Embed Size (px)
Citation preview

Clinical Grand Rounds
Wednesday, September 10th, 2003

History
CC: Feeling short of breath and tired HPI: 39 YO AA male who has a relatively
negative PMH presented with C/O fever, fatigue, and DOE. Noted he had slowly progressive fatigue and DOE over recent weeks. About a week PTA, he developed acute onset of fever. He noted he has had multiple life stressors recently, and his life has been "in turmoil".

History
He denied weight loss, night sweats, or hemoptysis. Denied any BRBPR, no melena, no N/V and no abdominal pain. No history of blood disorders, anemia, or any type of bleeding problem.
REVIEW OF SYSTEMS
Negative except as in history of present illness.

PAST MEDICAL HISTORY
Oral cancer, status post surgery with bone graft Skin rash treated with antifungal

ALLERGIES
None.

MEDICATIONS
Griseofulvin for skin rash No herbal, no OTC, no ASA, no chronic
NSAIDS

SOCIAL HISTORY
He is bisexual.
Not Married, no children
Has a supportive family
Hx of smoking crack, last use 9 mo ago
Denies IVDA, Occasional ETOH
Works in a warehouse distribution center
Has small grand nieces and grand nephews who he has been exposed to fairly recently, although they do not live with him. O/W no ill contacts.

FAMILY HISTORY
His mother is alive and well at 57 Father’s health unknown

PHYSICAL EXAMINATION
VS: T-max 103 on the day of admission, Nl sat%, HR 66, RR 18, BP 111/65.
HEENT: Left jaw scarring and deformity, PERRL, EOMI, non-icteric sclera
Neck: Supple. No LAD
Lungs: CTAB, no egophony
Cardiac: RRR. Nl S1, S2, 2/6 SEM, no R/G
Abdomen: Soft, NT/ND, no HSM

Physical Examination
Extremities: No cyanosis, clubbing, or edema. No petechiae. No rash.No axillary, neck, or inguinal LAD
Neurologic: Nonfocal, A/O x 4

Imaging and Lab
CXR NAD
Chem 8 WNL,TP is 8.2, alb 3.8, AP 88, AST 42, ALT 43, LDH 844 (upper limits of normal 618), TB 0.6, direct is 0.0. WBC 9.1, Hgb 4.5, Hct 13.1, MCV 89, platelet count 625, 70% polymorphs, 24% lymphocytes. Nucleated RBCs present. Reticulocyte, absolute 0.8 K/uL
Fibrinogen 391, Ddimer >1050
Stool heme negative

Lab
CT abd, pelvis, and chest: Small peripheral nodule 6 mm in the midline; small hypodensity in the right lobe of the liver reflecting possibly a hemangioma or cyst; 1 cm left external iliac chain node, and a 1 cm left groin node; no masses, abscesses, or free fluid was seen
HIV ELISA reactive, HIV PCR 110,000 Parvovirus IgM positive CD4: 130

Lab
Coombs’ negative normal iron, folate and
B12 levels ferritin 3223 Epo level 115 mU/ml
urine histo Ag negative serum crypto antigen
negative blood cultures negative


Anemia and HIVImpact
Prevalence 63-95% of HIV-infected patients
certain populations at higher risk African Americans low CD4 high viral load low MCV zidovudine
JID
Most common hem abnormality
most common symptom is fatigue
marked effect on QOL demonstrated

Anemia and HIVsurvival impact
Blood 1998, 91:301-8
CDC cohort study, >19,000 patients Median survival decreased regardless of
CD4, AIDS, age, neutropenia, throbocytopenia, antiretroviral therapy and PCP prophylaxis

Anemia and HIVsurvival impact
Reversal of anemia clearly associated with decreased hazard of death
increased hazard with increased CD4 (although decreased incidence)
not causal evidence

Anemia and HIVsurvival impact
EuroSIDA 6725 pts 12 mortality
3.1 % if no anemia 15.9% if Hgb 8-14 40.8% if Hgb<8
Prop. Hazards regression model controlled for CD4 and
viral load still 57% increased
hazard of death per drop in Hgb by 1g/dL (rel hazard 1.57, P0.0001)

JID 2002:185

JID 2002:185

Anemia and HIVDifferential diagnosis
opportunistic infection viral (CMV,
parvovirus) mycobacterial fungal (histoplasmosis,
cryptococcosis)
medications (25%) infiltrative marrow
processesJID
chronic disease nutritional deficiencies TTP DIC AIHA (1/3 Coombs +) direct HIV effect
marrow itself cytokines

Anemia and HIVDrug-induced
Marrow suppression zidovudine (AZT) ganciclovir
Hemolytic anemia ribavirin dapsone TMP/sulfa

Anemia and HIVEvaluation
Initial retic count, MCV, hemolysis labs, Fe studies
fungal antigens CMV antigen TB/fungal blood cultures Parvovirus PCR Bone marrow biopsy
Anemia and HIVTreatment
Transfusion ?association with worse
outcome
Nutritional supplements
Growth factors weekly equally
effective very safe and effective
HAART androgens
stimulate RBC production
increase epo production and decrease excretion

Parvovirus B19
Single stranded DNA Sample 19, panel B Human pathogen (1981) Replicates in late RBC
precursors (Erythrovirus genus) and is cytotoxic
Receptor blood group P antigen (globoside)
Rbc precursors Endothelial cells
Age 15-50% have IgG Spring predominant 50% attack rate in
household contacts Respiratory droplet 1/3000 units contain
parvovirus DNA Pooled blood products

Pediatric exanthems
1. Scarlet fever2. Rubeola3. Rubella4. Epidemic pseudoscarlatina (Filatov-Dukes
disease)5. Erythema infectiosum6. Roseola (exantham subitum, HHV6)

Parvovirus B19
Erythema infectiosum(Fifth disease) Transient aplastic crisis (increased erythropoiesis Polyarthopathy syndrome (adult women) Chronic anemia (usually immunodeficient) Hydrops fetalis/congenital anemia
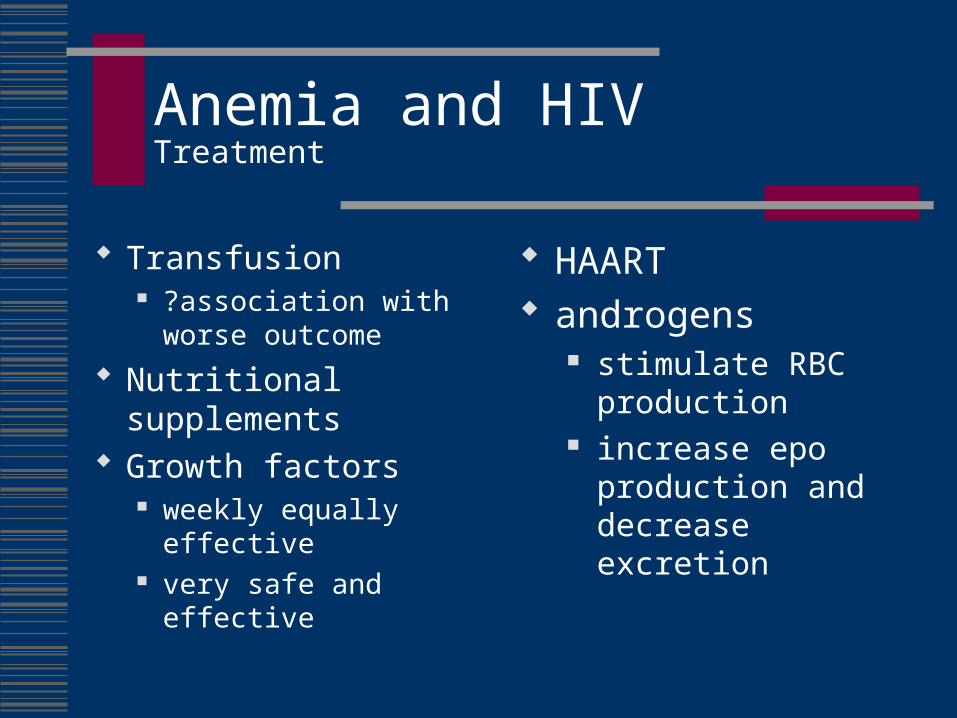
Feigin: Textbook of Pediatric Infectious Diseases, 4th ed., Copyright © 1998 W. B. Saunders Company
Parvovirus
Feigin: Textbook of Pediatric Infectious Diseases, 4th ed., Copyright © 1998 W. B. Saunders Company
Parvovirus B19erythema infectiosum
Nonspecific febrile illness Immune-mediated phase
2-3 weeks with IgM peak Slapped cheek rash/lacy
reticular Polyarthropathy syndrome
(symmetrical, distal, nondestructive)
Papular-;urpuric gloves and socks syndrome
PCR in tissue persists months
Balfour HH. Erythema infectiosum (fifth disease): Clinical review and description of 91 cases seen in an epidemic. Clin Pediatr (Phila). 1969;8:721-727
Anderson MJ, Higgins PG, Davis LR, et al. Experimental parvoviral infection in humans. J Infect Dis. 1985;152:257-265.
Parvovirus
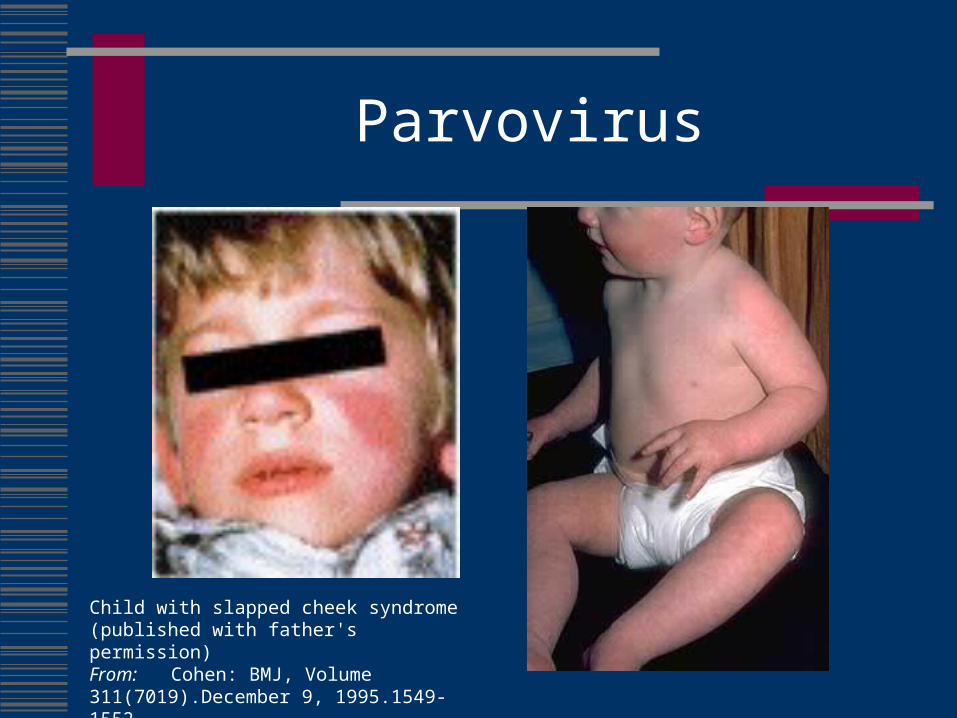
Child with slapped cheek syndrome (published with father's permission) From: Cohen: BMJ, Volume 311(7019).December 9, 1995.1549-1552

Typical ``slapped cheek'' rash is apparent in a two-year-old child with fifth disease (erythema infectiosum), caused by parvovirus B19 infection. The common lacelike erythema of the trunk is also present but not clearly in focus. This disease, which is usually self-limited, is one of the six classic childhood exanthems, which include measles (rubeola), scarlet fever, German measles (rubella), Filatov-Dukes disease (not a separate exanthem but a variant of scarlet fever or toxin-producing staphylococcus infection), and exanthema subitum, or roseola (human herpesvirus 6 infection). From: Feder: N Engl J Med, Volume 331(16).Oct 20, 1994.1062

Parvovirus B19Aplastic crisis
During viremia Retulocyte arrest due
to virus-induced cytotoxicity
Electron micrograph of B19 isolate showing morphology typical of a parvovirus (final magnification x 157 000) From: Cohen: BMJ, Volume 311(7019).December 9, 1995.1549-1552

TABLE 1 -- HEMATOLOGIC CONDITIONS PREDISPOSING PATIENTS TO PARVOVIRUS B19-ASSOCIATED ACUTE APLASTIC CRISIS
Hereditary Disorders
Sickle cell anemia
Hereditary spherocytosis and elliptocytosis
Thalassemia
Glucose-6-phosphate dehydrogenase deficiency
Pyruvate kinase deficiency
Pyrimidine-5'-nucleotidase deficiency
Congenital dyserythropoietic anemia
Acquired Disorders
Iron deficiency anemia
Chronic worn antibody-mediated autoimmune hemolyticanemia
Cold antibody-mediated autoimmune hemolytic anemia
Malaria
Blood loss
Paroxysmal nocturnal hemoglobinuria
Normal host
Pediatric Clinics of North AmericaVolume 43 • Number 3 • June 1996
Parvovirus B19Chronic anemia
Immunosuppressed hosts do not mount neutralizing antibody
Sera from patients with persistent B19 infection typically contain antibody to VP2 but not to VP1
Chronic persistent anemia Reticulocytopenia High B19 DNA in serum Scattered giant
pronormoblasts
Vaccine in clinical trials
IgIG 400mg/kg/day for 5-10
days Q 4 weeks

TABLE 2 -- IMMUNODEFICIENCY DISORDERS THAT HAVE BEEN ASSOCIATED WITH CHRONIC PARVOVIRUS B19 INFECTION
Congenital Immunodeficiency
Nezelof's syndrome
Common variable immunodeficiency
Severe combined immunodeficiency (SCID)
Fetus
Others
Acquired Immunodeficiency
HIV infection
Malignancy
Acute lymphoblastic leukemia
Acute myeloid leukemia
Non-Hodgkin's lymphoma
Brain tumors
Wilms tumor
Rhabdomyosarcoma
Organ transplant recipients
Renal transplantation
Liver transplantation
Cardiac transplantation
Bone marrow transplant recipients
Collagen vascular diseases
Systemic lupus erythematosus
Rheumatoid arthritis
Pediatric Clinics of North AmericaVolume 43 • Number 3 • June 1996
ParvovirusChronic anemia-HIV
B19 DNA was found in 5 (17%) of 30 transfusion-dependent HIV-seropositive homosexuals, and when a hematocrit of less than 20 was used as a criterion, 4 (31%) of 13 were positive. (J Infect Dis. 1997;176:269-273) Marrow may not be suggestive of PRCA and
giant prnormoblasts may not be present

(A) Bone marrow aspirate smear showing a giant pronormoblast with a large intranuclear inclusion. Note the size of this erythroid precursor in comparison with accompanying erythrocytes and lymphocyte (× 1250). (B) Immunohistochemical stain of the bone marrow biopsy, demonstrating numerous pronormoblasts positive for parvovirus B19 (× 250).
HSU, JACK W.. CZADER, MAGDALENA. ANDERS, VIKI. VOGELSANG, GEORGIA. BRODSKY, ROBERT A.. PARVOVIRUS B19-ASSOCIATED PURE RED CELL APLASIA IN CHRONIC GRAFT-VERSUS-HOST DISEASE. British Journal of Haematology. 119(1):280-282, October 2002

CROWLEY, BRENDAN 1. WOODCOCK, BARRIE 2. RED CELL APLASIA DUE TO PARVOVIRUS B19 IN A PATIENT TREATED WITH ALEMTUZUMAB. British Journal of Haematology. 119(1):279-280, October 2002.
Immune electron microscopy showing aggregates of parvovirus B19
particles in serum, confirming viraemia during the patient's illness.

Parvovirus B19other manifestations
Neutropenia Lymphopenia Thrombocytopenia Hemophagocytic syndrome Fetal infection
30% transplacental infection rate 9% second trimester loss rate 10-20% of nonimmune hydrops

Parvovirus B19Diagnosis
IgM antibodies in healthy individuals 3rd day of aplastic crisis Any rash Persist 2-3 months
Molecular detection in serum Direct dot-blot PCR (>108 copies/ml) May persist years in tissue, months in serum Bone marrow biopsy

British Journal of Haematology. 119(1):125-127, October 2002
Erythroblasts contain viral inclusions (thin arrows) at different stages of development. The giant proerythroblast on the left (thick arrow) demonstrates chromatin condensation at the periphery of the nucleus
and a central viral inclusion

Typical ‘gigantoproerythroblasts’ in parvovirus B19-associated PRCA. (A) Bone marrow histology with several gigantoproerythroblasts (marked by asterisks) that resemble Hodgkin cells. A small regressive erythroblast (marked with an arrow) typically contains the immunoreactive B19-antigen. (B) Bone marrow cytology of another patient with B19 infection showing two gigantoproerythroblasts (marked by asterisks).
British Journal of Haematology. 111(4-II):1010-1022, December 2000

Figure 2. Immunohistochemical stains using monoclonal antibodies against parvovirus highlight intranuclear inclusions (arrow) in erythroid precursors (×250). From: Pamidi: Transplantation, Volume 69(12).June 27, 2000.2666-2669


ParvovirusIsolation
Erythema infectiosum no longer viremic TAC requires droplet precautions for 7 days
or duration Pregnant HCWs should not care for patient

Case ReportOutcome
Transfused and quickly became asymptomatic
Discharged on Bactrim Follow-up Hgb 9.2 Cd4 178, viral load 220,00 Began non-AZT HAART regimen
(stavudine, lamivudine and efavirenz)