Embed Size (px)
Citation preview

correspondence
954 volume 41 | number 9 | september 2009 | nature genetics
CLCN2 variants in idiopathic generalized epilepsyTo the Editor: In 2003, we reported that mutations in CLCN2, the gene encoding the voltage-gated chloride channel ClC-2, are associated with the four major subtypes of idiopathic generalized epilepsy in three pedi-grees with an apparent autosomal dominant mode of inheritance. We concluded that these mutations confer a major gene effect. The observed heterogeneity of the epileptic phe-notypes prompted us to suggest that other, unknown genes might also be involved, in agreement with complex inheritance1.
Re-examination of the families and the molecular genetic data by a neurologist and a geneticist who were not involved in the origi-nal study has now revealed major differences from the published data in two of the three published pedigrees (presented in Figs. 1a and 1b of the aforementioned publication1), which are described in detail below. All stud-ies were approved by the Ethics Committee of the University of Bonn and informed consent was obtained from all subjects.
In the previously published pedigree of Family 1 (ref. 1), the identified mutation co-segregates in an autosomal dominant man-ner in five affected family members. Three of these were indicated to be suffering from juvenile myoclonic epilepsy (JME) and one from epilepsy with grand mal (also known as generalized tonic-clonic) seizures on awaken-ing (EGMA), and one was reported as show-ing generalized spike and wave discharges on an EEG without being clinically affected (Fig. 1a).
The family was re-contacted and re-ana-lyzed. This second evaluation revealed that only the index case had JME. She reported clas-sical bilateral myoclonic jerks on awakening since the age of 17 and one generalized tonic-clonic seizure in the morning that occurred when she was 18 years of age. She has been treated with valproate and has since remained seizure free for more than 15 years. EEG recordings were available only from the period when she was receiving valproate, and they did not show epileptic discharges. No other family members were reported as suffering
from epileptic seizures, and the pedigree structure was found to be different from that initially described (Fig. 1b).
We re-collected blood samples from nine available family members (Fig. 1b). The family structure was re-evaluated through molecu-lar fingerprinting with 15 highly polymorphic STR markers and one sex-specific marker (Powerplex 16, Promega). The family struc-ture obtained through the second recruit-ment proved to be correct. Re-sequencing of the CLCN2 gene revealed the published mutation c.597insG (p.M200fsX231) in three family members (the index patient, her unaffected sister and her unaffected father). Furthermore, three of the original DNA sam-
ples with the mutation proved to stem from one individual.
The previously published pedigree of Family 2 (ref. 1) indicates an autosomal dominant form of epilepsy with eight affected members. The index case was reported as suffering from childhood absence epilepsy (CAE), his sister as showing generalized spike and wave discharges on the EEG without being clinically affected, five other family members as suffering from EGMA, and the deceased great-grandfather of the index case was reported to have had unclas-sifiable epileptic seizures (Fig. 1c).
The family was re-contacted and the clinical phenotypes were re-evaluated using informa-tion obtained from the parents of the index
I
II
III
IV
1 2
1 2 +/m JME
1 2 3 +/+ +/m +/+ JME
1* 2 3* 4 +/m +/+ +/m +/m JME EGMA sw/psw-EEG
I
II
III
IV
1 2 +/+
1 2 3 4 5 +/m +/+ +/m +/+ ? EGMA
1 2 3 4 5 6 7 8 9 10 11 12 13 +/m +/+ +/+ +/+ +/+ +/m +/+ +/m +/+ +/m +/+ +/+EGMA EGMA EGMA unaffected
1 2 3 4* 5* 6 7 8 9 +/m +/m +/m +/+ +/+ +/+ +/+ sw-EEG CAE EGMA
I
II
1 2 +/m +/+ ?
1* 2 3* 4 +/m +/m +/m +/+ JAE JAE sw-EEG
IGE
1 2
1 2 3 4 5
1 2 3 4 5 6 7 8 9 10 11 12 13
1 2 3 4 5 6 7 8 9
I
II
III
IV
II
III
IV
+/m
+/+
+/++/++/+
+/+ +/+
+/m +/m
1 2 3 4
1 2 3 4
1 2
JME
a
b d
c e
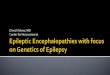
Figure 1 Family pedigrees. Pedigrees are shown as originally published (a,c,e) and after clinical and genetic re-analysis (b,d). (a) Family 1 as originally published in Figure 1a of ref. 1. (b) Family 1 as defined by the second recruitment. The mutational status shown was determined from the freshly collected blood samples. (c) Family 2 as originally published in Figure 1b of ref. 1. (d) Family 2 following re-evaluation of the clinical phenotypes. (e) Family 3 as originally published in Figure 1c of ref. 1 and as confirmed now. Asterisks in a,c,e mark individuals selected for mutation screening in the original study. IGE, idiopathic generalized epilepsy; CAE, childhood absence epilepsy; JME, juvenile myoclonic epilepsy; EGMA, epilepsy with grand-mal seizures on awakening; sw/psw-EEG, subclinical generalized spike-wave (sw) and/or polyspike-wave (psw) discharges in EEG recordings; +/+, individuals carrying two WT alleles; +/m, heterozygous mutation carriers.
©20
09 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.

correspondence
nature genetics | volume 41 | number 9 | september 2009 955
case and from written medical reports. The re-evaluation revealed the same pedigree structure, but only the index case and his great-grandfather were reported as suffering from epilepsy. The index case had one pro-longed epileptic seizure at five years of age that was witnessed by his mother, who described initial staring and unresponsiveness. He was still able to walk to the car but then developed clonic movements of the legs, automatisms of the hands, deeper breathing and urine loss en route to the hospital. Several EEG record-ings revealed bilateral frontal and generalized epileptic discharges, partially associated with probable myoclonic jerks of the arms. He was treated with valproate, which was discontin-ued after 2.5 years, and has remained seizure free (he is currently 14 years of age). We have now classified this type of epilepsy as a prob-able form of idiopathic generalized epilepsy (IGE) without further specification. In a medical report, his sister was indeed reported to have had epileptic discharges on the EEG (as was also originally reported1). However, available descriptions of these EEGs, includ-ing a continuous 24-hour EEG, do not suggest unequivocal epileptic discharges. The original EEG recordings were not available for inspec-tion. According to the reports of relatives, the affected boy’s great-grandfather had suffered from epileptic seizures, though further details are not available. No other family members were reported to have suffered from seizures (see pedigree in Fig. 1d). It was not possible for the boy’s great-grandmother (I:2) to have been included in the mutation analysis, as she was deceased at the time of the initial recruit-ment.
The family did not consent to further blood sampling, and so the genetic re-analysis relied on the original 16 DNA samples. Re-sequencing of the CLCN2 gene revealed the published mutation IVS2-14del11 in 9 of the 16 samples. However, molecular finger-printing revealed that the 16 DNA samples originate from only ten different individuals. Three samples from male mutation carriers had been assigned to two individuals each, and four DNA samples from male individuals not carrying the mutation originate from one individual. Thus, the DNA samples remaining in the laboratory originate from ten differ-ent individuals, among whom there are three male and three female mutation carriers. The mutation carriers stem from at least two generations. It was not, however, possible to
unequivocally reconstruct the pedigree by use of molecular fingerprinting due to an insuf-ficient number of available samples.
The family structure of Family 3 (ref. 1) was confirmed through molecular fingerprinting using the original samples. The mutation c.2144G>A (p.G715E) was confirmed in the three affected siblings and their father, who was classified with an unclear clinical status (unclassifiable seizures during childhood). The father now has severe alcoholism, which probably accounts for his generalized tonic-clonic seizures in adulthood (Fig. 1e).
The results of our re-investigations make it necessary to retract the original publica-tion, since we cannot maintain that mutations in CLCN2 cause a major gene effect in these pedigrees. However, other major aspects of the publication remain unaltered. For multiple rea-sons, we still believe that the reported genetic variations may contribute to the epileptic phe-notypes, and that rare variants in CLCN2 could represent a susceptibility factor for idiopathic generalized epilepsy. (i) Electrophysiological studies revealed functional consequences of all these variants1. Subsequent studies in other laboratories defined additional functional alterations2,3 and supported some of the func-tional changes that were originally reported3,4. (ii) An additional 4,700 healthy individuals from Germany have since been screened for the three reported mutations (Sequenom sys-tem), and none were detected in any of them. It is obvious, therefore, that the three mutations are extremely rare in the German population. (iii) The findings in Family 3 with at least three affected mutation carriers proved to be correct. (iv) In a recent independent study, two addi-tional CLCN2 mutations were found in indi-viduals with idiopathic generalized epilepsy. The variants did not completely co-segregate with the epileptic phenotypes, but they were not detected in controls and had functional consequences as demonstrated in physiologi-cal investigations. It was concluded that the mutations may act as susceptibility factors for epilepsy among other unknown genetic altera-tions in the affected individuals5.
AUTHOR CONTRIBUTIONSThe reanalysis of the pedigrees was performed by A.K.-L. (clinical phenotyping and collection of blood samples) and by W.F. (molecular fingerprinting, mutation analysis). S.C. examined the sample of 4,700 individuals from the general population for the three reported mutations in the CLCN2 gene. P.P., C.E.E. and H.L. designed, coordinated and supervised the re-investigations. P.P. and H.L. wrote
the manuscript. All coauthors discussed the results of the re-investigations and revised the manuscript.
Ailing Kleefuß-Lie1, Waltraut Friedl2, Sven Cichon3, Karsten Haug4, Maike Warnstedt5, Alexi Alekov6, Thomas Sander7, Alfredo Ramirez8, Barbara Poser9, Snezana Maljevic10, Simon Hebeisen11, Christian Kubisch8,Johannes Rebstock12, Steve Horvath13, Kerstin Hallmann1, Jörn S Dullinger14, Birgit Rau1, Fritz Haverkamp15, Stefan Beyenburg16, Herbert Schulz17, Dieter Janz18, Bernd Giese19, Gerhard Müller-Newen20, Peter Propping2, Christian E Elger1, Christoph Fahlke6 & Holger Lerche10
1Klinik für Epileptologie, 2Institut für Humangenetik and 3Abteilung für Genomik, Life & Brain Center, Universität Bonn, Bonn, Germany. 4Pränatalmedizin und Genetik, Düsseldorf, Germany. 5Praxisklinik am Neumarkt Institut für Endokrinologie und Reproduktionsmedizin, Köln, Germany. 6Institut für Neurophysiologie, Medizinische Hochschule Hannover, Hannover, Germany. 7Cologne Center for Genomics and 8Institut für Humangenetik, Universität zu Köln, Köln, Germany. 9Institut für Physiologie, Rheinisch-Westfälische Technische Hochschule Aachen, Aachen, Germany. 10Neurologische Klinik und Institut für Angewandte Physiologie, Universität Ulm, Ulm, Germany. 11bSys GmbH, The Ionchannel Company, bSys Witterswil, Witterswil, Switzerland. 12Epilepsiezentrum Kleinwachau, Radeberg, Germany. 13Human Genetics and Biostatistics, University of California Los Angeles, Los Angeles, California, USA. 14Neurologische Klinik und Poliklinik, Campus Virchow-Klinikum, Charité-Universitätsmedizin Berlin, Berlin, Germany. 15Evangelische Fachhochschule Rheinland-Westfalen-Lippe, Bochum, Germany. 16Centre Hospitalier de Luxembourg, Département des Neurosciences, Luxembourg. 17Max-Delbrueck-Center for Molecular Medicine, Berlin-Buch, Berlin, Germany. 18Neurologie, Charité-Universitätsmedizin Berlin, Berlin, Germany. 19AG Angewandte Bioinformatik und Zellbiologie, Institut für Mikrobiologie der Universität Greifswald, Greifswald, Germany. 20Universitätsklinikum der RWTH Aachen, Institut für Biochemie, Aachen, Germany. Correspondence should be addressed to H.L. ([email protected]).
1. Haug, K. et al. Nat. Genet. 33, 527–532 (2003).2. Scott, J.W. et al. J. Clin. Invest. 113, 274–284
(2004).3. Niemeyer, M.I. et al. Physiol. Genomics 19, 74–83
(2004).4. Blanz, J. et al. J. Neurosci. 27, 6581–6589 (2007).5. Saint-Martin, C. et al. Hum. Mutat. 30, 397–405
(2009).
©20
09 N
atu
re A
mer
ica,
Inc.
All
rig
hts
res
erve
d.