Embed Size (px)
Citation preview

CME
Otoplasty: Sequencing the Operation forImproved ResultsJames G. Hoehn, M.D., and Salman Ashruf, M.D.Albany, N.Y.
Learning Objectives: After studying this article, the participant should be able to: 1. Understand the anatomy andembryology of the external ear. 2. Understand the anatomic causes of the prominent ear. 3. Understand the operativemaneuvers used to shape the external ear. 4. Be able to sequence the otoplasty for consistent results. 5. Understand thepossible complications of the otoplasty procedure.
Correction of prominent ears is a commonplastic surgical procedure. Proper executionof the surgical techniques is dependent onthe surgeon’s understanding of the surgi-cal procedure. This understanding is bestfounded on an understanding of the histor-ical bases for the operative steps and the ex-ecution of these operative steps in a logicalfashion. This article describes the concept ofsequencing the operation of otoplasty to pro-duce predictable results combining the tech-nical contributions from many authors. Thehistorical, embryological, and anatomic basesfor the operation are also discussed. Finally,the authors’ preferred techniques are pre-sented. Sequencing the steps in the preoper-ative assessment, preoperative planning, pa-tient management, operative technique, andpostoperative care will produce reproducibleresults for the attentive surgeon. Carefulattention to the details of the opera-tion of otoplasty will avoid many post-operative problems. (Plast. Reconstr.Surg. 115: 5e, 2005.)
The prominent ear is a source of significantconcern to the affected patient. This article willreview the significant historical contributionsto the management of the prominent ear. We
will emphasize a composite technique for cor-rective otoplasty, which is applicable to essen-tially all presentations of the prominent ear.Other authors have combined operative tech-niques such as we present, but we wish to re-emphasize the concept proposed by Elliott thatsequencing the segments of the operative pro-cedure provides the plastic surgeon withgreater control of the operation and predict-ability of results.1–3
ANATOMY AND NOMENCLATURE
The normal ear consists of a convolutedsheet of cartilage with a thin cutaneous cover.Variations of these convoluted contours occurin all ears, but the basic components are gen-erally similar (Fig. 1). The usual nomenclatureis provided in Figure 2.
The helical rim of the naturally appearingear is located 16 to 21 mm from the temporo-mastoid surface of the skull at the point ofmaximum prominence.4 The prominent ear isdefined when this distance is exceeded. Theaverage ear is 6.5 cm long and 3.5 cm wide,with significant variations. The configurationof the ear is affected by age because gravity mayelongate the soft-tissue cover and the lobule.The projection of the plane of the ear from theside of the skull, as measured by the cephalo-auricular angle, is approximately 30 degrees.
The majority of the defects that contributeto the prominent ear are described as failure of
From the Division of Plastic Surgery, Department of Surgery, Albany Medical College. Received for publication March 27, 2003; revisedJuly 30, 2004.
DOI: 10.1097/01.PRS.0000146680.27906.90
5e

the antihelix to develop its convolutions. Thisdeformity leads to a flattened scapha and ex-ternal rotation of the upper pole of the ear anda widened cephaloauricular angle. Enlarge-ment of the concha may produce a prominentear even if a well-developed antihelical fold ispresent. Of course, both defects may coexist.Variations in the lobule, the tragus, and theantitragus do occur and should be recognizedand addressed to successfully correct thedeformity.
EMBRYOLOGY
In embryonic development, the first and sec-ond branchial arches give rise to the externalear at about the sixth week of gestational age.Ear development begins as six swellings knownas “hillocks” that are located on either side ofthe dorsal aspect of the first branchial groove(Fig. 3). The anterior three hillocks developfrom the first branchial (mandibular) arch andthe posterior three hillocks develop from thesecond branchial (hyoid) arch. With tissuegrowth, epithelial contact, mesodermal pene-tration, and, ultimately, fusion of the hillocks,the external ear cartilage assumes its charac-teristic shape. The skin cover closely mirrorsthe cartilage shape. The completion of theshape has occurred by the eighth week ofgestation. By the age of 5 years, the externalear has achieved approximately 85 percent ofits adult size.5
The arterial supply of the ear arises from theposterior auricular, the superficial temporal,and the occipital arteries. The venous drainageis to the posterior auricular, the superficialtemporal, and the retromandibular veins. Sen-sation is supplied to the ears by the great au-ricular nerve, the auriculotemporal nerve, andthe lesser occipital nerve. Nerve supply to theconcha is from the auricular branches of thetenth cranial (vagus) nerve, which coursealong the external auditory canal. The lym-phatic drainage of the ear is divided into thezones of the branchial arches from which theyarise. The anterior three hillocks and theircutaneous surfaces drain to the periparotidlymph nodes and thus into the lymphaticchains of the anterior triangle of the neck. Theposterior three hillocks drain into the retroau-ricular area of the neck and thus to the mastoidand occipital lymphatic chains in the posteriortriangle of the neck.
SURGICAL HISTORY
In 1968, McDowell6 proposed the goals of asuccessful otoplasty: (1) the protrusion in theupper third of the ear should be eliminated;(2) the helix of both ears should be seen lateralto the antihelix from the front view; (3) thehelix should have a smooth and regular con-tour throughout; (4) the postauricular sulcusshould not be markedly decreased or dis-turbed; (5) the ear should not be placed tooclose to the head, especially in males; and (6)the contours and position of the two earsshould match closely but not be symmetrical.These goals are still appropriate 35 years later(Table I).
Ely,7 in 1881, was the first surgeon to de-scribe a procedure for aesthetic correction ofthe prominent ear. His technique involved re-section of both skin and conchal cartilage car-ried out in two stages. Dieffenbach8 reported asimilar procedure in 1845 to reconstruct thetraumatically deficient ear.
Luckett,9 in 1910, realized that the defect inthe prominent ear is a congenital failure toform the antihelical fold. He was the first todescribe the setback of the prominent ear byexcision of postauricular skin. He also em-ployed a vertical curved incision through thelength of the ear cartilage in an attempt tocreate the absent antihelical fold. He main-tained the scaphal and conchal cartilagechanges through the use of everting (“Lem-bert”-style) sutures in the new antihelix. Unfor-
FIG. 1. The normal-appearing ear.
6e PLASTIC AND RECONSTRUCTIVE SURGERY, January 2005

tunately, the Luckett procedure tended to cre-ate an abnormally sharp antihelix, particularlyin the region of the superior crus, giving theappearance of a “surgically altered” ear. Luck-
ett’s lasting contribution of the excision of thepostauricular skin, however, became an inte-gral part of many subsequent otoplastytechniques.
Stenstrom,10 using a basic plastic surgicalprinciple described first by Gibson and Davis,11
proposed a technique to establish the gentlefold of the natural antihelix through multiplesuperficial abrasions of the anterior surface ofthe auricular cartilage to create a new antihe-lical fold. The experimental observations ofGibson and Davis demonstrated that cartilageincised (scored) on one surface would bendaway from the plane of the incisions. Stenstromand Heftner12 applied this technique to both
FIG. 2. The surface anatomy of the external ear. Reproduced with permission from J. G.McCarthy (Ed.), Plastic Surgery. Philadelphia: Saunders, 1990.
FIG. 3. Embryology of the ear. Reproduced with permission from J. G.McCarthy (Ed.), Plastic Surgery. Philadelphia: Saunders, 1990.
TABLE IMcDowell’s Goals in Otoplasty
1. The elimination of protrusion in the upper third of the ear2. The helix of both ears should be seen lateral to the antihelix
from the front view3. The helix should have a smooth and regular contour throughout4. The postauricular sulcus should not be markedly decreased or
disturbed5. The ear should not be placed too close to the head6. The contours and position of the two ears should match closely,
but not be symmetrical
Vol. 115, No. 1 / OTOPLASTY SEQUENCING 7e

insufficient folding of the antihelix and exces-sive cupping of the concha.
In 1963, Mustardé13 introduced his suturetechnique to create the new antihelical fold.This technique avoided the sharp visible mar-gins that result from any of the techniques thatincised or excised cartilage from the antiheli-cal fold. Mustardé’s eponymous technique uti-lized the placement of permanent sutures onthe posterior surface of the ear cartilage tocreate a soft, gentle antihelical fold.14 Thesescaphoconchal sutures must be preciselyplaced. Suture management during knot set-ting must be done gently to avoid suture “fa-tigue.” A drawback to this technique is the hightension under which the sutures may beplaced, which can lead to suture failure. Thetechnique is also not easily used in the heavycartilage found in adult male ears.
In 1967, Kaye15 combined the anterior scor-ing technique of Stenstrom with the posteriorsuture placement technique of Mustardé. This,the first of several composite techniques, in-volved the vertical curvilinear striations of theanterior perichondrium to weaken the cartilag-inous “spring” followed by the creation andsecuring of the new antihelical fold by place-ment of posterior mattress sutures.10 Kaye alsoadvocated the use of nonabsorbable sutures toavoid recurrence secondary to knot failure.Kaye also proposed the anterior placement ofthe mattress sutures, but frequent visual prom-inence of the knot beneath the thin antihelicalskin is a problem and few other surgeons haveadopted anterior placement for routine use.
Furnas, in 1968, introduced the technique ofcorrection of prominent ears by conchal-mastoid sutures.16,17 After removal of the con-tents of the postauricular groove (postauricu-laris muscle and fibrofatty tissues), the conchais rotated in a sagittal plane from posterior toanterior and anchored to the mastoid fasciawith nonabsorbable sutures.
Elliott2 proposed a procedure for conchalreduction that reduces the enlarged conchawhen suture setback alone is insufficient tocorrectly position the ear relative to the side ofthe head. The advantage of this technique isthe ease of implementation that it provides tothe surgeon. The choice of conchal reductionmay be made when the surgeon determinesthat a setback with sutures (after Furnas) willbe insufficient to correct the ear prominence.In this way, surgical reduction of the conchamay be threaded into the otoplasty seamlessly.
Elliott’s conchal reduction utilizes an anteriorincision placed within the “shadow zone” ofthe conchal margin. The skin of the anteriorsurface of the concha is widely undermined.The lateral edge of the conchal cartilage isincised from the top of the conchal margin tothe bottom. Gentle pressure is exerted on thehelix. The excess conchal cartilage thatprojects through the incision is resected. Theincised cartilage edges are approximated witha nonabsorbable suture for stability. The skinincision is closed and the excess skin is ab-sorbed over time by contraction.
Recently, Bauer et al.3 described a modifica-tion in which the cartilage and its overlyingskin are resected together. This option can beinstituted to manage excess conchal skin whennecessary at the conclusion of conchalreduction.
Webster18 added to the successful otoplastyby drawing attention to the control of the earlobule. He noted that the “tail” of the helix,when cleared on its posterior surface, can berepositioned medially with a change in orien-tation of the lobule.
Elliott2 is credited with the operative colla-tion of techniques from Luckett, Stenstrom,Mustardé, and Furnas, which provides repro-ducible results in most ears. His description of“sequencing” of the otoplasty also increases thepredictability of the operation.
PREFERRED SURGICAL TECHNIQUE
In most patients, a sequential approach tothe surgical correction of the ear is desirable.The major steps include (1) preoperative as-sessment and surgical planning; (2) skin exci-sion and management of the postauriculargroove; (3) preparation of the postauricularsurface and identification of the tail of thehelix; (4) management of the anterior carti-lage surface; (5) securing of the new antihelix;(6) management of the tail of the helix to
TABLE IISequencing the Otoplasty
1. Assessment and surgical planning2. Skin excision and management of the postauricular surface3. Preparation of the postauricular surface and identification of the
tail of the helix4. Management of the anterior surface of the cartilage5. Securing of the new antihelix6. Management of the helical tail and control of the lobule7. Positioning of the ear—repositioning of the concha versus
resection of the concha8. Skin closure and postoperative dressings
8e PLASTIC AND RECONSTRUCTIVE SURGERY, January 2005

control the lobule; (7) positioning of the ear—repositioning of the concha versus resection ofthe concha; and (8) skin closure and postop-erative dressings (Table II).
Step 1: Preoperative Assessment andSurgical Planning
During the preoperative consultation, a fo-cused history and physical examination areconducted. With children, it is important toassess their drives and desires so that attentionmay be paid to the real reasons for the surgicalconsult. Often, the parents desire the opera-tion and the child is indifferent. In most in-stances, however, teasing and ridicule that havebeen endured by the child has become astrong motivating factor.
It is preferable to direct the discussion of thesurgical procedure to the child in languagethat the child can understand, so that the childand the parents are familiar with the goals andthe objectives of the surgery. Prehospital prep-aration includes a thorough shampoo thenight before surgery. Special haircuts in theoperative area are not necessary. No hair isshaved in the operating room.
Anesthesia. General anesthesia is preferredin children and is supplemented with local an-esthesia as noted below. In adults, local anes-thesia utilizing 1% Xylocaine with 1/100,000parts of epinephrine may be used alone. A “di-amond block” of the entire ear is performedwith a local infiltration of the conchal cup toanesthetize the auricular branch of the vagusnerve.
Sequencing the otoplasty: Preoperative preparationof the operative site. The cleansing of the exter-nal ear and the external auditory canal is per-formed with agents of the surgeon’s choice.The head is draped to allow visualization ofboth ears. An ophthalmologic adhesive vinyldrape is placed over the ear for additional fieldisolation and hair control. A small cotton ball isplaced in the external auditory canal to preventblood from accumulating on the tympanicmembrane (Fig. 4).
The desired ear contours are again pro-duced by exerting gentle digital pressure onthe helix to determine the desired antihelicalfold, which is marked on the skin (Fig. 4).Through-and-through markings with a needleand India ink are not necessary, so potentialtattooing of the cartilage is avoided.
Step 2: Skin Excision and Management of thePostauricular Surface
The posterior skin excision (Luckett) is cen-tered over the depth of the postauriculargroove (Fig. 5, above, left). The incision may beovoid or slightly “dumbbell” shaped andshould taper gently to a narrow “v” to allowsmooth closure. Excision of the skin may con-veniently include the subcutaneous tissue andthe contents of the postauricular groove—thepostauricularis muscle and the fibrocollag-enous tissue surrounding it (Fig. 5, above,right). Care should be taken to identify theposterior surface of the cartilaginous portionof the external auditory canal, to prevent inad-vertent injury. Hemostasis is secured.
Step 3: Preparation of the Postauricular Surface andIdentification of the Tail of the Helix
The skin of the posterior surface of the ear iswidely undermined to the outer border of thehelical rim (Fig. 5, center, left). The helical car-tilage prominence is then followed inferiorlyuntil the tail of the helix is encountered. Me-dial to the tail is a “slot” in the edge of thecartilage that allows access to the anterior sur-face of the ear (Fig. 5, center, left). Dissection tofree the tail of the helix anticipates the use ofthe tail to control the position of the lobule.
FIG. 4. Protection of the external auditory canal and an-tihelical markings.
Vol. 115, No. 1 / OTOPLASTY SEQUENCING 9e

FIG. 5. (Above, left) Design of the posterior skin excision. (Above, right) Excision of contents ofpostauricular groove. (Center, left) Undermining of the posterior surface of the ear and identificationof the tail of the helix. (Center, right) Access to the anterior surface of the ear. (Below, left) Scoring ofthe cartilage. (Below, right) Placement of Mustardé sutures.
10e PLASTIC AND RECONSTRUCTIVE SURGERY, January 2005

Step 4: Management of the Anterior Surface ofthe Cartilage
Using the access to the anterior surface ofthe ear noted above, a tunnel is created overthe course of the proposed new antihelicalfold by undermining with a pair of fine scis-sors. This tunnel will have to be wide enoughto admit the abrading instrument (Fig. 5,center, right); an otoabrader described byDingman is commonly used. The cartilage isscored through the perichondrium (Fig. 5,below, left). Weakening of the cartilaginoussurface by several gentle passes with the oto-abrader will allow the cartilage to bend awayfrom the anterior plane into the desired an-tihelical fold. Although the antihelical foldwill appear and increase its curvature withdeeper abrasion, care must be taken to avoidscoring through the thickness of the carti-lage. A full-thickness cartilaginous scoring in-cision, when fully healed, will often producea sharp edge, instead of the desired gentlecurve. This sharp edge is a telltale sign of asurgical otoplasty.
Step 5: Securing the New Antihelix
Once the antihelical fold is scored and thecurvature is satisfactory, attention is turned againto the posterior surface. Experience has taughtus that leaving the scored antihelical fold unse-cured will result in gradual flattening of the cur-vature, resulting in recurrence of the defect.Thus, permanent sutures should be placed, assuggested by Mustardé and emphasized by Elliott
(Fig. 5, below, right). We prefer to use 4-0 whiteMersilene suture on a cutting needle.
Care is taken to align the horizontal mattresssuture at the proper distances from the apex ofthe new antihelical fold to prevent distortionand warping. Each suture is secured with asingle “surgeon’s” throw without knotting. Allsutures are placed before any are permanentlytied. Usually three to six separate sutures arerequired.
Once the desired antihelical fold is achieved,each suture is then permanently secured, insequence, from superior to inferior, which al-lows the tension to secure the desired fold tobe adjusted sequentially. The knots can be tied“blindly” while observing the development ofthe antihelical fold from the anterior aspect.
Step 6: Management of the Helical Tail and Controlof the Lobule
Webster has demonstrated the role of the tailof the helix in the management of the laterallydisplaced lobule. After the tail of the helix hasbeen freed during the dissection of the posteriorcartilaginous surface (step 3), the tail can berotated medially over the posterior surface of theconcha and secured to this surface with a perma-nent suture (Fig. 6, left). Observing the helical tailin several positions allows the surgeon to directlyvisualize the effect of such movement on thelobule. One or two sutures are commonly used topermanently anchor the helical tail.
FIG. 6. (Left) Securing of the tail of the helix. (Right) Placement of the concha-mastoid sutures.
Vol. 115, No. 1 / OTOPLASTY SEQUENCING 11e

Step 7: Positioning the Ear—Repositioning theConcha versus Resection of the Concha
The conchal-mastoid groove has previouslybeen cleared of the fibrofatty tissue and thepostauricularis muscle as described by Furnas.The concha can now be positioned by gentlepressure on the anterior surface of the bowl ofthe concha. This will produce a medial rota-tion of the entire ear cartilage, which results ina movement of the entire ear toward the mid-line. This movement can be quantified with aruler and the ear positioned at approximately15 mm from the helical rim to the mastoidsurface. The concha can be permanently se-cured in this position with nonabsorbable su-tures (Fig. 6, right). Two or three sutures areusually required.
If excessive medial rotation is required toachieve adequate set back, the tragus will beforced to rotate in a lateral direction, whichproduces an unsightly prominence and, occa-sionally, a deformity of the tragus. In this situ-ation, a conchal reduction is required.
Conchal reduction. The anterior surface ofthe concha is marked for incision just inside theedge of the antihelix (Fig. 7, left). The natural“shadow line” will mask the residual scar.
The bowl of the concha is infiltrated withsimilar Xylocaine local anesthesia containingepinephrine. If the anesthesia is injected in thesubperichondrial plane, the resultant hydrodis-section will elevate the conchal skin.
A curving incision is made as noted above.The dissection is completed, widely undermin-ing the entire bowl.
The cartilage is incised and the medial edgeis allowed to override the lateral edge (Fig. 7,center). With gentle pressure on the helix, theamount of overriding required to producethe desired ear position can be determined.The excess cartilage is resected. Stabilization ofthe two edges of the cartilage is achieved byinterrupted, inverted nonabsorbable sutures(Fig. 7, right). In this location, it is importantthat clear or white sutures be used to obviatevisibility through the thin conchal skin.
Skin closure of this conchal incision can bethe surgeon’s choice. A well-healed scar canbecome almost invisible, as healing in this areais usually good. Our preference is for 6-0 nylonor silk removed by the third postoperative day.
Adjunctive procedures. Removal of Darwiniantubercles on the helical rim can be approachedfrom the posterior incision with a small amount ofadditional undermining. Reduction of the lobulecan be done at the conclusion if indicated. Severalsurgical flap designs have been proposed.5 Man-agement of transverse bars can be accomplishedby reversed anchoring cartilaginous flaps.19
Step 8: Skin Closure and Postoperative Dressings
Postauricular skin closure is the surgeon’schoice. This anatomic area is cosmetically “si-lent” but should be closed with the same atten-tion to detail that is given to any other wound.
FIG. 7. (Left) Marking the anterior surface of the concha for incision. (Center) Dissection of conchal cartilage. (Right)Stabilization of the lateral and the medial conchal edges.
12e PLASTIC AND RECONSTRUCTIVE SURGERY, January 2005

We have preferred a running, locked 4-0 chro-mic suture that is bathed starting on the sev-enth postoperative day and dissolves veryshortly thereafter. It obviates the discomfort ofsuture removal, especially in children.
Control of the new ear contours in the earlypostoperative period is very important. Theeffects of shear, especially in the younger pa-tient, can be disastrous.
We use a single layer of Xeroform gauze overthe postauricular suture line. Then a fluffed,dry, all-cotton gauze dressing is wetted andcarefully placed into the new antihelical foldsand the concha (Fig. 8). This gauze is contin-ued to the posterior surface over the Xeroformdressing; it also supports the ear in the desiredrelationship to the mastoid surface of the skull.Dry, fluffed, all-cotton gauze is then placedover the wet gauze. In a short period, the mois-ture from the wet gauze is absorbed into thedry gauze, leaving a soft mold of the desiredshape to support the new contours. Drainsshould not be needed if adequate hemostasishas been achieved.
The gauzes are held in place with cling wrapand finished with an Ace bandage (Fig. 9). Thisdressing is left in place for 7 days. At the firstpostoperative visit, the entire dressing is re-moved. The patient is then instructed to wear anear protector (either a skier’s ear protector or atennis sweat band) each night for a month toprevent accidental stresses on the ear duringsleep (Fig. 10). Vigorous activities such as sportsand dancing are permitted 1 month from the dayof surgery. After the dressing is removed, showers
and shampooing are allowed. Gentle scrubbingof the postauricular suture line is necessary toencourage suture dissolution. Postoperative pho-tographs are taken at the 2-month visit.
COMPLICATIONS
Complications Related to Appearance
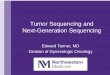
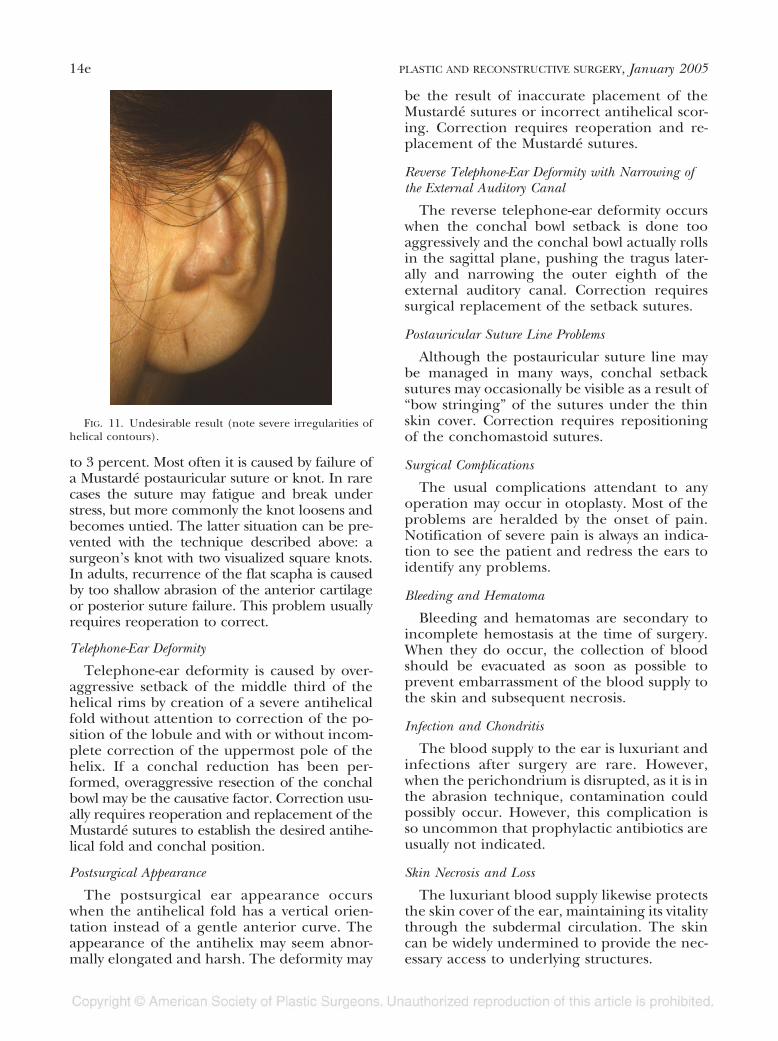
Most of the problems after otoplasty relateto undesirable appearance deformities of theoperated ear (Fig. 11). Several of these prob-lems deserve discussion to reflect on meth-ods of prevention.
Recurrence of the Deformity
In young children, the deformity recurrencerate has been reported to range from 1.8 percentFIG. 8. Dressing the postoperative ear.
FIG. 9. Securing the dressings.
FIG. 10. Late protection of the ear.
Vol. 115, No. 1 / OTOPLASTY SEQUENCING 13e
to 3 percent. Most often it is caused by failure ofa Mustardé postauricular suture or knot. In rarecases the suture may fatigue and break understress, but more commonly the knot loosens andbecomes untied. The latter situation can be pre-vented with the technique described above: asurgeon’s knot with two visualized square knots.In adults, recurrence of the flat scapha is causedby too shallow abrasion of the anterior cartilageor posterior suture failure. This problem usuallyrequires reoperation to correct.
Telephone-Ear Deformity
Telephone-ear deformity is caused by over-aggressive setback of the middle third of thehelical rims by creation of a severe antihelicalfold without attention to correction of the po-sition of the lobule and with or without incom-plete correction of the uppermost pole of thehelix. If a conchal reduction has been per-formed, overaggressive resection of the conchalbowl may be the causative factor. Correction usu-ally requires reoperation and replacement of theMustardé sutures to establish the desired antihe-lical fold and conchal position.
Postsurgical Appearance
The postsurgical ear appearance occurswhen the antihelical fold has a vertical orien-tation instead of a gentle anterior curve. Theappearance of the antihelix may seem abnor-mally elongated and harsh. The deformity may
be the result of inaccurate placement of theMustardé sutures or incorrect antihelical scor-ing. Correction requires reoperation and re-placement of the Mustardé sutures.
Reverse Telephone-Ear Deformity with Narrowing ofthe External Auditory Canal
The reverse telephone-ear deformity occurswhen the conchal bowl setback is done tooaggressively and the conchal bowl actually rollsin the sagittal plane, pushing the tragus later-ally and narrowing the outer eighth of theexternal auditory canal. Correction requiressurgical replacement of the setback sutures.
Postauricular Suture Line Problems
Although the postauricular suture line maybe managed in many ways, conchal setbacksutures may occasionally be visible as a result of“bow stringing” of the sutures under the thinskin cover. Correction requires repositioningof the conchomastoid sutures.
Surgical Complications
The usual complications attendant to anyoperation may occur in otoplasty. Most of theproblems are heralded by the onset of pain.Notification of severe pain is always an indica-tion to see the patient and redress the ears toidentify any problems.
Bleeding and Hematoma
Bleeding and hematomas are secondary toincomplete hemostasis at the time of surgery.When they do occur, the collection of bloodshould be evacuated as soon as possible toprevent embarrassment of the blood supply tothe skin and subsequent necrosis.
Infection and Chondritis
The blood supply to the ear is luxuriant andinfections after surgery are rare. However,when the perichondrium is disrupted, as it is inthe abrasion technique, contamination couldpossibly occur. However, this complication isso uncommon that prophylactic antibiotics areusually not indicated.
Skin Necrosis and Loss
The luxuriant blood supply likewise protectsthe skin cover of the ear, maintaining its vitalitythrough the subdermal circulation. The skincan be widely undermined to provide the nec-essary access to underlying structures.
FIG. 11. Undesirable result (note severe irregularities ofhelical contours).
14e PLASTIC AND RECONSTRUCTIVE SURGERY, January 2005

Conforming dressings, if applied too tightly,however, can obstruct the venous circulation inthe subdermal plexus, with resulting loss ofskin in the involved area. This complicationcan be avoided with appropriate dressings.
Abnormal Scar Formation
In approximately 2 percent of patients,scar tissue hypertrophy of the postauricularsuture line occurs. Hypertrophic scars areclinically diagnosed by the triad of (1) scarenlargement in the confines of the originalwound (does not invade normal tissue), (2)
scar tenderness, and (3) no racial predilec-tion. Management with serial intralesionalsteroid injections will usually control theovergrowth of scar tissue.
Keloid formation can occur in African Ameri-cans. The clinical diagnosis of keloid scarring ismade by the clinical triad of (1) scar enlarge-ment extending outside the operative site (invad-ing otherwise normal tissue), (2) no scar tender-ness, and (3) predilection for people of Negroiddescent. Management is more difficult and oftenconsists of intralesional excision and steroid in-jections followed by cutaneous irradiation in der-
FIG. 12. (Above, left) Preoperative anterior view. (Above, right) Postoperative anteriorview. (Below, left) Postoperative left lateral view. (Below, right) Postoperative right lateralview.
Vol. 115, No. 1 / OTOPLASTY SEQUENCING 15e

mal doses. Recurrence of keloid scars, even aftertreatment, is not uncommon.
Suture Line Granulomas
Occasionally, a buried suture will accrete agranulomatous formation around it. If the of-fending suture is close enough to the skin,extrusion occurs and removal of the suture issufficient. The typical late occurrence of sutureline granulomas allows local treatment by re-moval and topical wound care without changein the surgical contours.
Hyperesthesias and Dysthesias
Disturbances of fine sensation are not uncom-mon after incisions in the postauricular groove.The nerve disturbance is caused by the incisions,abrasions, and undermining, but not by directsectioning, of a named nerve branch. Althoughgradual spontaneous return of acceptable sensa-tion is the normal course of events, the occa-sional patient will need supportive care over thepostoperative period.
CONCLUSIONS
Sequencing the steps in the preoperative as-sessment, preoperative planning, patient man-agement, operative technique, and postoperativecare produces reproducible results (Fig. 12) forthe attentive surgeon. Careful attention to thedetails of the operation of otoplasty will avoidmany postoperative problems.
James G. Hoehn, M.D.4 Executive ParkAlbany, N.Y. [email protected]
REFERENCES
1. Elliott,R.A.,andHoehn,J.G. Otoplasty for prominent ears:A composite approach (Microfiche). Int. J. Aesthetic Plast.Surg. 1972A.
2. Elliott, R. A. Otoplasty: A combined approach. Clin.Plast. Surg. 17: 373, 1990.
3. Bauer, B. S., Song, D. H., and Aitken, M. E. A combinedotoplasty technique: Chondrocutaneous conchal re-section as the cornerstone to correction of the prom-inent ear. Plast. Reconstr. Surg. 110: 1033, 2002.
4. Adamson, J. E., Horton, C. E., and Crawford, H. H.Growth patterns of the external ear. Plast. Reconstr.Surg. 36: 466, 1965.
5. Rodriguez-Camps, S. Our procedure for integral aes-thetic otoplasty. Aesthetic Plast. Surg. 21: 332, 1997.
6. McDowell, A. J. Goals in otoplasty for protruding ears.Plast. Reconstr. Surg. 41: 17, 1968.
7. Ely, E. An operation for prominence of the auricles.Arch. Otolaryngol. 10: 97, 1881.
8. Dieffenbach, L. F. Die Operative Chirugie. Leipzig: F. A.Brockhaus, 1845.
9. Luckett, W. H. A new operation for prominent earsbased on the anatomy of the deformity. Surg. Gynecol.Obstet. 10: 635, 1910.
10. Stenstrom, S. J. A “natural” technique for correction ofcongenitally prominent ears. Plast. Reconstr. Surg. 26:640, 1960.
11. Gibson, T. W., and Davis, W. The distortion of autog-enous cartilage grafts: Its cause and prevention. Br. J.Plast. Surg. 10: 257, 1958.
12. Stenstrom, S. J., and Heftner, J. The Stenstrom oto-plasty. Clin. Plast. Surg. 5: 465, 1978.
13. Mustardé, J. C. The correction of prominent ears by usingsimple mattress sutures. Br. J. Plast. Surg. 16: 170, 1963.
14. Mustardé, J. C. Correction of prominent ears using bur-ied mattress sutures. Clin. Plast. Surg. 5: 459, 1978.
15. Kaye, B. L. A simplified method for correcting theprominent ear. Plast. Reconstr. Surg. 40: 44, 1967.
16. Furnas, D. W. Correction of prominent ears by con-chomastoid sutures. Plast. Reconstr. Surg. 42: 189, 1968.
17. Furnas, D. W. Otoplasty for prominent ears. Clin. Plast.Surg. 29: 273, 2002.
18. Webster, G. V. The tail of the helix as a key to otoplasty.Plast. Reconstr. Surg. 44: 455, 1969.
19. Hoehn, J. G., and Ashruf, S. Personal communication.February 22, 2003.
16e PLASTIC AND RECONSTRUCTIVE SURGERY, January 2005