied in a blindedevaluation and enabling the assessment of appropriate tests ofdiagnostic accuracy
Class II Evidence provided by a prospective study of a narrowspectrum of persons with the suspected condition or a well de-signed retrospective study of a broad spectrum of persons with anestablished condition (by ldquogold standardrdquo) compared to a broadspectrum of controls where test is applied in a blinded evaluationand enabling the assessment of appropriate tests of diagnosticaccuracy
Class III Evidence provided by a retrospective study whereeither persons with the established condition or controls are of anarrow spectrum and where test is applied in a blinded evalua-tion
Class IV Any design where test is not applied in blinded eval-uation OR evidence provided by expert opinion alone or in descrip-tive case series (without controls)
Definitions for classification of prognostic evidence
Class I Evidence provided by a prospective study of a broadspectrum of persons who may be at risk for developing the out-come (eg target disease work status) The study measures thepredictive ability using an independent gold standard for casedefinition The predictor is measured in an evaluation that ismasked to clinical presentation and the outcome is measured inan evaluation that is masked to the presence of the predictor
Class II Evidence provided by a prospective study of a narrowspectrum of persons who may be at risk for developing the out-come or by a retrospective study of a broad spectrum of personswith the outcome compared to a broad spectrum of controls Thestudy measures the predictive ability using an acceptable inde-pendent gold standard for case definition The risk factor is mea-sured in an evaluation that is masked to the outcome
Class III Evidence provided by a retrospective study whereeither the persons with the condition or the controls are of anarrow spectrum The study measures the predictive ability usingan acceptable independent gold standard for case definition Therisk factor is measured in an evaluation that is masked to theoutcome
Class IV Any design where the predictor is not applied in amasked evaluation OR evidence provided by expert opinion orcase series without controls
Appendix 3
Definitions for strength of recommendations
Level A Established as usefulpredictive or not usefulpredic-tive for the given condition in the specified population (requires atleast one convincing class I study or at least two consistent con-vincing class II studies)
Level B Probably usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leastone convincing class II study or at least three consistent class IIIstudies)
Level C Possibly usefulpredictive or not usefulpredictive forthe given condition in the specified population (requires at leasttwo convincing and consistent class III studies)
Level U Data inadequate or conflicting Given current knowl-edge testpredictor is unproven
AcknowledgmentThe authors thank Wendy Edlund Alison Nakashima Vicki Glas-cow Marjorene Ainley and Nancy DiMaio for bibliographic andeditorial support and Karol Katz for computing assistance
References1 Hack M Taylor HG Klein N Mercuri-Minich N Functional
limitations and special health care needs of 10- to 14-year-oldchildren weighing less than 750 grams at birth Pediatrics2000106554ndash560
2 Mercuri E Ricci D Cowan FM et al Head growth in infantswith hypoxic-ischemic encephalopathy correlation with neo-natal magnetic resonance imaging Pediatrics 2000106235ndash243
3 Sreenan C Bhargava R Robertson CM Cerebral infarctionin the term newborn clinical presentation and long-termoutcome J Pediatr 2000137351ndash355
4 Wood NS Marlow N Costeloe K Gibson AT Wilkinson ARNeurologic and developmental disability after extremely pre-term birth N Engl J Med 2000343378ndash384
5 Guyer B MacDorman MF Martin JA Peters KD StrobinoDM Annual summary of vital statisticsmdash1997 Pediatrics19981021333ndash1349
6 Guyer B Hoyert DL Martin JA Ventura SJ MacDormanMF Strobino DM Annual summary of vital statisticsmdash1998Pediatrics 19991041229ndash1246
7 Allen MC Developmental outcome of neonatal intensivecare what questions are we asking Curr Opin Pediatr 200012116ndash122
June (2 of 2) 2002 NEUROLOGY 58 1735
RETIRED
RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

RETIRED
8 Hutton JL Colver AF Mackie PC Effect of severity of dis-ability on survival in a northeast England cerebral palsycohort Arch Dis Child 200083468ndash474
9 McCarton C Brooks-Gunn J Wallace I Bauer C Results atage 8 years of early intervention for low-birth-weight prema-ture infants JAMA 1997277126ndash132
10 McCormick M Workman-Daniels K Brooks-Gunn J The be-havioral and emotional well-being of school-age children withdifferent birth weights Pediatrics 19969718ndash25
11 Salokorpi T Rautio T Sajaniemi N Serenius-Sirve S TuomiH von Wendt L Neurological development up to the age offour years of extremely low birth weight infants born insouthern Finland in 1991-94 Acta Paediatr 200190218ndash221
12 Stevenson DK Wright LL Lemons JA et al Very low birthweight outcomes of the National Institute of Child Healthand Human Development Neonatal Research Network Jan-uary 1993 through December 1994 Am J Obstet Gynecol19981791632ndash1639
13 Taylor HG Klein N Hack M School-age consequences ofbirth weight less than 750 g a review and update Dev Neu-ropsychol 200017289ndash321
14 Barnes PD Neuroimaging and the timing of fetal and neona-tal brain injury J Perinatol 20012144ndash60
15 Huppi PS Barnes PD Magnetic resonance techniques in theevaluation of the newborn brain Clin Perinatol 199724693ndash723
16 Volpe JJ Brain injury in the premature infant Clin Perina-tol 199724567ndash587
17 Hack M Horbar JD Malloy MH Tyson JE Wright EWright L Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development NeonatalNetwork Pediatrics 199187587ndash597
18 Hack M Fanaroff AA Outcomes of extremely immature in-fantsmdasha perinatal dilemma N Engl J Med 19933291649ndash1650
19 Hack M Wright LL Shankaran S et al Very-low-birth-weight outcomes of the National Institute of Child Health andHuman Development Neonatal Network November 1989 toOctober 1990 Am J Obstet Gynecol 1995172457ndash464
20 Holshouser BA Ashwal S Shu S Hinshaw DB Jr ProtonMR spectroscopy in children with acute brain injury compar-ison of short and long echo time acquisitions J Magn ResonImaging 2000119ndash19
21 Novotny E Ashwal S Shevell M Proton magnetic resonancespectroscopy an emerging technology in pediatric neurologyresearch Pediatr Res 1998441ndash10
22 Barkovich AJ The encephalopathic neonate choosing theproper imaging technique AJNR Am J Neuroradiol 1997181816ndash1820
23 Rivkin MJ Developmental neuroimaging of children usingmagnetic resonance techniques MRDD Res Rev 2000668ndash80
24 Lemons JA Bauer CR Oh W et al Very low birth weightoutcomes of the National Institute of Child Health and Hu-man Development Neonatal Research Network January1995 through December 1996 NICHD Neonatal ResearchNetwork Pediatrics 2001107E1
25 Harding D Kuschel C Evans N Should preterm infantsborn after 29 weeksrsquo gestation be screened for intraventricu-lar haemorrhage J Paediatr Child Health 19983457ndash59
26 Maalouf EF Duggan PJ Counsell SJ et al Comparison offindings on cranial ultrasound and magnetic resonance imag-ing in preterm neonates Pediatrics 2001107719ndash727
27 Hayakawa F Okumura A Kato T Kuno K Watanabe KDetermination of the timing of brain injury in preterm in-fants with periventricular leukomalacia with serial neonatalelectroencephalography Pediatrics 19991041077ndash1081
28 Perlman JM Rollins N Surveillance protocol for the detec-tion of intracranial abnormalities in premature neonatesArch Pediatr Adolesc Med 2000154822ndash826
29 Papile LS Burstein J Burstein R Incidence and evolution ofthe subependymal intraventricular hemorrhage a study ofinfants with weights less than 1500 grams J Pediatr 197892529ndash534
30 Dammann O Leviton A Duration of transient hyperechoicimages of white matter in very low birth weight infants aproposed classification Dev Med Child Neurol 1997392ndash5
31 Maalouf EF Duggan PJ Rutherford MA et al Magneticresonance imaging of the brain in a cohort of extremely pre-term infants J Pediatr 1999135351ndash357
32 Paneth N Rudelli R Monte W et al White matter necrosisin very low birth weight infants neuropathologic and ultra-sonographic findings in infants surviving six days or longerJ Pediatr 1990116975ndash984
33 Poland RL Slovis TL Shankaran S Normal values for ven-tricular size as determined by real time sonographic tech-niques Pediatr Radiol 19851512ndash14
34 Allan WC Vohr B Makuch RW Ment LR Antecedents ofcerebral palsy in a multicenter trial of indomethacin for IVHArch Pediatr Adolesc Med 1997151580ndash585
35 Babcock DS Bove KE Han BK Intracranial hemorrhage inpremature infants sonographic-pathologic correlation AJNRAm J Neuroradiol 19823309ndash317
36 Mack LA Wright K Hirsch JH et al Intracranial hemor-rhage in premature infants accuracy in sonographic evalua-tion AJR Am J Roentgenol 1981137245ndash250
37 Pape KE Bennett-Britton S Szymonowicz W Martin DJFitz CR Becker LE Diagnostic accuracy of neonatal brainimaging a postmortem correlation of computed tomographyand ultrasound scans J Pediatr 1983102275ndash280
38 Trounce JQ Fagan D Levene MI Intraventricular haemor-rhage and periventricular leukomalacia ultrasound and au-topsy correlation Arch Dis Child 1986611203ndash1207
39 Behar R Coen RW Merrit TA et al Focal necrosis of thewhite matter (periventricular leukomalacia) sonographicpathologic and electroencephalographic features AJNRAm J Neuroradiol 198671073ndash1080
40 Levene MI Wigglesworth JS Dubowitz V Hemorrhagicperiventricular leukomalacia in the neonate a real-time ul-trasound study Pediatrics 198371794ndash797
41 Batton DG Holtrop P DeWitte D Pryce C Roberts C Cur-rent gestational age-related incidence of major intraventricu-lar hemorrhage J Pediatr 1994125623ndash625
42 Boal DK Watterberg KL Miles S Gifford KL Optimal cost-effective timing of cranial ultrasound screening in low-birth-weight infants Pediatr Radiol 199525425ndash428
43 Goetz MC Gretebeck RJ Oh KS Shaffer D Hermansen MCIncidence timing and follow-up of periventricular leukoma-lacia Am J Perinatol 199512325ndash327
44 Ito T Hashimotor K Kadowaki K et al Ultrasonographicfindings in the periventricular region in premature newbornswith antenatal periventricular leukomalacia J Perinat Med199725180ndash183
45 Dolfin T Skidmore MB Fong KW Kosins EM Shennan ATIncidence severity and timing of subependymal and intra-ventricular hemorrhage in preterm infants born in a perina-tal unit as detected by serial real-time ultrasound Pediatrics198371541ndash546
46 McDonald MM Koop BL Johnson ML Timing and anteced-ents of intracranial hemorrhage in the newborn Pediatrics19848432ndash36
47 Ment LR Duncan CC Ehrenkranz RA Intraventricularhemorrhage of the preterm neonate timing and cerebralblood flow changes J Pediatr 1984104419ndash425
48 Perlman JM Volpe JJ Intraventricular hemorrhage in ex-tremely small premature infants Am J Dis Child 19861401122ndash1124
49 Inder TE Huppi PS Warfield S et al Periventricular whitematter injury in the premature neonate is followed by re-duced cerebral cortical gray matter volume at term AnnNeurol 199946755ndash760
50 Sie LT vander Knapp MD van Wezel-Meijler G Taets vanAerongen AH Lafeber HN Valk J Early MR features ofhypoxic-ischemic brain injury in neonates with periventricu-lar densities on sonograms AJNR Am J Neuroradiol 200021852ndash861
51 Doyle LW Outcome at 5 years of age of children 23-27 weeksGA refining the prognosis Pediatrics 2001108134ndash141
52 Strathearn L Gray PH OrsquoCallaghan MJ Wood DO Child-hood neglect and cognitive development in extremely lowbirth weight infants a prospective study Pediatrics 2001108142ndash151
53 Bass WT Jones MA White LE Montgomery TR Aiello FIKarlowicz MG Ultrasonographic differential diagnosis and
1736 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
RETIRED
neurodevelopmental outcome of cerebral white matter le-sions in premature infants J Perinatol 199919330ndash336
54 deVries LS Eken P Groenendaal F Rademaker KJ Hooger-vorst B Bruines HW Antenatal onset of haemorrhagicandor ischaemic lesions in preterm infants prevalence andassociated obstetric variables Arch Dis Child Fetal NeonatalEd 199878F51ndashF56
55 Piecuch R Leonard C Cooper B Sehring S Outcome ofextremely low birth weight infants (500-999 grams) over a12-year period Pediatrics 1997100633ndash639
56 Pinto-Martin JA Riolo S Cnaan A Holzman C Susser MWPaneth N Cranial ultrasound prediction of disabling andnondisabling cerebral palsy at age two in a low birth weightpopulation Pediatrics 199595249ndash254
57 van de Bor M Ens-Dokkum M Schreuder AM Veen SBrand R Verloove-Vanhorick SP Outcome of periven-tricular-intraventricular hemorrhage at five years of ageDev Med Child Neurol 19933533ndash41
58 Pinto-Martin JA Whitaker AH Feldman J van Rossem RPaneth N Relation of cranial ultrasound abnormalities inlow-birth-weight infants to motor or cognitive performance atages 2 6 and 9 years Dev Med Child Neurol 199941826ndash833
59 Wilson-Costello D Borawski E Friedman H Redline R Fan-aroff AA Perinatal correlates of cerebral palsy and otherneurologic impairment among very low birth weight chil-dren Pediatrics 1998102315ndash322
60 Bozynski ME DiPietro MA Meisels SJ Plunkett JW Bur-pee B Claflin CJ Cranial sonography and neurologic exami-nation at term and motor performance through 19 months ofage Dev Behav Pediatr 199314112ndash116
61 Lai FF Tsou KY Transient periventricular echodensitiesand developmental outcome in preterm infants Pediatr Neu-rol 199921797ndash801
62 Pierrat V Eken P DeVries LS The predictive value of cra-nial ultrasound and of somatosensory evoked potentials afternerve stimulation for adverse neurological outcome in pre-term infants Dev Med Child Neurol 199739398ndash403
63 Ment LR Vohr B Allan W et al The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weightpreterm infants Pediatrics 1999104210ndash215
64 Whitaker AG Feldman JF Rossem RV et al Neonatal cra-nial ultrasound abnormalities in low birth weight infantsrelation to cognitive outcomes at six years of age Pediatrics199698719ndash729
65 Whitaker AH van Rossem R Feldman JF et al Psychiatricoutcomes in low-birth-weight children at age 6 years rela-tion to neonatal cranial ultrasound abnormalities Arch GenPsychiatry 199754847ndash856
66 Edwards AD Nelson KB Neonatal encephalopathies Timeto reconsider the cause of encephalopathies [editorial] BMJ19983171537ndash1538
67 Nelson KB Grether JK Selection of neonates for neuropro-tective therapies one set of criteria applied to a populationArch Pediatr Adolesc Med 1999153393ndash398
68 Grether JK Nelson KB Maternal infection and cerebralpalsy in infants of normal birth weight JAMA 1998279207ndash211
69 Johnston MV Hypoxic-ischemic encephalopathy Curr TreatOptions Neurol 20002109ndash116
70 Whitelaw A Systematic review of therapy after hypoxic-ischaemic brain injury in the perinatal period Semin Neona-tol 2000533ndash40
71 Rovertson NJ Edwards AD Recent advances in developingneuroprotective strategies for perinatal asphyxia Curr OpinPediatr 199810575ndash580
72 Hauth JC Merenstein GB Guidelines for perinatal care 4thed Elk Grove Village IL American Academy of Pediatricsand American College of Obstetricians and Gynecologists1997122ndash123
73 Badawi N Kurinczuk JJ Keogh JM et al Antepartum riskfactors for newborn encephalopathy the Western Australiancase-control study BMJ 19983171549ndash1555
74 Perlman JM Risser R Can asphyxiated infants at risk forneonatal seizures be rapidly identified by current high-riskmarkers Pediatrics 199697456ndash462
75 Boo N Chandran V Zulfiqar M et al Early cranial ultra-sound changes as predictors of outcome during the first year
of life in term infants with perinatal asphyxia J PaediatrChild Health 200036363ndash369
76 Stark JE Seibert JJ Cerebral artery Doppler ultrasonogra-phy for prediction of outcome after perinatal asphyxia JUltrasound Med 199413595ndash600
77 Eken P Toet MC Groenendaal F de Vries LS Predictivevalue of early neuroimaging pulsed Doppler and neurophys-iology in full term infants with hypoxic-ischaemic encepha-lopathy Arch Dis Child 199573F75ndashF80
78 Gray PH Tudehope DI Masel JP et al Perinatal hypoxic-ischemic brain injury prediction of outcome Dev Med ChildNeurol 199335965ndash973
79 Rutherford MA Pennock JM Doubowitz LMS Cranial ultra-sound and magnetic resonance imaging in hypoxic-ischaemicencephalopathy a comparison with outcome Dev Med ChildNeurol 199436813ndash825
80 Blankenberg FG Loh N-N Bracci P et al Sonography CTand MR imaging a prospective comparison of neonates withsuspected intracranial ischemia and hemorrhage AJNRAm J Neuroradiol 200021213ndash218
81 Blankenberg FG Norbash AM Lane B Stevenson DKBracci PM Enzmann DR Neonatal intracranial ischemiaand hemorrhage diagnosis with US CT and MR imagingRadiology 1996199253ndash259
82 Okumura A Hayakawa F Kato T Kuno K Watanabe KBilateral basal ganglia-thalamic lesions subsequent to pro-longed fetal bradycardia Early Hum Dev 200058111ndash118
83 Perrin RG Rutka JT Drake JM et al Management andoutcomes of posterior fossa subdural hematomas in neonatesNeurosurgery 1997401190ndash2000
84 Roland EH Poskitt K Rodriguez E Lupton BA Hill A Peri-natal hypoxic-ischemic thalamic injury clinical features andneuroimaging Ann Neurol 199844161ndash166
85 Odita JC Hebi S CT and MRI characteristics of intracranialhemorrhage complicating breech and vacuum delivery Pedi-atr Radiol 199626782ndash785
86 Cowan FM Pennock JM Hanrahan JD Manji KP EdwardsAD Early detection of cerebral infarction and hypoxic ische-mic encephalopathy in neonates using diffusion-weightedmagnetic resonance imaging Neuropediatrics 199425172ndash175
87 Jouvet P Cowan FM Cox P et al Reproducibility and accu-racy of MR imaging of the brain after severe birth asphyxiaAJNR Am J Neuroradiol 1999201343ndash1348
88 Aida N Nishimura G Hachiya Y Matsui K Takeuchi MItani Y MR imaging of perinatal brain damage comparisonof clinical outcome with initial and follow-up MR findingsAJNR Am J Neuroradiol 1998191909ndash1921
89 Barkovich AJ Hajnal BL Vigneron D et al Prediction ofneuromotor outcome in perinatal asphyxia evaluation of MRscoring systems AJNR Am J Neuroradiol 199819143ndash149
90 Biagioni E Mercuri E Rutherford MA et al Combined useof electroencephalogram and magnetic resonance imaging infull-term neonates with acute encephalopathy Pediatrics2001107461ndash468
91 Kuenzle C Baenziger O Martin E et al Prognostic value ofearly MR imaging in term infants with severe perinatal as-phyxia Neuropediatrics 199425191ndash200
92 Leth H Toft PB Herning M Peitersen B Lou HC Neonatalseizures associated with cerebral lesions shown by magneticresonance imaging Arch Dis Child 199777F105ndashF110
93 Roelants-van Rijn AM van der Grond J DeVries LSGroenendaal F Value of 1H-MRS using different echo timesin neonates with cerebral hypoxia-ischemia Pediatr Res200149356ndash362
94 Rutherford MA Pennock JM Counsell SJ et al Abnormalmagnetic resonance signal in the internal capsule predictspoor neurodevelopmental outcome in infants with hypoxic-ischemic encephalopathy Pediatrics 1998102323ndash328
95 Barkovich AJ Westmark K Partridge C Perinatal asphyxiaMR findings in the first ten days AJNR Am J Neuroradiol199516427ndash438
96 Albers GW Lansberg MG Norbash AM et al Yield ofdiffusion-weighted MRI for detection of potentially relevantfindings in stroke patients Neurology 2000541562ndash1567
97 Johnson AJ Lee BCP Lin W Echoplanar diffusion-weightedimaging in neonates and infants with suspected hypoxic-
June (2 of 2) 2002 NEUROLOGY 58 1737
RETIRED
RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

RETIRED
ischemic injury correlation with patient outcome AJR Am JRoentgenol 1999172219ndash226
98 Krishnamoorthy KS Soman TB Takeoka M Schaefer PWDiffusion-weighted imaging in neonatal cerebral infarctionclinical utility and follow-up J Child Neurol 200015592ndash602
99 Robertson RL Ben-Sira L Barnes PD et al MR line-scandiffusion-weighted imaging of term neonates with perinatalbrain ischemia AJNR Am J Neuroradiol 1999201658ndash1670
100 Wolf RL Zimmerman RA Clancy RR Haselgrove JH Quan-titative apparent diffusion coefficient measurements in termneonates for early detection of hypoxic-ischemic brain injuryinitial experience Radiology 2001218825ndash833
101 Hanrahan JD Cox IJ Azzopardi D et al Relation betweenproton magnetic resonance spectroscopy within 18 hours ofbirth asphyxia and neurodevelopment at 1 year of age DevMed Child Neurol 19994176ndash82
102 Barkovich AJ Baranski K Vigneron D et al Proton MR spec-troscopy for the evaluation of brain injury in asphyxiated termneonates AJNR Am J Neuroradiol 1999201399ndash1405
103 Robertson NJ Cox IJ Cowan FM Counsell SJ Azzopardi DEdwards AD Cerebral intracellular lactic alkalosis persist-ing months after neonatal encephalopathy measured bymagnetic resonance spectroscopy Pediatr Res 199946287ndash296
104 Shu SK Ashwal S Holshouser BA Nystrom G Hinshaw DBJr Prognostic value of 1H-MRS in perinatal CNS insultsPediatr Neurol 199717309ndash318
105 Nelson K Can magnesium sulfate reduce the risk of cerebralpalsy in very low birth weight infants Pediatrics 199595263ndash269
106 Neil JJ Shiran SI McKinsstry RC et al Normal brain inhuman newborns apparent diffusion coefficient and diffu-sion anisotropy measured by using diffusion tensor imagingRadiology 199820957ndash66
107 Morriss MC Zimmerman RA Bilaniuk LT Hunter JV Ha-selgrove JC Changes in brain water diffusion during child-hood Neuroradiology 199941929ndash934
108 Huppi PS Maier SEP Zientara GP Barnes PD Jolesz FAVolpe JJ Microstructural development of human newborncerebral white matter assessed in vivo by diffusion tensormagnetic resonance imaging Pediatr Res 199844584ndash590
109 Levine D Barnes Madsen JR Abbott J et al Fetal CNSanomalies revealed on ultrafast MR imaging AJR Am JRoentgenol 1999172813ndash818
110 Whitby E Paley MN Davies N Sprigg A Griffiths PD Ul-trafast magnetic resonance imaging of central nervous sys-tem abnormalities in utero in the second and third trimesterof pregnancy comparison with ultrasound Br J ObstetGynaecol 2001108519ndash526
111 Anderson AW Marois R Colson ER et al Neonatal auditoryactivation detected by functional magnetic resonance imag-ing Magn Reson Imaging 2001191ndash5
112 Born P Leth H Miranda MJ et al Visual activation ininfants and young children studied by functional magneticresonance imaging Pediatr Res 199844578ndash583
113 Born AP Miranda MJ Rostrup E et al Functional magneticresonance imaging of the normal and abnormal visual sys-tem in early life Neuropediatrics 20003124ndash32
114 DeVries LS Eken P Dubowitz LMS The spectrum of leuco-malacia using cranial ultrasound Behav Brain Res 1992491ndash6
115 Hesser U Katz-Salamon M Mortensson W Flodmark OForssberg H Diagnosis of intracranial lesions in very lowbirth weight infants by ultrasound incidence and associationwith potential risk factors Acta Paediatr 1997419(suppl)116ndash126
116 Am Acad Ped Am Coll Obstet Gynecol Neonatal encepha-lopathy and subsequent cerebral palsy defining the patho-genesis and pathology Elk Grove Village IL AAPWashington DC ACOG in press 2002
117 Chaterl JF Quesson B Brun M et al Localized proton mag-netic resonance spectroscopy of the brain after perinatal hyp-oxia a preliminary report Pediatr Radiol 199929199ndash205
1738 NEUROLOGY 58 June (2 of 2) 2002
RETIRED
DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology

DOI 101212WNL581217262002581726-1738 Neurology
L R Ment H S Bada P Barnes et al Committee of the Child Neurology Society
Standards Subcommittee of the American Academy of Neurology and the Practice Practice parameter Neuroimaging of the neonate [RETIRED] Report of the Quality
This information is current as of June 25 2002
ServicesUpdated Information amp
httpnneurologyorgcontent58121726fullhtmlincluding high resolution figures can be found at
Supplementary Material httpnneurologyorgcontentsuppl2002052958121726DC1
Supplementary material can be found at
Citations httpnneurologyorgcontent58121726fullhtmlotherarticles
This article has been cited by 30 HighWire-hosted articles
Permissions amp Licensing
httpnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Online ISSN 1526-632X1951 it is now a weekly with 48 issues per year Copyright All rights reserved Print ISSN 0028-3878
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology