Embed Size (px)
Citation preview

Clinical Guideline Implementation Clinical Guideline Implementation with Order Sets in a Commercial with Order Sets in a Commercial
Emergency Department Emergency Department Information SystemInformation System
Phil Asaro, MDPhil Asaro, MDWashington University in St. LouisWashington University in St. Louis
Advancing Practice, Instruction and Advancing Practice, Instruction and Innovation Through Informatics (APIII)Innovation Through Informatics (APIII)
Pittsburgh, PennsylvaniaPittsburgh, Pennsylvania
September 11, 2007September 11, 2007
Presentation OutlinePresentation Outline
Our experience - Acute Coronary Our experience - Acute Coronary Syndrome Guideline/Order-setsSyndrome Guideline/Order-setsThe Guideline/Order-setsThe Guideline/Order-setsPhysician surveyPhysician surveyOrdering behaviorOrdering behavior
PerspectivePerspectiveOther reportsOther reportsPublished issuesPublished issues

Clinical GuidelinesClinical GuidelinesClinical guidelines can improve careClinical guidelines can improve careClinicians must be convinced of validityClinicians must be convinced of validityMust be delivered in actionable form at Must be delivered in actionable form at
appropriate timesappropriate timesVarious methods of presentationVarious methods of presentation
Pre-constructed order-setsPre-constructed order-setsContext-specific linksContext-specific linksPPatient-specific guidance atient-specific guidance Immediate feedback - alerts and remindersImmediate feedback - alerts and reminders
Patterns of Guideline Adherence and Care Delivery for Patients with Unstable Angina and Non–ST-segment Elevation Myocardial Infarction (From the CRUSADE Quality Improvement Initiative)
Pierluigi Tricoci, MD, MHS,* Eric D. Peterson, MD, MPH, and Matthew T. Roe, MD, MHS
Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the American College of Cardiology/American Heart Association Guidelines (CRUSADE)
A rapid-cycle quality-improvement initiative
American College of Cardiology (ACC)American Heart Association (AHA)
Am J Cardiol 2006;98[suppl]:30Q–35Q

CRUSADECRUSADE
At the hospital level…
for each 10% increase in the composite adherence to the ACC/AHA guidelines, there was a 10% decrease in the odds of in-hospital mortality

Acute Coronary Syndrome (ACS) Acute Coronary Syndrome (ACS) ED Guideline / Order-setsED Guideline / Order-sets
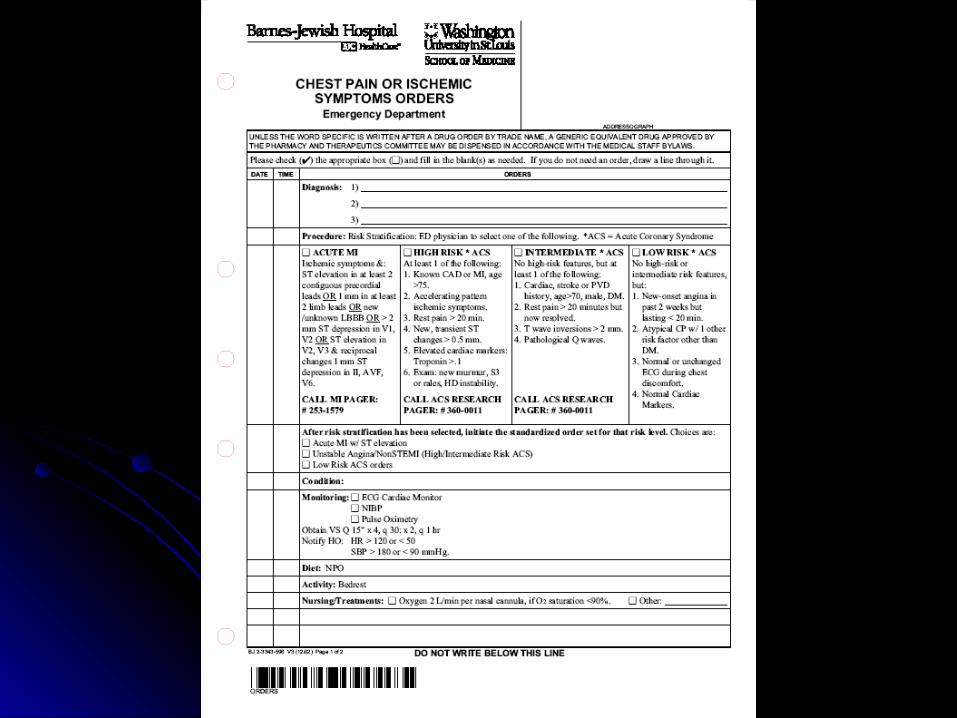
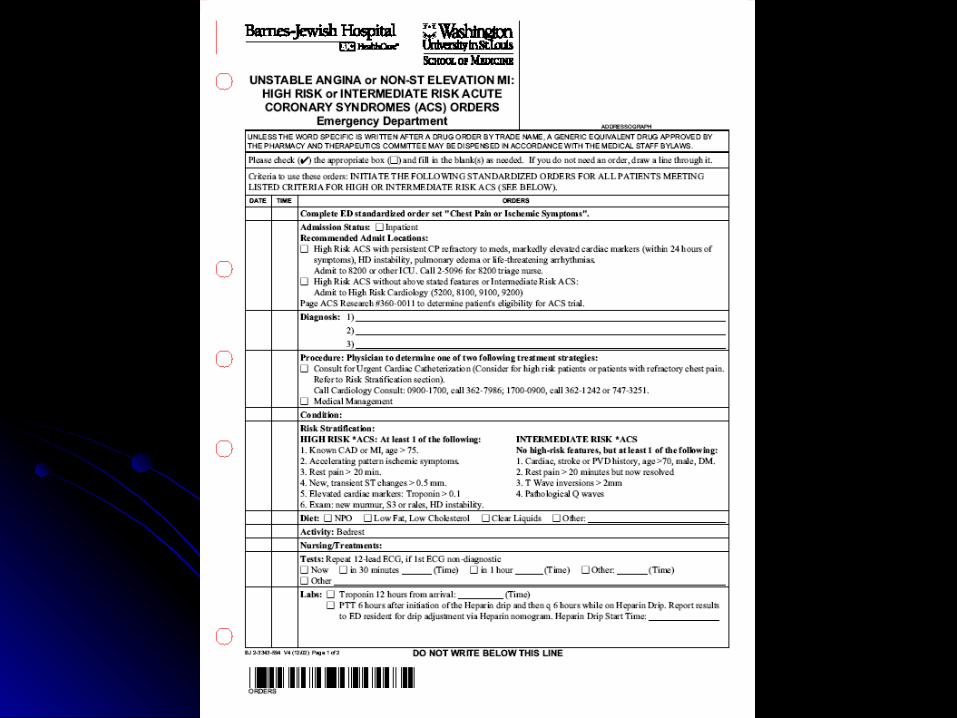
Joint effort - cardiology and EM over 6 monthsJoint effort - cardiology and EM over 6 months Preprinted paper order formsPreprinted paper order forms
Check-off ordersCheck-off orders Fill-in-the-blankFill-in-the-blank Embedded guideline informationEmbedded guideline information
Four forms – each 2-3 pagesFour forms – each 2-3 pages Initial care and risk stratification – all patientsInitial care and risk stratification – all patients Three risk-specific formsThree risk-specific forms
Expected useExpected use Initial order set form + one risk-specific order set formInitial order set form + one risk-specific order set form
Problem:Problem:
Released the paper forms just a few months Released the paper forms just a few months before CPOE implementation was to before CPOE implementation was to eliminate all paper orderseliminate all paper orders

BACKGROUNDBACKGROUNDBarnes-Jewish HospitalBarnes-Jewish Hospital
Large, urban, academic, tertiary care medical Large, urban, academic, tertiary care medical centercenter
EDIS is Healthmatics ED (HMED) EDIS is Healthmatics ED (HMED) Allscripts (acquired with A4 Health Systems)Allscripts (acquired with A4 Health Systems) Incremental implementionIncremental implemention
Original implementation September 2001Original implementation September 2001CPOE including electronic order sets May 2003CPOE including electronic order sets May 2003

What We Had To Work WithWhat We Had To Work With
Problem oriented order-setsProblem oriented order-setsThree-level hierarchyThree-level hierarchy
Order-set name (problem based)Order-set name (problem based)Orders or Subheading (Lab, Medication, etc.)Orders or Subheading (Lab, Medication, etc.)OrdersOrders
““Globe” - URL link at bottom of screenGlobe” - URL link at bottom of screenWe placed pdf’s of the paper forms thereWe placed pdf’s of the paper forms there

Unopened Order-Sets
+ Abdominal Pain+ Chest Pain Criteria+ CP/ACS/MI Initial Orders+ CP/STEMI Orders+ CP/ACS High/Mod Risk Orders+ CP/ACS Low Risk Orders+ Extremity Trauma+ Female GU

+ Abdominal Pain+Chest Pain Criteria
+** Acute MI w/ ST elev:**Ischem Sx AND one of:**ST elev in 2 contiguous**---precordial leads**ST elev, 1mm or more**---in 2 limb leads** New/unknown LBBB** ST depr, more than 2mm**---in V1 and V2**ST elev V2, V3 w/ 1mm**---ST depr II, AVF, V6**Call MI team 253-1579
+**ACS High Risk Criteria:+**ACS Mod Risk Criteria:+**ACS Low Risk Criteria:+**AMI Fibrinolytic Criteria:
+ CP/ACS/MI Initial Orders+ CP/STEMI Orders
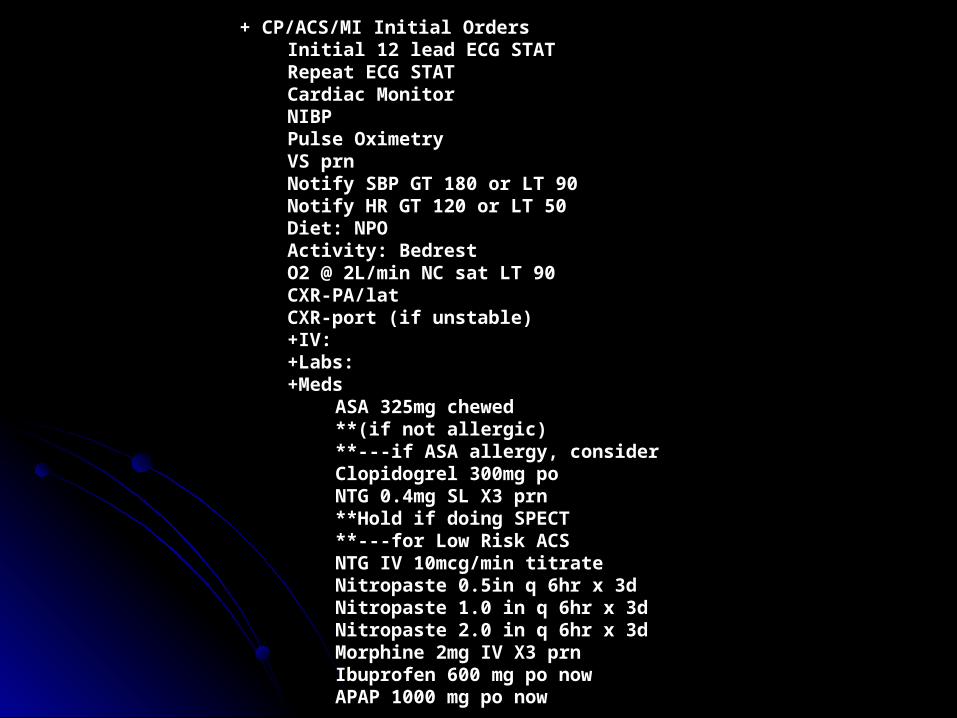
+ CP/ACS/MI Initial OrdersInitial 12 lead ECG STATRepeat ECG STATCardiac MonitorNIBPPulse OximetryVS prn Notify SBP GT 180 or LT 90Notify HR GT 120 or LT 50Diet: NPOActivity: BedrestO2 @ 2L/min NC sat LT 90CXR-PA/latCXR-port (if unstable)+IV:+Labs:+Meds
ASA 325mg chewed **(if not allergic)**---if ASA allergy, considerClopidogrel 300mg poNTG 0.4mg SL X3 prn **Hold if doing SPECT **---for Low Risk ACSNTG IV 10mcg/min titrateNitropaste 0.5in q 6hr x 3dNitropaste 1.0 in q 6hr x 3dNitropaste 2.0 in q 6hr x 3dMorphine 2mg IV X3 prnIbuprofen 600 mg po nowAPAP 1000 mg po now

Anonymous SurveysAnonymous Surveys Pre-CPOE - paper versionPre-CPOE - paper version Post-CPOE - CPOE versionPost-CPOE - CPOE version
Surveys distributed Surveys distributed At an EM weekly conferenceAt an EM weekly conference Mailboxes Mailboxes

Survey Regarding the BJH-ED Chest Pain / Acute Coronary Syndrome Guideline
The following questions are in reference to the HMED Chest Pain / Acute Coronary Syndrome (CP/ACS) order sets and the incorporated guideline information that have been in use since CPOE was implemented in May 2003. This is an anonymous survey aimed at determining the usefulness of the guideline and order set.
1. Please circle one of the following: Attending R1 R2 R3 R4
2. Are you aware of the Chest Pain / Acute Coronary Syndrome Order Set in HMED?
YES NO
3. Please rate the ease of use of the current HMED guideline:
Difficult to use 1----2----3----4----5----6----7----8----9----10 Easy to use
4. Have you had any experience with the preprinted paper version of the CP/ACS order sheets in the BJH-ED? YES NO
5. Skip if your answer to 4 was NO. Please compare the ease of use of the current HMED order-set guideline to the previously used paper order sheets / guideline:
Paper guideline easier 1---2---3---4---5---6---7---8---9---10 HMED guideline easier
6. How useful are the abbreviated stratification criteria on the order set tab?
Not useful 1----2----3----4----5----6----7----8----9----10 Very useful
7. How useful are the expanded risk stratification criteria available from the “globe”?
Not useful 1----2----3----4----5----6----7----8----9----10 Very useful
8. How useful are the intermingled prompts that are imbedded in the orders?
Not useful 1----2----3----4----5----6----7----8----9----10 Very useful
9. Do you agree with this statement?
“The HMED CP/ACS guideline assists me by prompting organized and complete orders."
Disagree 1----2----3----4----5----6----7----8----9----10 Agree
10. Do you agree with this statement?
"The HMED CP/ACS guideline (order set) leads to better patient care"
Disagree 1----2----3----4----5----6----7----8----9----10 Agree
11. Additional comments (Please feel free to use the reverse side if necessary):

Pre- or Post-
CPOE
Attending mean (SD)
Resident mean (SD)
Sig ofDifference
Please rate the ease of use of the current guideline
Pre 5.2 (4.0) 5.9 (2.3) p = 0.70
Post 5.4 (2.3) 7.4 (1.6) p = 0.02
The current CP/ACS guideline (order-set) assists me by prompting organized and complete orders
Pre 4.8 (3.5) 6.3 (2.8) p = 0.39
Post 5.5 (2.5) 7.0 (2.1) p = 0.10
The current CP/ACS guideline (order-set) leads to better patient care
Pre 4.6 (2.3) 6.2 (2.6) p = 0.17
Post 6.2 (2.5) 7.1 (2.4) p = 0.30
Compare the ease of use of the current CPOE order-set guideline to the previously used paper order sheets/guideline
Post 6.6 (2.0) 7.3 (2.2) p = 0.46
How useful are the abbreviated stratification criteria on the order-set tab?
Post 3.8 (2.4) 6.4 (2.0) p = 0.01
How useful are the expanded risk stratification criteria available from the “globe”?
Post 4.1 (3.0) 5.8 (2.4) p = 0.13
How useful are the intermingled prompts that are imbedded in the orders?
Post 4.2 (2.7) 6.6 (2.3) p = 0.02
Mean Survey Responses – Attending vs. Resident
Risk Stratification CriteriaRisk Stratification Criteria
Opened 6 times in 97 patientsOpened 6 times in 97 patientsOnly 3 times with expected use patternOnly 3 times with expected use pattern

Pre- or Post-
CPOE
Correlation with Level of Training
Ease of UsePre -0.18(0.40)
Post -0.42(0.01)
Organized OrdersPre -0.37(0.08)
Post -0.42(0.01)
Better Patient CarePre -0.49(0.02)
Post -0.26(0.13)
CPOE Easier Than Paper Post -0.17(0.37)
Abbrev Criteria Useful Post -0.38(0.02)
Expanded Criteria Useful Post -0.35(0.06)
Integrated Prompts Useful Post -.046(0.01)
Correlation with level of trainingSpearman’s Rho (p-value)

Chart ReviewsChart Reviews Selection criteria - ED diagnosis of MI, ACS, or Selection criteria - ED diagnosis of MI, ACS, or
unstable anginaunstable angina Four one-month periods:Four one-month periods:
Before guideline – simple chest pain orders availableBefore guideline – simple chest pain orders available After paper guideline released - before CPOE After paper guideline released - before CPOE Beginning one month after CPOE implementationBeginning one month after CPOE implementation Beginning three months after CPOE implementationBeginning three months after CPOE implementation
Retrospective chart reviewsRetrospective chart reviews Risk-stratification criteriaRisk-stratification criteria Order-set use Order-set use Compliance with the guideline recommendation for Compliance with the guideline recommendation for
β-blocker useβ-blocker use

NoneInitial or Advanced(not both)
Initial and Multiple
Advanced Sets
Initial and One Risk-Specific
(simple preprinted form in Phase 1)
Phase 1 33/45 (73%) 12/45 (27%)
Phase 2 36/66 (55%) 20/66 (30%) 10/66 (15%)
Phase 3 12/48 (25%) 17/48 (35%) 3/48 (6%) 16/48 (33%)
Phase 4 8/49 (16%) 14/49 (29%) 8/49 (16%) 19/49 (39%)
Order-set use by phase of study

N% β-
BlockerNone
Initial or Advanced(not both)
Initial and Multiple
Advanced Sets
Initial and One Risk-Specific
(simple preprinted form in Phase 1)
Phase 1 21 81% 88% of 16 60% of 5
Phase 2 37 68% 68% of 22 70% of 10 60% of 5
Phase 3 26 69% 33% of 6 88% of 8 100% of 1 73% of 11
Phase 4 26 77% 67% of 3 43% of 7 80% of 5 100% of 11
Beta-Blocker Orders by Order-Set Use and Phase
Patients without contraindication to a β-Blocker (heart block, hypotension, or bradycardia)

Summarizing Our ExperienceSummarizing Our Experience Minimal actual use of criteria listsMinimal actual use of criteria lists Suboptimal use of the order setsSuboptimal use of the order sets Overall unchanged ordering behaviorOverall unchanged ordering behavior Less than enthusiastic survey responsesLess than enthusiastic survey responses
Our attempt at guideline implementation using CPOE Our attempt at guideline implementation using CPOE order-sets in a commercial information system lacking order-sets in a commercial information system lacking more advanced decision-support functionality was not more advanced decision-support functionality was not effectiveeffective
However….However….Less experienced physicians appear more open to Less experienced physicians appear more open to guidance offered in the information systemguidance offered in the information system
Acknowledgements: Amy Sheldahl and Douglas Char, MDAcknowledgements: Amy Sheldahl and Douglas Char, MD

On the Other HandOn the Other Hand
Improving Patient Care And Medical Improving Patient Care And Medical Workflow Using Evidence Based Workflow Using Evidence Based
Order SetsOrder Sets
AMIA Annual Symp Proceedings 2005, 1063AMIA Annual Symp Proceedings 2005, 1063
Chris O'connor , Katherine Decaire , Jan Friedrich
Trillium Health Center
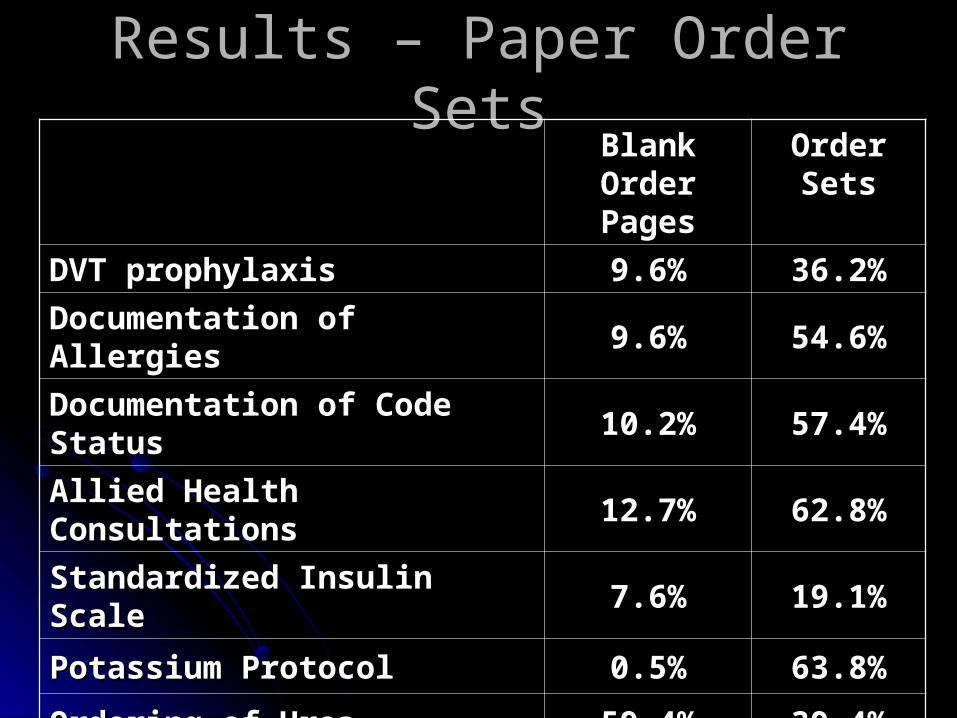
Results – Paper Order SetsResults – Paper Order SetsBlank Order Blank Order
PagesPagesOrder Order SetsSets
DVT prophylaxisDVT prophylaxis 9.6%9.6% 36.2%36.2%
Documentation of AllergiesDocumentation of Allergies 9.6%9.6% 54.6%54.6%
Documentation of Code StatusDocumentation of Code Status 10.2%10.2% 57.4%57.4%
Allied Health ConsultationsAllied Health Consultations 12.7%12.7% 62.8%62.8%
Standardized Insulin ScaleStandardized Insulin Scale 7.6%7.6% 19.1%19.1%
Potassium ProtocolPotassium Protocol 0.5%0.5% 63.8%63.8%
Ordering of UreaOrdering of Urea 59.4%59.4% 39.4%39.4%
ConclusionConclusion
““Order sets are an effective method to Order sets are an effective method to improve compliance with evidence based improve compliance with evidence based practice and improve order quality in a practice and improve order quality in a voluntary paper based order system voluntary paper based order system without the need for significant education.”without the need for significant education.”

Congestive Heart Failure Management: Use of Electronic Order Entry to Enhance Practice
Guideline ComplianceAHA 5th Scientific Forum on Quality of Care in
Cardiovascular Disease and Stroke, Washington, DC; May 16, 2004 (Poster Presentation)
Raymond Dusman, Carolyn Hart, Doug Horner,Jerry Mourey, Karl LaPan, Mark O’Shaughnessy, Robert Plant, David Schleinkofer, Michael Mirro
Fort Wayne Cardiology / Parkview Research CenterFort Wayne, IN

ResultsResults
ACE Inhibitor use increased:From 52.3% (508 of 971) to 85.2% (248 of 291)
Beta Blocker use increased:From 49.1% (477 of 971) to 80.1% (233 of 291)
Spironolactone use in eligible Class III and IV patients increased:From 95.8% (207 of 216) to 100% (75 of 75)

The Role Of Computerized Order The Role Of Computerized Order Sets In Pediatric Inpatient Sets In Pediatric Inpatient
Asthma TreatmentAsthma Treatment
Pediatr Allergy Immunol 2006: 17: 199–206Pediatr Allergy Immunol 2006: 17: 199–206
Chisolm DJ, McAlearney AS, Veneris S, Fisher D, Holtzlander M, McCoy KS.
Columbus Children's Research InstituteOhio State University

ResultsResults
Systemic Systemic SteroidsSteroids MDIMDI Pulse Pulse
OximetryOximetry
Pre- Pre- Order SetOrder SetN=261N=261
75.1%75.1% 47.9%47.9% 78.9%78.9%
Post- Post- Order Order SetSet
Order set Order set not usednot used
N=63N=6377.8%77.8% 39.7%39.7% 82.5%82.5%
Order set Order set usedused
N=466N=46694.4%94.4% 55.6%55.6% 90.8%90.8%

Other Order Set SuccessesOther Order Set Successes
DVT prophylaxisDVT prophylaxisPeri-operative antibiotic compliancePeri-operative antibiotic compliancePain managementPain managementGlucose managementGlucose managementAnticoagulation managementAnticoagulation management

Integrating "Best of Care" Protocols into Integrating "Best of Care" Protocols into Clinicians' Workflow via Care Provider Clinicians' Workflow via Care Provider Order Entry: Impact on Quality-of-Care Order Entry: Impact on Quality-of-Care
Indicators for Acute Myocardial InfarctionIndicators for Acute Myocardial Infarction
J Am Med Inform AssocJ Am Med Inform Assoc. 2006;13:188-196. 2006;13:188-196
Asli Ozdas, PhD, Theodore Speroff, PhD, L. Russell Asli Ozdas, PhD, Theodore Speroff, PhD, L. Russell Waitman, PhD, Judy Ozbolt, PhD, Javed Butler, MD Waitman, PhD, Judy Ozbolt, PhD, Javed Butler, MD
and Randolph A. Miller, MDand Randolph A. Miller, MD
Vanderbilt University HospitalVanderbilt University Hospital

Existing order entry system with ACS order setsExisting order entry system with ACS order sets
Intervention studied -- a CDS mechanism to Intervention studied -- a CDS mechanism to direct physicians to appropriate order sets direct physicians to appropriate order sets when writing admission orderswhen writing admission orders
ACS ACS order set use order set use - suspected MI:- suspected MI:60% (189 of 313) 60% (189 of 313) 70% (161 of 227) 70% (161 of 227)
B-blocker use:B-blocker use:70% 70% 78% (not quite statistically significant) 78% (not quite statistically significant)

A Survey Of Factors Affecting Clinician Acceptance Of Clinical
Decision Support
BMC Medical Informatics and Decision Making 2006, 6:6
Dean F Sittig, Michael A Krall, Richard H Dykstra, Allen Russell and Homer L Chin
Kaiser Permanente

Factors ConsideredFactors Considered Patient
reason for visit – acute vs. chronic severity of illness – number of medications, number of
chronic conditions age
Provider age, gender number of years with Kaiser Permanente
Alert type of alert number of alerts received
Environment presence of a computer in exam room clinician behind schedule

Pertinent ResultsPertinent Results Patient factors
CDS more acceptable when patient is elderly, has multiple medications, has chronic conditions
CDS less acceptable when visit for acute condition – (Productivity vs. Prevention)
Environmental factors Clinicians often behind schedule CDS less acceptable when behind schedule
In principle – CDS most helpful when clinician is least apt to remember…

Specificity Of Computerized Physician Specificity Of Computerized Physician Order Entry Has A Significant Effect On Order Entry Has A Significant Effect On
The Efficiency Of Workflow For The Efficiency Of Workflow For Critically ICritically Illll Patients Patients
Crit Care Med 2005; 33:110 –114)
Naeem A. Ali, MD; Hagop S. Mekhjian, MD; P. Lynn Kuehn, RN, MS; Thomas D. Bentley, RN, MS; Rajee Kumar, PhD;
Amy K. Ferketich, PhD; Stephen P. Hoffmann, MD
The Ohio State University Health System
CPOE deployed in a rapid system-wide approachCPOE deployed in a rapid system-wide approach
Initially implemented in MICU with “generic” order Initially implemented in MICU with “generic” order sets – not designed specifically for the ICUsets – not designed specifically for the ICU
““A striking number of problems occurred early A striking number of problems occurred early and persistently after implementation in the and persistently after implementation in the MICU, unlike other units in the hospital”MICU, unlike other units in the hospital”
MICU returned to paper until further analysis and MICU returned to paper until further analysis and development of specific order setsdevelopment of specific order sets
Subsequently CPOE was implemented in the Subsequently CPOE was implemented in the MICU with successMICU with success

Reflecting back to the paper ordering world…
“Written orders, by convention, had been condensed to very simplified shorthand that facilitated their entry. However, it was with a combination of nurse interpretation and verbally issued clarifications that the request was matched to “standard” unit practice…
…this shorthand may have made care more efficient but also less precise, potentially affecting patient safety”.

Reflecting on the new CPOE world with appropriate order sets…
“We believe that streamlined CPOE ordering aided in standardizing the process of patient care and both benefited patients by introducing best practices and practitioners by facilitating their efficiency”.
Viewpoint: Controversies Viewpoint: Controversies Surrounding Use of Order Sets for Surrounding Use of Order Sets for
Clinical Decision Support in Clinical Decision Support in Computerized Provider Order EntryComputerized Provider Order Entry
J Am Med Inform Assoc. 2007;14:41-47J Am Med Inform Assoc. 2007;14:41-47
Anne M. Bobb, BS Pharm, Thomas H. Payne, MD Anne M. Bobb, BS Pharm, Thomas H. Payne, MD
and Peter A. Gross, MDand Peter A. Gross, MD
From a collection of manuscripts in the Jan/Feb 2007 From a collection of manuscripts in the Jan/Feb 2007 issue of JAMIA produced by a 2005 conference on issue of JAMIA produced by a 2005 conference on
CDS in CPOECDS in CPOE

#1#1
… … most CPOE systems make the most CPOE systems make the utilization of order sets for any given utilization of order sets for any given patient voluntary for clinician-userspatient voluntary for clinician-users
……patients do not benefit when their care patients do not benefit when their care providers bypass evidence-based order providers bypass evidence-based order sets usagesets usage

Related CommentsRelated Comments
Smart system to suggest an order set Smart system to suggest an order set based on complaint or other patient-specific based on complaint or other patient-specific information in the electronic recordinformation in the electronic record
Default orders within an order setDefault orders within an order setAll ordersAll ordersSelect ordersSelect ordersMedication orders?Medication orders?

#2#2
……CPOE vendors and free-standing CPOE vendors and free-standing vendors supply "evidence-based" order vendors supply "evidence-based" order sets for CPOE customerssets for CPOE customers
……it is difficult for institutions to adopt it is difficult for institutions to adopt order sets from other institutionsorder sets from other institutions

#2#2
““Until a national-standard set of defined Until a national-standard set of defined CPOE orderables is developed, to which CPOE orderables is developed, to which each vendor or institution can map their each vendor or institution can map their own "orderables“ —at both the order name own "orderables“ —at both the order name and individual fields’ levels—little progress and individual fields’ levels—little progress may be mademay be made””

#3#3
… … there remain significant limitations to there remain significant limitations to what CPOE-based order sets can dowhat CPOE-based order sets can do

Desirable FunctionalityDesirable Functionality Linked ordersLinked orders
Begin together e.g. monitoring lab ordersBegin together e.g. monitoring lab orders Discontinue at same time e.g. PCA, heparin protocolsDiscontinue at same time e.g. PCA, heparin protocols Mutually exclusive – alternate ABMutually exclusive – alternate AB
Patient-specific dose calculations based on Patient-specific dose calculations based on weight, age, or body surface areaweight, age, or body surface area
Ideally would also considerIdeally would also consider currently active medicationscurrently active medications current laboratory results current laboratory results
““Pop-up" algorithmic "advisors" that go beyond Pop-up" algorithmic "advisors" that go beyond the capabilities of order sets to take dynamic the capabilities of order sets to take dynamic patient states into considerationpatient states into consideration
#4#4
……While evidence-based order sets can make it While evidence-based order sets can make it easier for CPOE clinician-users to "do the easier for CPOE clinician-users to "do the right thing," clinical knowledge advances right thing," clinical knowledge advances rapidly…rapidly…
……When order sets are implemented without When order sets are implemented without organization standards and clinical review or organization standards and clinical review or inadequately maintained, they become inadequately maintained, they become templates for efficiently practicing outdated templates for efficiently practicing outdated medicine on a widespread basismedicine on a widespread basis

Then AgainThen Again
““Many times clinical practice changes are Many times clinical practice changes are recognized at the clinician level, but never recognized at the clinician level, but never communicated to the group managing communicated to the group managing order sets in the system. Clinicians create order sets in the system. Clinicians create ‘standard work-arounds’ to meet their ‘standard work-arounds’ to meet their needs and train their residents and others needs and train their residents and others to use the work-around, thus reverting to to use the work-around, thus reverting to reliance on memory and increasing the reliance on memory and increasing the risk of error”risk of error”

#5#5
……Allow individual clinicians to develop Allow individual clinicians to develop their own "private" order sets? their own "private" order sets?
……Potentially removes the evidence-Potentially removes the evidence-based nature of order sets, and based nature of order sets, and introduces other maintenance issuesintroduces other maintenance issues
CRUSADECRUSADE
Paradoxical CarePatients with higher risk of adverse
outcomes are expected to have a greater absolute benefit from aggressive therapies.
CRUSADE analyses have reported that the highest-risk patients are less likely to be adequately treated.

CRUSADECRUSADE
About 15% of patients with NSTE ACS have moderate-to-severe chronic kidney disease
These patients are older and have more comorbidities, such as diabetes, heart failure and prior history of coronary artery disease
Concerns about complications from antithrombotic drugs and invasive procedures may at least partially explain lower guideline compliance -- data regarding efficacy and safety in these subpopulations is lacking.
CRUSADECRUSADE
Among the strongest predictors of blood transfusion use in patients with NSTE ACS: • renal insufficiency• advanced age
CRUSADECRUSADEMedication overdosing was associated with a
significant increase in major bleeding --dose response effect• degree of excess dose• number of drugs administered in excess
42% of patients with NSTE ACS received an initial dose in excess of that recommended of at least one of: unfractionated heparin low-molecular-weight heparin GP IIb/IIIa inhibitor

Desirable FunctionalityDesirable Functionality Linked ordersLinked orders
Begin together e.g. monitoring lab ordersBegin together e.g. monitoring lab orders Discontinue at same time e.g. PCA, heparin protocolsDiscontinue at same time e.g. PCA, heparin protocols Mutually exclusive – alternate ABMutually exclusive – alternate AB
Patient-specific dose calculations based on Patient-specific dose calculations based on weight, age, or body surface areaweight, age, or body surface area
Ideally would also considerIdeally would also consider currently active medicationscurrently active medications current laboratory results current laboratory results
““Pop-up" algorithmic "advisors" that go beyond Pop-up" algorithmic "advisors" that go beyond the capabilities of order sets to take dynamic the capabilities of order sets to take dynamic patient states into considerationpatient states into consideration

CRUSADECRUSADE
Even simple and harmless interventions are underused among patients with chronic kidney diseasesmoking cessation, counseling, dietary
modification, and referral to cardiac rehabilitation
May reflect the lack of outcome expectancy in this subset of patients.

In ConclusionIn Conclusion Guidelines can improve careGuidelines can improve care Order-sets can make it easier for clinicians to do the Order-sets can make it easier for clinicians to do the
right thingright thing Technology is exciting and wonderfulTechnology is exciting and wonderful Better tools are neededBetter tools are needed
Focus attention on critical decisionsFocus attention on critical decisions Provide additional information at key decision pointsProvide additional information at key decision points
Clinician acceptance importantClinician acceptance important Convincing evidence of safety and efficacyConvincing evidence of safety and efficacy Must be seen as improving clinician workflow, not interfering Must be seen as improving clinician workflow, not interfering
Go for the low hanging fruitGo for the low hanging fruit Keep working on the harder stuffKeep working on the harder stuff
Push vendors to improve functionalityPush vendors to improve functionality Certification of HIT should helpCertification of HIT should help
Phil AsaroPhil Asaro
Washington University in St. LouisWashington University in St. Louis
[email protected]@msnotes.wustl.edu