Embed Size (px)
Citation preview

Clinical Evaluation 101-A Key Requirement to Gaining Access to the European Market
Suzanne Halliday
BSI Healthcare
16.June.2011

22
Course Description:
Clinical evaluation is the assessment and analysis of clinical data pertaining to a medical device in order to verify the clinical safety and performance of the medical device.
In this session you will gain a basic understanding of Clinical Evaluation process which covers the totality of information used to demonstrate compliance and can include: Clinical Trial, Literature Review and Product Performance History.

33
Learning Objectives:
• Understand the European Regulatory Framework• Definition of Clinical Data• Learn the Clinical Evaluation Process• How the scope of data required is proportional to the
Risk of the Device • Obtain a listing of useful resources

MedDev 2.7.1 Dec 2009
http://ec.europa.eu/consumers/sectors/medical-devices/documents/guidelines/index_en.htm

5
MedDev 2.7.1 ≅ GHTF N2R8
• New EU additions – Clause 10 and Appendix F
• The role of the Notified Body in the assessment of clinical data:
10.1. Examination of a design dossier or type examination dossier
10.1.1 Decision-making by the Notified Body10.1.2 The report of the Notified Body
10.2. Evaluation as part of quality system related procedures
10.2.1 Review of the manufacturer’s procedures10.2.2 Review of samples and their technical documentation
10.3. Notified Body Specific Procedures and Expertise

6
Design Dossier (Annex II.4 & III) verification of:
1. Followed relevant Procedures, Standards & Guidance.
2. Verified Device Characteristics & Performance.
3. Completed Risk Analysis – Severity, Probability & Multidisciplinary Approach.
4. Identified, Appraised, Analysed & Assessed Clinical Data.
5. Addressed Relevance, Equivalence, Similarity & Limitations of Clinical Data.

Design Dossier (Annex II.4 & III) verification of:
6. Safety, Performance & Risk-Benefit – ERs 1, 3 & 6.
7. Demonstrated Conformity with Relevant ERs.
8. Provided relevant Clinical Investigation documents – CIP, Amendments, Ethics, Informed Consent, Case Report Forms, Regulatory Authority approval and Final Signed & Dated Report.
9. Provided Conclusions and Justifications.
10. Justified appropriateness of Post Market Surveillance includingPost Market Clinical Follow-up.
7

1. Followed relevant Procedures, Standards & Guidance
• Verify relevant procedures followed
• NB report should cover procedures and use of harmonised standards

9
GHTF N2R8 / MedDev 2.7.1 / * ISO 14155 (2011)Systematic Review GHTF
N2R8(2007)
MedDev 2.7.1(2009)
1. Objectives • Safety• Performance• Substantiated Claims
2. Identify3. Select – Similar or Equivalent4. Appraise / Review / Analyse / Weight5. Critically Evaluate6. Clinical Evaluation / Risk Management
Relationship7. Inclusion of PMS Information8. Conclusions9. References10. Qualifications
… Clinical Investigations … See #8.

2. Verified Device Characteristics & Performance.
• Verify characteristics and performance
• Evaluate validation of clinical claims
• NB report should cover description and product specification

11Primary total hip replacement surgery: a systematic review of outcomes 1998 – Health Technology Assessment NHS R&D HTA Programme

12Primary total hip replacement surgery: a systematic review of outcomes 1998 – Health Technology Assessment NHS R&D HTA Programme

13
Charnley, Müller, PCA, Ring, McKee-Farrar, Harris-Galante, Stanmore, Charnley-Müller, Lubinus, Exeter …
* Different Design Characteristics
* Different Clinical Performance

3. Completed Risk Analysis –Severity, Probability & Multidisciplinary Approach
• Verify risk analysis, estimates of side effects and involvement of clinicalexpertise in risk analysis
• NB report should cover risks identified by hazards, severity of hazardsand probability of occurrence of harm
15
Is reassessment of risk necessary? (9)
Yes No
Prepare risk management report (8)
Review production & post-production information (9)
EN ISO 14971:2009

Knees – Loosenings
25.0%
10.0%
27.0%
---
36.5%
33.0%
---
39.2%
38.0%
---
16
Knees – Fractures
2.0%
3.0%
---
---
5.2%
5.0%
---
1.0%
1.0%
---
Probability of Occurrence

17
Functional Area Signature Date
Information Systems 11/October/2008
Development Engineer 11/October/2008
Research 11/October/2008
Clinical 12/October/2008
Marketing 11/October/2008
Regulatory 12/October/2008
Multidisciplinary Approach

4. Identified, appraised, analysed & assessed Clinical Data
• Verify use of MedDev 2.7.1
• NB report should cover complete and adequate documentation perMedDev 2.7.1

19Unicompartmental Knee Arthroplasty for Unicompartmental Osteoarthritis: A Systematic Review. 2005 – ASERNIP – S
Identify

20
Include
Unicompartmental Knee Arthroplasty for Unicompartmental Osteoarthritis: A Systematic Review. 2005 – ASERNIP – S
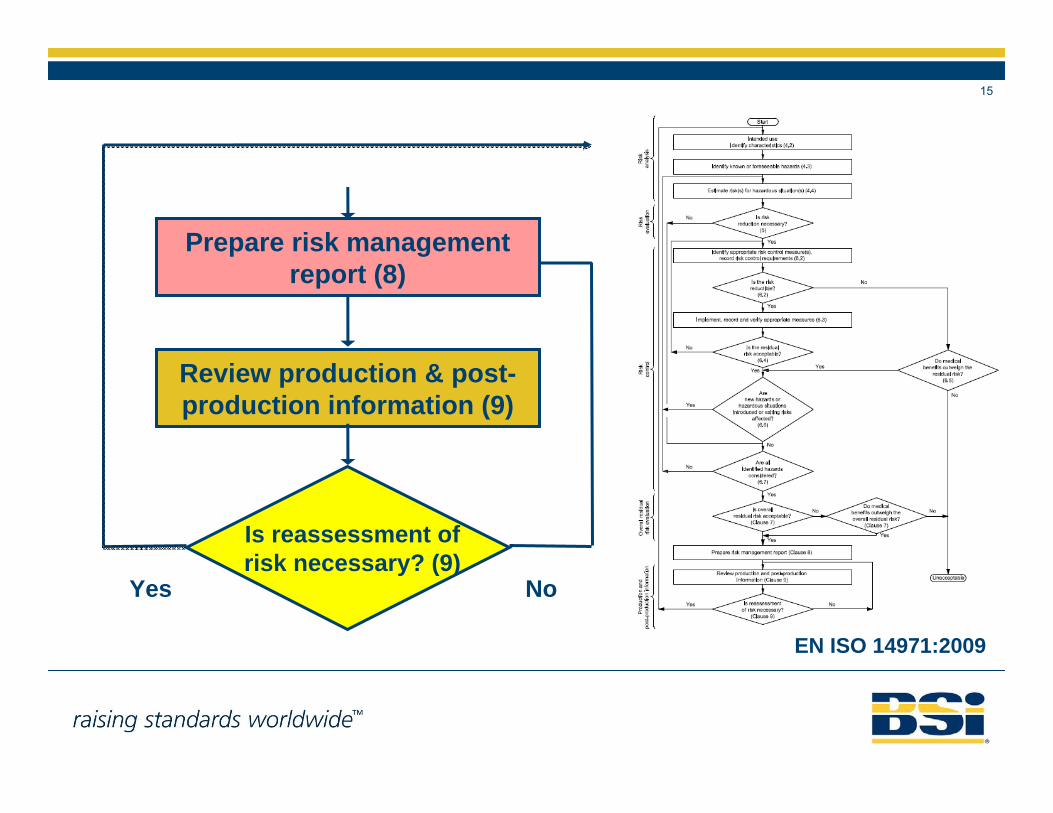
21
Exclude
Unicompartmental Knee Arthroplasty for Unicompartmental Osteoarthritis: A Systematic Review. 2005 – ASERNIP – S

22
Definitions
1. Appraise – to assess merits or quality.
2. Analyse – to examine something in great detail in order to understand it.
3. Assess – to examine something in order to evaluate it.

23
Appraise
Unicompartmental Knee Arthroplasty for Unicompartmental Osteoarthritis: A Systematic Review. 2005 – ASERNIP – S

24
Types of StudiesTherapeutic Studies—Investigating the Results of Treatment
Prognostic Studies—Investigating the Effect of a Patient Characteristic on the Outcome of Disease
Diagnostic Studies—Investigating a Diagnostic Test
Economic and Decision Analyses—Developing an Economic or Decision Model
Level I High-quality randomized controlled trial with statistically significant difference or no statistically significant difference but narrow confidence intervals
Systematic review of Level-I randomized controlled trials (and study results were homogeneous)
High-quality prospective study (all patients were enrolled at the same point in their disease with ≥80% follow-up of enrolled patients)
Systematic review of Level-I studies
Testing of previously developed diagnostic criteria in series of consecutive patients (with universally applied reference "gold" standard)
Systematic review of Level-I studies
Sensible costs and alternatives; values obtained from many studies; multiway sensitivity analyses
Systematic review of Level-I studies
Level II Lesser-quality randomized controlled trial (e.g., <80% follow-up, no blinding, or improper randomization)
Prospective comparative study
Systematic review of Level-II studies or Level-I studies with inconsistent results
Retrospective studyUntreated controls from
a randomized controlled trial
Lesser-quality prospective study (e.g., patients enrolled at different points in their disease or <80% follow-up)
Systematic review of Level-II studies
Development of diagnostic criteria on basis of consecutive patients (with universally applied reference "gold" standard)
Systematic review of Level-II studies
Sensible costs and alternatives; values obtained from limited studies; multiway sensitivity analyses
Systematic review of Level-II studies
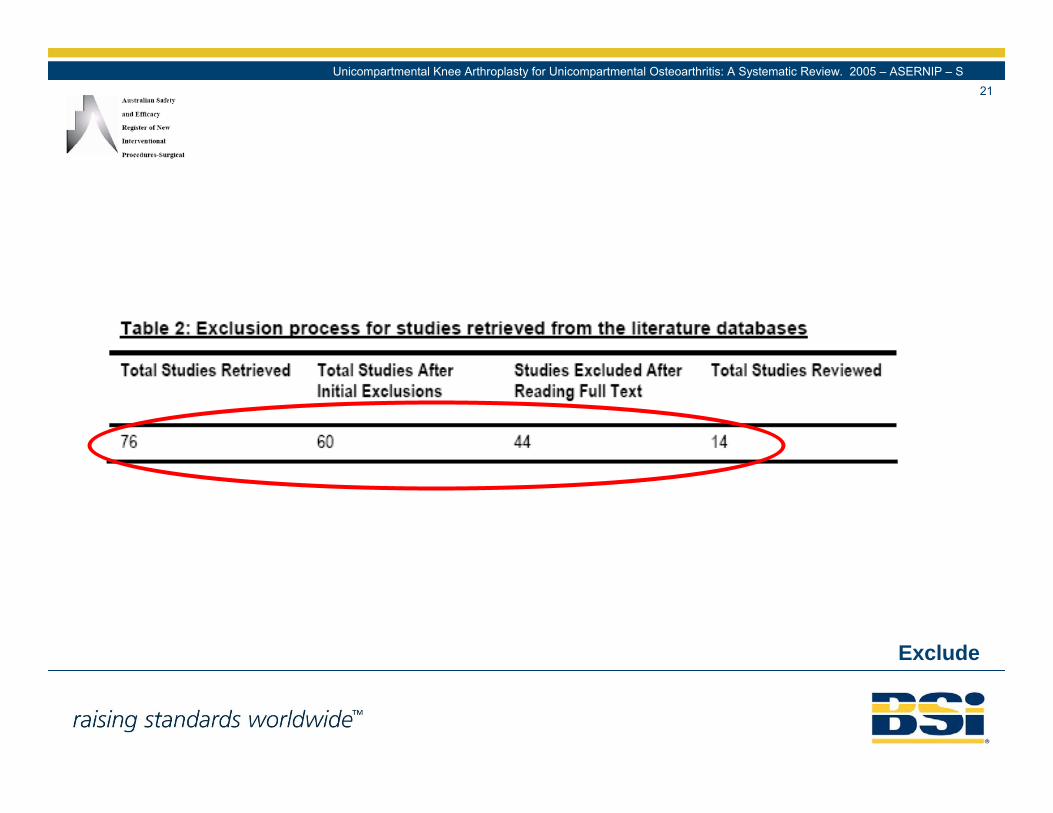
JBJS Levels of Evidence
25
Types of StudiesTherapeutic Studies—Investigating the Results of Treatment
Prognostic Studies—Investigating the Effect of a Patient Characteristic on the Outcome of Disease
Diagnostic Studies—Investigating a Diagnostic Test
Economic and Decision Analyses—Developing an Economic or Decision Model
Level III Case-control studyRetrospective comparative
studySystematic review of Level-
III studies
Case-control study Study of non-consecutive patients (without consistently applied reference "gold" standard)
Systematic review of Level-III studies
Analyses based on limited alternatives and costs; poor estimates
Systematic review of Level-III studies
Level IV Case series Case series Case-control studyPoor reference
standard
No sensitivity analyses
Level V Expert opinion Expert opinion Expert opinion Expert opinion
JBJS Levels of Evidence

26
Analyse
Unicompartmental Knee Arthroplasty for Unicompartmental Osteoarthritis: A Systematic Review. 2005 – ASERNIP – S

27
Assess
Unicompartmental Knee Arthroplasty for Unicompartmental Osteoarthritis: A Systematic Review. 2005 – ASERNIP – S

5. Addressed relevance, equivalence / similarity & limitations of Clinical Data
• Verify relevance and inclusion of safety, performance and risks<benefits
• NB report should cover suitability of data, limitations of data and validity of any justifications

29State of the Science on Implant Dentistry. 2006 – The International Journal of Oral & Maxillofacial Implants
Relevance

30
“Implants” ?????
Equivalence / Similarity

31
“Equivalent” or “Similar”:Clinical:
• same clinical condition or purpose• same site in the body• similar population (including age, anatomy, physiology)• similar relevant critical performance for specific intended use
Technical:
• similar conditions of use• similar specifications and properties • similar design• similar principles of operation
Biological:
• same materials in contact with the same tissues or body fluids
Checklist

32
“Implants” ?????
Limitations

6. Addressed safety, performance & risk-benefit –ERs 1, 3 & 6
• Verify relevance and inclusion of safety, performance and risks<benefits
• NB report should cover suitability of data, limitations of data and validityof any justifications

34Evidence Report/Technology Assessment – Total Knee Replacement. 2003 – Agency for Healthcare Research and Quality.
Demographics
35
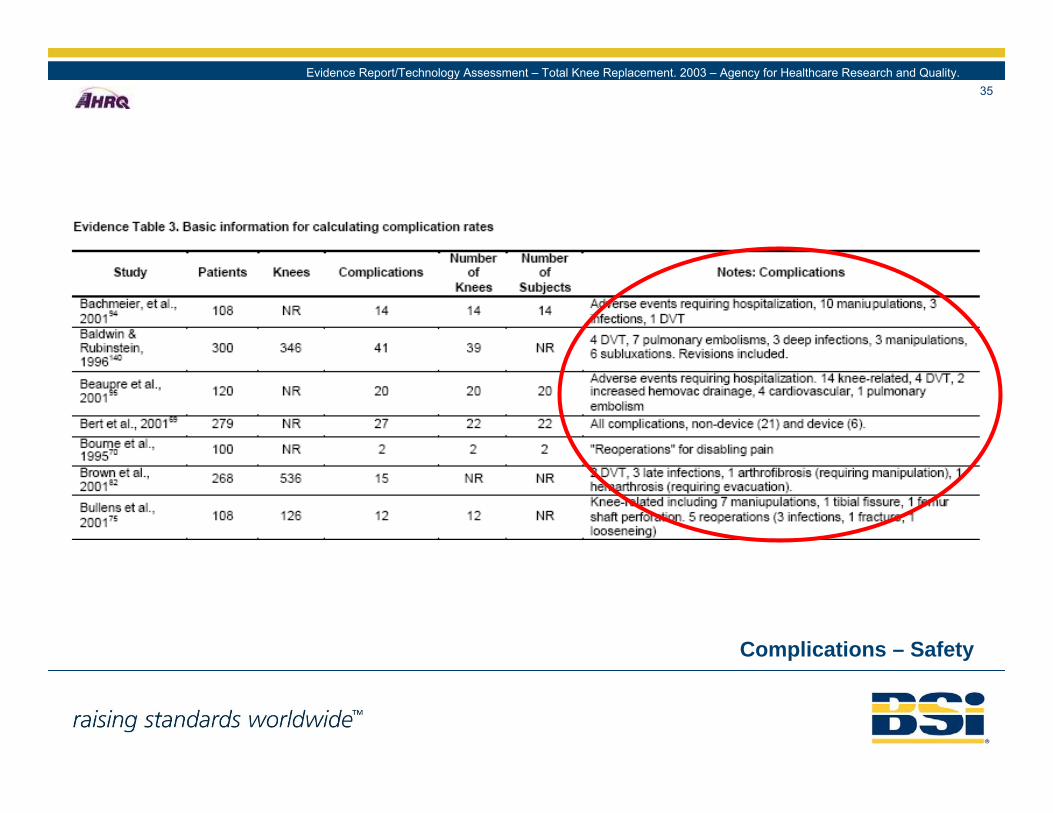
Complications – Safety
Evidence Report/Technology Assessment – Total Knee Replacement. 2003 – Agency for Healthcare Research and Quality.
36
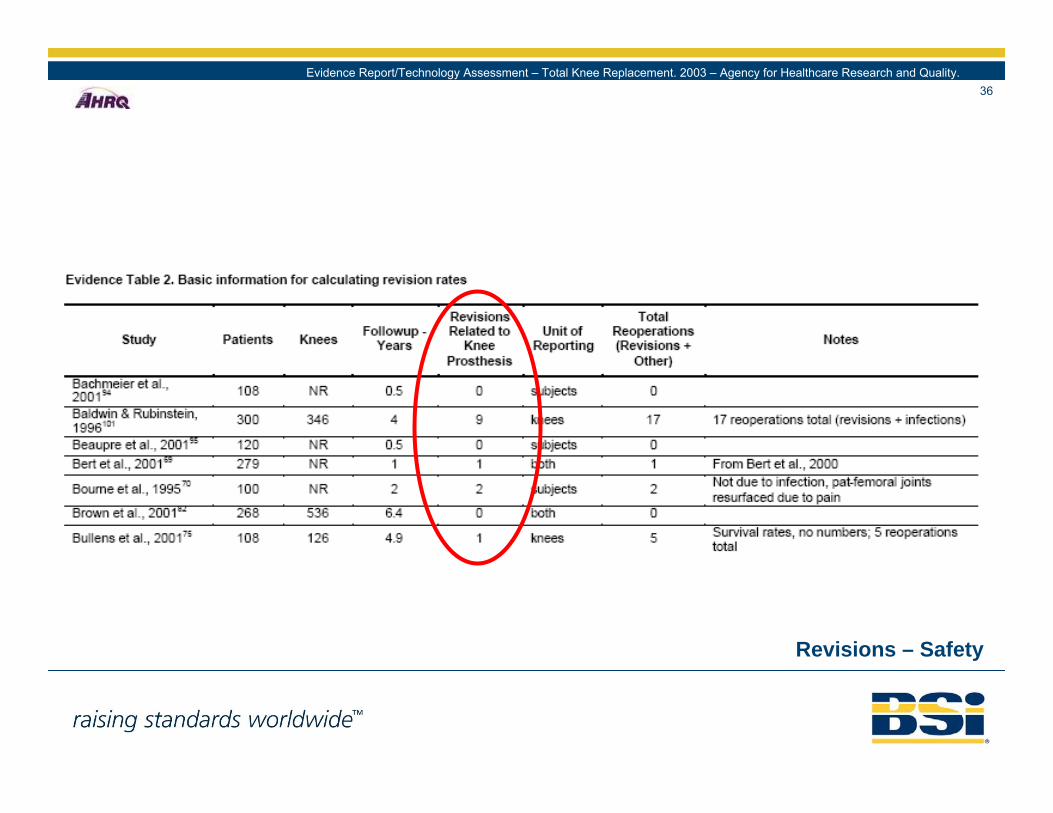
Revisions – Safety
Evidence Report/Technology Assessment – Total Knee Replacement. 2003 – Agency for Healthcare Research and Quality.
37
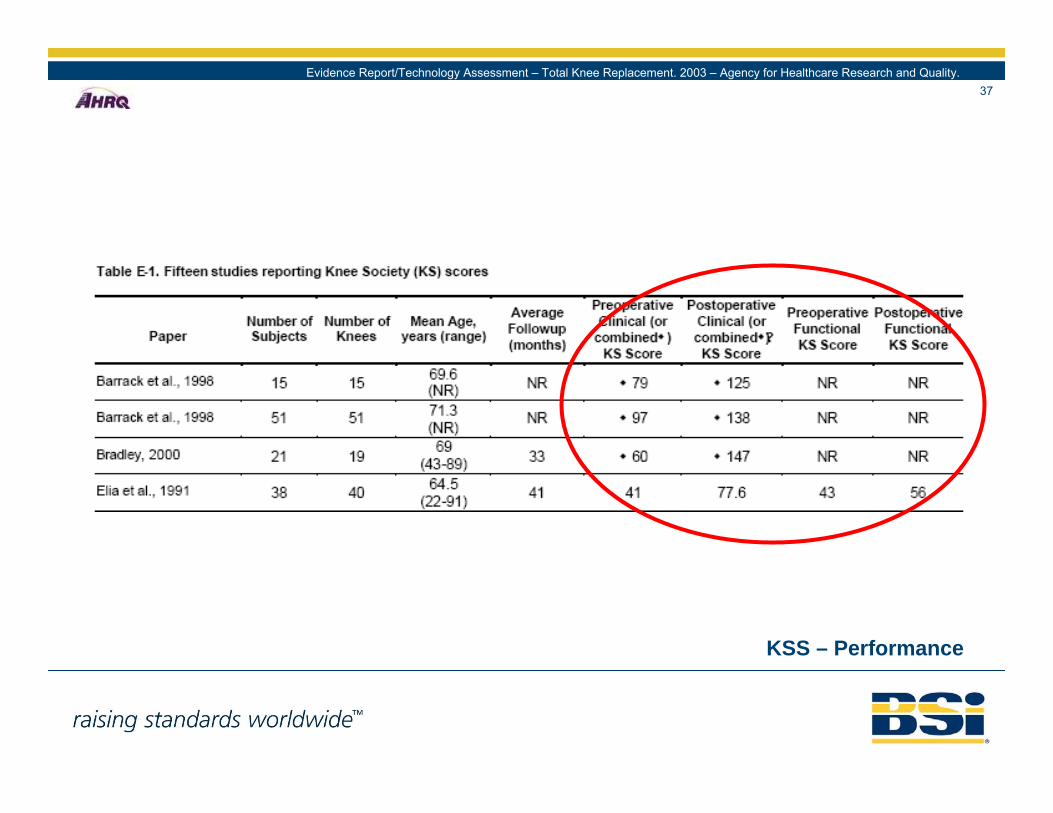
KSS – Performance
Evidence Report/Technology Assessment – Total Knee Replacement. 2003 – Agency for Healthcare Research and Quality.

38
HSS – Performance
Evidence Report/Technology Assessment – Total Knee Replacement. 2003 – Agency for Healthcare Research and Quality.

39
Risks < Benefits
RISKS
BENEFITS

7. Demonstrated conformity with relevant ERs
• Verify data meets relevant ERs
• NB report should cover proof of clinical performance and expected benefits