Embed Size (px)
Citation preview

OR.IGIIIAL A^m'�,-'Y r ":f-+:'K" r r{_-L.tr *tiiffiti,r_,,,,;li=.
Clrthoglxettaic surgnn y and d euLtofacretrortnropndics iffi aCutnt ill'ess [[ E]ivision Itreetmrnl,lt: h'zfem dibwl'ar sasif.tal silXi t ffi sf,nffitffirutv
-!L' J
vf,l s,ris F{'*tbsfr anlX,:liarnceSahine. Ftuf, OD$, Sr med dent habi[," anci tr-llans Fanchreru, DD$. Odont Sn, FCDST-IK,{Hora}bfJ crn, J-in,it r,e iI u.ru I, a n d ti i t: :;,.r r! tL, i ; e rm t il t .t,
Th* ainr of thin stuclv was to asseas to what extent adult Herbst treatrnent is an alierrrativs tc ortirog;nathic;surgery' bV conrparirrg tl-re dentostretetal'treatmenl etfects in 46 adult Clase tt Division 1 subjects treateci witl'ra combined orthcldontic-odhognathic surgery approach lmandibular sagittal spiit osteotomy withoui:genioplasty) arrd 23 aduli Class ll Division 1 subjects treatecl with the Flerbst appiiance. Lateral lreadfilms inirabitual occlusion trom before anrl after treairnent (muliibracl<et appiiance. treatment after surgery or Herbsttreatment) were analyzecl. Alt surglery and Herbst subjects were treatecl
'successfully to Class I occlusal
relationships with normal overjet and overbite. ln the surgery group, the improvement in sagittal occlusionwas achieved by skeletal rnore than ciental changes; in the Herbst qroup, the crpposite was the Gase. Sl<eletaland soft tissue facial profile convexity was reduced signiiicantly in both groups; but the amount of profileconvexiiy reduction was larger in the surgery group. Tlre success and predictability "of Herbst treatment forocclusal correction was as high as for surgery. Thus, Herbst treatment can be considered an alternative toorthognathic surgery in borderline adult skeletal Class ll malocclusions,. especially when a great facialimprovement is not the main treatment goal. (Am J Orthod Dentofacial Orthop 2004;126:140-52)
n adrili subiects.having slceietal Cirus lI malocclu- is eff'ective in correcting adult Cla*ss Il maiocciu-sions with rnandibular deficiency, there rradition- sions.l-ti Tire Flerbst erppiiance can stimulate condylaraliy are 2 possibie treatnrent oprions. The first gtrowth and remodei the glenoid fossa in chiidren and
option is camouflage orthodontics-extracting the adrrlts.l'l This stimulatory effect on. thi temporoman-maxillary prenoolars to allorl rekusion of tbe maxillary dibular-joint (I.MJ) structures has:'been .also proven.incisor$"to normalize ihe overjet and mask the under- histologically in adult Rhesus monkeys hi:ated with the
.lying skeletal probleni. The second option is ortlrog- Herbst appliiance.? Thus, the Herbst appliance mighr be'nathic surgery to reposition the mandible atrteriorly. an onhopedic tool for nondurgical, nonext-action treat-
ln the orth<.rdontic iiteraure, there is little disagree- mcnt in borderline Ciass II adults.rnent aboul which treatment option to chriose for mikl Tire aim of this study vras to lrssess the extent ofand severe Ciass II adults. Mild Clzrss II probiems are Herbst treatrirent as an aiternative to ortirognathicsoived. i:), canroufiage. ortirotiontics and severe ones by surgery by comparing the"-dentoskeletai ancj facialorthogRatiric surgery. Disagreenrent arises, lrowever, in treatment effects in Ciass.II adults treated either vrithborcleriine cases" which might be'suirable to either ortirognathic surgery (manclibuiar sagittal spiit osteot-
the last few years have shown that the llerbst appliance MlErTEFllA.L AND *#ET*ODS
,,proicss'r.ancr he:rcr. f)epartmcnr. tif orrhodonrics, univcrsitv o[ [:iem, Bern. The'subjects were 46 adult's (3ti r'vomen' B rnen)
treateci bv orthognatl"lic surgery and 23 aciults (19Switzerlirrrd.t 'Prolessor anti ircld, Dcpurtrrrent ol Orriroclonr.icri, Univcrsirv of'Gicsscn. w(}nlen, 4 ruen) trcated b), the Fierbst approach. lt i lciesse*' Gerrrranv' patienls iracj Ciass I] Division I malocclusions, ancJ allItcpriu. rsquc$tri. to: Prof' I lr Slbine ltuf, I(i ir i ik i ' i . ir Kieierorrhopiidie,univcrsiri ir Bem, Frcihurs:itrltsrr: ?" cLl-301() Bcrn. {iwirz.crron,r .-*if. were treateci i lclnextr[ctiorr. Tooth alignnient before tntl
treatrnen[ option.Furthernore. clinicai practice and i'esearch during
snLrirrc.ru l'tlii znrli.u nibc" ch,
Subnritted. Novenrbur 2(103: rcvirud anri :rcccprecl, Fcbnurr.v 200.{.08rt9-,54(!6/$30.00
Clirpvriglit O 2(X).1 hv lhe nnrcricrrr r\ssoc:iirtitur ul- ()rrhodon!.isL.;.
t loi : I 0, l 0i ( l ' f .qr i lo.?(XU.02.0 I l
"140
onry witiiout geniolrlastyi or tlre Fierbst appiiance.
aft.el surgerY artd afier Herbst ffeatn'lent'uvas per{ttrnredr.'vith muitibrackef. appliances. A.r tlre end oi' treatment.all surgery niiacl Fieri:st subiects 'hacj Ciass I occiusionl;tryitfr normal r:rreriei ancl overiice.

Arnerican Journal. oJ' Orthodontics and Dentofacial O rthrspedicsValunte 126, Number 2
The m.ean pretrearrnent ages were 26 years (15.7-47.6 years) tor the surgery sr"rbjects ancJ 21.9 'years(L5.744.4 years) for the Herbst patienrs. Adulthood inthe Herbst subiects was defined by the pretreatn'lenthand-wrist radiographic skeletal rnaturiry stages R-IJ (4subjects) or R-.1 (.19 subjecrs) according to Fliigg anclTaranger.s At the encl o{'treailnent. all Herbst sutrjectshad reached the stage R-J. Altlrourgh no slceletal maturrity data existed I'or the surgery subjects, ull wereconsidered to have linisl'recl their growth.
The 46.surgery subjects were treat.ed with mandib-ular advancenrent with a retronrcllar sagittal split osteot-orny without geniopiasty; 23 were treated at the Cr-thognathic Surgery Clinic in Mairrro, Sweclen, with arnodification of the osteotomy according to Hunsuclceand Eplter,lo ancl the other 23 were treatecl at theOrthognathic Surgery Clinic in Minden, Germerny, witha modification according to Obwegeserl I and DalPont.'3 The Herbst patients were all treated at tireDepartment of Orthodontics, University of Giessen,Germany, with a carsted splint Herbst arppliance.13 Totaltreatment times averaged L.7 years tor the surgerysubjects,ancl 1.8 years for: the Herbst subjects.
Lateral headfilms in habitual occiusion from beforetreatment aurd after all treatment (after multibracket
.. appliance treatment after surgery and Herbst, respec-tively) were anaiyzed. Tracings of the radiographs werernade, and iinear ancl anguiar measurements were takento. the nearest 0.5 rnrn and 0,5o, respectively. Nocorrection was .mad.e for iinear enlargement.(approxi-mateiy \Vo in the rnedian plane). To reduce the methoclerror, all registrations of the 2 headfilms from eachsubject were done in the same session. Furthermore, allregistrations were done twice with an intervil of at least2 weeks between tl're registrations. In the final evalua-lion, the mean value of the registrations was used.
ln the surgery subjects, A-point was transferredfrom the first to the second radiograph after superim-posing tire headfilms on the stabie structures of theanterior cranial base.'o This pro-cedure was consideredvalid because all subjects were nongrowing, the surgerywas iimited to the mandible, and no marked dentalchanges were expected in the maxilla. In tire Herbstsubjects, ori the other hand, A-point wa.s,located oneach lateral headfilm, because dentai maxillary changesinfluencing A-point are known to occur.
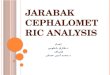
Cephalometric changes of sagittai and vertical jaw-base relationship" incisor relationship, facial height,facial profile convexity, and iip position were assessedby using standard variables not described in detail. Thecephalometric landmarks are shown in Figure L
The sagittal-occiusal anaiysis (SO anaiysis) ofPancirerzt5 was used. to analyze tire sagittal occlr,rsal
Ruf arzd. Pancherz 141
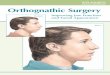
changes during the observation period. For all re-cordings on the pretreatment and posttreatnrent ra-ciiographs, the occlusal l ine (OL) (ciefinect by theincisal t ip of the most protruded maxil lary incisorand the distobuccal cusp of t lre first permanentmaxil lary rnolar) and the gcclusal i ine perpendicular(OLp) through sella l'roni tlre first hear.d{ilni were usedas tire reierence grid. Tlre grid was transferred fromthe pretreatment to the posttreatrnent radiograrphafter superinrposing the radiographs on the stableirone structures of the anterior cranial base.ra The SOanalysis conrprisecl the following l inear variables(F ig 2 ) :
f . is/Ol-p minus iiiOlp : twerjet2. Ms/OLp minus MilOLp : rnoiar relationship (pos-
itive value indicates distal relationship; negativevalue indicates nonnal or mesial relationship)
3. A/OLp : position of tire maxillary jaw base4. Pg/OLp = position of the mandibular jaw'ba^se5. Is/OLp : position of the maxillary central incisor6. Ii/OLp : position of the mandibula-r cenrral incisor7. Ms/OLp, position of the maxillary pennanent first
molarB. Mi/OLp : position of the mandibular permanent
first rnoiar
Changes in the different measuring points in relation toOLp during treatment were calculated as after-minus-before differences (D) in iandmuk position. Variabies3 and 4 describe skeletal changes, and variables 1, 2,and 5 through B represent a composite effect of skeletaland dental changes. Variables for dental changes in themaxilla and mandibie were obtained by the followingcalcuiations (variables 9-12):
9: Is/OLp (D) minus'A/OLp (D) = changes in posi-tion of the maxillary incisor
10. fi/Ol-p (D) rninus Pg/OLp (D) : changes inposition of the mandibuiar iridisor
11. Ms/OLp (D) minus A/OLp (D) : changes in thepositi.on of.the maxiliary permanent first moiar
12. MilOLp (D) minus Pg/OLp (D) : changes in theposition of the mandibular pefinanent first molar
.An important measure of success and predictabil-ity for a certain treatment approach is the consistency,of treatment clranges. This consistency'was caicu-iated as the percentage of subiects exhibiting acertain treatment cirange larger than or equal to 0.5oor 0.5 mm, respectively.
Statistical methods
For tire different variabies, tire arithrnetic mean(mean) anci tire staridard cleviation (SD) wele calcuiated.

'r49. RuJ' cuzcl Pant:lzerz
H-tine
Fig t. Reference points and iines used in standardcephalometric analysis.
Student I tests fcr unpairecl samples were perforrned toassess possible ciiff'erences between the 2 surgicai ap-
. proacires " (Sweciish and Gennan samptres) as well asbetween the surgery and Herbst gtroups. Student f tests forpaired sarnples were pertorrned to assess the significanceof treatment changes in the surgery and ltrerbst ggoups.Tlre stati.stical significance was deterunined at the A.7Vo,17o, irnd 5% ieveis of coniidence. A ievei iarger than SVowas considered statisticaliy not significant.
Tire method error of tire double registrations (.trac-
ings and measurements from before ancl Cier treatmentroentgenograms) of atrl subjects was calculated iry usingthe formuia of Dahibers:r6
t-Fi-;, . ' ' r ?
I ) . 4 -h t E : r l : * -
\ r nwhere d is ti:e difference between 2 measurements of apair ancl n is the number of subjects. The maximum
. rnethod error for dentai changes v/as 1.0 rnm. Forskeletatr and sofi tissue changes, the method error^ ciidnot exceed 0"7 mnr for iinear variabJes. l.0o for anguialvariabies, and 1.2 f'or inde)'; var-iabies"
tsxts\fr [ t I t-"
Because of'the snraill number of men in the surgen (n: [J)'ancl tire F{erosi (n : 4) gfoups as v,'e]i ertc the idenucaireiative irequency (L1%) cf nr*n irr tire 2. grouns, se;<
Arne rican,l o urnaL o.{' O nhod rm.tir: s a rLtl. D ent of aciul. (} rtho petli cs
August 2004
Fig 2" OUOLp reference grid and measuring landmarksusecl in cephalometric analysis of sagittal occlusalchanges (SO analysis).
differences were not considered. Thus, the male andfernaies samples in each treatrnent group were pooled.
Eecause the comparison of the treatment effects ofthe 2 rnodifications of tire retromoiar sagittal splitosteotorny (HunsuclcEpker ancl Obwegeser/Dal Pont)showed no statistically significant clifterences, the 2surgery samples were evaiuated as I group.
The cephalometric records of the sur.'gery andFlerbst groups before and after treatrnent ale shownin Tabies I and I[, With respecf- to the. cepiraiometricstandard variabies (Table I) from before treatrnent,the surgery group compared with tire llerbst grouphad a iarger Wits value (mean 2.2 mm; P < .01), aiarger posterior facial treighi index (mean 5.5;P < .001), a smaiier interjaw-base arngie (mean 5.5;P < .01), and a iarger soft t issue prclf i ie convexityinciuciing the nose (mean 4:9; Prespect to tire variabies of the SO analvsis (Table lI)from hefore treatment, no statisticaiiy significantcliffererrces between tire surgery and the Herbstgroups were fciund"
$tandard cephalcmetric treatmrent changies
Tire rreatmeni changes in the $urgery and Herbstgroup:; are sirovrn in Table i l l . Tire ciranges insagittai rn:rxil lar"y position (SllA) were cornparabiein i:otir grolrpsr Tire surger\/ groitp had greatermanoihuiar advancenrent (Sf ' IB. mean 1.3".

Anrcrican Jounnl of Orthodontics and Dentofacial OrtlwpedicsVolurne 126, Numher 2
Ruf artd Pancherc 143
Table t. Cephalometric standard record.s (rnean, SD) before and after treatment in 46 adults treated withor:thognathic_surgery (mandibular sagittal split osteotomy) followed by multibracket appliance and 23 adultstreilted wjth Herbst appliance followed by multibraclcet appiiance
Srrrgery Hcrhst
Be.fore. A.fier After
Yu.riahlc Meun SD
Bqfbre--J--
Mcan. ,SD Mean:
Sagrttal iawrelation
Vertical iawrelation
Incisor relation
Facial height
Profiie convexity
Lip position
SNA (")
SNB ( " )
SNPg (")
ANB (")
ANPg ( " ) '
W i rs (mm)
ML/NSL (")
NL/NSL (")
ML/NL (")
Overbite (mrn)
Spa-Gn x IOOAI-Gn (index)
Spp-Go' X 100/S-Go' (index)
NAPg (")
NS/Sn/PgS (")
NS/No/PgS (')
UL-EJine (mrn)
LL-E-line (mm)
81.4r 4 .0175.37 3.3977.08 3.756.04 2.754.33 3.464.72 3.01
30.08 7.'328.77 2.91
21.3 r 7.344.73 2.84
54.84 2.3446.r]9 4.89
170.87 7.33158.12 6.71121.35 4.22-2.55 2.84-r.67 3.27
81. r2 3 .11977.4() 3.4178.68 3.803.62 2.73?.44 3.190.61 3,36
33.41 7.868.39 3.57
25.02 7.782.16 0.94
56.11 2.5844.88 5.64
175.32 6.-19163.57 6.71124.55 4"50-s.05 2.87-2.79 3.38
80.46 3.2375.27 4..0676.84 4.285. r B 1.693.(tZ 2.30?.5-5 2.(Xt
34.1? t].617.29) 3.15
26.ti3 7.914.43 1.83
54.55 1.8341.40 5.26
172-08 5.21159.68 6.25126.30 3.93-:3.11. 2.28- 1.64 3.28
80.57 3.2776,09 4. t977.54 4.584.48 t.793.02 ?.4s1.47 1.95
33.43 8.976.77 3.61
26.72 7-721.95 0.68
54.97 t:1442.43 5.rB
173.17 5.42162.82 6.79127.?4 4.32-4.37 ?.49- 1.90 3.02
Tahle ll. SO analysis. Cephalometric records (mean, SD) before and alter treatment in 46 adult Class tr Division1subjectstre-at.e-dwithqrthogrrathicsurgery(rrrandibularsagittalsp1itosteotomy)followedbymu1tibracket���appliance and 23 adult Class II Division t subjects treated with Herbst appliance followed by multibracketappliance
Surgery Herbst
Bgfore
Mean SD Mean
After Before After
Varitrhle (mm) Mean Mean ^tD
l. Overjetis/Olp-li/OLp
2. Molar relation*Ms/OLp-Mi/OLp
3. Maxillary. baseA/OLp
4. Mendibular basePg/0Lp
5. Maxillary incisoris/OLp
6. Mandibular incisorIi/0Lp
7. h4uxiliary rnolarMsiOl-p
B. N4andibular moiarMi/OLp
9.69
+'t.77*
78.89
77.67
88.36
78.66
56.37
54;60
2.68
1.97
4.80
5.54
5 . 1 I
5.41
5.95
3.38
78.89
81.72
86.99
83.61
57.06
64.29
1 .13
3.00
4.80
5.97
5.59
5.81
1 / l
6.6s
8.88
+ 1.53+
78.52
80.07
88.21
79.33
57.78
56.25
1.35
.3.99
4.94
4.47
5.36
4.70
5.32
? t c
-2.58*
78.9i
81-35
85.42
83.29
s6.35
s8.92
0.61
0.98
5 . t I
4.77
4.80
4.88
4.68
4.97
'lPlus (*) implies Class II molar reiationship; minus (-) implies Class I nrolar relationship.
P < .001; Sl , lPg, mean 0.9oQuentil, greater decreases intionship angles (ANB, mean
P < .01) and conse-sagittal jaur-base rela-L . 7 " , P < . 0 0 1 ; S N P g ,
- - f \ ! v ' v
t
Tire arnount of overbite reductionthe surgery and Flerbst subjects.
iarger reduction in the surgery than in tire Herbstgroup (Wits mean, 3.0o, P < .001).
was comparabieThe mandibuiarrnean 1.3,o, p .-_ .001). Tire Wits appraisal showed a for

144 Rrl' untl, Iltutcite.rT. A ntc rica n J o u rnul. o,l' o rt lu t do n t iu ruu.l D en t ol i.r c' iul o rt h o p c d i c.t
,\r.r14ttst 20(N
Tabte l le. Sta'clarcl cepgal6nretricr;. Comparison <)1'treatment ohangcs (menn. SD) in 4(r adtrit Ci1.1 II lf ivision I
' , t . , i . .L - r iearcc lw i t l i t r r t l . r t lg ,n i , t t , l r i cou 'g , . i y ( r r la r rc l i [ ru l i r rsag i l ' t i t l . sp i i t r rs te t l { '< ln ry ) l .o l l t lwe ,d � � � � � � � � � � � � � � � � � � �ap1r l ianco i r r rdJ- ] ru iL r l tC l . i ss r rn iv is i t in . , l su i r ' i ec : ts l rea te i lw i t | r . l - Ie rbs t i rp1r I i i l r i ce | t r l l t l t , ved t ry � � � � � � � � � � � � � � � � �appl i i rncc
T rt.ntmrtr l t ' l tuntt. t ( ul ' t tr-bc. l l tr t)
,5'rrr,qrrv I'l t'rln';l Surgtryt-l larb'tl
. J L . l lVlutrr :;I}
Sagirul iawrcl i t t ion
Vertical .iawrelation
lncisctr relnttott
Fncirl heiglit
Pro{iie convexity
Lip position
,s l ' lA ( ' )
i i l .JLi {" IS N I ' g ( " )
A l ' l l l f " )
u\ l ' i lrg (")
Vy' i t i ( rum)
ML-/NSL (")
NL / t ' lSL ( " )
ML,/NL (")( )vcrhi te (nrm)
fipl-Cn X 100/N-tin (index)
Spl-fiol x l0()/ti-Go' (index)
I ' { APg'( ' )
l{l i/SnlPgS (")
l. lS/No/t'gS (")
UL-E-I ine (mtn)
LL-E-Iino (nrm)
-0.1(,)n l , t
I .()U- '2.r11: I . l i t l- 4 . 1 I
_ ) . - ) J
* u.3ti? ? l
*2;06
t .77-
- : . \ , l
4 .45d . 4 <^ t . - l . . ,
3.2(l- 1 l ( )
l . t - ,
t.:J lr . 3 1l . 2 t )I . " ) . ' )
1.9( )2.4lir . 7 l2.63
(1.92
7.511,.ti03.?,72.ff|r .14l , . J J
- t , / :
l0"9l"l ' l
9 .25' f- 1 2 . 7 t +
*t .5{) : l j
* lzl.{r4'l 'g . l : ' f
* 1 .47" .
9.541'- 5.4:l+
9.1i6+. - -5 . ,43h
t0 .7 t t+10.!)?+8.12 ' t
-9.731'-3.261'
0 . I It r - o i
0.70-( ] .7( )*0 .60- I .Oi i-0.trq-i l . ;r2- ( i . l i-2.4ii
0.42t . ( )31,01)3 . l 4l.()4
-0.26
0.64{J.7}i().1:i50.1'l( ) . t i lI .? { r1 . 2 1t . 451 . 5 et .q40.731.45i.5l i1 .791.971.07l . l \ . ,
1 r . i ) -
5 . ( )3 x
3.r)6'*4 .3 J ' i '- - - 1 . / i )
- 4 . l 2 ' '- ' . ( ) l *
1 n a l l s* l . / , r
- ( ) .33" '
* 6 . 1 4 *
1.75't '3 . 4 1 1
3 . 3 1 i
8.3!J{a < A +
*5.{l.r'I t a n N- t ^ t , . 1
-( ) .4i)i .:i0( ).!)()
- 1 . 1 1- 1 .2 t t- 3 . t ) l
4.il ' l{1 .14.3.0( )0.4f0 .85
- 3.{)53 .3b- . . 1 I
l - l t i- r . 2 3*().86
I t , { l l s- t . r l t
/ r . L4l . J.-t
2.901* 5.7( )'f-"4.0-l l '
, r r . l .- f ) . / - 1 '
7.()5'l '
0 .3:""
4.g l ' l '
0.6li"*
3.7 i )1 '* i r . l ? t
5 . 1 ? ' l
2'9(rt
-3,t)(tt
- 1.62n*
ns inrplies P > .05 (rrot signii icant).j ' impi ies P < .05.t inrpl ies P <.01.Tirnpl ies P -- .0()1.
piane angie showed opposite changes in the 2 treatrnent
groop*. In the surgery group' tire MLA{SL increased
(mean 3.3o. P < .001), whereas a decrease (nrean 0'7",
P < .05) was noted in the Herbst $oup. The interjaw-
base angle (ML/NL) increasecl in the surgery grotlp
(rneatr 3.7o. P < .001) and decreased in the Elerbst
group (mean 0.1o, not significant). The inclination ot
the inaxilia in reiation to the anterior cranial base
(NL/NSL) was unatfected by either surgery or Herbst
treatment.Anterior facial height increased more in the surgery
group than in tire Herbst group (index mean 0'8. P <
.(}0i). simiiu-ro tire cirailges of the rnandibuiar piane
angle, tire posterior facial height showed opposite
chirnges in the 2 groups. A reclucticin in posterior facial
heigirt tocilc place in the surgery grclllp (index mean 2'0.
P < .001), wirereas an increlse was seen in tlre Fierbst
gr:oup (index l l-)ean 1'0: P ": .01)'
Tire amount of pnifiie convexity reciuction vrtL$
iarger in the surgery group tiran in the Herbrst group'
fhe largesf crclup difference (mean 3.4o) r,vas fourici f'or
sireietal profi le cclnvexitlr (lrJAPg, mean '3.4o,
P < '001)
und. tire smallest for soft tissue pr:ofiie coiryexity inciud-
ing tire nose (l '{,S/No/PgS' nlean }-.2', P < .01)'
The po:ritiorrs of the' r-rpper and lorver lips becanre
mofe retrusrve rn both treatment groups. A statistically
significant group diflerence was f'ound oniy for the
upper lip (UL-E-line), which became more retrusive
(1.2 rnm, P < .01) in tire surgery groltp.
S0 analysis treatrnent changes
The treatment changes in the surgery and Herbst
gl.oups are shown in Table IV. The amounts of overjet
reduction (surgery, 6.3 rnrn; Herbst, 6-7 mm), Class II
molar correction (surgery, 5.0 mm; Flerbst, 4' l mm),
ancl mandibular moial mesiaiization (surgery, l'6 mm,
Herb.sl, 1.4 mm) were comparabie in tl-re 2 groups' The
surgery group iracl greater (mean 2.8 mm, P < '001)
manclibular advancement than the Herirst group. Itt
coprparisor-l with the surgery groLlp, the llerbst group
sir6wed greater 1rzuii}l1ry trase forward deveiopnrent
(nrean 0.4 mm; P .< .00I), rn&xil lary incisor Ietltrsion
(mean 1.8 mlrl, P
pralrusiott (mean LE mm; P < -(l l). Tire maxil lar5t
moiars moveii iri opposite direclions in tire 2 groups. A
pesial moveiTrent ol 'the maxil iary molari; was found in
the surgery group (n-rean 0.7 mm' t) <* .05). and a distai
ffrovement \\1as seen in the Fier:bst gror-rp (n-lean 1 'B mm"
P < . 0 0 1 ) . iThe r:ei6.tionsirip between ciental aucl slteletai

Ameri can,l ourna I at a nhodo ntics tmd Dentofacial A rthope dicsVolume 126, Ntunber 2
Ruf and Pctncherz 145
Table lv. So-Ana'lysis, Comparison of treatment chenges (mean. SD) in 46 adult Class Il Divisiorr 1 subjectsh'eated with orthognathic surgery (nrandibular sargittal split osteotomy) {bllowed by rnultibraclcet arppliance and 23adult Class II Division I subjects treated with Herbst appliance {'ollowed by nir"rlt ibracket appliance
Trcu rment cluut.gc:s ( u.fter-b e{b re )
Srr,qcrj Hcrhst SurgenlHerhsl
Vuriublc (nzm) Mecut Meunsi).il)
l. C)verjetis/oLp(D)-liloLp(D)
2. Mollr rel i t t ionMs/oLp(D)-Mi/OLp(D)
3. Maxillary b*ieA/OLp(D)
4. Mlndibulur basePg/OLp(D)
9. Maxil lary incisorIs/OLp (D)-A/OLp (D)
10. Mandibulrr incisorii/oLp(D)-Pg/Olp(D)
I l . Muil lary nrolnrMs/oLp(D)-A/OLp(D)
12. Mrndibulrr nrolnrMi/oLp(D)-Pg/olp(D)
*6.31
-s.oo
0
4.05
- i . 36
'0.90
0.69
i.64
2.46 - 17.407
3. i3 - 10.84*
0 Ons
2.49 11.03*
2.21 4.17'�r
2"36 2.56r
I O O I ? { r k
2.02 5.51+
-6.75
- 4 . 1 I
0.39
i"2B
n t n* J . l /
2.69
- 1 .83
1.39
l .O-r
1.45
0.65
I .25
2 . 1 1
1.93
1 . 1 0
t . l 4
- 12.30'f
- 13.61*
2.89i
4 .9 t +
-7.21+
6.67+
-7.95+
5.85'l
o.4 0.66"*
-0.89 , - 1.25n*
-0.39 *3.90{
2.77 4.86t
1.81 3.301
- i .79 -3.03'r
2.52 548*
0.2.5 0.51n'
n.r impiies P > 0.05 (not significant).+irnplies P "-- 0.05.rimplies P < 0.01.rinrplies P < 0.001.
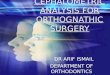
changes contributing to Class II correction in theincisor and rnolar regions is shown in Figure 3. In theHerbst group, the improvement in sagittal occlusionwas achieved by dental more than skeletal changes; inthe surgery group, the opposite was the case: Theamount of skeletal change's coutributing to overjet arrdrnolar correction was iarger in the surgery (637o andBOa/o, respectively) than in.the Herbst (I3Vo and 17Vo,
respectively) group
Individual changes
The individual changes for 8 of the 25 analyzedcephalometric variables are givdn in Figure 4. Allvariabies had substantial interindividual variation inboth the groups.
The maximurn arnounts of changes in individualsubjects of the 2 groups are given in Table V. Thelargest amount of overiet reduction was in a Herbstsubject (12.2 rnm). For all other variables, the rnaxi-rnum amount of individual changes was noted in thesurgery subjects. Even if the arnount of changes dif-fered between the groups. the direction of changes wasthe sanre, except for the mandibular plane angie andposterior facial height.
The consistencl, of treatment reaction is given inTable V. Overiet and overbite were reduced consis-
tently in both the surgery QSVa for both variables) andthe Herbst QAAVo and 96Vo, respectively) subiects;l\OVo of the Herbst and 93Vo of the surgery subjectshad improved moiar relationships. Mandibular progna-thism increased more consistently in the surgery (SNB: 917o) than in the Herbst (SNB _ 74Vo) subjects.Correspondingly, more patienls with an ANB recluctionwere seen in the surgery than in the Herbst (987o andT49o, respectiveiy) groups. The vefiical jau'-base rela-tionship and flre anterior and posterjor facial heightswere more consistently affected.,.ly surgery (91Vo in-crease, BTVI increase, and TBVo d.ecrease, respectively)than by Herbst treatment (56Vn decrease, 52(% increase,and 659c, increase. respectively). Skeietal profile con-vexity and sotl tissue profiie convexity including andexciuding the nose were reduced more consistently inthe surgery (97V0,96Vo, and 76Va, respectively) than inthe FI erbs t (7 }Vo, 9 6Vo . and 83 Vo, respecti vel y ) sr-r bj ecls.
The skeietofacial changes during treatment. areshown far 2 surgeryr sub.iects (Figs 5 ancl 6) and 2Herbst subjects (Figs 7 and B).
D!SCUSSrOt{
The subiects in this investigation can be consideredto be unselected.,The Swedisir and Germau sampiesincluded all Clasd II Division 1 subjects (except those
: r1:+f ,.rijr.::ill, j iij.::- :,.. t- -,.- "r

'i4.6 [tu'{' cuu!. l"ttnclu:t'z /\tttcri.cu.rL .lournttL rs.t' Ltilint.ilt1zlics uru.l llenttittcial ttrihttpr:tiics
Attg,t tst )Lt01
fr"lwerled. ilcl m"e crlor I
Sr;r-qq:fi," $,3 mrn 1'10CI %
Flerirsl $.tj mrn /' l(r0 %'
[*_--_- *fferera/
ii S 4"t} ntm / 63'}'; i| ry -: il-ryr-l-:ill. *-l
i *-
L*"lafII It X.i:l rrlrri ,'37' ?i,
ig_ s.P i!:!!l$rJ
IWaxilla
S 0.€) mrn I {^t %bf - Q.6 rwrn / -'l# i'a
rit
ff
S.{iarsdrt$ie
4""il rnm / [J01'/a?..3 rnm / 32 9',
&LSI I
Adaxfffa
* 0.7 nrm /-'t4 %'l-8 rnrw / 44 "ti,
f#andfl*de
$ 1,7 rnm 134.Yi# |"4 mnt i 34 "ri
Fig S. Mechanisrn of cverjet ancl molar correction in 46 Class ll Division 'i adults treated with
ofthr:gnathic surgery {manciibular sagittal split osteotomy)foliowed by rnultibracket appiiances and
2S Class ![ Sivision 1 adults treatecJ with Herbst appliances followed hy multibracket appiiances.
witir severe oilen bite) treat'*d during 10 years. Tire
Herbst rlample cornprisecl consecutive Ciass I]. Division
i aduits treated ra'ith tire Fierbst "rppliance at the
orthodcntic clepartrnent iri Giessen,There vv'ils Ll cleai: overrspresentaticlu clf tt'zomen in
'hoth sarnpie:;. This l.grees witi: eariier stulciies of arlult
orllrtidnr-ltic a.ncl orthognathic; s urgery paLienri;. I 7-2 i -filp
rea$()n lcl tiris unequai se>i distrij:ution is unknowrL" but
it. might. be iissociatecl r,vrth v/otrer)'rl greater interest in
. irnproving tirei:: facial ancJ clental appeariurce.ll
Foi: th e pre'tre il tm eut cepha i omelri c: ilirarnetet'il' tht
sLlrger:i grouT] hlcl i sicnifirtitttif ilrrget: lrosierior taci;rl
ir*igirt at:cl a s;lallei" intr:rjtrt'i*oii:ie angie. Tiiui;, coir$iil
ering tlte .,rerLjcal .iav,,-lust* r eiationship. ther surgcri'
sarbjects irad slir,lirtl1' l:etter ilt'etre,lttnlsnt cq:nditionl; I oi'
Ciasri I] cone.:riur t irari did ti ie Herbst subtects.lr '2' i i l l '
firt i-rthel" lil:lnr! tirt vri rts rrrpl'll-isal anci tirc soi'i tiril;tt':prcfi I e con -r,ex ii-rt i nc i r-i d i n g th e tros'-. \,vere :li gni ii canti "v
iiitrrs;.' in thr:, tilii:t*:i.ri iii ollri" Therei'r:rc. il'om tir* i;;t'Jlf"t.ili
discrepanclt point oi' vierv" tire surgery group haci
siightiy more $evers pretreatntent conditions.
Ali subiects iri both groups were treated success-
fully 16 a Class I ccclusal relatiqlnship, The amount of
overiet reducrion was greatest in the F{erbst subjects'
Tiris was true when ccrnpariuti groill:l {lvsrase$ and
lcloiting at the ma,tinturn irrdir.'idual overiei recluciiot-t"
Protiiit et" 'aj.zi stated that orttrodontic'ireatment was
likei'1t tcl faii {even in aclolescents wl'reri growth assists
Ciass; tr] correcticin) if thr. or.'erjet exceeds l0 mnr" Irt our
Ftrer'bst sarnpie-" itorarever. iarger over-iet reclucrions(n:ra-xirnun: reduc'fion, iZ.2 rutn] were fourld. ,/tverage
overbite i'eciuctici, rlsr.r wal; iitrgel-il.; ti-lt: Hsrbst than in
thr: surge.r\/ grouJ:1. wirereas Clnsll nI n:olar t:on'ectiori
\r/as, {}n ilveri}ge" siiuhlii, trture t:rclnouncecl in tire
i ;ur l ' , i f \ r gtouE.
Even l.li'.ruglh Ciaili; Ii correciion \iilllll very liuccessfiti
irr tlr.e trieri;st patienrs, tir* meciranilint trsi.rind it w;tl;
ciiff'erenr ft'r;t-tt thar irr tfrt 'oalients t;:eared rvilli ortirci.li*
rS"0 nrrn I8{t 9'r{,1-$ r'nnr / }2 "tt,
5.0 rnm / J{} %3.? mnr /78 %

OverjetSurgeryDecrease 6-3 mm#
American Journal of Orthodontics and Dentofacia:I. Onhopedics
Volume L76. Ntnnber 2
Meilar nelation$urgery
Ruf and Pancherz '147
Overbite$urgeryDecrease 2.1 mm
.-
Surgery
SI\IE
l-lerbst
dggrees
Anterior facial height
lndex
Profile Gonvexity excl. NoseSurgery Herbst
opposite was the case. This finding agrees with previ-ous studies comparing tire trearrnent effects of ortho-dontics and orthog4athic surgery in adulm.17'2r
The most profound difference between the surgery
10-q .
0
-5
-10
- t c
Normalisation 5.0 mm*Y[-lerbstNormaiisaticln 4.f mm'
$r,;I
fi$
1[
bU
50
40
degrees 30
2A
10
0
tr Before!lAfter
ML/NSL
$urgery .Herbstlncrease 3.J degrees *
Posterior facial
$urgeryDecrease 2i0 *
height
HerbstIncrease 1.0 *
deorees
Fig 4. lndividual treatment changes of overjeto overbite, molar relation, SNB angle, MIJNSL angle,anterior facial height, posterior facial height, and profile convexity excluding nose in 46 Class llDivision 1 adults treated with orlhognathic surgery (mandibular sagittal split osteotomy)followed bymultibracket appliances and 23 Class ll Division 1 adults treated with Herbst appliances followed bymultibracket appliances.
natiric surgery. Botli the standard cephaiometric recordsand the SO anaiysis showed that the Class II malocclu-sions in the Herbst subjects were corrected by dentainrore than skeletal changes; in the surgery subjects, the
increase 2.1 degrees
HerbstIncrease 0.4 *
Decrease 5.5 degrees * Decrease 3.1 degrees *

'l4P' lluf untl tr'crncheri. Atnt:ricun ,lournul- ttl' Orl.hrxlttttti.r:,s' aml Dcntofhcial Ortlmperiics
Ar'tgttst 2004
Tahte V. MaxirrrLlit individual cepfi it lomctricr treiltnrent chitnges antl
i l ; l i Cl:.rss Il Divisiorr I suh.iccls treiltctl with .rt irognitthic sutgery
ir\, nrLrlt ibftrcl<et appli:,rnce uri.t :: i"rch-rlf class [l Divisiorr I srrlr. iects
niuI t ibrrc l tet rPPl i lnce
cottsist.ency ol ' trelrtnretr l clr l trr :e:; (%') in 46
(nranc l ibu lar l ;ag i t t t r l sp l i t os lc( ) lo tny) f t l l lo rved
treuteci wit l i l - ter lrst l rppl i iuice f i i l lowed iry
T' r c r r| n t r:n.l c h t.t tr 11 c's ( u.!i r r- I t t:t.l r t rt )
. lrrrgrt-r,
lvf uximunt Ottttsi ' lcnr| cl i '
I i erl,sl
A4 a.r.i ttt.ttttt. Cirlrsi,rlr:rtrt' 7oVu'iultlc
lncisor relation
Molru- relatit:t1"'
Slgittnl iaw reii lt ir)n
Veriical jaur rciaiiorl
F:rcirl heiglr
Proflle c0nvcxlty
Over- iet ( rnmi
C)verbi ie imm)
trrnr )l ; t ' l l . ] ( " )
Ar l ' l l , ] ( " )
Mt- /h ls l , ( " )
i ipir-( irr >i I(X)/1{-ilr-r (iLrtjcx)
fipp-Co' X 1(X)/:i-Go' i irrdex)
N A P g ( ' )
t . lS/Sn/ I 'gS (")
NS/NoiPgS ( ' )
I I ? t- t t - / . r
-9.5t)- 16 . (x )
-)./-)/ j . l {
- " . ) . - - j
1 1 . 7 54 .5 t )
* i 1 . s 012"(X)t1 .509.75
!) lir) l.i
I'J( l t
r),q
9 lr ) -l i /
t o
Q 1
96^76
* 13.15-Cr.15-(r.'f"5
2.71t* 3 . (X )-2.15
t . r i53 .1 : izl 7' :
7.504.fi)
l ( x )96
l ( x )
14
5fr5:l()^ )7(i9fi
rt3
' l 'mi l lus ( - ) i rnpi ies nt tnnal iz i t t i t t t t
Fig 5. A,, Pretreatment and E, posttreatment lateral
headfilms of 33-year-old fernale surgery subject {man-dibular sagittal split osteotorny).
and the F{erbst subjects was the sreater manciihr-rlar base
advancement (SNB, SNPg, Fg/OLp), resulting in iarger
recluctions of tire ANB urgie, tire Wits appruisal, and
the skeletai apd so{'t tissue profile convexities in tlre'
surgery group. The greater upper lip retrusion in tire
surgerJv group was nost lil<ely ciue to the iarger lTtitn-
dibgiar-'nirsr,. lcivancenrent i i i those subiects. i\s a result
of the marreiibuial' aclvanceruent. tire reference line
(estl ietic l ine) alrLornatically became lnore rnleriorlv
positiorred. thus r:esultirrg iri a lelative l ip retrLtsiou"
Otlrer nraricecl dif ier:ences iretween tire 2 trsatmenl
gl'oltp:i were tire direction irr changell ofthe mapdibr1iar
plane ;ngie lncl posterior faciai height. Althpggir.a
ioro.1 incrcase in poste.rior faciai heigirt tiritrr in anterior
Fig 6. A, Pretreatnrent andheadfilms of 22-Year-old maleular sagittal sPlit osteotomY)'
B, posttreatment lateralsurgery subiect (mandib-
faciai height (resulting in a reduction in tire mandibr-rlar
piane erngle) was notecl in the Herbst group, the oppo-
site was tme in tlre surgery group. Becattse the pretleat-
ment rnaurciibuiar piane angle tlf the surgery group wils
nclrmal.s(' tlre irlcrease in the anqie flIust be consiclered
unfavorable in Ciass ll treatment' The urguiar increase
in the sursel-Jl subjects was most' probabllr duc' tc bone
renrocieling in the gonion alea. Tiris renrodeling hts
Lreen showri to continue io*g atter surg ary.2tt^=' Possibie
Cslsefi are &n iirnciecluate overiap L-retwee.n the 2 $onv
fr-agmelts 3t the lime o1'surgety.?oi'"" the pal'tial deracir-
ntent cl{' the eievntor muscles fi"om the gonion area
(operarion accoreiing r() obwegeser/Dal Por-rt oniy) and
their sulisequent reattacirment arrd arJaptatiott.zT tl"re

A mericun. I ou.mal. oJ' O rtltodr nt ics und D ent ofacial O rthop e tl icsVolume 126. Nu.ntber 2
FiE 7" A, Pretreatment and B, posttreatment laterallreadfilms of 19-year-old female Herbst subiect.
general postsurgical adaptive processes of all softti$r;uer;, tenrlons, imc\ muscles that hrve been directiy orindirectly af{tctecl 'Lry the surgical .in* clisplace-ment,??'30'31 ancl the possible conclyieu resorption thathus treen reportecl rather trequently in orthognatiricsurgeqr patients,lT'27 especially in tlrose with a pretreat-nrent internal derangement of the TMJ.32
The clirection of maxillary nrolar movements dif-ferecl between the 2 treatment groups. Although thedistal movement of the maxiliary nroliu in the Flerbstgroup was to be expected frorn tl-re lreadgear effect oftire appliance,33 the mesial movement of the maxillarymolars in tlre surgery group was unexpectecl because allsubjects were treated nonextraction. Even.if decreases.in maxillary and mandibular arch lengths in aclulthoodoccur;3a the amourrts of change in the surgery subjectswere lar:ger than tirose normally reporteci to occur over1 decade. A possible explanation for tlre mesial move-ment oi the maxill.ary molars is a transverse maxiliaryexpansion most iilcely perfonned in mosl. of the patientsduring the presurgical ortlrocioi:rtic phase. The spacegained by tlris expansion might have been reciprocaliyciosecl, leacling to the observecl retrusion of the muil-lary incison; ( 1.4 mrn) ancl the mesial movement of thernaxillury nrolars (0.7 rnm)
The con.sistency in treatment reaction was larger forthe surgery group than for the Herbst group foi vari-abies clirectly or inciirectly affectecl by.the amonnt ofrnandibuiar acivancement (SNB, ANB, skel.etal profileconvexity). On tlre other hanci, the rerluctio' i' softtissue profi'le convexity exch-rciing the nose was thesame (96To) in both groups, whereas, for the recluctionof the sofi ris;s;ue profi ie convexity inciuding tire nose,the consistencv was larger in the Herbsi subiects.Fufiirernrc,re. io, tire Ciass II c'nective variables (over-Jsl' overbite. nraiar relationship), no marl<ed group
Rul'and. Pan.cherz 149
Fig 8. A, Pretreatment and ts, posttreatment lateralheadfilms of 2O-year-old male Herbst subject.
differences were d.etected. Therefore, the predictabilityof the tr:eatment outconre in Lernrs of consislency ofclrmges waso on average, comparable ior both grclups.This agrees with the findings of Tulloch et al,:r-s whoconcluded that the success rarte of overjet reducticln wasonly slightly higher for orthodontic thzur fbr sr,rrgicalfreatnren.t inespective of age and malocclusion severity.
Thus,.the question arrises which is ttre best treatmentrnodaiity for a borderiine Class II adul.t. Even when theknowledge fiom this study is aclded to what is luownfrorn the iiterature,'there seems to be no single, con-clusive answer to tlie question. Several factors must beconsidered in the treatment decision process: (1) thereason the patient is seeking treatment; (2) the effectstirat can be provided by Flerbst tleatrnent iurd ortho-gnathic surgery, respectively; and (3) the costs andrisks of the 2 treatlnent approaches.
There is agreement in the literature that the mainreasons for adr-rlts seeking treatment are dentai andfacial esthetics as well as stomatognathic or functionalimprovement.3G3s Patients with severe skeletal Ciass Ilmalocciusions are more motivated to undergo ortho.dontic tlran surgical treatment.3s This is not surprisingbecause most people prefer the least invasive measLlreto solve their problems. Interestingly, the type offieatment selected (surgery or orthodontics) dependsrnainly on tl're sub-iect's self-perception of his.or herfacial profiie and is not associated with the clegree ofdentoslieletal discrepan.cy. This means that the nroredissatisfied tlre patients are with tireir facial esthetics.the more lihely they are to choose surgery..e'au FIow-ever. after treatfftent, surgical and clrthodontic patientswere, equally satisfiecl rvith their profile changes.lT.?o
In our stud5r. iarger reductions in profile convexitywere found in tire ryrrgery/ group tiran in the Herirstgrolrp. In contrast. Strell and V{ooclsal found that.

i50 lluJ' arul Pctnch'ery,
reg:rrcliess o1' wftetfrer Cllss II pilt iell ls were trealed
r,vith growtlr mOclif icnlion clr-rring tclolesccnce oI oI-
thggrr:.rthic siLlrgery cir-rripg lrlull.ir11gcl. l'acial estiretics
irnplrvecl to n sin'ri i lr exten[. Furtlternrore. thcr reduc*
rion in la.cial pr.i i ie: cr>nver.it.y ucli ievecl lry [-lcrbst
trcit l l l l .cIt secnll i r]ot to hc ase-clepetrtlcnL''
Even if, t lre Occlrrsiotl ci-rr. l be cttrlectetl vcry st-lc*
cessl'r-rlly lry acir-rlt FIerbst. treilf ll}cpt, chilr prtrjeciign tnd
tirr-rs {ircial elit.helics nrighL lre trtit be optirnll l1'ter
tl ieri lp5u. It, lrowcver, chin prornincnce is the rtit irt
i rpt f ler l lgr I l rc pir t icnl . i t r lv l tncentenf ; lerr i< lp lasty oi-
I 'e[1l lt lr:ss col;ty.. lcss risltf i t l lcrnaLivel { 'o enhil l.tcc l ' l tci;"t l'
esthet.ici l t iran I m"rLrti i$uiitr si iuit.t,al siri i t l i l i tctt l.t lmy.'12'-l: '
Ever r tlrOr-tgh t;tg rn it tggtti-ttfri c: t lr- l'rt t tcli tltrl,tl i nrprovel*
nrf,nt iS the tit':ct.lntJ trtosl ii'eC1r-rcnt rcilf;Clll l'clr ltciults ltt
ssgii {.1erturent. tittie is i<nown airr;ut tlre changes in
masticil()ry i'uncl.icln aftel ortlroguitthic surgery- FOr
Cl.nss III pafients, scientific di.ita sirow n1r siglificant
improvemerit irr p'stciperative rnasticatory futicl ion-ilJ
For Class Ii patients, tltr tire otirer lrirnd" at leasl. tcl our
iint-rwleclge. il() such data exist.
Altirougir there is controversy about the effbct of
orthgglntiric surgery on TM.I functiol, recent dataas
seem to sLrpp6rt the view tiri'rt patients v'rith pr:eexisting
articglar clisc dis'placeprents ulciergoing mandibulal
acivancement, surgery are iil<eiy to irave a significant
worsening oF the TMJ dysfnnction problenr postsuf-
gery. No comparabie dain exist for ildult }ierbst treat-
rnent. H.owever. in a group of Herbst sLibjects that
inciuclecl B of the present adults, Tt\4J function was
founcl to improve during treatment'46
when iooi<ing at the costs of combirred orthodon-
tic-orthognathic surgery treatment , 60Vo-7 5Vo are due to
tle surgicirl pilrt.'t7-4" Tirerel'ore, a remaricable cost
recluction in aciult Ciass II treatrnent can be achieved
with tire Herbst appliance instead of orthognatiric sur-
gery.The most comrnon surgical rislc of rnandibular
advancement is neurosensory ciisrurbances of the iower
lip th.rt afiect abcrut 507c cif the sr-rbjects.S0 Acidition-
aliv. nonunion or mal-union of the Lrtiny fritgrnents, bad
,piitr,t' a'cl conclylar resorptionlT'3? are lrecluent conr-
piicatiols" Even if neurosensoly disturblpcel; o{'the i ip
,r""u, atter geni.oplilsty alOne, the prevalence is signif-
icantly lower thap r,vith nanclilrular slgittal spiit or a
con'rbination of sagittal spiit anci gerricipiastr''s2
A nrain conrplicatior: in orthOdonticl; is root resotp-
tiol. Tire anrount t-ll r"oot rssolption has been for-rnd to
conelate 1vitir the rlllOulll ol' rlverjef reciuctiolr lnci
i lorizontal tooth movement.5s Furthermore. extensive
paiaral root rorque. wirich is likeil, to be appiied during
orthcldontic Ciass I] treatment, irei; beeu sirown to be iL
preclisposing factor for root resolption of the mandiL'-
A nte ric un'l o ttrnul, of' ( ) rt lw d rsnl it: s ttn d I) e nttlfucirtl O rt lwpedicsAugtrst 2004
ulai ' i t tcisors-sa Tirus, wiren compitr ing sl lrgery i tnd
tlentgl 'aciui oltht ipedics (Herbs{ rpJrl i :rnce), t l -re r isl ts
associated ' ,viLh sulrgery i l re ohvit lusly much greit ter '
Final ly, the fai iure 'ato oi j sr.rrgici t l Ciass I l trertnrenl is
higircr t frarr thut l i l r l clentoi ' tcial t l r thopecl ic/ort lrorion-
t ic : lppro: rch. r ' ' The lc l 'o re . ' t l re inrpor t rn t q t les t io l ] in
t l .ei l t l lent pl lrrrni lru, ir ; wlrefhcr thu srcatcr i t trprt lvet i lcnt
in l 'aci i t l est irel- i f i ; accOmpiislrecl by oi l l r t-rgnit t l i ic sur-
g,ery L:otltp:lrecl with clentol'acial OrLiropeciic$ witlr the
FIeri :sf. appi iapce is; wtlr l i r l i re increltsecl cclsts and r isl<-s
o1' t .he, surgiclr l aPProirch-
f,cltvGN-[.isl0i{s
The Fierbr;l. ailpiiar]ce iir apgweti't-tl [Oql {i:r nonsur--
gical. nonextractiorr Lrentl lenl of atlLrlt ciass I.[ rnaloc-
cinsions" Tirus, tfte trent,rrent apnrgach can be copl;id-
erecl as Lul alternltive t0 orthogrratiric sllrgery in
irordcrline slceletal Class U sr-rbjectr"s. For class Il
correction, tire succes$ rill.e ancl prcclictability of l-lerbst
treirtnent is as high as fur orthognatiric surgery. If,
however, the patient's maln wisir is it greirt ly improved
facirl protiie. ortirognathic surgery is the better treat-
ment all,ern:rtive.
we thank tlie crthognathic surg,ery Department in
Maimo, sweden, and f)rs witschel irnd wrede in Ead
Oeynhaul;en, Germany, tor providing access to the
clinical records ancl the iateral headfrlms of the surgery
subjects.
REFERENCES
1. Pancherz F[. Dentofacial orthopeclics ororthognathic surgery: is
it a nrntter of age? Am ] orthod Dentofacial orthop 2000;1i?:
5714 .
2. Pancirerz H. Ruf s. The flerbst appliirnce-researsir basetl
uptiarecl clinicai possibil it ies. worlti orthod J 2000:l:t7-:l l."
3. Ruf S, Pancherz FI. I{,iet'e.rgeienltwachstumsadaptittion bei jun-
gen Erwachsenen wiihrencl Behandlung mit der Herbst-Appara-
tur. Eine prospektive magnetrddonanztomographische und
kephllometrische studie. lnf orthocl lii eferortlrr:p I 998 :30 :735-
50.
4. Ruf S, I}mclrerz, F[. Dentoskeleta] effects and facial profiie
chituses itt vuung rtdulLs treated with the Herbst appliance' Angle
Orthod I 9!)9;69:23!l*46'
5. I{uf S^ Prncirerz Fl. Ten'rporonranclibular.ioint renocleling it i
acioles;cents and young adults during Herbst treal]llent: ir pf()spec-
tive lorr gi trrtl i nrl magnetic resr:nance im aging ancl cephalornetric
radiographic investigltion. Am J Orthtld Dentolaciirl orti lop
l l )99 \ ; l l 5 :6 { )7 - l t j .
6 . I t t r l . s . P l n c h e r z H . W h e n i s t i r e i d e a l p e r i o d i ' o r H e r b s ttlreraplr-elrly or Iate? Sentirr Orthod 2003;9:4?-56'
?, Mcj..l lnirra JA. Fetersttn JE,' Parrcherz H. I.l istoiogic: changes
Irss0ciatetl with tire Helbst tppliance in adu]t rhesris rnonicevs
t A4 uc tt c' r: tr nu'tLtrtt n\. Sem i n Orthocl 2()03 :9 :26-4t)'
l i . H l i g g U ' T n r a n g , . e r J . S ] c e l e r a l s i t a g e l r o i ' t i r e l r a n t l a n d w r i s t a s
intlisarors ol' tlie puirerttl srorvth spuri. Acta Odontol Scand
1980:3P,: l [ i7-200.

Anttt riccut,l ot.trnal of O rthod ontics ancl Dento.fac ia| 0 rthope tlic sVol.ume 126, Numher 2
RUJ'and Pancherz 151
',liii
ri;r, ,i'i,
.,,.1,';rll' ' i '
, , i i i r;,:::|''
', l:{l
9. HunsncliEE. A modified intrixlrirl sagittal splinting rechnique ftrrcorreclion of mandibular prognathism. J Oral Surg I9tr8;26:l-s0-3.
10.' Epher BN. Moclil ications in t.lre sugitnl osreotomy of the man-dible. .l Orrl Surg lc)77:35:157-9.
I l. Obwegeser H. The sursical con'ection of n:undibulxp progner-tl 'r isnr und retmgnutlrit witlr considerntion ol' genioplasty. OralSurg 1957 : l0 :677-89 .
12. Dtt Pont C, Retrontollr osteotonly 1'or the <.:orrection of prrrgn-rttlris^m. .l Orll Surg I9(rl ;19:42-7.
l3..Plncherz. H. The Herbst appliance. Sevilin, Spain: EditorialAguirunr; 1995.
14. B. i t i rk A. .Skic l ler V. ,Norml l nrrd lbnurmir l grorvth o1' thernandilrle. A syuthesis ol' longituclinnl cephllometric implantstudies over; r per iod o1'?5 years. Eur J Ort l r t ic l l t ) t l3 ;5: l -46-
15. Plnclrerz Fl. Tlre mechunism of Cllss ll corectit ln in Herbstlppli lncc tfeil l.rl-rcnt. A cephalonretric iuvestigirtion. Am J Ortll ldI 9t i2:u2: 104- I 3.
16. D.rhlberg G. Stntistic,al methocls lbr meclicirl ancl biologicalstudents. New York: lnterscience Publications; 1940,
17. Cmsidy DW, Hcrhosa EC, Rotskotf I(S, Johnston LE. Acomplrison ol' surgely and orthoclontics in "borderiine" adultswith Cltss II Division I nrulocciusions. Anr J Orthod DentofacialC)rtlrop I 993; I 04:455-70.
lB- Gerzirnic L, Jagsch R, Watziie lM. Psychologic implications ofortlrognathic surgery in pntients with skeletul Ciass II or Cierss tIInralocclusion. Int J Adult Orthod Orthognuth Surg 2002;lT:75-B t .
19. Lrwrence. TN, Ellis E, McNamara JA. The frequency andclistribution of slcdletal and dental cornponents in Class IIorthognathic surgery patients. J Oral Maxillofac Surg l9B5;43:^ f , - A/ + - \ 4
20- Mihtlih CA, Proffit WR, Phillips C. Long-rerrn follow-up ofCiass II adults treated with orthodontic camouflage: a compari-son with orthgnathic surgery outcomes. Am J Orthocl DentofircialOrthr:p 2003 : I 23 :?tr6-78.
2l- Proffit WR, Phill ips'C, Douvartziclis N. A comparison of'
outcomes o1'ortlrodontic and surgical-orthodontic treatment ofClass I[ malocclusion in adults. Am.l Orthod Dentofacial Orthon1992; l0 i :5-5(r-65.
22- Hoppenreijs TJ. Hakman EC, vanot Hof MA, Stoelinga pJ,
Tuinzing DB, Freiirofer HP. Psycirologic implications of surgicalorlhodontic, treirtment in patients with anterjor open bite. int JAdult Orthod Ortlrognath Surg 1999;14:101-12.
23. Hirzel HG. Grewe JM. Acrivators: a practical approach, Arn JOrtlrod 197 4',66:557 -7 0..
24. sltieller v, Bjiirlt A, Linde Hansen T. Precliction of mandibulargrowth rotntion evitluated from a longitudinal impiant sample.Am .l Orthod l9tl4:tt6:359-70.
25. Prol'f it WR. Phill ips C, Tulloch JFC, Medland pH. Surgicalversus orthockrntic correction of skeieul class II maiocclusion initdoler'^cents: efl'ects ancl indications. Int, J Atiult onhod orthoe-nnth Surg l9L)2:7 :ZAL) -.2A.
2b. Bathil Sti. Leightorr BC. A manual of facial growth. A computeritnrlysis of longiturlinal growth data. oxforci: oxforci universityPress; 1993.
27. Schubert P, Bailey I-TJ. WlriLe Rp. proffit WR. Long-rermcephrrlonretric clianues in untreatecl adults comparecl to thosetrearerl with orrliognathic surgery,. int J Adnlt Orthod OrthoenathSurg 1999 : t4 :91 -9 .
28. I(ohn MW. Analvsis of relapse after mandibulnr arlvancementr;Lrrgerv. .l Oral Surg l9TB;9:676_tt4.
29, L.r Blnnc. Jp, Turvev T. Epker BN, Hill C. Resulrs following
sinrultaneous nlrbil ization oI the maxilla anc] muhdible lor thecorrection of tjerrrtrtircial dei'ormities.'Ord Surs Ornl Med Or-alIr:rl"hol I 982:54:607- I 2.
30. Epker BN, Wessberg C. Mechanisnrs ol'early skeletal relapselollowing surgical udvancemerlt of the manclible. Br J OriLLl Surgl982:20: t7-5-82.
31. Turvey T, Phill ips C. Laytodn FlS, Protfir WR. Sinrultiulecrussuperior repositioning trl ' the nraxil la ancl rntndibulal advlnce-nrent. A report on sr.lhility. Arn .l C)rthorl .Denrollcial C)rthopl988: t )4:372-t i3.
32. Schetlhrs l(P, Piper MA, Bessetre RW, Will<es CH. Mandibularretrusion, tenrprlrumantlibultr joint clerangen-lcnt, and ortlrog-nathic surgcry plnnning. Plast Reconsn' .Srrrg 1992:90:21ti-2L).
33. Panclrerz H, Anehus Plncherz M. The heitclgear eflect of theHerhst. npplilnce: u cephLrionretric long-term .study. Am J Ort.hodDentoiacial Orttrop I 993; I 03:5 l0-20.
34. Akgtil AA, ToygarTU. Nmturul craniofacial changes in the thirddecnde of lilb: a longitudinal stncly. Am J Ortlrocl DenrofacialOrthop 2002: t22:5 12-23.
35. Tulkrch JFC, Lenz BE, Phili ips C: Surgicll versus orthoclonticcorrection ibr Class II patients: age and severity in lre{rtmentplmning lnd trentnrent outconre. Semin Ortlrod 1999;5:13t-40.
36. Flanary.CM. Bnrnwell CM, Alexander JM. Fatients' perceptionso1'ortlrognatl 'ric suryery. Am J Orthod l9B5:88:13't-45.
37. Mayo I(H, Dryland-Vig I(WL, Vig PS, I(t:walski CJ. Atrituclevariabies of dentofacial deforrnity patienls: denrographic chnrac-
. teristics and msociations. J Oral Maxiliofac Surg l99l;49:594602.
38. Wilmot JJ, Barber HD, Chou DG, Vig KWL. Associationsbetween severity of dentofacial defbrmity and motivation forortlrodontic-ortlrognathic surgery rrearment. Angle Orthocl I 993 I63:283-8.
39. Bell R, Kiyak HA, Joondeph DR, McNeill.RW. Wallen TR.Perceptions of facial proiiie and their influence on the decision toundergo orrhosn[thic surgery. Anr J Orthod 1985;88:37j-3?.. -
40. I$ynt HA, McNeill RW, West RA. Hohl T. Heaton PJ. Person-ality characteri$tics as predictors imd sequale of surgical andconventinnal ortlrodontics. Am J Ortirod t986:89:383-92.
41. Shell TL, Woocls WG. Perception of facial esthetics: t compar-ison o1' similar Class II cases treated with attempred grofihmodification or iater orthognzrthic surgery. Angle Orthoci 2003173:365-73.
42. Brons R. Chin corrections. In: Brons li,i'erlitor.'Facial harmony.Standards for orthognathic surgery and orthociontics. Lontlou:
Quintessence; 1998. 145-58.
43. Profirt WR. Turvey T, Moriarly JD. Augmentation genioplasty asan adiunct to conservative orthodontic trearment. Am J Orthod79111;79:473-91.
44. Shiratsuchi Y, Itouno K, Ta.shiro H. Evaluation of masticatoryfunction tbllowing orthognathic surgicli correction ol' manciibu-lar prognathism.. l Cranio Max Fac Surg 1991;19:299-303.
45. Wolfbrd LM" Reiche-Fisclrel O, Pushl<ar M, Chirnges in tem-poronundibular .ioint dysfuncrion ai'ter ortirognathic surgery.J Oral lr4axil lofac Surg 2003:61:65_5-60.
46. Ru{' S. Pancherz H. Does bite-jurnping damage the TM.I? Aprospective Iongitudinal ciinical uncl MRI srucJy of Herbsr. pa-tients. Angle Ortirod 2000:70: I 83-99.
47. Dolan P, White RP, Tullocli JFC. An anaiysis of hospital clrarge.sfor orthognathic sur$ery. int .i Adult Orthod Orthognath Sr.rrg1987 :1 :9 - | 4 .
'.ali[;.
r ; t i. l i . i i

152 llrd' r.utd I'unc:het7,
4S. I,urrula Ir., l(crslti-Nisrria L. ltc:ski-lri isLrll lt. Oilt lririen ](. l(cr;lt i-
I ' l i s r r l l r 5 i . C ' r r l ; r i l o { ' s t r rg i cu l -o r l i i o t l r l r r { i c l r ' c : t t l t t u t l t i n c t l t t r tT r t t r t i t y
i rospi ta l c i l l 'c : u l l lnulvs i r ; o l thc c l i t ' i 'c lc t r t l r l t l t t ;e l o i ' l t 'e l t t t t renl . l t t l
.1. At l t r I I ( ) r l l io t l C)r l l tognath Srrrg 2(X)2: I7: f ( )7- .1(Xr.
49. ' l ' lroni:-ul l)N4. Or-t.hotlrl ltt it: clltrtt ltt l l l t!,c vefiit l l i ttrl-httgnll it ic r;ur-
gcr \ / in thc t r r - :utr lc l t t o l nr ,urrd i tur la l t lc l ic icncv. J ( t r l l Mi tx i l lo f l tc
Sr r rg l ' r r r5 , . ; -1 ;57 t r - l i ? .
5U. I i i -y ; r l l - l i . r " l lc l l l t . l r l ivc:htrsociu l uorrr ; ic lqnrt iu l r l ; i r r surgcry tnd
or lhot lo l r l i * ; . ln : l ) r r r l ' f i t Wl l l . l4 l l r r tc l l [ ] ' . , c t l i l t l r : ; . ! iurg icnl-or{ l to-
rkrtrl. i ct t t 'LltlLt ) tct l L.,ti;r in l l-oui r;: IVItrr;h17 ; l qq(). 7q-8{).
5 i. P;lnuiu I ',1, (ti l ialrrrcti tri. Fit-rrte i ' i .. ltrcirJcnco c;1' cti l-t:piicttionl; iutti
Antt:ritttri. J<ltnzal r4f'Orthgdontics tuu! Ilentilittial. ()rlhopcr.li.t:,r^
Attl4ust 2004
pnrtrlcmli rcrlutecl to ot't lrogttitthic sttrgcrv: lr rsvjew o1 655
p i r t i e r r t l ; . . l O r i r l N4 l r x i l l o l ' r u : S ru 'g 2 {X) I : I ( . } : I I l l i - : 17 .
Ci i ; rnni AR. 13ig l io i i F, lJozzet t i A. Br l r r ; r r t i I i . NcLrror is l l r i { ) r 'y
I t l tcr ; , r l - ionl i o l ' lhc rn lcr- i t r r l t lveolar rnt l r l rCnt ; t l l tervc . ; t l t .et gc-nio-
pIsty l r lgnc 6r ' t tssoci t t lec l wi t l r s : rg i t tu l ( ) l i tc() to l . l ly t i l the t r t l tn-
t.l i bLtlrr ri lnrtui. . l (lrirn i ortrltx i l lol lrc Surg 2( X)1:30:2tt5-1103'
Slr r re: i l r i rn: r CT, l l inc l r r i r r l : 'N4, Prct l ic t i r rg I rnt l prcvcnt ing r t lnt
rcsr l rpt iun. l , I r i i rgnrrr ; t ic l l . rc lot :s. Ant . l [ t r t l r tx l Dert to l t tc iu l
t ) r ' l l r op 2 (X l l : I l 9 :50 ' i - l ( ) .
5. i . h r r l cy . l . I ) i r i l i i q l ; C . l iac io t ' r ; re l l r t cd t ( ] ] ' ( i ( ) l resorJ r l i t t l r i r t t l t c
orthotionl ic pt ' l t : t ice. Arrgle {}r{Iori [1]9! : i r i : l?5-32.
5L
53 .
ru tr#dffi ffitrffiwffiffDon't nriss a singie issue of the iournal! To ensure prompt service when you change your address, please
photocopy irnd compiete the forrn be]ow-
F1ease seftd your clrcmge of acklless notifrc.s,tion at least six weeks before yoar nxove to ensu.Ye conti.rcued ser-
vir,r,. Wr: rcsre-t we caruxot guarante{ | eplecewteilt of isswes nfissed d.ue tu late notiiication"Y M .
JOUIT.NAL TETLH,:Fill in the title of the journal here.
ox,D aDsltE$s:.d,ffix the address iabel from a recenl issue oi the joumal irere.
E N D IY Til U A[. S TilJS Cft "Tff EI,ISCOn:'l' AI\II) I\4AIX- T[-I[S FO[i.h{ T]Ct:Elsevier Inc.Subscriptiot] Customer,S ervice627? Sea Fiartror DrOrlaniio. FL 32FiU7
NFJW AI}DTTESS:Cieruly print vour nr.w adriress ircre.
j,,larne
Address
City/5lete/ZIF
cR. Floli Tc:407-363-9ir61
SR. E-M.AiIE :eispost@eisevier. com
OIT FFtrOi,iE:800-654-2451Outside tirs {.J.S., cttii407-345-4{XXj