Embed Size (px)
Citation preview

Hindawi Publishing CorporationBioMed Research InternationalVolume 2013 Article ID 971096 6 pageshttpdxdoiorg1011552013971096
Clinical StudyEfficacy and Safety of Docetaxel Plus Oxaliplatin andCapecitabine in the First Line Treatment of AdvancedGastric Adenocarcinoma
Ying Liu1 Zhengbao Ye1 Wenqi Xi1 Tao Ma1 Min Shi12 Liu Yang1
Zhenggang Zhu12 and Jun Zhang12
1 Department of Surgery Ruijin Hospital Shanghai Jiaotong University School of Medicine No 197 Ruijin er RoadShanghai 200025 China
2 Shanghai Institute of Digestive Surgery Ruijin Hospital Shanghai Jiaotong University School of Medicine No 197 Ruijin er RoadShanghai 200025 China
Correspondence should be addressed to Zhenggang Zhu zzg1954hotmailcom and Jun Zhang jun zj10977163com
Received 29 April 2013 Revised 20 July 2013 Accepted 16 August 2013
Academic Editor Izumi Takeyoshi
Copyright copy 2013 Ying Liu et alThis is an open access article distributed under the Creative Commons Attribution License whichpermits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Objective To evaluate the efficacy and safety of docetaxel plus oxaliplatin and capecitabine (DOX) in the first line treatment ofadvanced gastric adenocarcinoma Methods A total of 37 patients were enrolled into this study and they received DOX regimen(docetaxel 75mgm2 and oxaliplatin 130mgm2 intravenous infusion on day 1 and capecitabine 1000mgm2 orally twice dailyon d1ndash14) treatment was repeated every 3 weeks Results All 37 patients were assessable for evaluation The numbers of patientswith complete response (CR) partial responses (PR) stable disease (SD) and progressive disease (PD) were 1 10 23 and 3respectively The objective response rate (ORR) was 297 with the disease control rate (DCR) of 919 Median progression-free survival (mPFS) and overall survival (mOS) were 197 days and 364 days respectively The most common grade 34 toxicitieswere hematological toxicities The most common grade 34 nonhematological toxicities were fatigue nausea vomiting anorexiadiarrhea and hand-foot syndrome Conclusion The DOX regimen demonstrated a promising efficacy as the first line regimen intreating advanced gastric cancer patients with good performance status the toxicities were tolerated and controllable Large-scaleclinical observation is necessary to get further evidence
1 Background
Gastric cancer is the second most common cause of cancer-related deaths worldwide The outcome of advanced gastriccancer patients is poor and the median survival time ofuntreated patients is less than 6 months [1] A numberof randomized clinical trials have established the role ofchemotherapy in the treatment of patients with advancedgastric cancer Compared with those in best support care(BSC) group the median survival time in chemotherapygroups was longer (75ndash12 months versus 3ndash5 months) Theimprovement of median overall survival after chemotherapywas significant in three of the four previously reported
studies [2ndash5] Formany years 5-fluorouracil plus cisplatin hasbeen considered as the backbone doublet regimen In somecountries anthracyclin is added to form triplet regimen suchas epirubicin cisplatin and continuous-infusion 5-FU (ECF)
During the past decade several new agents have emergedincluding taxanes (paclitaxel docetaxel) topoisomerase-Iinhibitor irinotecan and third-generation platinum deriva-tive oxaliplatin which provided more effective and bettertolerated regimens in treating this life-threatening disease
Although taxanes share a number of pharmacologiccharacteristics and similar mechanisms of action (tubulinstabilization and cell cycle arrest) they are distinctly differentDocetaxel demonstrated greater affinity for tubulin longer
2 BioMed Research International
plasma half-life and intracellular retention time than pacli-taxel In addition the taxanes exhibit different profiles ofdrug resistance [6ndash10] Docetaxel has shown activity againstgastric cancer either as single agent or in combination withother agents The results of the V325 trial confirmed thesurvival benefit and acceptable toxicities of adding doc-etaxel to cisplatin and fluorouracil in treating advanced ormetastatic gastric cancer [11] Based on the results of this trialdocetaxel was approved by the FDA in 2006 in combinationwith 5-FU and cisplatin for advanced or metastatic gastricadenocarcinoma
Oral fluoropyrimidine agents such as capecitabine andS-1 may provide an alternative to standard infusional 5-FUCunningham et al [12] addressed the results of randomizedphase III trial REAL-2 It was a 2 plus 2 factorial designbased on the standard European triplet regimen ECF Theoverall survival of EOX group which contains two newcytotoxic agents (oxaliplatin and capecitabine) reached 112months and significantly longer than those in other groupsThe results of REAL-2 study indicated that oxaliplatin wasmore noninferior than cisplatin and capecitabine was morenoninferior than infusional 5-FU in the first line treatment ofadvanced and metastatic gastric or gastroesophageal cancer
Based upon the results of V-325 and REAL-2 studies wedesign this single armphase II study to evaluate the safety andefficacy of DOX (docetaxel oxaliplatin capecitabine) regi-men in treating unresectable locally advanced or metastaticgastric cancer
2 Methods
21 Patients Characteristics The main eligibility criteriaincluded (1) age 18ndash75 yrs (2) histologically proven gastricadenocarcinoma (3) measurable andor evaluable targetedlesion according to RECIST criteria (version 10) (4) goodperformance status with the Eastern Cooperative OncologyGroup (ECOG) score of 0ndash2 (5) no prior chemotherapy and(6) adequate hepatic renal and hematological function
Exclusion criteria included (1) concomitant cancers(except melanoma skin cancer and carcinoma in situ ofcervix) (2) neuropathy brain or leptomeningeal involve-ment (3) uncontrolled significant comorbid conditions (4)patient could not comprehend the purpose of the study andcould not comply with the protocol and (5) womenwhowerepregnant or breastfeeding The Ethics Committee at RuijinHospital affiliated to Shanghai Jiaotong University School ofMedicine approved the study and written informed consentwas obtained
22 Treatments Docetaxel 75mgm2 was give intravenousinfusion for 2 hours on day 1 oxaliplatin 130mgm2 was alsointravenous infusion for 2 hours on day 1 and capecitabine1000mgm2 were orally intaked twice daily on d1ndash14 Theregimen was repeated every 3 weeksThe dosage of docetaxelwas referred from TAX 325 trial the dosages of oxaliplatinand capecitabine were referred from REAL-2 and ML17032trials Only those who completed at least 2 cycles were
assessed efficacy Patients who finished all 8 cycles of treat-ment without disease progression were turned into follow-upperiod
23 Evaluation and Outcomes Before entering the study allpatients received physical examination full blood count andserum chemistry analyses Chest X-ray ECG upper gas-trointestinal endoscopies abdominal computer tomographic(CT) scans and other appropriate procedures were alsoperformed as needed During treatment full blood count andserum chemistry analyses were conducted before each cycleand X-ray and CT scans were conducted every two cyclesAfter the treatment completed patients were receiving theseevaluations every 2 months PFS (progression-free survival)was defined from the day of enrollment to first evidence ofdisease progression or death occurring within 12 weeks ofthe last assessable tumor assessment OS (overall survival)was defined from the date of enrollment to death from anycause DCR (disease control rate) was defined as followscomplete response (CR) + partial response (PR) + stabledisease (SD)all enrolled patients Responses were evaluatedaccording to RECIST criteria (version 10) Toxicities weregraded according to the National Cancer Institute of CanadaCommon Toxicity Criteria (version 10) The primary end-point of this study was response rates (RR) The secondaryendpoints were PFS OS DCR and the toxicity profilePatients were considered assessable for response if theyreceived at least two cycles of chemotherapy Safety analysesincluded all treated patients and involved the analysis oftreatment-emergent adverse events
24 Statistical Analysis The statistical analysis was carriedout using SPSS software (version 130 SPSS Chicago ILUSA) Descriptive statistics were used for safety evaluationORR and DCR and their two-sided 95 confidence interval(CI) were calculated PFS and OS were estimated usingKaplan-Meier method and their medians along with two-sided 95 CIs were calculated
3 Results
31 Patients and Treatment Characteristics A total of 37 latestage gastric cancer patients were enrolled from April 2007to April 2013 The demographics and baseline characteristicsof these patients are presented in Table 1 The median age ofthese patients was 48 (range 27ndash72) All patients had goodperformance status andwith ECOGperformance status scoreof 0 Twenty-five patients were confirmed pathologically aspoorly differentiated (including signet ring and mucinouscarcinoma) 2 patients were moderately differentiated andthe other 10 patients were confirmed as well-differentiatedadenocarcinoma Thirty-one patients had multimetastaticlesions and the other 6 had locally advanced diseases
32 Overall Response and Survival The median number oftreatment cycles was six ranging from one to eight withthe total cycles of 216 According to the RECIST criteria(version 10) CR was observed in one patient while PR was
BioMed Research International 3
10
08
06
04
02
00
0 500 1000 1500 2000 2500
Progression-free survivalOverall survival
Cum
surv
ival
Time
Figure 1 Kaplan-Meier curves of progression-free survival (PFS197 days) and overall survival (OS 364 days) of DOX regimen
observed in 10 patients SD was in 23 patients and PD in 3patients The ORR was 297 (95 CI 15ndash444) whileDCR was 919 (95 CI 839ndash99) Median progression-free survival (mPFS) and overall survival (mOS) time were197 days (95 CI 138ndash255 days) and 364 days (95 CI 255ndash472 days) respectively (Figure 1)
33 Toxicities The most common grade 34 toxicities werehematological toxicities The percentages of patients withgrade 34 leucopenia neutropenia and febrile neutropeniawere 378 378 and 108 respectivelyThemost commongrade 34 nonhematological toxicities were fatigue nau-sea vomiting anorexia diarrhea and hand-foot syndromewith the percentages of 270 54 54 81 27 and81 accordingly No severe liver or renal dysfunction orchemotherapy-related death was observed Only one patientdeveloped grade 2 peripheral neuropathy (Table 2)
34 Dose Reduction Patients who developed grade 4 hema-tological toxicities or grade 3 nonhematological toxicitiesreceived a 20 dosage reduction Among all enrolledpatients 13 had one time dose reduction (docetaxel andoxalipatin were 80 of the initial dose) and other 3 patientsgot one dose reduction of capecitabine owing to grade 3 hand-foot syndrome
4 Discussion
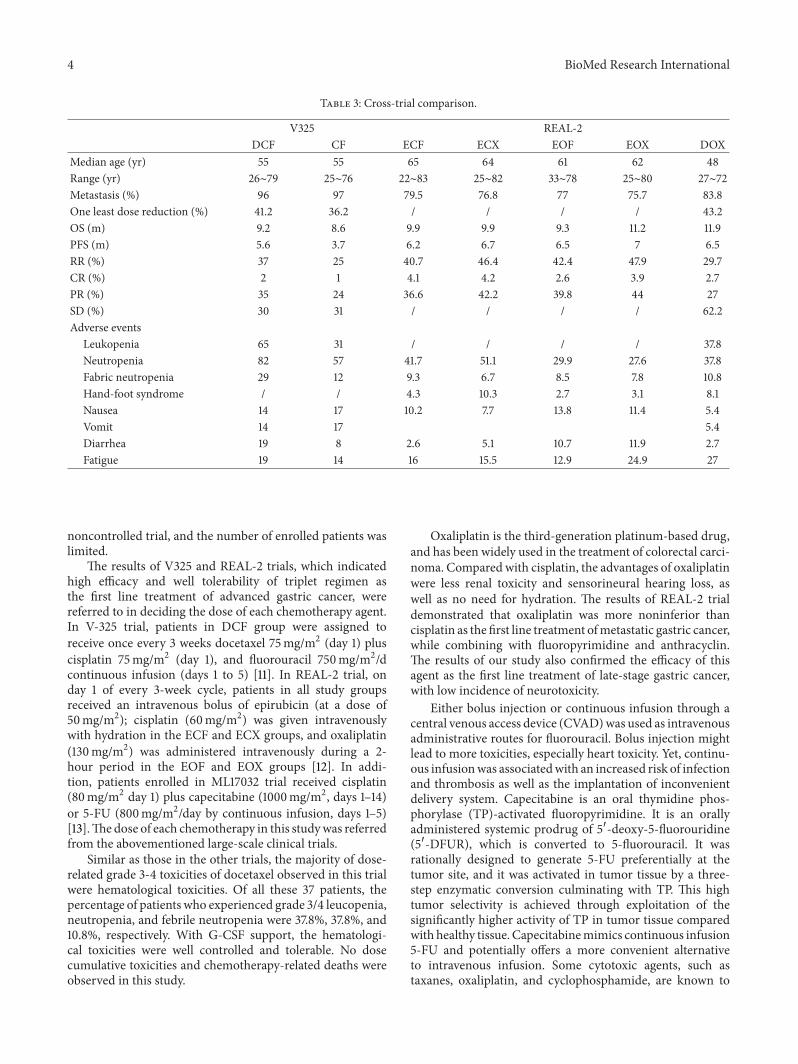
The results of this trial showed that triplet regimen withnovel agents demonstrated obvious survival benefit as thefirst-line treatment of late stage gastric adenocarcinoma Theprogression-free survival time was 197 days and the overallsurvival time was 364 days which was significantly longerthan those in REAL-2 and V-325 trials (Table 3) The reasons
Table 1 Patients characteristics (119899 = 37)
Characteristics NoSex
Male 23Female 14
Age (yr)Median 48Range 27ndash72
ECOG0-1 372 0
Extent of diseaseLocally advanced 6Metastasis 31
PathologyModerate 2Poor 25Other 10
Organs involvedLiver 12Lung 2Bone 3Pelvic cavity 11Virchowrsquos LN 3
Previous treatmentExploratory laparotomy 8Gastrectomy 7Chemotherapy 0
Table 2 Grade 3-4 toxicities of DOX regimen
Toxicity 119899 ()Hematological toxicity
Leukopenia 14 (378)Neutropenia 14 (378)Febrile neutropenia 4 (108)
Nonhematological toxicityGastrointestinal toxicity
Nausea 2 (54)Vomiting 2 (54)Anorexia 3 (81)Diarrhea 1 (27)
Neurosensory toxicity 1 (27)Hepatic 1 (27)Other
Fatigue 10 (270)Hand-foot syndrome 3 (81)
might be as follows First compared with DCF group in V-325 trial and EOX group in REAL-2 trial the percentageof metastatic diseases was lower in our study (96 versus755 versus 838) Second this trial was a single arm
4 BioMed Research International
Table 3 Cross-trial comparison
V325 REAL-2DCF CF ECF ECX EOF EOX DOX
Median age (yr) 55 55 65 64 61 62 48Range (yr) 26sim79 25sim76 22sim83 25sim82 33sim78 25sim80 27sim72Metastasis () 96 97 795 768 77 757 838One least dose reduction () 412 362 432OS (m) 92 86 99 99 93 112 119PFS (m) 56 37 62 67 65 7 65RR () 37 25 407 464 424 479 297CR () 2 1 41 42 26 39 27PR () 35 24 366 422 398 44 27SD () 30 31 622Adverse events
Leukopenia 65 31 378Neutropenia 82 57 417 511 299 276 378Fabric neutropenia 29 12 93 67 85 78 108Hand-foot syndrome 43 103 27 31 81Nausea 14 17 102 77 138 114 54Vomit 14 17 54Diarrhea 19 8 26 51 107 119 27Fatigue 19 14 16 155 129 249 27
noncontrolled trial and the number of enrolled patients waslimited
The results of V325 and REAL-2 trials which indicatedhigh efficacy and well tolerability of triplet regimen asthe first line treatment of advanced gastric cancer werereferred to in deciding the dose of each chemotherapy agentIn V-325 trial patients in DCF group were assigned toreceive once every 3 weeks docetaxel 75mgm2 (day 1) pluscisplatin 75mgm2 (day 1) and fluorouracil 750mgm2dcontinuous infusion (days 1 to 5) [11] In REAL-2 trial onday 1 of every 3-week cycle patients in all study groupsreceived an intravenous bolus of epirubicin (at a dose of50mgm2) cisplatin (60mgm2) was given intravenouslywith hydration in the ECF and ECX groups and oxaliplatin(130mgm2) was administered intravenously during a 2-hour period in the EOF and EOX groups [12] In addi-tion patients enrolled in ML17032 trial received cisplatin(80mgm2 day 1) plus capecitabine (1000mgm2 days 1ndash14)or 5-FU (800mgm2day by continuous infusion days 1ndash5)[13]Thedose of each chemotherapy in this studywas referredfrom the abovementioned large-scale clinical trials
Similar as those in the other trials the majority of dose-related grade 3-4 toxicities of docetaxel observed in this trialwere hematological toxicities Of all these 37 patients thepercentage of patients who experienced grade 34 leucopenianeutropenia and febrile neutropenia were 378 378 and108 respectively With G-CSF support the hematologi-cal toxicities were well controlled and tolerable No dosecumulative toxicities and chemotherapy-related deaths wereobserved in this study
Oxaliplatin is the third-generation platinum-based drugand has been widely used in the treatment of colorectal carci-noma Compared with cisplatin the advantages of oxaliplatinwere less renal toxicity and sensorineural hearing loss aswell as no need for hydration The results of REAL-2 trialdemonstrated that oxaliplatin was more noninferior thancisplatin as the first line treatment ofmetastatic gastric cancerwhile combining with fluoropyrimidine and anthracyclinThe results of our study also confirmed the efficacy of thisagent as the first line treatment of late-stage gastric cancerwith low incidence of neurotoxicity
Either bolus injection or continuous infusion through acentral venous access device (CVAD)was used as intravenousadministrative routes for fluorouracil Bolus injection mightlead to more toxicities especially heart toxicity Yet continu-ous infusionwas associatedwith an increased risk of infectionand thrombosis as well as the implantation of inconvenientdelivery system Capecitabine is an oral thymidine phos-phorylase (TP)-activated fluoropyrimidine It is an orallyadministered systemic prodrug of 51015840-deoxy-5-fluorouridine(51015840-DFUR) which is converted to 5-fluorouracil It wasrationally designed to generate 5-FU preferentially at thetumor site and it was activated in tumor tissue by a three-step enzymatic conversion culminating with TP This hightumor selectivity is achieved through exploitation of thesignificantly higher activity of TP in tumor tissue comparedwith healthy tissue Capecitabinemimics continuous infusion5-FU and potentially offers a more convenient alternativeto intravenous infusion Some cytotoxic agents such astaxanes oxaliplatin and cyclophosphamide are known to
BioMed Research International 5
up-regulate TP activity in tumor cells offering potentialsynergistic action Several powerful clinical trials such asREAL-2 ML17032 and ToGA have elucidated the efficacy ofcapecitabine in chemonaıve gastric cancer patients [14]
The SPIRITS trial evaluated S-1 plus cisplatin versus S-1alone in the first-line treatment of advanced gastric cancerA total of 148 patients were assigned to S-1 plus cisplatingroup and 150 patients were assigned to S-1 monotherapygroup Median overall survival was significantly longer in S-1 plus cisplatin group than that in S-1 group (130 monthsversus 110 months HR = 077 95 CI 061ndash098 119875 = 004)Progression-free survival was also significantly longer indoublet group (60 months versus 40 months 119875 lt 00001)[15] In another phase II study of docetaxel and S-1 com-bination therapy for advanced or recurrent gastric canceran overall response rate of 563 (95 confidence interval(95 CI) 38ndash66) was observed and the tumor control rate(complete response partial response and stable disease) was938 (95 CI 83ndash98) Median overall survival was 143months (95 CI 107ndash203 months) and median time totumor progression was 73 months (95CI 43ndash100months)[16] All these two trials demonstrated survival benefits ofS-1 in advanced gastric cancer which holds the promiseof becoming a backbone agent in the first-line regimen intreating advanced gastric cancer
The results of AVAGAST [17] andREAL-3 [18] trials failedto demonstrated survival benefit of adding bevacizumab orpanitumumab to standard chemotherapy in the first line ofgastric cancer HER-2 enrichment designed study ToGA trialshowed the efficacy and safety of trastuzumab in the firstline treatment of HER-2 positive advanced gastric cancerPatients with HER-2 immunohistochemistry (IHC)+++ orIHC++FISH positive (15sim20) can benefit from this tar-geted agent with mOS of 160 months For those with HER-2negative the optional chemotherapeutic strategies includingthe selection of agents and regimen the lines to be addressedand the potential role of target identification should befurther investigated
The results of our study demonstrated a promising goodresponse survival benefit and well tolerance of triplet regi-men including docetaxel oxaliplatin and oral fluoropyrim-idine capecitabine in the first line treatment of late stagegastric cancer patients with good performance status Theshortage of this study is single arm limited patient numberand lack of biomarker explorationThe precise efficacy of thisregimen and the subgroup of gastric cancer patients whobenefit more from this regimen need to be investigated by alarge-scale study
Conflict of Interests
The authors have declared that no conflict of interests exists
Acknowledgments
This study was supported by grants from the ShanghaiNatural Science Foundation from municipal government(13ZR1425900) The authors are grateful to all the enrolled
patients and their families as well as all the staff whocontributed to this study
References
[1] M Garcia A Jernal E M Ward et al Global Cancer Facts andFigures American Society Atlanta Ga USA 2007
[2] A M Murad F F Santiago A Petroianu P R S Rocha MA G Rodrigues and M Rausch ldquoModified therapy with 5-fluorouracil doxorubicin andmethotrexate in advanced gastriccancerrdquo Cancer vol 72 no 1 pp 37ndash41 1993
[3] S Pyrhonen T Kuitunen P Nyandoto and M KourildquoRandomised comparison of fluorouracil epidoxorubicin andmethotrexate (FEMTX) plus supportive care with supportivecare alone in patientswith non-resectable gastric cancerrdquoBritishJournal of Cancer vol 71 no 3 pp 587ndash591 1995
[4] B Glimelius K Ekstrom K Hoffman et al ldquoRandomizedcomparison between chemotherapy plus best supportive carewith best supportive care in advanced gastric cancerrdquo Annalsof Oncology vol 8 no 2 pp 163ndash168 1997
[5] A D Wagner W Grothe J Haerting G Kleber A Grotheyand W E Fleig ldquoChemotherapy in advanced gastric cancer asystematic review and meta-analysis based on aggregate datardquoJournal of Clinical Oncology vol 24 no 18 pp 2903ndash2909 2006
[6] I Ringel and S B Horwitiz ldquoStudies with RP 56976 (taxotere) asemisynthetic analogue of taxolrdquo Journal of the National CancerInstitute vol 83 no 4 pp 288ndash291 1991
[7] M V Blagosklonny T Schulte P Nguyen J Trepel and L MNeckers ldquoTaxol-induced apoptosis and phosphorylation of Bcl-2 protein involves c- Raf-1 and represents a novel c-Raf-1 signaltransduction pathwayrdquo Cancer Research vol 56 no 8 pp 1851ndash1854 1996
[8] D S Grant T L Williams M Zahaczewsky and A PDicker ldquoComparison of antiangiogenic activities using pacli-taxel (taxol) and docetaxel (taxotere)rdquo International Journal ofCancer vol 104 no 1 pp 121ndash129 2003
[9] K A Hotchkiss A W Ashton R Mahmood R G Russell JA Sparano and E L Schwartz ldquoInhibition of endothelial cellfunction in vitro and angiogenesis in vivo by docetaxel (Tax-otere) association with impaired repositioning of the micro-tubule organizing centerrdquo Molecular Cancer Therapeutics vol1 no 13 pp 1191ndash1200 2002
[10] A Vacca D Ribatti M Iurlaro et al ldquoDocetaxel versus pacli-taxel for antiangiogenesisrdquo Journal of Hematotherapy and StemCell Research vol 11 no 1 pp 103ndash118 2002
[11] J A Ajani V M Moiseyenko S Tjulandin et al ldquoClinicalbenefit with docetaxel plus fluorouracil and cisplatin comparedwith cisplatin and fluorouracil in a phase III trial of advancedgastric or gastroesophageal cancer adenocarcinoma the V-325study grouprdquo Journal of Clinical Oncology vol 25 no 22 pp3205ndash3209 2007
[12] D Cunningham A F C Okines and S Ashley ldquoCapecitabineand oxaliplatin for advanced esophagogastric cancerrdquoThe NewEngland Journal of Medicine vol 362 no 9 pp 858ndash859 2010
[13] Y-K Kang W-K Kang D-B Shin et al ldquoCapecitabinecisplatin versus 5-fluorouracilcisplatin as first-line therapy inpatients with advanced gastric cancer a randomised phase IIInoninferiority trialrdquoAnnals of Oncology vol 20 no 4 pp 666ndash673 2009
[14] A F C Okines A R Norman P McCloud Y-K Kang andD Cunningham ldquoMeta-analysis of the REAL-2 and ML17032
6 BioMed Research International
trials evaluating capecitabine-based combination chemother-apy and infused 5-fluorouracil-based combination chemother-apy for the treatment of advanced oesophago-gastric cancerrdquoAnnals of Oncology vol 20 no 9 pp 1529ndash1534 2009
[15] W Koizumi H Narahara T Hara et al ldquoS-1 plus cisplatinversus S-1 alone for first-line treatment of advanced gastriccancer (SPIRITS trial) a phase III trialrdquo The Lancet Oncologyvol 9 no 3 pp 215ndash221 2008
[16] K Yoshida M Ninomiya N Takakura et al ldquoPhase II studyof docetaxel and S-1 combination therapy for advanced orrecurrent gastric cancerrdquo Clinical Cancer Research vol 12 no11 pp 3402ndash3407 2006
[17] E Van Cutsem S de Haas Y K Kang et al ldquoBevacizumabin combination with chemotherapy as first-line therapy inadvanced gastriccancer a biomarker evaluation from the AVA-GAST randomized phase III trialrdquo Journal of Clinical Oncologyvol 30 no 17 pp 2119ndash2127 2012
[18] A F C Okines S E Ashley D Cunningham et al ldquoEpirubicinoxaliplatin and capecitabine with or without panitumumabfor advanced esophagogastric cancer dose-finding study forthe prospective multicenter randomized phase IIIII REAL-3trialrdquo Journal of ClinicalOncology vol 28 no 25 pp 3945ndash39502010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
plasma half-life and intracellular retention time than pacli-taxel In addition the taxanes exhibit different profiles ofdrug resistance [6ndash10] Docetaxel has shown activity againstgastric cancer either as single agent or in combination withother agents The results of the V325 trial confirmed thesurvival benefit and acceptable toxicities of adding doc-etaxel to cisplatin and fluorouracil in treating advanced ormetastatic gastric cancer [11] Based on the results of this trialdocetaxel was approved by the FDA in 2006 in combinationwith 5-FU and cisplatin for advanced or metastatic gastricadenocarcinoma
Oral fluoropyrimidine agents such as capecitabine andS-1 may provide an alternative to standard infusional 5-FUCunningham et al [12] addressed the results of randomizedphase III trial REAL-2 It was a 2 plus 2 factorial designbased on the standard European triplet regimen ECF Theoverall survival of EOX group which contains two newcytotoxic agents (oxaliplatin and capecitabine) reached 112months and significantly longer than those in other groupsThe results of REAL-2 study indicated that oxaliplatin wasmore noninferior than cisplatin and capecitabine was morenoninferior than infusional 5-FU in the first line treatment ofadvanced and metastatic gastric or gastroesophageal cancer
Based upon the results of V-325 and REAL-2 studies wedesign this single armphase II study to evaluate the safety andefficacy of DOX (docetaxel oxaliplatin capecitabine) regi-men in treating unresectable locally advanced or metastaticgastric cancer
2 Methods
21 Patients Characteristics The main eligibility criteriaincluded (1) age 18ndash75 yrs (2) histologically proven gastricadenocarcinoma (3) measurable andor evaluable targetedlesion according to RECIST criteria (version 10) (4) goodperformance status with the Eastern Cooperative OncologyGroup (ECOG) score of 0ndash2 (5) no prior chemotherapy and(6) adequate hepatic renal and hematological function
Exclusion criteria included (1) concomitant cancers(except melanoma skin cancer and carcinoma in situ ofcervix) (2) neuropathy brain or leptomeningeal involve-ment (3) uncontrolled significant comorbid conditions (4)patient could not comprehend the purpose of the study andcould not comply with the protocol and (5) womenwhowerepregnant or breastfeeding The Ethics Committee at RuijinHospital affiliated to Shanghai Jiaotong University School ofMedicine approved the study and written informed consentwas obtained
22 Treatments Docetaxel 75mgm2 was give intravenousinfusion for 2 hours on day 1 oxaliplatin 130mgm2 was alsointravenous infusion for 2 hours on day 1 and capecitabine1000mgm2 were orally intaked twice daily on d1ndash14 Theregimen was repeated every 3 weeksThe dosage of docetaxelwas referred from TAX 325 trial the dosages of oxaliplatinand capecitabine were referred from REAL-2 and ML17032trials Only those who completed at least 2 cycles were
assessed efficacy Patients who finished all 8 cycles of treat-ment without disease progression were turned into follow-upperiod
23 Evaluation and Outcomes Before entering the study allpatients received physical examination full blood count andserum chemistry analyses Chest X-ray ECG upper gas-trointestinal endoscopies abdominal computer tomographic(CT) scans and other appropriate procedures were alsoperformed as needed During treatment full blood count andserum chemistry analyses were conducted before each cycleand X-ray and CT scans were conducted every two cyclesAfter the treatment completed patients were receiving theseevaluations every 2 months PFS (progression-free survival)was defined from the day of enrollment to first evidence ofdisease progression or death occurring within 12 weeks ofthe last assessable tumor assessment OS (overall survival)was defined from the date of enrollment to death from anycause DCR (disease control rate) was defined as followscomplete response (CR) + partial response (PR) + stabledisease (SD)all enrolled patients Responses were evaluatedaccording to RECIST criteria (version 10) Toxicities weregraded according to the National Cancer Institute of CanadaCommon Toxicity Criteria (version 10) The primary end-point of this study was response rates (RR) The secondaryendpoints were PFS OS DCR and the toxicity profilePatients were considered assessable for response if theyreceived at least two cycles of chemotherapy Safety analysesincluded all treated patients and involved the analysis oftreatment-emergent adverse events
24 Statistical Analysis The statistical analysis was carriedout using SPSS software (version 130 SPSS Chicago ILUSA) Descriptive statistics were used for safety evaluationORR and DCR and their two-sided 95 confidence interval(CI) were calculated PFS and OS were estimated usingKaplan-Meier method and their medians along with two-sided 95 CIs were calculated
3 Results
31 Patients and Treatment Characteristics A total of 37 latestage gastric cancer patients were enrolled from April 2007to April 2013 The demographics and baseline characteristicsof these patients are presented in Table 1 The median age ofthese patients was 48 (range 27ndash72) All patients had goodperformance status andwith ECOGperformance status scoreof 0 Twenty-five patients were confirmed pathologically aspoorly differentiated (including signet ring and mucinouscarcinoma) 2 patients were moderately differentiated andthe other 10 patients were confirmed as well-differentiatedadenocarcinoma Thirty-one patients had multimetastaticlesions and the other 6 had locally advanced diseases
32 Overall Response and Survival The median number oftreatment cycles was six ranging from one to eight withthe total cycles of 216 According to the RECIST criteria(version 10) CR was observed in one patient while PR was
BioMed Research International 3
10
08
06
04
02
00
0 500 1000 1500 2000 2500
Progression-free survivalOverall survival
Cum
surv
ival
Time
Figure 1 Kaplan-Meier curves of progression-free survival (PFS197 days) and overall survival (OS 364 days) of DOX regimen
observed in 10 patients SD was in 23 patients and PD in 3patients The ORR was 297 (95 CI 15ndash444) whileDCR was 919 (95 CI 839ndash99) Median progression-free survival (mPFS) and overall survival (mOS) time were197 days (95 CI 138ndash255 days) and 364 days (95 CI 255ndash472 days) respectively (Figure 1)
33 Toxicities The most common grade 34 toxicities werehematological toxicities The percentages of patients withgrade 34 leucopenia neutropenia and febrile neutropeniawere 378 378 and 108 respectivelyThemost commongrade 34 nonhematological toxicities were fatigue nau-sea vomiting anorexia diarrhea and hand-foot syndromewith the percentages of 270 54 54 81 27 and81 accordingly No severe liver or renal dysfunction orchemotherapy-related death was observed Only one patientdeveloped grade 2 peripheral neuropathy (Table 2)
34 Dose Reduction Patients who developed grade 4 hema-tological toxicities or grade 3 nonhematological toxicitiesreceived a 20 dosage reduction Among all enrolledpatients 13 had one time dose reduction (docetaxel andoxalipatin were 80 of the initial dose) and other 3 patientsgot one dose reduction of capecitabine owing to grade 3 hand-foot syndrome
4 Discussion
The results of this trial showed that triplet regimen withnovel agents demonstrated obvious survival benefit as thefirst-line treatment of late stage gastric adenocarcinoma Theprogression-free survival time was 197 days and the overallsurvival time was 364 days which was significantly longerthan those in REAL-2 and V-325 trials (Table 3) The reasons
Table 1 Patients characteristics (119899 = 37)
Characteristics NoSex
Male 23Female 14
Age (yr)Median 48Range 27ndash72
ECOG0-1 372 0
Extent of diseaseLocally advanced 6Metastasis 31
PathologyModerate 2Poor 25Other 10
Organs involvedLiver 12Lung 2Bone 3Pelvic cavity 11Virchowrsquos LN 3
Previous treatmentExploratory laparotomy 8Gastrectomy 7Chemotherapy 0
Table 2 Grade 3-4 toxicities of DOX regimen
Toxicity 119899 ()Hematological toxicity
Leukopenia 14 (378)Neutropenia 14 (378)Febrile neutropenia 4 (108)
Nonhematological toxicityGastrointestinal toxicity
Nausea 2 (54)Vomiting 2 (54)Anorexia 3 (81)Diarrhea 1 (27)
Neurosensory toxicity 1 (27)Hepatic 1 (27)Other
Fatigue 10 (270)Hand-foot syndrome 3 (81)
might be as follows First compared with DCF group in V-325 trial and EOX group in REAL-2 trial the percentageof metastatic diseases was lower in our study (96 versus755 versus 838) Second this trial was a single arm
4 BioMed Research International
Table 3 Cross-trial comparison
V325 REAL-2DCF CF ECF ECX EOF EOX DOX
Median age (yr) 55 55 65 64 61 62 48Range (yr) 26sim79 25sim76 22sim83 25sim82 33sim78 25sim80 27sim72Metastasis () 96 97 795 768 77 757 838One least dose reduction () 412 362 432OS (m) 92 86 99 99 93 112 119PFS (m) 56 37 62 67 65 7 65RR () 37 25 407 464 424 479 297CR () 2 1 41 42 26 39 27PR () 35 24 366 422 398 44 27SD () 30 31 622Adverse events
Leukopenia 65 31 378Neutropenia 82 57 417 511 299 276 378Fabric neutropenia 29 12 93 67 85 78 108Hand-foot syndrome 43 103 27 31 81Nausea 14 17 102 77 138 114 54Vomit 14 17 54Diarrhea 19 8 26 51 107 119 27Fatigue 19 14 16 155 129 249 27
noncontrolled trial and the number of enrolled patients waslimited
The results of V325 and REAL-2 trials which indicatedhigh efficacy and well tolerability of triplet regimen asthe first line treatment of advanced gastric cancer werereferred to in deciding the dose of each chemotherapy agentIn V-325 trial patients in DCF group were assigned toreceive once every 3 weeks docetaxel 75mgm2 (day 1) pluscisplatin 75mgm2 (day 1) and fluorouracil 750mgm2dcontinuous infusion (days 1 to 5) [11] In REAL-2 trial onday 1 of every 3-week cycle patients in all study groupsreceived an intravenous bolus of epirubicin (at a dose of50mgm2) cisplatin (60mgm2) was given intravenouslywith hydration in the ECF and ECX groups and oxaliplatin(130mgm2) was administered intravenously during a 2-hour period in the EOF and EOX groups [12] In addi-tion patients enrolled in ML17032 trial received cisplatin(80mgm2 day 1) plus capecitabine (1000mgm2 days 1ndash14)or 5-FU (800mgm2day by continuous infusion days 1ndash5)[13]Thedose of each chemotherapy in this studywas referredfrom the abovementioned large-scale clinical trials
Similar as those in the other trials the majority of dose-related grade 3-4 toxicities of docetaxel observed in this trialwere hematological toxicities Of all these 37 patients thepercentage of patients who experienced grade 34 leucopenianeutropenia and febrile neutropenia were 378 378 and108 respectively With G-CSF support the hematologi-cal toxicities were well controlled and tolerable No dosecumulative toxicities and chemotherapy-related deaths wereobserved in this study
Oxaliplatin is the third-generation platinum-based drugand has been widely used in the treatment of colorectal carci-noma Compared with cisplatin the advantages of oxaliplatinwere less renal toxicity and sensorineural hearing loss aswell as no need for hydration The results of REAL-2 trialdemonstrated that oxaliplatin was more noninferior thancisplatin as the first line treatment ofmetastatic gastric cancerwhile combining with fluoropyrimidine and anthracyclinThe results of our study also confirmed the efficacy of thisagent as the first line treatment of late-stage gastric cancerwith low incidence of neurotoxicity
Either bolus injection or continuous infusion through acentral venous access device (CVAD)was used as intravenousadministrative routes for fluorouracil Bolus injection mightlead to more toxicities especially heart toxicity Yet continu-ous infusionwas associatedwith an increased risk of infectionand thrombosis as well as the implantation of inconvenientdelivery system Capecitabine is an oral thymidine phos-phorylase (TP)-activated fluoropyrimidine It is an orallyadministered systemic prodrug of 51015840-deoxy-5-fluorouridine(51015840-DFUR) which is converted to 5-fluorouracil It wasrationally designed to generate 5-FU preferentially at thetumor site and it was activated in tumor tissue by a three-step enzymatic conversion culminating with TP This hightumor selectivity is achieved through exploitation of thesignificantly higher activity of TP in tumor tissue comparedwith healthy tissue Capecitabinemimics continuous infusion5-FU and potentially offers a more convenient alternativeto intravenous infusion Some cytotoxic agents such astaxanes oxaliplatin and cyclophosphamide are known to
BioMed Research International 5
up-regulate TP activity in tumor cells offering potentialsynergistic action Several powerful clinical trials such asREAL-2 ML17032 and ToGA have elucidated the efficacy ofcapecitabine in chemonaıve gastric cancer patients [14]
The SPIRITS trial evaluated S-1 plus cisplatin versus S-1alone in the first-line treatment of advanced gastric cancerA total of 148 patients were assigned to S-1 plus cisplatingroup and 150 patients were assigned to S-1 monotherapygroup Median overall survival was significantly longer in S-1 plus cisplatin group than that in S-1 group (130 monthsversus 110 months HR = 077 95 CI 061ndash098 119875 = 004)Progression-free survival was also significantly longer indoublet group (60 months versus 40 months 119875 lt 00001)[15] In another phase II study of docetaxel and S-1 com-bination therapy for advanced or recurrent gastric canceran overall response rate of 563 (95 confidence interval(95 CI) 38ndash66) was observed and the tumor control rate(complete response partial response and stable disease) was938 (95 CI 83ndash98) Median overall survival was 143months (95 CI 107ndash203 months) and median time totumor progression was 73 months (95CI 43ndash100months)[16] All these two trials demonstrated survival benefits ofS-1 in advanced gastric cancer which holds the promiseof becoming a backbone agent in the first-line regimen intreating advanced gastric cancer
The results of AVAGAST [17] andREAL-3 [18] trials failedto demonstrated survival benefit of adding bevacizumab orpanitumumab to standard chemotherapy in the first line ofgastric cancer HER-2 enrichment designed study ToGA trialshowed the efficacy and safety of trastuzumab in the firstline treatment of HER-2 positive advanced gastric cancerPatients with HER-2 immunohistochemistry (IHC)+++ orIHC++FISH positive (15sim20) can benefit from this tar-geted agent with mOS of 160 months For those with HER-2negative the optional chemotherapeutic strategies includingthe selection of agents and regimen the lines to be addressedand the potential role of target identification should befurther investigated
The results of our study demonstrated a promising goodresponse survival benefit and well tolerance of triplet regi-men including docetaxel oxaliplatin and oral fluoropyrim-idine capecitabine in the first line treatment of late stagegastric cancer patients with good performance status Theshortage of this study is single arm limited patient numberand lack of biomarker explorationThe precise efficacy of thisregimen and the subgroup of gastric cancer patients whobenefit more from this regimen need to be investigated by alarge-scale study
Conflict of Interests
The authors have declared that no conflict of interests exists
Acknowledgments
This study was supported by grants from the ShanghaiNatural Science Foundation from municipal government(13ZR1425900) The authors are grateful to all the enrolled
patients and their families as well as all the staff whocontributed to this study
References
[1] M Garcia A Jernal E M Ward et al Global Cancer Facts andFigures American Society Atlanta Ga USA 2007
[2] A M Murad F F Santiago A Petroianu P R S Rocha MA G Rodrigues and M Rausch ldquoModified therapy with 5-fluorouracil doxorubicin andmethotrexate in advanced gastriccancerrdquo Cancer vol 72 no 1 pp 37ndash41 1993
[3] S Pyrhonen T Kuitunen P Nyandoto and M KourildquoRandomised comparison of fluorouracil epidoxorubicin andmethotrexate (FEMTX) plus supportive care with supportivecare alone in patientswith non-resectable gastric cancerrdquoBritishJournal of Cancer vol 71 no 3 pp 587ndash591 1995
[4] B Glimelius K Ekstrom K Hoffman et al ldquoRandomizedcomparison between chemotherapy plus best supportive carewith best supportive care in advanced gastric cancerrdquo Annalsof Oncology vol 8 no 2 pp 163ndash168 1997
[5] A D Wagner W Grothe J Haerting G Kleber A Grotheyand W E Fleig ldquoChemotherapy in advanced gastric cancer asystematic review and meta-analysis based on aggregate datardquoJournal of Clinical Oncology vol 24 no 18 pp 2903ndash2909 2006
[6] I Ringel and S B Horwitiz ldquoStudies with RP 56976 (taxotere) asemisynthetic analogue of taxolrdquo Journal of the National CancerInstitute vol 83 no 4 pp 288ndash291 1991
[7] M V Blagosklonny T Schulte P Nguyen J Trepel and L MNeckers ldquoTaxol-induced apoptosis and phosphorylation of Bcl-2 protein involves c- Raf-1 and represents a novel c-Raf-1 signaltransduction pathwayrdquo Cancer Research vol 56 no 8 pp 1851ndash1854 1996
[8] D S Grant T L Williams M Zahaczewsky and A PDicker ldquoComparison of antiangiogenic activities using pacli-taxel (taxol) and docetaxel (taxotere)rdquo International Journal ofCancer vol 104 no 1 pp 121ndash129 2003
[9] K A Hotchkiss A W Ashton R Mahmood R G Russell JA Sparano and E L Schwartz ldquoInhibition of endothelial cellfunction in vitro and angiogenesis in vivo by docetaxel (Tax-otere) association with impaired repositioning of the micro-tubule organizing centerrdquo Molecular Cancer Therapeutics vol1 no 13 pp 1191ndash1200 2002
[10] A Vacca D Ribatti M Iurlaro et al ldquoDocetaxel versus pacli-taxel for antiangiogenesisrdquo Journal of Hematotherapy and StemCell Research vol 11 no 1 pp 103ndash118 2002
[11] J A Ajani V M Moiseyenko S Tjulandin et al ldquoClinicalbenefit with docetaxel plus fluorouracil and cisplatin comparedwith cisplatin and fluorouracil in a phase III trial of advancedgastric or gastroesophageal cancer adenocarcinoma the V-325study grouprdquo Journal of Clinical Oncology vol 25 no 22 pp3205ndash3209 2007
[12] D Cunningham A F C Okines and S Ashley ldquoCapecitabineand oxaliplatin for advanced esophagogastric cancerrdquoThe NewEngland Journal of Medicine vol 362 no 9 pp 858ndash859 2010
[13] Y-K Kang W-K Kang D-B Shin et al ldquoCapecitabinecisplatin versus 5-fluorouracilcisplatin as first-line therapy inpatients with advanced gastric cancer a randomised phase IIInoninferiority trialrdquoAnnals of Oncology vol 20 no 4 pp 666ndash673 2009
[14] A F C Okines A R Norman P McCloud Y-K Kang andD Cunningham ldquoMeta-analysis of the REAL-2 and ML17032
6 BioMed Research International
trials evaluating capecitabine-based combination chemother-apy and infused 5-fluorouracil-based combination chemother-apy for the treatment of advanced oesophago-gastric cancerrdquoAnnals of Oncology vol 20 no 9 pp 1529ndash1534 2009
[15] W Koizumi H Narahara T Hara et al ldquoS-1 plus cisplatinversus S-1 alone for first-line treatment of advanced gastriccancer (SPIRITS trial) a phase III trialrdquo The Lancet Oncologyvol 9 no 3 pp 215ndash221 2008
[16] K Yoshida M Ninomiya N Takakura et al ldquoPhase II studyof docetaxel and S-1 combination therapy for advanced orrecurrent gastric cancerrdquo Clinical Cancer Research vol 12 no11 pp 3402ndash3407 2006
[17] E Van Cutsem S de Haas Y K Kang et al ldquoBevacizumabin combination with chemotherapy as first-line therapy inadvanced gastriccancer a biomarker evaluation from the AVA-GAST randomized phase III trialrdquo Journal of Clinical Oncologyvol 30 no 17 pp 2119ndash2127 2012
[18] A F C Okines S E Ashley D Cunningham et al ldquoEpirubicinoxaliplatin and capecitabine with or without panitumumabfor advanced esophagogastric cancer dose-finding study forthe prospective multicenter randomized phase IIIII REAL-3trialrdquo Journal of ClinicalOncology vol 28 no 25 pp 3945ndash39502010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
10
08
06
04
02
00
0 500 1000 1500 2000 2500
Progression-free survivalOverall survival
Cum
surv
ival
Time
Figure 1 Kaplan-Meier curves of progression-free survival (PFS197 days) and overall survival (OS 364 days) of DOX regimen
observed in 10 patients SD was in 23 patients and PD in 3patients The ORR was 297 (95 CI 15ndash444) whileDCR was 919 (95 CI 839ndash99) Median progression-free survival (mPFS) and overall survival (mOS) time were197 days (95 CI 138ndash255 days) and 364 days (95 CI 255ndash472 days) respectively (Figure 1)
33 Toxicities The most common grade 34 toxicities werehematological toxicities The percentages of patients withgrade 34 leucopenia neutropenia and febrile neutropeniawere 378 378 and 108 respectivelyThemost commongrade 34 nonhematological toxicities were fatigue nau-sea vomiting anorexia diarrhea and hand-foot syndromewith the percentages of 270 54 54 81 27 and81 accordingly No severe liver or renal dysfunction orchemotherapy-related death was observed Only one patientdeveloped grade 2 peripheral neuropathy (Table 2)
34 Dose Reduction Patients who developed grade 4 hema-tological toxicities or grade 3 nonhematological toxicitiesreceived a 20 dosage reduction Among all enrolledpatients 13 had one time dose reduction (docetaxel andoxalipatin were 80 of the initial dose) and other 3 patientsgot one dose reduction of capecitabine owing to grade 3 hand-foot syndrome
4 Discussion
The results of this trial showed that triplet regimen withnovel agents demonstrated obvious survival benefit as thefirst-line treatment of late stage gastric adenocarcinoma Theprogression-free survival time was 197 days and the overallsurvival time was 364 days which was significantly longerthan those in REAL-2 and V-325 trials (Table 3) The reasons
Table 1 Patients characteristics (119899 = 37)
Characteristics NoSex
Male 23Female 14
Age (yr)Median 48Range 27ndash72
ECOG0-1 372 0
Extent of diseaseLocally advanced 6Metastasis 31
PathologyModerate 2Poor 25Other 10
Organs involvedLiver 12Lung 2Bone 3Pelvic cavity 11Virchowrsquos LN 3
Previous treatmentExploratory laparotomy 8Gastrectomy 7Chemotherapy 0
Table 2 Grade 3-4 toxicities of DOX regimen
Toxicity 119899 ()Hematological toxicity
Leukopenia 14 (378)Neutropenia 14 (378)Febrile neutropenia 4 (108)
Nonhematological toxicityGastrointestinal toxicity
Nausea 2 (54)Vomiting 2 (54)Anorexia 3 (81)Diarrhea 1 (27)
Neurosensory toxicity 1 (27)Hepatic 1 (27)Other
Fatigue 10 (270)Hand-foot syndrome 3 (81)
might be as follows First compared with DCF group in V-325 trial and EOX group in REAL-2 trial the percentageof metastatic diseases was lower in our study (96 versus755 versus 838) Second this trial was a single arm
4 BioMed Research International
Table 3 Cross-trial comparison
V325 REAL-2DCF CF ECF ECX EOF EOX DOX
Median age (yr) 55 55 65 64 61 62 48Range (yr) 26sim79 25sim76 22sim83 25sim82 33sim78 25sim80 27sim72Metastasis () 96 97 795 768 77 757 838One least dose reduction () 412 362 432OS (m) 92 86 99 99 93 112 119PFS (m) 56 37 62 67 65 7 65RR () 37 25 407 464 424 479 297CR () 2 1 41 42 26 39 27PR () 35 24 366 422 398 44 27SD () 30 31 622Adverse events
Leukopenia 65 31 378Neutropenia 82 57 417 511 299 276 378Fabric neutropenia 29 12 93 67 85 78 108Hand-foot syndrome 43 103 27 31 81Nausea 14 17 102 77 138 114 54Vomit 14 17 54Diarrhea 19 8 26 51 107 119 27Fatigue 19 14 16 155 129 249 27
noncontrolled trial and the number of enrolled patients waslimited
The results of V325 and REAL-2 trials which indicatedhigh efficacy and well tolerability of triplet regimen asthe first line treatment of advanced gastric cancer werereferred to in deciding the dose of each chemotherapy agentIn V-325 trial patients in DCF group were assigned toreceive once every 3 weeks docetaxel 75mgm2 (day 1) pluscisplatin 75mgm2 (day 1) and fluorouracil 750mgm2dcontinuous infusion (days 1 to 5) [11] In REAL-2 trial onday 1 of every 3-week cycle patients in all study groupsreceived an intravenous bolus of epirubicin (at a dose of50mgm2) cisplatin (60mgm2) was given intravenouslywith hydration in the ECF and ECX groups and oxaliplatin(130mgm2) was administered intravenously during a 2-hour period in the EOF and EOX groups [12] In addi-tion patients enrolled in ML17032 trial received cisplatin(80mgm2 day 1) plus capecitabine (1000mgm2 days 1ndash14)or 5-FU (800mgm2day by continuous infusion days 1ndash5)[13]Thedose of each chemotherapy in this studywas referredfrom the abovementioned large-scale clinical trials
Similar as those in the other trials the majority of dose-related grade 3-4 toxicities of docetaxel observed in this trialwere hematological toxicities Of all these 37 patients thepercentage of patients who experienced grade 34 leucopenianeutropenia and febrile neutropenia were 378 378 and108 respectively With G-CSF support the hematologi-cal toxicities were well controlled and tolerable No dosecumulative toxicities and chemotherapy-related deaths wereobserved in this study
Oxaliplatin is the third-generation platinum-based drugand has been widely used in the treatment of colorectal carci-noma Compared with cisplatin the advantages of oxaliplatinwere less renal toxicity and sensorineural hearing loss aswell as no need for hydration The results of REAL-2 trialdemonstrated that oxaliplatin was more noninferior thancisplatin as the first line treatment ofmetastatic gastric cancerwhile combining with fluoropyrimidine and anthracyclinThe results of our study also confirmed the efficacy of thisagent as the first line treatment of late-stage gastric cancerwith low incidence of neurotoxicity
Either bolus injection or continuous infusion through acentral venous access device (CVAD)was used as intravenousadministrative routes for fluorouracil Bolus injection mightlead to more toxicities especially heart toxicity Yet continu-ous infusionwas associatedwith an increased risk of infectionand thrombosis as well as the implantation of inconvenientdelivery system Capecitabine is an oral thymidine phos-phorylase (TP)-activated fluoropyrimidine It is an orallyadministered systemic prodrug of 51015840-deoxy-5-fluorouridine(51015840-DFUR) which is converted to 5-fluorouracil It wasrationally designed to generate 5-FU preferentially at thetumor site and it was activated in tumor tissue by a three-step enzymatic conversion culminating with TP This hightumor selectivity is achieved through exploitation of thesignificantly higher activity of TP in tumor tissue comparedwith healthy tissue Capecitabinemimics continuous infusion5-FU and potentially offers a more convenient alternativeto intravenous infusion Some cytotoxic agents such astaxanes oxaliplatin and cyclophosphamide are known to
BioMed Research International 5
up-regulate TP activity in tumor cells offering potentialsynergistic action Several powerful clinical trials such asREAL-2 ML17032 and ToGA have elucidated the efficacy ofcapecitabine in chemonaıve gastric cancer patients [14]
The SPIRITS trial evaluated S-1 plus cisplatin versus S-1alone in the first-line treatment of advanced gastric cancerA total of 148 patients were assigned to S-1 plus cisplatingroup and 150 patients were assigned to S-1 monotherapygroup Median overall survival was significantly longer in S-1 plus cisplatin group than that in S-1 group (130 monthsversus 110 months HR = 077 95 CI 061ndash098 119875 = 004)Progression-free survival was also significantly longer indoublet group (60 months versus 40 months 119875 lt 00001)[15] In another phase II study of docetaxel and S-1 com-bination therapy for advanced or recurrent gastric canceran overall response rate of 563 (95 confidence interval(95 CI) 38ndash66) was observed and the tumor control rate(complete response partial response and stable disease) was938 (95 CI 83ndash98) Median overall survival was 143months (95 CI 107ndash203 months) and median time totumor progression was 73 months (95CI 43ndash100months)[16] All these two trials demonstrated survival benefits ofS-1 in advanced gastric cancer which holds the promiseof becoming a backbone agent in the first-line regimen intreating advanced gastric cancer
The results of AVAGAST [17] andREAL-3 [18] trials failedto demonstrated survival benefit of adding bevacizumab orpanitumumab to standard chemotherapy in the first line ofgastric cancer HER-2 enrichment designed study ToGA trialshowed the efficacy and safety of trastuzumab in the firstline treatment of HER-2 positive advanced gastric cancerPatients with HER-2 immunohistochemistry (IHC)+++ orIHC++FISH positive (15sim20) can benefit from this tar-geted agent with mOS of 160 months For those with HER-2negative the optional chemotherapeutic strategies includingthe selection of agents and regimen the lines to be addressedand the potential role of target identification should befurther investigated
The results of our study demonstrated a promising goodresponse survival benefit and well tolerance of triplet regi-men including docetaxel oxaliplatin and oral fluoropyrim-idine capecitabine in the first line treatment of late stagegastric cancer patients with good performance status Theshortage of this study is single arm limited patient numberand lack of biomarker explorationThe precise efficacy of thisregimen and the subgroup of gastric cancer patients whobenefit more from this regimen need to be investigated by alarge-scale study
Conflict of Interests
The authors have declared that no conflict of interests exists
Acknowledgments
This study was supported by grants from the ShanghaiNatural Science Foundation from municipal government(13ZR1425900) The authors are grateful to all the enrolled
patients and their families as well as all the staff whocontributed to this study
References
[1] M Garcia A Jernal E M Ward et al Global Cancer Facts andFigures American Society Atlanta Ga USA 2007
[2] A M Murad F F Santiago A Petroianu P R S Rocha MA G Rodrigues and M Rausch ldquoModified therapy with 5-fluorouracil doxorubicin andmethotrexate in advanced gastriccancerrdquo Cancer vol 72 no 1 pp 37ndash41 1993
[3] S Pyrhonen T Kuitunen P Nyandoto and M KourildquoRandomised comparison of fluorouracil epidoxorubicin andmethotrexate (FEMTX) plus supportive care with supportivecare alone in patientswith non-resectable gastric cancerrdquoBritishJournal of Cancer vol 71 no 3 pp 587ndash591 1995
[4] B Glimelius K Ekstrom K Hoffman et al ldquoRandomizedcomparison between chemotherapy plus best supportive carewith best supportive care in advanced gastric cancerrdquo Annalsof Oncology vol 8 no 2 pp 163ndash168 1997
[5] A D Wagner W Grothe J Haerting G Kleber A Grotheyand W E Fleig ldquoChemotherapy in advanced gastric cancer asystematic review and meta-analysis based on aggregate datardquoJournal of Clinical Oncology vol 24 no 18 pp 2903ndash2909 2006
[6] I Ringel and S B Horwitiz ldquoStudies with RP 56976 (taxotere) asemisynthetic analogue of taxolrdquo Journal of the National CancerInstitute vol 83 no 4 pp 288ndash291 1991
[7] M V Blagosklonny T Schulte P Nguyen J Trepel and L MNeckers ldquoTaxol-induced apoptosis and phosphorylation of Bcl-2 protein involves c- Raf-1 and represents a novel c-Raf-1 signaltransduction pathwayrdquo Cancer Research vol 56 no 8 pp 1851ndash1854 1996
[8] D S Grant T L Williams M Zahaczewsky and A PDicker ldquoComparison of antiangiogenic activities using pacli-taxel (taxol) and docetaxel (taxotere)rdquo International Journal ofCancer vol 104 no 1 pp 121ndash129 2003
[9] K A Hotchkiss A W Ashton R Mahmood R G Russell JA Sparano and E L Schwartz ldquoInhibition of endothelial cellfunction in vitro and angiogenesis in vivo by docetaxel (Tax-otere) association with impaired repositioning of the micro-tubule organizing centerrdquo Molecular Cancer Therapeutics vol1 no 13 pp 1191ndash1200 2002
[10] A Vacca D Ribatti M Iurlaro et al ldquoDocetaxel versus pacli-taxel for antiangiogenesisrdquo Journal of Hematotherapy and StemCell Research vol 11 no 1 pp 103ndash118 2002
[11] J A Ajani V M Moiseyenko S Tjulandin et al ldquoClinicalbenefit with docetaxel plus fluorouracil and cisplatin comparedwith cisplatin and fluorouracil in a phase III trial of advancedgastric or gastroesophageal cancer adenocarcinoma the V-325study grouprdquo Journal of Clinical Oncology vol 25 no 22 pp3205ndash3209 2007
[12] D Cunningham A F C Okines and S Ashley ldquoCapecitabineand oxaliplatin for advanced esophagogastric cancerrdquoThe NewEngland Journal of Medicine vol 362 no 9 pp 858ndash859 2010
[13] Y-K Kang W-K Kang D-B Shin et al ldquoCapecitabinecisplatin versus 5-fluorouracilcisplatin as first-line therapy inpatients with advanced gastric cancer a randomised phase IIInoninferiority trialrdquoAnnals of Oncology vol 20 no 4 pp 666ndash673 2009
[14] A F C Okines A R Norman P McCloud Y-K Kang andD Cunningham ldquoMeta-analysis of the REAL-2 and ML17032
6 BioMed Research International
trials evaluating capecitabine-based combination chemother-apy and infused 5-fluorouracil-based combination chemother-apy for the treatment of advanced oesophago-gastric cancerrdquoAnnals of Oncology vol 20 no 9 pp 1529ndash1534 2009
[15] W Koizumi H Narahara T Hara et al ldquoS-1 plus cisplatinversus S-1 alone for first-line treatment of advanced gastriccancer (SPIRITS trial) a phase III trialrdquo The Lancet Oncologyvol 9 no 3 pp 215ndash221 2008
[16] K Yoshida M Ninomiya N Takakura et al ldquoPhase II studyof docetaxel and S-1 combination therapy for advanced orrecurrent gastric cancerrdquo Clinical Cancer Research vol 12 no11 pp 3402ndash3407 2006
[17] E Van Cutsem S de Haas Y K Kang et al ldquoBevacizumabin combination with chemotherapy as first-line therapy inadvanced gastriccancer a biomarker evaluation from the AVA-GAST randomized phase III trialrdquo Journal of Clinical Oncologyvol 30 no 17 pp 2119ndash2127 2012
[18] A F C Okines S E Ashley D Cunningham et al ldquoEpirubicinoxaliplatin and capecitabine with or without panitumumabfor advanced esophagogastric cancer dose-finding study forthe prospective multicenter randomized phase IIIII REAL-3trialrdquo Journal of ClinicalOncology vol 28 no 25 pp 3945ndash39502010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
4 BioMed Research International
Table 3 Cross-trial comparison
V325 REAL-2DCF CF ECF ECX EOF EOX DOX
Median age (yr) 55 55 65 64 61 62 48Range (yr) 26sim79 25sim76 22sim83 25sim82 33sim78 25sim80 27sim72Metastasis () 96 97 795 768 77 757 838One least dose reduction () 412 362 432OS (m) 92 86 99 99 93 112 119PFS (m) 56 37 62 67 65 7 65RR () 37 25 407 464 424 479 297CR () 2 1 41 42 26 39 27PR () 35 24 366 422 398 44 27SD () 30 31 622Adverse events
Leukopenia 65 31 378Neutropenia 82 57 417 511 299 276 378Fabric neutropenia 29 12 93 67 85 78 108Hand-foot syndrome 43 103 27 31 81Nausea 14 17 102 77 138 114 54Vomit 14 17 54Diarrhea 19 8 26 51 107 119 27Fatigue 19 14 16 155 129 249 27
noncontrolled trial and the number of enrolled patients waslimited
The results of V325 and REAL-2 trials which indicatedhigh efficacy and well tolerability of triplet regimen asthe first line treatment of advanced gastric cancer werereferred to in deciding the dose of each chemotherapy agentIn V-325 trial patients in DCF group were assigned toreceive once every 3 weeks docetaxel 75mgm2 (day 1) pluscisplatin 75mgm2 (day 1) and fluorouracil 750mgm2dcontinuous infusion (days 1 to 5) [11] In REAL-2 trial onday 1 of every 3-week cycle patients in all study groupsreceived an intravenous bolus of epirubicin (at a dose of50mgm2) cisplatin (60mgm2) was given intravenouslywith hydration in the ECF and ECX groups and oxaliplatin(130mgm2) was administered intravenously during a 2-hour period in the EOF and EOX groups [12] In addi-tion patients enrolled in ML17032 trial received cisplatin(80mgm2 day 1) plus capecitabine (1000mgm2 days 1ndash14)or 5-FU (800mgm2day by continuous infusion days 1ndash5)[13]Thedose of each chemotherapy in this studywas referredfrom the abovementioned large-scale clinical trials
Similar as those in the other trials the majority of dose-related grade 3-4 toxicities of docetaxel observed in this trialwere hematological toxicities Of all these 37 patients thepercentage of patients who experienced grade 34 leucopenianeutropenia and febrile neutropenia were 378 378 and108 respectively With G-CSF support the hematologi-cal toxicities were well controlled and tolerable No dosecumulative toxicities and chemotherapy-related deaths wereobserved in this study
Oxaliplatin is the third-generation platinum-based drugand has been widely used in the treatment of colorectal carci-noma Compared with cisplatin the advantages of oxaliplatinwere less renal toxicity and sensorineural hearing loss aswell as no need for hydration The results of REAL-2 trialdemonstrated that oxaliplatin was more noninferior thancisplatin as the first line treatment ofmetastatic gastric cancerwhile combining with fluoropyrimidine and anthracyclinThe results of our study also confirmed the efficacy of thisagent as the first line treatment of late-stage gastric cancerwith low incidence of neurotoxicity
Either bolus injection or continuous infusion through acentral venous access device (CVAD)was used as intravenousadministrative routes for fluorouracil Bolus injection mightlead to more toxicities especially heart toxicity Yet continu-ous infusionwas associatedwith an increased risk of infectionand thrombosis as well as the implantation of inconvenientdelivery system Capecitabine is an oral thymidine phos-phorylase (TP)-activated fluoropyrimidine It is an orallyadministered systemic prodrug of 51015840-deoxy-5-fluorouridine(51015840-DFUR) which is converted to 5-fluorouracil It wasrationally designed to generate 5-FU preferentially at thetumor site and it was activated in tumor tissue by a three-step enzymatic conversion culminating with TP This hightumor selectivity is achieved through exploitation of thesignificantly higher activity of TP in tumor tissue comparedwith healthy tissue Capecitabinemimics continuous infusion5-FU and potentially offers a more convenient alternativeto intravenous infusion Some cytotoxic agents such astaxanes oxaliplatin and cyclophosphamide are known to
BioMed Research International 5
up-regulate TP activity in tumor cells offering potentialsynergistic action Several powerful clinical trials such asREAL-2 ML17032 and ToGA have elucidated the efficacy ofcapecitabine in chemonaıve gastric cancer patients [14]
The SPIRITS trial evaluated S-1 plus cisplatin versus S-1alone in the first-line treatment of advanced gastric cancerA total of 148 patients were assigned to S-1 plus cisplatingroup and 150 patients were assigned to S-1 monotherapygroup Median overall survival was significantly longer in S-1 plus cisplatin group than that in S-1 group (130 monthsversus 110 months HR = 077 95 CI 061ndash098 119875 = 004)Progression-free survival was also significantly longer indoublet group (60 months versus 40 months 119875 lt 00001)[15] In another phase II study of docetaxel and S-1 com-bination therapy for advanced or recurrent gastric canceran overall response rate of 563 (95 confidence interval(95 CI) 38ndash66) was observed and the tumor control rate(complete response partial response and stable disease) was938 (95 CI 83ndash98) Median overall survival was 143months (95 CI 107ndash203 months) and median time totumor progression was 73 months (95CI 43ndash100months)[16] All these two trials demonstrated survival benefits ofS-1 in advanced gastric cancer which holds the promiseof becoming a backbone agent in the first-line regimen intreating advanced gastric cancer
The results of AVAGAST [17] andREAL-3 [18] trials failedto demonstrated survival benefit of adding bevacizumab orpanitumumab to standard chemotherapy in the first line ofgastric cancer HER-2 enrichment designed study ToGA trialshowed the efficacy and safety of trastuzumab in the firstline treatment of HER-2 positive advanced gastric cancerPatients with HER-2 immunohistochemistry (IHC)+++ orIHC++FISH positive (15sim20) can benefit from this tar-geted agent with mOS of 160 months For those with HER-2negative the optional chemotherapeutic strategies includingthe selection of agents and regimen the lines to be addressedand the potential role of target identification should befurther investigated
The results of our study demonstrated a promising goodresponse survival benefit and well tolerance of triplet regi-men including docetaxel oxaliplatin and oral fluoropyrim-idine capecitabine in the first line treatment of late stagegastric cancer patients with good performance status Theshortage of this study is single arm limited patient numberand lack of biomarker explorationThe precise efficacy of thisregimen and the subgroup of gastric cancer patients whobenefit more from this regimen need to be investigated by alarge-scale study
Conflict of Interests
The authors have declared that no conflict of interests exists
Acknowledgments
This study was supported by grants from the ShanghaiNatural Science Foundation from municipal government(13ZR1425900) The authors are grateful to all the enrolled
patients and their families as well as all the staff whocontributed to this study
References
[1] M Garcia A Jernal E M Ward et al Global Cancer Facts andFigures American Society Atlanta Ga USA 2007
[2] A M Murad F F Santiago A Petroianu P R S Rocha MA G Rodrigues and M Rausch ldquoModified therapy with 5-fluorouracil doxorubicin andmethotrexate in advanced gastriccancerrdquo Cancer vol 72 no 1 pp 37ndash41 1993
[3] S Pyrhonen T Kuitunen P Nyandoto and M KourildquoRandomised comparison of fluorouracil epidoxorubicin andmethotrexate (FEMTX) plus supportive care with supportivecare alone in patientswith non-resectable gastric cancerrdquoBritishJournal of Cancer vol 71 no 3 pp 587ndash591 1995
[4] B Glimelius K Ekstrom K Hoffman et al ldquoRandomizedcomparison between chemotherapy plus best supportive carewith best supportive care in advanced gastric cancerrdquo Annalsof Oncology vol 8 no 2 pp 163ndash168 1997
[5] A D Wagner W Grothe J Haerting G Kleber A Grotheyand W E Fleig ldquoChemotherapy in advanced gastric cancer asystematic review and meta-analysis based on aggregate datardquoJournal of Clinical Oncology vol 24 no 18 pp 2903ndash2909 2006
[6] I Ringel and S B Horwitiz ldquoStudies with RP 56976 (taxotere) asemisynthetic analogue of taxolrdquo Journal of the National CancerInstitute vol 83 no 4 pp 288ndash291 1991
[7] M V Blagosklonny T Schulte P Nguyen J Trepel and L MNeckers ldquoTaxol-induced apoptosis and phosphorylation of Bcl-2 protein involves c- Raf-1 and represents a novel c-Raf-1 signaltransduction pathwayrdquo Cancer Research vol 56 no 8 pp 1851ndash1854 1996
[8] D S Grant T L Williams M Zahaczewsky and A PDicker ldquoComparison of antiangiogenic activities using pacli-taxel (taxol) and docetaxel (taxotere)rdquo International Journal ofCancer vol 104 no 1 pp 121ndash129 2003
[9] K A Hotchkiss A W Ashton R Mahmood R G Russell JA Sparano and E L Schwartz ldquoInhibition of endothelial cellfunction in vitro and angiogenesis in vivo by docetaxel (Tax-otere) association with impaired repositioning of the micro-tubule organizing centerrdquo Molecular Cancer Therapeutics vol1 no 13 pp 1191ndash1200 2002
[10] A Vacca D Ribatti M Iurlaro et al ldquoDocetaxel versus pacli-taxel for antiangiogenesisrdquo Journal of Hematotherapy and StemCell Research vol 11 no 1 pp 103ndash118 2002
[11] J A Ajani V M Moiseyenko S Tjulandin et al ldquoClinicalbenefit with docetaxel plus fluorouracil and cisplatin comparedwith cisplatin and fluorouracil in a phase III trial of advancedgastric or gastroesophageal cancer adenocarcinoma the V-325study grouprdquo Journal of Clinical Oncology vol 25 no 22 pp3205ndash3209 2007
[12] D Cunningham A F C Okines and S Ashley ldquoCapecitabineand oxaliplatin for advanced esophagogastric cancerrdquoThe NewEngland Journal of Medicine vol 362 no 9 pp 858ndash859 2010
[13] Y-K Kang W-K Kang D-B Shin et al ldquoCapecitabinecisplatin versus 5-fluorouracilcisplatin as first-line therapy inpatients with advanced gastric cancer a randomised phase IIInoninferiority trialrdquoAnnals of Oncology vol 20 no 4 pp 666ndash673 2009
[14] A F C Okines A R Norman P McCloud Y-K Kang andD Cunningham ldquoMeta-analysis of the REAL-2 and ML17032
6 BioMed Research International
trials evaluating capecitabine-based combination chemother-apy and infused 5-fluorouracil-based combination chemother-apy for the treatment of advanced oesophago-gastric cancerrdquoAnnals of Oncology vol 20 no 9 pp 1529ndash1534 2009
[15] W Koizumi H Narahara T Hara et al ldquoS-1 plus cisplatinversus S-1 alone for first-line treatment of advanced gastriccancer (SPIRITS trial) a phase III trialrdquo The Lancet Oncologyvol 9 no 3 pp 215ndash221 2008
[16] K Yoshida M Ninomiya N Takakura et al ldquoPhase II studyof docetaxel and S-1 combination therapy for advanced orrecurrent gastric cancerrdquo Clinical Cancer Research vol 12 no11 pp 3402ndash3407 2006
[17] E Van Cutsem S de Haas Y K Kang et al ldquoBevacizumabin combination with chemotherapy as first-line therapy inadvanced gastriccancer a biomarker evaluation from the AVA-GAST randomized phase III trialrdquo Journal of Clinical Oncologyvol 30 no 17 pp 2119ndash2127 2012
[18] A F C Okines S E Ashley D Cunningham et al ldquoEpirubicinoxaliplatin and capecitabine with or without panitumumabfor advanced esophagogastric cancer dose-finding study forthe prospective multicenter randomized phase IIIII REAL-3trialrdquo Journal of ClinicalOncology vol 28 no 25 pp 3945ndash39502010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
up-regulate TP activity in tumor cells offering potentialsynergistic action Several powerful clinical trials such asREAL-2 ML17032 and ToGA have elucidated the efficacy ofcapecitabine in chemonaıve gastric cancer patients [14]
The SPIRITS trial evaluated S-1 plus cisplatin versus S-1alone in the first-line treatment of advanced gastric cancerA total of 148 patients were assigned to S-1 plus cisplatingroup and 150 patients were assigned to S-1 monotherapygroup Median overall survival was significantly longer in S-1 plus cisplatin group than that in S-1 group (130 monthsversus 110 months HR = 077 95 CI 061ndash098 119875 = 004)Progression-free survival was also significantly longer indoublet group (60 months versus 40 months 119875 lt 00001)[15] In another phase II study of docetaxel and S-1 com-bination therapy for advanced or recurrent gastric canceran overall response rate of 563 (95 confidence interval(95 CI) 38ndash66) was observed and the tumor control rate(complete response partial response and stable disease) was938 (95 CI 83ndash98) Median overall survival was 143months (95 CI 107ndash203 months) and median time totumor progression was 73 months (95CI 43ndash100months)[16] All these two trials demonstrated survival benefits ofS-1 in advanced gastric cancer which holds the promiseof becoming a backbone agent in the first-line regimen intreating advanced gastric cancer
The results of AVAGAST [17] andREAL-3 [18] trials failedto demonstrated survival benefit of adding bevacizumab orpanitumumab to standard chemotherapy in the first line ofgastric cancer HER-2 enrichment designed study ToGA trialshowed the efficacy and safety of trastuzumab in the firstline treatment of HER-2 positive advanced gastric cancerPatients with HER-2 immunohistochemistry (IHC)+++ orIHC++FISH positive (15sim20) can benefit from this tar-geted agent with mOS of 160 months For those with HER-2negative the optional chemotherapeutic strategies includingthe selection of agents and regimen the lines to be addressedand the potential role of target identification should befurther investigated
The results of our study demonstrated a promising goodresponse survival benefit and well tolerance of triplet regi-men including docetaxel oxaliplatin and oral fluoropyrim-idine capecitabine in the first line treatment of late stagegastric cancer patients with good performance status Theshortage of this study is single arm limited patient numberand lack of biomarker explorationThe precise efficacy of thisregimen and the subgroup of gastric cancer patients whobenefit more from this regimen need to be investigated by alarge-scale study
Conflict of Interests
The authors have declared that no conflict of interests exists
Acknowledgments
This study was supported by grants from the ShanghaiNatural Science Foundation from municipal government(13ZR1425900) The authors are grateful to all the enrolled
patients and their families as well as all the staff whocontributed to this study
References
[1] M Garcia A Jernal E M Ward et al Global Cancer Facts andFigures American Society Atlanta Ga USA 2007
[2] A M Murad F F Santiago A Petroianu P R S Rocha MA G Rodrigues and M Rausch ldquoModified therapy with 5-fluorouracil doxorubicin andmethotrexate in advanced gastriccancerrdquo Cancer vol 72 no 1 pp 37ndash41 1993
[3] S Pyrhonen T Kuitunen P Nyandoto and M KourildquoRandomised comparison of fluorouracil epidoxorubicin andmethotrexate (FEMTX) plus supportive care with supportivecare alone in patientswith non-resectable gastric cancerrdquoBritishJournal of Cancer vol 71 no 3 pp 587ndash591 1995
[4] B Glimelius K Ekstrom K Hoffman et al ldquoRandomizedcomparison between chemotherapy plus best supportive carewith best supportive care in advanced gastric cancerrdquo Annalsof Oncology vol 8 no 2 pp 163ndash168 1997
[5] A D Wagner W Grothe J Haerting G Kleber A Grotheyand W E Fleig ldquoChemotherapy in advanced gastric cancer asystematic review and meta-analysis based on aggregate datardquoJournal of Clinical Oncology vol 24 no 18 pp 2903ndash2909 2006
[6] I Ringel and S B Horwitiz ldquoStudies with RP 56976 (taxotere) asemisynthetic analogue of taxolrdquo Journal of the National CancerInstitute vol 83 no 4 pp 288ndash291 1991
[7] M V Blagosklonny T Schulte P Nguyen J Trepel and L MNeckers ldquoTaxol-induced apoptosis and phosphorylation of Bcl-2 protein involves c- Raf-1 and represents a novel c-Raf-1 signaltransduction pathwayrdquo Cancer Research vol 56 no 8 pp 1851ndash1854 1996
[8] D S Grant T L Williams M Zahaczewsky and A PDicker ldquoComparison of antiangiogenic activities using pacli-taxel (taxol) and docetaxel (taxotere)rdquo International Journal ofCancer vol 104 no 1 pp 121ndash129 2003
[9] K A Hotchkiss A W Ashton R Mahmood R G Russell JA Sparano and E L Schwartz ldquoInhibition of endothelial cellfunction in vitro and angiogenesis in vivo by docetaxel (Tax-otere) association with impaired repositioning of the micro-tubule organizing centerrdquo Molecular Cancer Therapeutics vol1 no 13 pp 1191ndash1200 2002
[10] A Vacca D Ribatti M Iurlaro et al ldquoDocetaxel versus pacli-taxel for antiangiogenesisrdquo Journal of Hematotherapy and StemCell Research vol 11 no 1 pp 103ndash118 2002
[11] J A Ajani V M Moiseyenko S Tjulandin et al ldquoClinicalbenefit with docetaxel plus fluorouracil and cisplatin comparedwith cisplatin and fluorouracil in a phase III trial of advancedgastric or gastroesophageal cancer adenocarcinoma the V-325study grouprdquo Journal of Clinical Oncology vol 25 no 22 pp3205ndash3209 2007
[12] D Cunningham A F C Okines and S Ashley ldquoCapecitabineand oxaliplatin for advanced esophagogastric cancerrdquoThe NewEngland Journal of Medicine vol 362 no 9 pp 858ndash859 2010
[13] Y-K Kang W-K Kang D-B Shin et al ldquoCapecitabinecisplatin versus 5-fluorouracilcisplatin as first-line therapy inpatients with advanced gastric cancer a randomised phase IIInoninferiority trialrdquoAnnals of Oncology vol 20 no 4 pp 666ndash673 2009
[14] A F C Okines A R Norman P McCloud Y-K Kang andD Cunningham ldquoMeta-analysis of the REAL-2 and ML17032
6 BioMed Research International
trials evaluating capecitabine-based combination chemother-apy and infused 5-fluorouracil-based combination chemother-apy for the treatment of advanced oesophago-gastric cancerrdquoAnnals of Oncology vol 20 no 9 pp 1529ndash1534 2009
[15] W Koizumi H Narahara T Hara et al ldquoS-1 plus cisplatinversus S-1 alone for first-line treatment of advanced gastriccancer (SPIRITS trial) a phase III trialrdquo The Lancet Oncologyvol 9 no 3 pp 215ndash221 2008
[16] K Yoshida M Ninomiya N Takakura et al ldquoPhase II studyof docetaxel and S-1 combination therapy for advanced orrecurrent gastric cancerrdquo Clinical Cancer Research vol 12 no11 pp 3402ndash3407 2006
[17] E Van Cutsem S de Haas Y K Kang et al ldquoBevacizumabin combination with chemotherapy as first-line therapy inadvanced gastriccancer a biomarker evaluation from the AVA-GAST randomized phase III trialrdquo Journal of Clinical Oncologyvol 30 no 17 pp 2119ndash2127 2012
[18] A F C Okines S E Ashley D Cunningham et al ldquoEpirubicinoxaliplatin and capecitabine with or without panitumumabfor advanced esophagogastric cancer dose-finding study forthe prospective multicenter randomized phase IIIII REAL-3trialrdquo Journal of ClinicalOncology vol 28 no 25 pp 3945ndash39502010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
trials evaluating capecitabine-based combination chemother-apy and infused 5-fluorouracil-based combination chemother-apy for the treatment of advanced oesophago-gastric cancerrdquoAnnals of Oncology vol 20 no 9 pp 1529ndash1534 2009
[15] W Koizumi H Narahara T Hara et al ldquoS-1 plus cisplatinversus S-1 alone for first-line treatment of advanced gastriccancer (SPIRITS trial) a phase III trialrdquo The Lancet Oncologyvol 9 no 3 pp 215ndash221 2008
[16] K Yoshida M Ninomiya N Takakura et al ldquoPhase II studyof docetaxel and S-1 combination therapy for advanced orrecurrent gastric cancerrdquo Clinical Cancer Research vol 12 no11 pp 3402ndash3407 2006
[17] E Van Cutsem S de Haas Y K Kang et al ldquoBevacizumabin combination with chemotherapy as first-line therapy inadvanced gastriccancer a biomarker evaluation from the AVA-GAST randomized phase III trialrdquo Journal of Clinical Oncologyvol 30 no 17 pp 2119ndash2127 2012
[18] A F C Okines S E Ashley D Cunningham et al ldquoEpirubicinoxaliplatin and capecitabine with or without panitumumabfor advanced esophagogastric cancer dose-finding study forthe prospective multicenter randomized phase IIIII REAL-3trialrdquo Journal of ClinicalOncology vol 28 no 25 pp 3945ndash39502010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom





























