Embed Size (px)
Citation preview
I Clinical and Community Studies
Clinical profile and prevalenceof fetal alcohol syndrome in an isolatedcommunity in British Columbia
Geoffrey C. Robinson, MD, FRCPCJulianne L. Conry, PhDRobert F. Conry, PhD
The authors were invited by the band council tocarry out a study to determine the prevalence ofalcohol embryopathy among children in a na-tive Indian community in British Columbia. Themothers of the 123 children aged 18 years or lesswho lived in the community were interviewed.In addition, educational screening was carriedout for children in grades 1 through 12, and 116of the children underwent medical examination.A diagnosis of fetal alcohol syndrome or fetalalcohol effects (FAS/FAE) was made in 22 chil-dren aged 3 to 18 years. Each of these childrenwas matched for age and sex with an unaffectedchild in the same community, and both groupsunderwent psychoeducational testing. The chil-dren with FAS/FAE showed a generalized de-pressed level of functioning compared with theunaffected children. The finding that two thirdsof the children with FAS/FAE were mentallyretarded points to a major health and educationproblem.
A la demande du conseil de bande, nous avonsentrepris d'etablir la frequence de l'embryopa-
Dr. Robinson is a professor in the Department of Paediatrics,Faculty of Medicine, University of British Columbia, Vancouver.Dr. Julianne Conry is an assistant professor and Dr. RobertConry an associate professor in the university's Department ofEducational Psychology and Special Education, Faculty ofEducation.
Reprint requests to: Dr. Geoffrey C. Robinson, Department ofPaediatrics, BC Children's Hospital, 4480 Oak St., Vancouver,BC V6H 3V4
thie alcoolique chez les enfants d'un villageamerindien de Colombie britannique. Entrevuedes meres de 123 sujets ages de moins de 19 ans.Etude de la scolarisation des enfants de la le 'a la12e annee. Examen medical de 116 enfants. Nousposons un diagnostic d'embryopathie alcooliquecaracterisee ou soupconnee (EAC/EAS) chez 22enfants ages de 3 'a 18 ans. Chacun de ceux-ciayant ete apparie pour le sexe et l'age a unenfant indemne vivant dans le meme village, onprocede a des tests psychologiques et scolairessur tous ces sujets. Les porteurs d'EAC/EASmanifestent une inferiorite generale en regarddes temoins. Les deux tiers d'entre eux sontdebiles mentaux. II s'agit donc d'un grave pro-bleme sanitaire et educatif.
S1 tudies of the prevalence of clinical problemsprovide baseline data for preventive andtherapeutic measures, but the difficulties in
conducting them are formidable. An invitation tosurvey a population of children in an isolatedcommunity in British Columbia for signs of alcoholembryopathy permitted us an unusual opportunityto conduct a prevalence study. In this paper wereport the prevalence of fetal alcohol syndromeand fetal alcohol effects (FAS/FAE) in this groupas well as the results of psychoeducational studiesin the affected children and in a comparison groupfrom the same community.
Methods
During the winter of 1984 and the spring of
CMAJ, VOL. 137, AUGUST 1, 1987 203- For prescribing information see page 252

1985 there were approximately 350 registeredmembers in the native Indian community, includ-ing 155 children aged 18 years or less, 123 ofwhom were living on the reserve.
The minimal criteria for diagnosis used werethose recommended by the Fetal Alcohol StudyGroup of the Research Society on Alcoholism.' Thediagnosis of FAS was made if there was a historyof maternal alcohol abuse or FAS in a sibling, andthe child had prenatal or postnatal growth retarda-tion (height and weight below the 10th percentilewhen corrected for gestational age), central ner-vous system (CNS) dysfunction (including neuro-logic abnormalities, developmental delay and intel-lectual impairment) and characteristic craniofacialabnormalities, including at least two of the follow-ing three: microcephaly (head circumference belowthe third percentile), microphthalmia or short pal-pebral fissures, and poorly developed philtrum,thin upper lip and flattening of the maxillary area.
Clinical experience indicates a wide range ofeffects of alcohol on the developing fetus, withFAS at the severe end of the spectrum. When thechild shows only one or two of growth retardation,CNS dysfunction and craniofacial abnormalitiesthe term FAE is used.2
Three procedures - an interview with themothers, educational screening and a medical ex-amination - were used to identify the affectedchildren. All the children identified as affectedwere then assessed by means of a battery ofpsychoeducational tests to measure the degree ofintellectual impairment. To exclude the possibilitythat cognitive deficits were associated with en-vironmental deprivation a comparison group ofunaffected children from the same communitymatched for age and sex underwent the sameassessment. Comparison of the data for the twogroups permitted estimation of the magnitude ofcognitive deficits apparently due to FAS/FAE.
For the interview with the mothers, all womenwith children aged up to 18 years were inter-viewed. A community health nurse visited eachwoman to explain the purpose of the survey and tohave consent forms signed. Each child's date andplace of birth and birth weight were confirmed,and the mother's impressions of the child's growthand development since birth were obtained. Themother's background and health history werebriefly reviewed, and an appointment was madefor completing the interview. At the second inter-view the following information was sought foreach child: prenatal and perinatal history; themother's health-related behaviour, including theextent of alcohol use, before and during thepregnancy; the child's current behaviour character-istics, including sleeping, eating and activity pat-terns; details of the child's growth and develop-ment and medical history; and the background ofthe child's father. Although it was possible todetermine whether alcohol had been used duringthe pregnancy, the women often could not remem-ber the amount consumed.
For educational screening a school learningprofile was completed for each of the 82 childrenin grades 1 to 12 in the community school by theteacher(s) who best knew the details of each child'sacademic performance. The form was not complet-ed for the 20 children in kindergarten or forstudents over 18 years of age. The informationobtained included a rating of the child's generallearning ability, ratings of ability in five specificsubject areas, ratings of the child's activity level(e.g., hyperactive) and aggressiveness, and an indi-cation of whether school personnel wished to referthe child for in-depth psychoeducational assess-ment. If a referral was indicated on this form, anadditional sheet was completed, providing back-ground details for the examiner's information.
During the medical examination measure-ments of height, weight and head circumferencewere obtained, and hearing and vision were as-sessed with standard screening tests (Zenith PureTone Audiometer, Zenith Controls, Inc., Chicago,and Keystone Telebinocular, Mast DevelopmentCo., Davenport, Iowa). Photographs of the head(anteroposterior and lateral views) were obtainedby a professional photographer. Measurements offacial traits were made by means of proceduresdescribed by Vitez and colleagues.3 The photo-graphs were of value in reviewing the diagnoses,but the presence of epicanthic folds and otheranthropomorphic features of native Indians limitedthe comparability of these measures to standardsreported from other research. Physical examinationwas performed by one of two physicians, whowere unaware of the maternal history of alcoholuse during the pregnancy. The clinical findingswere recorded on a medical form that itemized thevarious neurologic, craniofacial and other abnor-malities.
Using the information obtained from thesethree procedures we made a provisional diagnosisof FAS/FAE. Each affected child was then matchedwith another child who was of the same sex, wasnot affected (on the basis of the results of themedical examination), was not a sibling of a childwith FAS and had the closest possible date ofbirth. The comparison children were chosen with-out regard to the results of the interview with themother or of the educational screening.
A provisional diagnosis of FAS/FAE wasmade in 22 children. When the results of thepsychoeducational assessment and examination ofthe photographs, reflecting CNS dysfunction andcraniofacial abnormalities respectively, were avail-able, we reviewed all the data and made a finaldiagnosis of FAS or FAE. One child was removedfrom and one added to the FAS/FAE group. Thus,there were 22 children in the FAS/FAE group butonly 21 in the comparison group owing to theremoval of one child matched with the removedaffected child.
The battery of psychoeducational tests wasdesigned to provide an assessment of a broadrange of abilities and learning styles, particularly
204 CMAJ, VOL. 137, AUGUST 1, 1987
those sensitive to CNS insult due to maternalalcohol use. The results of intelligence tests thatreflect CNS dysfunction are described in thispaper; details of the results of the other psycho-educational measures are available from the au-
thors on request.Depending on the child's age, the appropriate
Wechsler Intelligence Scale or, if preschool age, theMcCarthy Scale of Children's Abilities was admin-istered. The subtests on the Wechsler IntelligenceScale establish a verbal intelligence quotient (IQ)(ability to acquire information, use words andunderstand social situations), a performance IQ(ability to solve problems requiring the manipula-tion of objects, often labelled perceptual organiza-tion) and a composite full-scale IQ. Additionally,these tests demand various degrees of acquiredknowledge, memory, and fine motor and otherskills that are complemented by other tests in thebattery. The McCarthy Scale of Children's Abilitiesprovides a general cognitive index and includesseparate verbal, perceptual, motor, memory andquantitative subtests, thus paralleling the testsadministered to the older children.
Results
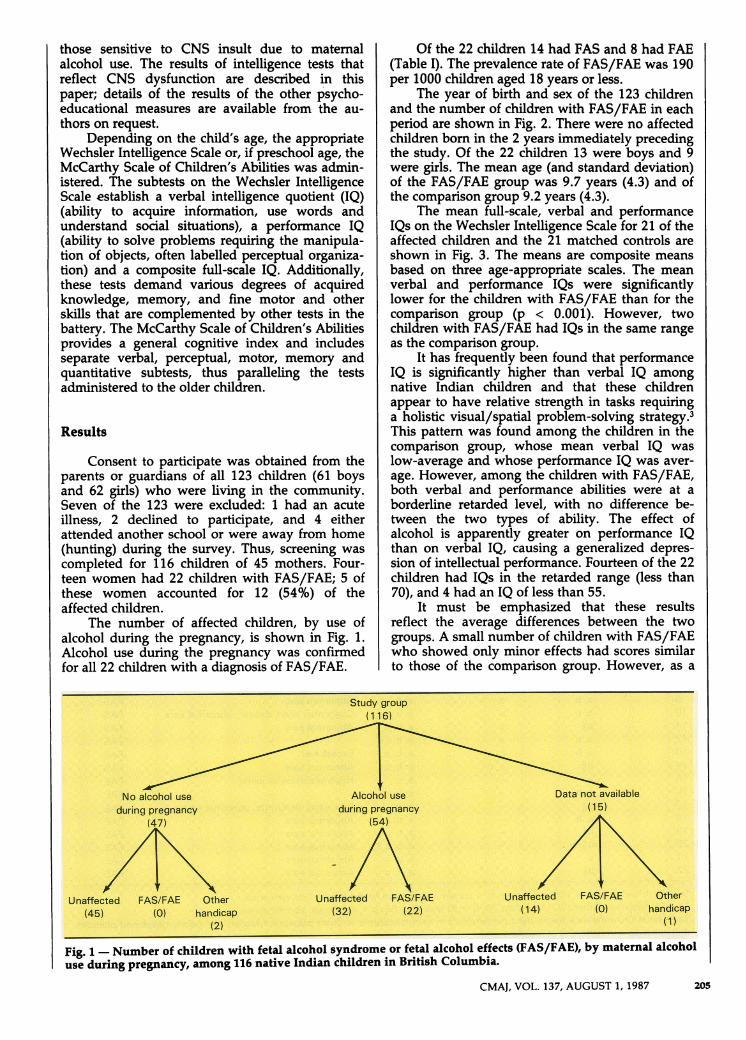
Consent to participate was obtained from theparents or guardians of all 123 children (61 boysand 62 girls) who were living in the community.Seven of the 123 were excluded: 1 had an acuteillness, 2 declined to participate, and 4 eitherattended another school or were away from home(hunting) during the survey. Thus, screening was
completed for 116 children of 45 mothers. Four-teen women had 22 children with FAS/FAE; 5 ofthese women accounted for 12 (54%) of theaffected children.
The number of affected children, by use ofalcohol during the pregnancy, is shown in Fig. 1.Alcohol use during the pregnancy was confirmedfor all 22 children with a diagnosis of FAS/FAE.
Of the 22 children 14 had FAS and 8 had FAE(Table I). The prevalence rate of FAS/FAE was 190per 1000 children aged 18 years or less.
The year of birth and sex of the 123 childrenand the number of children with FAS/FAE in eachperiod are shown in Fig. 2. There were no affectedchildren born in the 2 years immediately precedingthe study. Of the 22 children 13 were boys and 9were girls. The mean age (and standard deviation)of the FAS/FAE group was 9.7 years (4.3) and ofthe comparison group 9.2 years (4.3).
The mean full-scale, verbal and performanceIQs on the Wechsler Intelligence Scale for 21 of theaffected children and the 21 matched controls are
shown in Fig. 3. The means are composite means
based on three age-appropriate scales. The mean
verbal and performance IQs were significantlylower for the children with FAS/FAE than for thecomparison group (p < 0.001). However, twochildren with FAS/FAE had IQs in the same range
as the comparison group.It has frequently been found that performance
IQ is significantly higher than verbal IQ among
native Indian children and that these childrenappear to have relative strength in tasks requiringa holistic visual/spatial problem-solving strategy.3This pattern was found among the children in thecomparison group, whose mean verbal IQ waslow-average and whose performance IQ was aver-
age. However, among the children with FAS/FAE,both verbal and performance abilities were at a
borderline retarded level, with no difference be-tween the two types of ability. The effect ofalcohol is apparently greater on performance IQthan on verbal IQ, causing a generalized depres-sion of intellectual performance. Fourteen of the 22children had IQs in the retarded range (less than70), and 4 had an IQ of less than 55.
It must be emphasized that these resultsreflect the average differences between the twogroups. A small number of children with FAS/FAEwho showed only minor effects had scores similarto those of the comparison group. However, as a
C. c. X .. .. . .. - :...... ..-. .....
-. ................
. 2;.:: ' 4 2 s ' -. ' . . . : . ' -8''.-'Sr0w':
--
*Sl\ : S.:Ss \ 4 .. /~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~.......
CMAJ, VOL. 137, AUGUST 1, 1987 205
Fig. 1 - Number of children with fetal alcohol syndrome or fetal alcohol effects (FAS/FAE), by maternal alcoholuse during pregnancy, among 116 native Indian children in British Columbia.
.

group the children with FAS/FAE had a general-ized depression of neurodevelopmental perfor-mance. There are indications in the data of acumulative deficit: the older children appearedrelatively worse off compared with their peers thanthe younger children; that is, as the children growolder they lag further and further behind.
There was no evidence of increased severity ofFAS in subsequent children, as measured by the IQof the second or third child of the same woman.
Discussion
The frequency of maternal alcohol abuse andthe resultant effect on the children in a communityare difficult to determine for several reasons. Ma-ternal alcohol abuse is often denied, and thediagnosis of FAS/FAE is not easy to establish.There is no single diagnostic test, and the clinicalfindings range from overt FAS to one or moresuggestive signs. While it is possible to documentgrowth retardation and CNS dysfunction, recogni-tion of some of the craniofacial characteristics issubjective. Measurements of facial traits, includingpalpebral fissures and nose and lip anomalies,have been described as objective signs,4 but theanthropomorphic characteristics of Indian childrenreduced the value of these measures in our study.
As a result, underdiagnosis probably occurred.Streissguth5 summarized the available data on thebirth prevalence of FAS and noted that theyderived from local studies of available samples andwere not designed for broad generalization.
Three studies in northern France,6 Sweden7and the United States8 showed prevalence rates ofFAS in the range of 1 per 750 births. May andcolleagues9 reported higher rates, ranging from 1per 100 to 1 per 750 live births, among variousIndian tribes in the southwestern United States.Studies in British Columbia have indicated preva-lence rates ranging from 1 per 2717 live births forthe general population to 1 per 150 live births fornative Indians (BC Health Surveillance Registry:personal communication, 1983).
Obtaining an accurate measurement of theprevalence of FAS/FAE in a given region involvesthe study of every family and child; this is timeconsuming, costly and rarely possible. In ourstudy, however, we had this opportunity, and eachchild was carefully studied, with particular atten-tion to maternal alcohol use during pregnancy. Theprevalence rate of FAS/FAE of 190/1000 childrenaged up to 18 years was unexpectedly high. In arecent study of handicapped children aged 16years or less in 23 communities in northwesternBritish Columbia and 14 communities in theYukon Territory, prevalence rates of FAS/FAE of
r .
O4Bb*1-40wr. abnOriAbnmal sears
Ex .hair
Pto, abnormaConpnital hear
_o0gMIat hawtANoral ears
wr daec
ears FASt dease FAS
PAS
FASFAA
a.t its
71
M.
iG .
-.~~~~~~~Q!
206 CMAJ, VOL. 137, AUGUST 1, 1987
..I, .....2 ..
7 .S
t817..
.; .%is._
a
.a
*a..i, f .
bb, c
b
aa
a
aa
.F, c
b
R. b;Z..
aw,b
a, b
-aba.
a b..i.
a,b, ica. ca,. b.c
*sic
a, b, ca,b, c
a, b.c
.a, .,c
a, b, ca, b, ca, b,ca.
a. b,c~a,b,ca;:he
,.i '!'

26 and 46 per 1000 Indian children were found(Kwadwo Asante and Joyce Nelms-Matzke: un-published data, 1985). Higher rates would proba-bly have been found in severely affected commu-nities in these two regions if it had been practicalto use the methods of our study. Furthermore, theelevated death rate among infants with FAS/FAEreduces the number of live affected children;hence, the prevalence rate may be an underesti-mate.
In our study most of the children with devel-opmental delay, as observable on clinical examina-tion, were assigned to the affected group. Thus, itis not surprising that the psychoeducational studiesshowed that the average IQ was significantly lowerin the affected group than in the unaffected group.
10
9
8
7
6
MF MF MF MF MF MF MF MF MF66-68 68-70 70-72 72-74 74-76 76-78 78-80 80-82 82-84
Year
Fig. 2 - Year of birth and sex of study population (n= 123). Striped areas of bars represent children withFAS/FAE; M = male; F = female. Each 2-year periodbegins on Oct. 1 and ends on Sept. 30.
120
110
100
0 90- ~~~~~88.0
0
7006
-
40
Full-scale Verbal Performance
Fig. 3- Mean full-scale intelligence quotient (IQ),verbal IQ and performance IQ for 21 children withFAS/FAE (striped boxes) and 21 control children(white boxes). Boxes extend to 1 standard deviation(SD), vertical lines to + 2 SD.
However, the severity of the intellectual deficit wasunexpected. Of the 22 children with FAS/FAE64% were mentally retarded. Thus, in addition tothe psychologic correlates of environmental depri-vation and social disadvantage that may occur inisolated communities, children in such communi-ties whose mothers used alcohol during the preg-nancy exhibit other effects.
The finding that two-thirds of the childrenwith FAS/FAE in this community are mentallyretarded highlights a major health and educationproblem. FAS is obviously the most common causeof mental retardation in this community. Recentstudies indicate that significant behavioural diffi-culties continue into adolescence and adult-hood,10'11 and this will surely apply in this com-munity as well. The tragedy is that these disabili-ties are preventable.
We gratefully acknowledge the assistance of JoyceNelms-Matzke in conducting the interviews with themothers, Gail Orr, community health nurse, in coordi-nating the study and Dr. Kwadwo Asante in performingthe physical examinations.
This study was supported by a grant fron theNational Native Advisory Council on Alcohol and DrugAbuse.
References
1. Rosett HL: A clinical perspective of the fetal alcoholsyndrome. Alcoholism (NY) 1980; 4:119-122
2. Clarren SK, Smith DW: The fetal alcohol syndrome. N EngiJMed 1978; 298: 1063-1067
3. Seyfort B, Spreen 0, Lahmer V: A critical look at theWISC-R with native Indian children. Alta J Educ Res 1980;26 (1): 14-24
4. Vitez M, Koranyi G, Gonczy E et al: A semiquantitativescore system for epidemiologic studies of fetal alcoholsyndrome. Am JEpidemiol 1984; 119: 301-308
5. Streissguth AP: Alcohol and pregnancy: an overview andan update. Subst Alcohol Actions Misuse 1983; 4: 149-173
6. Dehaene P, Crepin G, Delahousse D et al: Aspects 6pidemi-ologiques du syndrome d'alcoolisme foetal. Nouv PresseMed 1981; 10: 2639-2643
7. Olegard R, Sabel KG, Aronsson M et al: Effects on the childof alcohol abuse during pregnancy. Acta Paediatr Scand[SupplJ 1979; 275: 112-121
8. Hanson JW, Streissguth AP, Smith DW: The effects ofmoderate alcohol consumption during pregnancy on fetalgrowth and morphogenesis. J Pediatr 1978; 92: 457-460
9. May PA, Hymbaugh KJ, Aase JM: The epidemiology offetal alcohol syndrome among American Indians of thesouthwest. Soc Biol 1983; 30: 374-387
10. Streissguth AP, Clarren SK, Jones KJ: Natural history of thefetal alcohol syndrome: a 10-year follow-up of elevenpatients. Lancet 1985; 2: 85-91
11. Streissguth AP, LaDue RA: Fetal alcohol: teratogenic causesof developmental disabilities. In Schroeder SR (ed): ToxicSubstances and Mental Retardation, Am Assoc Ment Defic,Washington, 1987: 1-32
CMAJ, VOL. 137, AUGUST 1, 1987 207









![Prevalence of Children with Severe Fetal Alcohol Spectrum ...FAS prevalence of 3.7 to 7.4 per 1,000. Overall FASD was estimated as 35 per 1,000 (3.5%) [38], Overall FASD was estimated](https://img.dokumen.tips/doc/110x75/5fa3fe3b02308246357b1359/prevalence-of-children-with-severe-fetal-alcohol-spectrum-fas-prevalence-of.jpg)