Embed Size (px)
Citation preview

Circulating and Tissue Eosinophils
in Ulcerative Colitis
RALPH WRIGHT, M.D., D.PHIL., M.R.C.P., and SIDNEY C. TRUELOVE, M.D., F.R.C.P.
T IIERE HAVE BEEN isolated reports of eosinophilia in the circulating blood and in the tissues of patients with ulcerative colitis. Riisager I found a
drcula t ing eosinophilia in some patients with active ulcerative colitis, and this has recently been confirmed by Juhlin= and by Riis and Anthonisen.8 Tissue eosinophilia in the colon has been noted by most observers who have examined large numbers of histological sections from patients with ulcerative colitis. 4-v Eosinophilia has also been observed in the inflammatory exudate, s-10 and Riis and Anthonisen 3 found it more commonly in the exudate than in the blood.
T h e cause of the eosinophilia sometimes seen in ulcerative colitis is unknown but the frequent association of eosinophilia with allergic states II-a8 raises the possibility of an ,allergic disorder in this disease.
It has been suggested on clinical grounds that allergy to food, particularly milk, might be an etiological factor in ulcerative colitis. 14-1a In view of these reports we have studied the effect of various diets on the clinical course of the disease by means of a controlled clinical trial.
T h e results of the clinical trial and of the immunological studies relating to the clinical trial have been reported in detail elsewhere. 2°, 92 T h e present report deals with serial observations made on the level of circulating eosinophils in the peripheral blood of patients admitted to the clinical trial of diet. Rectal biopsies were taken simultaneously so that an at tempt could be made to quant i ta te the coincident infiltration of the tissues by eosinophils.
M A T E R I A L AND M E T H O D S
PATIENTS STUDIED
Seventy-seven patients with ulcerative colitis in relapse were distributed at random with respect to 3 diets--a milk-free diet, a gluten-free plus milk- free diet, and a dummy diet which was essentially normal. T h e patients were seen at monthly intervals for assessment and investigations which included rectal biopsy, total eosinophil count, and immunological studies. T h e initial relapse and subsequent relapses during the course of the trial were treated with a standard course of oral prednisolone 20 mg. daily and daily rectal infusions
From the Nuttield Department of Clinical Medicine, University of Oxford, Oxford, England.
1966 by HOEEER MEDICAL DIVISION * HARPER g: Row, PUBLISHERS, INCORPORATED, NeW York.
New Series, Vol. [I, No. II, 1966 831

Wrigh+ & Truelove
of 100 rag. hydrocortisone hemisuccinate, the oral prednisolone being used for 6 weeks and the local hydrocortisone for 8 weeks. If the response was poor, the dose was doubled. At the end of the year the patients were asked to go back to a normal diet.
T h e relative effect of the 3 diets on the clinical course of the disease was judged by the n u m b e r of relapses of ulcerative colitis developing dur ing the trial period.
~EosINOPHIL COUNT
Eosinophils were counted by the method of Dunger as modified by Hills e t al . 22 About 1 ml. of whole blood ,taken by venipuncture was placed in a tube containing heparin. Blood was drawn up into a leukocyte-counting p ipet to the "1" mark and the pipet was then filled with an eosin-acetone d i lu t ing fluid and allowed to stand for 10 min. After mixing in the pipet, a few drops of the contents were transferred to a Fuchs-Rosenthal counting chamber 0.2 ram. in depth. T h e prepara t ion was allowed to stand for a few minutes and the number of eosinophils in the ruled area on both sides of the chamber were counted. For practical reasons it was possible for only one count to be made on each specimen. T h e total n u m b e r of leukocytes was not counted.
T h e figures shown in the tables are for the actual n u m b e r of eosinophils coun, ted. T o convert these numbers to the count per cubic mil l imeter of blood it is necessary to mult iply by a factor of 1.5626. An actual count greater than 140 eosinophils has been regarded as abnormal ly high for the purpose of this study. I f converted to eosinophils per cubic millimeter, this represents a count of 218, which is a little above the accepted upper l imit of normal (200/cu. ram.) for the method. 22
T h e eosinophils were counted by a technician who was unaware of the clinical state of the patients or of the nature of their diet.
RECTAL BIOPSY
Rectal biopsy specimens were obtained at sigmoidoscopy 4-6 inches f rom the anal verge using a Truelove-Salt suction biopsy instrument . T h e biopsy specimens were fixed in 10% formolsaline and embedded in paratfin wax. Serial sections were cut from each specimen and stained with hematoxyl in and eosin.
Each specimen was given a code num ber which was the same as that of the specimen of blood taken for the eosinophil counts and immunological studies. T h e histologic sections were examined by one observer without knowledge of the clinical state of the ulcerative colitis or the nature of the diet.
T h e degree of inf lammation in each specimen was classified as not significant, mild, moderate, or severe on the basis of the classification of True love and Richards. 4 Infi l t rat ion of the rectal biopsy specimens with eosinophils was graded as absent, doubtful, 1+, and 2+.
T h e distinction between the different grades was not clear-cut. However,
8 3 2 American Journal of D~cjes÷ive Diseases

Eosinophils in Ulcerative Colitis
repeat examinat ion usually produced closely similar results and there was close agreement when a sample was checked by a second observer using the same criteria.
R E S U L T S
T h e milk-free diet was superior to the gluten-free plus milk-free and dummy diets. More patients on the milk-free diet remained well for the year than on the other diets, and fewer had repeated relapses. From the figures, the best estimate appeared to be that a milk-free diet is likely to be beneficial to about 1 in 5 patients with ulcerative colitis, with a suggestion that the propor t ion might be higher in patients in their first at tack of the disease.
T h e results obtained with the milk-free plus gluten-free diet were similar to those obtained with an ordinary diet, bu t it was thought that the relative failure of this group was due to the fact that patients found it difficult to adhere to the diet strictly and that milk protein had inadvertently been included in the diet.
CIRCULATING EOSINOPHILS
T h e actual number of eosinophils counted was recorded on special charts on which the clinical data obtained dur ing the trial had already been noted. I t was therefore possible to obtain some informat ion by inspection of the charts.
The following tentative conclusions could be drawn in this way: 1. In the individual patient, fluctuations in the eosinophil count occurred
from one observation to the next, bu t some patients consistently ran a higher count than others (Fig. I ) .
2. In some patients there was a marked rise in the eosinophil count dur ing a clinical relapse of the ulcerative colitis (Fig. 2).
3. T rea tmen t with systemic corticosteroid drugs almost invariably produced a marked fall in the eosinophil count, bu t the count often rose when systemic t reatment was discontinued (despite the cont inued use of local corticosteroid therapy) .
4. There was no consistent change in the eosinophil count after patients who had been on a milk-free diet with or without a gluten-free diet were challenged with the proteins which had been excluded. However, in 2 patients who had a frank clinical relapse of the ulcerative colitis after challenge with milk, there was, in association with the relapse, a rise in the eosinophil count to above the levels dur ing remission.
Relationship to the Clinical Activity of the Ulcerative Colitis
In Tab le 1 the nu m ber of occasions on which an abnormal ly high eosinophil count was observed is related to the clinical state of the colitis and to t reatment with corticosteroid drugs. This shows that the n u m b e r of high eosinophil counts was greater dur ing a relapse of the ulcerative colitis than dur ing a re- mission, but the difference is not statistically significant (X2~ = 2.63; P > 0.05). An abnormal ly high eosinophil count was rare dur ing t reatment with corti-
New Series, Vol. 11, No. 11, 1966 833

25
0~
N.,
~~
'~
.......
Rec
tal b
iop
sy.
Cor
ticos
tero
id
trea
tmen
tl
J ¢
O
H.L
, ~-
'."~'!'?
,l M
oder
ate.
~
'x~
Sy
stem
ic *
loc
al,
0--
-@
J.S
. ~
M
ild.
m
Loca
l only
. R
elap
sl
....
tx
M
S.
/
20(
I 1
Nor
mal
. /
),,
, %
~ M
ilk-f
ree
diet
. /
, j
/
u 15
1 ~
/ .
, I/
~
/ i
-" R
elap
,se
I "a
I
I .-.
~'"
" " .
...
~"
~,
t --
-~
....
...
~-
- I
I I
I I
I I
,,1,,
I 1-
-.
• t
I ,
I I
....
0 0-
5 1
2 3
4 5
6 7
8 9
10
11
12
Mon
ths.
M
ilk
chal
leng
e.
H.L
j~
.!:.': I
E///
;U//~
~
r--I
1
7~
~
1~
~
[7-/-
-/Jl
we
lt.
Rel
apse
.
J.S,
~ I--
'I r-
-]
i i
~ ~
M.D.
17-
///F-/-
~ ~
I I
I 1
~ ~
I I
~"V*
/~]~
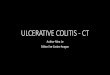
Fig
. 1.
C
ircu
lati
ng e
osin
ophi
t co
unt
in
peri
pher
al
bloo
d,
and
seve
rity
of
infl
amm
atio
n in
re
ctal
bi
opsy
spe
cim
ens
in
3 pa
tien
ts
who
rem
aine
d w
ell
on m
ilk-
free
di
et
duri
ng
tria
l pe
riod
.

Eoslnophils in Ulcerative Colitis
costeroid drugs. High counts were slightly more common when local corti- costeroid t reatment alone was being used, than when systemic corticosteroid drugs were being given in addition. These differences are independent of the type of diet to which the patients adhered.
Figure 3 records the difference between the eosinophil count dur ing a relapse and the previous eosinophil count when the pat ient was in remission. (Obser- vations made while the patients were on corticosteroid t reatment are ex- cluded.) This shows that the eosinophil count is more likely to rise than to fall during a relapse. A difference greater than 50 between the two counts was significantly more common when there was a rise in the eosinophil count than when it fell (X2~ ---- 3.976; P < 0.05), as shown in Tab l e 2. This suggests that there is a relat ionship between the eosinophil count and the activity of the disease.
However, when compar ing the eosinophil count dur ing a clinical relapse with that dur ing a clinical remission of the colitis, no account is taken of the
250
c
8 -- 2 0 0
c .c
160 I , I \ '
100 I I I I )
I I ) I I I
I I I I 2 5 7 8 9
Recta) biopsy. Cort icosterotd t r e a t r r ~ n t
I lIIUlIII s~ ..... ~ Sy,te~i:.io~,L
1171-A ..~.
I I I I I 1 I , i / ~ . . . . . ~ o . . j . o J.L
0 0"5 1 3 4 6 10 11 12 Months.
Recta[
b,op~y IIIlUU - I - -1 ES] ~ ~ ~ ~ - ~ ~ - Tissue -+ - + - eos inophJ Is
Fig. 2. Circulating eosinophil count in peripheral blood, and severity of inflammation in rectal biopsy specimens in patient J.L., illustrating marked rise in eosinophil count during relapse of colitis.
New Series, Vol. I I , No. 11, t966 835

Wright & Truelove
fact t ha t h i s to logic evidence of ac t iv i ty of the u lcera t ive coli t is is of ten p resen t in the absence of symptoms. A be t t e r i n d i c a t i o n of the r e l a t i o n s h i p of the eos i noph i l coun t to the ac t iv i ty of the disease m i g h t the re fo re be o b t a i n e d by c o m p a r i n g the counts d o n e at a t ime when the rec ta l b iopsy a p p e a r a n c e s were n o r m a l w i th those when the b iopsy was a b n o r m a l . Because cor t i cos te ro id t reat- m e n t affects the eos inoph i l count , this compa r i son was m a d e on ly on those pa t i en t s who r e m a i n e d wel l t h r o u g h o u t the year. E o s i n o p h i l counts f rom the s ix th to the twel f th m o n t h s were r e l a t ed to the b iopsy a p p e a r a n c e a n d com- p a r e d wi th the in i t i a l eos inoph i l coun t t aken d u r i n g re lapse at the t ime of admiss ion to the t r ial . T a b l e 3 shows tha t eos inoph i l counts d u r i n g remiss ion at the t ime of a n o r m a l rec ta l b iopsy were s ignif icant ly lower t h a n d u r i n g the in i t i a l r e lapse (X~ ---- 8.396; P < 0.01). Eos inop h i l counts d u r i n g c l in ica l re- miss ion at the t ime of a n o r m a l rec ta l b iopsy were also s igni f icant ly lower than counts t aken in remiss ion when the b iopsy was a b n o r m a l (Xe,, = 6.157; P < 0.05). Pa t i en t s on cor t icos te ro id t r e a t m e n t were e x c l u d e d a n d on ly those ob- servat ions m a d e be tween the s ix th a n d twe l f th m o n t h s were used to assess the
TABLE I. RELATIONSHIP OF EOSINOPHIL COUNT, CLINICAL ACTIVITY OF ULCERATIVE COLITIS, AND TREATMENT WITH CORTICOSTEROIDS
No. of patients
On treatment Circulating eosinophil With systemic With local
count In remission* In relapse* corticosteroids corticosteroids
M I L K - F R E E DIET
<140 146 26 56 41 140+ 23 20 2 2
TOTAL 169 46 58 43
D U M M y DIET
<140 I03 33 65 41 140+ 20 22 4 4
TOTAL 123 55 69 45
G L U T E N - F R E E j MILK-lZREE DIET
<140 126 42 74 37 140+ 24 12 3 5
TOTAL 150 54 77 42
ALL DIETS
<140 375 I01 195 119 140+ 67 (15.1%) 54 (34.8%) 9 (4.4%) 11 (8.5%)
TOTAL 442 155 204 130
*Not on treatment.
836 A,~r~c~n Journal of Diaesfive Diseases

Eosinophils in Ulcera÷ive Coil÷is
relat ionship in remission so as to exclude the possibility of a p ro longed effect of the init ial t reatment . T h e r e was little difference in the counts when the biopsy specimen was abnormal , whether taken du r ing clinical remission o r du r ing a relapse. T h e differences are i l lustrated in Fig. 4.
Fig. 3. Distribution of pa- tients (circles) according to amount by which eosinophil counts rose or fell during a re- lapse of ulcerative colitis (rela- tive to counts taken during re- mission immediately preceding relapse) .
IO0
< B0
= 5c o
40 Z
5 20
Z D
o 0 u
..a
o 20 Z N o, z 40
60
z
8O
100
0 0 0 0 0 0
~O
o 1_3
o o
8o o
80 {~ 2O
8 18
o
_2
Relationship to the Relapse Rate
In Tab le 4 the init ial eosinophi l count in pat ients who were no t receiving cort icosteroid t rea tment is related to the subsequent relapse rate. Th i s shows that the eosinophil count has no bear ing on the short- term prognosis as j udged by the relapse rate du r ing the fol lowing 12 months . T h e dis t r ibut ion was similar in the 3 die tary groups. Fur thermore , the initial eosinophi l count~ in 6 patients in w h o m there was good clinical evidence of milk in to lerance were 18, 25, 48, 78, 114, and 216, which shows a scatter s imilar to that in t he series as a whole. T h e eosinophi l count is, therefore, of no value in p red ic t ing the response to a milk-free diet.
Relationship to Diet
T h e possibility that diet may have bad an effect on the eosinophi l c o u n t d u r i n g the course of the trial has been examined. In T a b l e 5 the p r o p o r t i o n
New Series, VoI. I I, No. I I , 1966 8 3 7

Wright & Truelove
of abnormal ly h igh eosinophi l counts du r ing relapse of the ulcerat ive colitis is compared wi th respect to diet. Those on a milk-free diet tended to have a h igh coun t du r ing relapse somewhat more f requent ly than the pat ients on the o the r diets, bu t the difference is no t significant. T h e eosinophi l coun t appeared to differ significantly in re la t ion to diet in only one way: a greater n u m b e r of low counts (below 50) were recorded in pat ients who had remained well on a milk-free diet than in those on a d u m m y diet (Table 6) .
TISSUE ]~OSINOPHILS
A n average of approx ima te ly 8 serial biopsy specimens were examined f rom each pa t ien t (633 biopsy specimens f rom the 77 pa t ien ts ) .
I n T a b l e 7 the presence of tissue eosinophi l ia is re la ted to the clinical ac- t ivity of tile colitis. I t is shown that pat ients wi th ulcerative colitis in relapse were more likely to have tissue eosinophil ia than those in remission, bu t the difference is no t as marked as in the case of the c i rcula t ing eosinophils. In- fi l tration of the tissues wi th eosinophils tends to decrease du r ing t r ea tment with corticosteroids.
T a b l e 8 shows tha t there is no re la t ionship between the degree of infi l t rat ion of the initial biopsy specimen with eosinophils and the subsequent relapse rate.
TABLE 2. DISTRIBUTION OF PATIENTS ACCORDING TO DIRECTION AND SIZE OF CHANGE*' IN CIRCULATING EOSINOPHIL COUNT DURING RELAPSE OF
ULCERATIVE COLITIS
Eosinophil count change No. of patients
Rise <50 20
50+ 13 Fall
<50 18 50+ 2
X~c = 3.976; P < 0.05 #Relative to count immediately preceding relapse.
TABLE 3. RELATIONSHIP OF THE CIRCULATING EOSINOPHIL COUNT TO RECTAL BIOPSY APPEARANCE DURING REMISSION AND DURING THE INITIAL
RELAPSE IN PATIENTS WHO REMAINED WELL FOR 1 YEAR
Eosinophil count
Biopsy appearance <100 100+ Significance of difference
Abnormal in relapse 9
Normal in remission 50
Abnormal in remission 14
9 ~ X2~ = 8.390 8 ~ P < 0.01
1 X~c = 6.157 lO P < 0.05
838 American Journal of Digestive Diseases

Eosinophils in Uleeratlve Colitis
RELATIONSHIP OF CIRCULATING EOSINOPI-nLS TO TISSUE IEosINOPHILS
Table 9 and Fig. 5 show the relationship between circulating and tissue eosinophils dur ing remission and during relapse of the ulcerative colitis and while the patient was being treated with corticosteroid drugs. I t can be seen
Fig. 4. Relationship of cir- culating eosinophil count to rectal biopsy appearance dur- ing remission and during ini- tial relapse in those patients who remained well for 1 year.
I00 o
~ 8o
r
~ 60
o
c~ 4o
u .~- 20 C)
0 Abnormal in Normal in
remission. retapse.
[ • EO$ir tophi l COUnt
less than 100.
Eosinophi l count - - t'~x'xI 100 or more
Abnormat in remission.
that although a high circulating eosinophil count is frequently associated with an excess of eosinophils in the biopsy specimen, approximately half the patients with marked tissue eosinophilia had a circulating count of less than 140.
DISCUSSION
T h e present study confirms the observation first emphasized by Riisager 1 that some patients with ulcerative colitis have an increase in circulating eosino- phils in the peripheral blood during a relapse of the illness.
I t has been shown that the eosinophil count was above the upper limit of normal in approximately one-third of the attacks in which a count was made before corticosteroid treatment was started. This suggests that there is a re- lationship between the eosinophil count and the activity of the disease.
A more accurate estimate of the frequency with which an increase in eosinophils in the peripheral blood occurs during an active phase of the disease might be obtained by relating the eosinophil count during a relapse to the patient 's own "normal" range during remission. For example, in pat ient M.D. (Fig. 1) the eosinophil count during the relapse provoked by milk was greater than at any time dur ing the period of freedom from symptoms although the count was only 60.
Because of the high relapse rate and the effect of corticosteroid drugs on circulating eosinophils, it has been possible to study the relationship between the eosinophil count in complete remission and the eosinophil count during
New Series, Vol. I I , No. I I , 1966 8 3 9

TA
BL
E
4.
DIS
TR
IBU
TIO
N
OF
P
AT
IEN
TS
A
CC
OR
DIN
G
TO
N
UM
BE
R
OF
R
EL
AP
SE
S
AN
D
INIT
IAL
V
AL
UE
S
OF
C
IRC
UL
AT
ING
E
OS
INO
PH
ILS
Cir
c~da
ting
eos
inop
hil
coun
t
No.
ol
re
laps
es
Milk
-fre
e,
Mil
k-[t
ee
diet
D
um
my
diet
gl
uten
.ire
e di
et
All
die
ts
<50
<
70 <
140
140-
+
<50
<
70 <
140
140+
<
50
<70
<14
0 14
0+
<50
<
70 <
140
140+
TO
TA
L
0 3
4 6
3 (9
) 1
2 2
2 (4
) 2
2 ~
2 (7
) 6
8 13
7
(20)
l
1 2
4 3
(7)
1 l
3 3
(6)
2 4
4 2
(6)
4 7
ll
8 09
) 2
1 2
2 1
(3)
1 --
(1
) 3
1 (4
) l
2 6
2 (S
) 3
1 1
(2)
3 3
4 5
(9)
4 4
4 1
(5)
7 7
9 7
(t6)
5 8
13
8 (2
1)
5 6
10
10
(20)
8
10
16
6 (2
2)
18
24
39
24
(63)
Fig
ure
in
par
enth
eses
is
tota
l in
gro
up
. *
Pat
ien
ts o
n co
rtic
oste
roid
tr
eatm
ent
at
the
tim
e of
the
eos
inop
hil
cou
nt
are
excl
uded
.

Eosinophils in Ulcera+ive Coli+is
activity of the disease in only a few of the pat ients in the series. Nevertheless, T a b l e 3 shows that there is a significant correla t ion between the biopsy appear- ance and the eosinophi l count . Th i s is clearly i l lustrated in Fig. 4.
T h e r e is good evidence that eosinophils antagonize his tamine and, since h is tamine is l iberated at the site of an t igen-an t ibody reactions, this might account for the accumula t ion of eosinophils a,t the site of such reactions. 2z V a u g h n 24 suggested tha t the func t ion of eosinophils was to remove his tamine f rom the body, and Welsh and Gree t 2~ have demons t ra ted phagocytosis by eosinophils of the granules of mast cells, which are known to conta in hista- mine. I t is, therefore, of interest that mast cells as well as eosinophils are increased in the colon in ulcerative colitis. Accord ing to Archer, 2z the distribu- t ion of mast cells and eosinophils is no t parallel unless the former have become degranu la ted and are releasing histamine.
Speirs believes that the func t ion of the eosinophi l is no t s imply that of detoxi- fication, bu t is direct ly concerned in an t ibody synthesis by t ranspor t ing ant igen to an t ibody- forming cells. 26, 2r However , Sabesin 2s used electron microscopy to demons t ra te phagocytosis of ferr i t in-ant ibody complexes by eosinophils, and conc luded tha t this may merely represent a specific a t t ract ion of eosinophils by i m m u n e complexes, and that they need no t be impl icated in the p roduc t ion of an t ibody or the media t ion of the hypersensit ive state.
Th i s does no t resolve the quest ion of the significance of c i rculat ing and tissue
TABLE 5. DISTRIBUTION OF PATIENTS %TITH CIRCULATING EOSINOPHIL COUNT OF GREATER THAN I40 AT TttE TIME OF RELAPSE DURING THE TRIAL
Circulating eosinophil count
Gluten-free, No. of Milk-free diet Dummy diet milk-free diet All diets
relapses >140 >140 >140 >140
1 4 ( 9 ) 4 ( 8 ) 0 (5 ) 8 (22) 2 2 (7) 2 (6) 2 (I0) 6 (23) 3 6 (9) 6 (21) 4 (17) 16 (47)
TOTAL 12 (25) 1~ (35) 6 (32) 30 (92)
Figure in parentheses is total for group. *The initial relapse at the time of admission to the trial and values while on corticosteroid
treatment are excluded.
TABLE 6. DISTRIBUTION OF SYMPTOM-FREE PATIENTS NOT ON CORTICO- STEROID TREATMENT IN RELATION TO CIRCULATING EOSINOPHIL COUNTS
Eosinophil count
Diet <50 504-
Milk-free Dummy Gluten-free plus milk-free
49 45 ~ X2, = 6.196 13 33 ~ P < 0.05 25 47
New Series, Vol. I I , No. I I , 1966 841

TA
BL
E 7
. D
IST
RIB
UT
ION
O
F P
AT
IEN
TS
AC
CO
RD
ING
T
O
RE
LA
TIO
N
OF
TIS
SU
E E
OS
INO
PH
ILIA
IN
T
HE
R
EC
TA
L
BIO
PS
Y
SP
EC
IME
NS
A
ND
T
HE
C
LIN
ICA
L
AC
TIV
ITY
O
F
TH
E
UL
CE
RA
TIV
E
CO
LIT
IS
Deg
ree
of t
issu
e eo
sino
phil
ia
Glu
ten-
free
, M
ilk-
free
die
t D
umm
y di
et
mil
k-fr
ee
diet
A
ll d
iets
--
± +
++
--
±
+ +
+
--
+__
+ +
+
--
± +
++
In r
emis
sion
56
14
18
b
(93)
34
13
22
11
(8
0)
47
20
16
3 (8
6)
(not
on
trea
tmen
t)
In r
elap
se
(not
7
7 14
4
(32)
11
11
14
8
(44)
8
16
13
1 (3
8)
on t
reat
men
t)
On
trea
tmen
t 25
12
12
--
(4
9)
15
23
20
3 (6
1)
13
15
11
2 (4
1)
wit
h sy
stem
ic
cort
icos
tero
ids
On
trea
tmen
t 18
8
3 2
(31)
12
6
9 3
(30)
14
4
7 --
(2
5)
wit
h lo
cal
cort
icos
tero
ids
1375
2.9%
47
18.
2% 5
621.
6%
19
7.3%
(2
59)
2622
.8%
34
29.8
%
41 3
5.9%
13
11.
4%
(114
)
5336
.1%
50
33.1
%
4328
.5%
5
3.3%
(1
51)
4451
.2%
18
20.9
%
1922
.1%
5
5.8%
(8
6)
*Fig
ures
in
pare
nthe
ses
indi
cate
tot
al f
or g
roup
.

Eoslnoph~ls in Ulcerative Co[i~'is
eosinophilia in ulcerative colitis. Although, by analogy with the infiltration of the bronchial mucosa in asthma and the nasal mucosa in hay fever, the tissue eosinophilia in ulcerative colitis may be considered to be a reaction to an external allergen, there is little evidence to support this. The number of eosinophils in the stools has, however, been shown to be of diagnostic value in milk allergy in childhood, which indicates that the colon, like the nasal and bronchial mucosae, can produce an exudate rich in eosinophils in allergic reactions. 29 Riis and Anthonisen 3 considered that 80% of cases of ulcerative colitis had eosinophilia in the inflammatory exudate compared with 28% with circulating eosinophilia. In the present study, eosinophilia in the rectal biopsy specimens was noted in nearly half the observations made during a relapse of the disease, but it is doubtful whether methods of quanti tat ing cells, either in the tissues or in tile inflammatory exudate, are sufficiently accurate to allow more than a rough quantitative assessment to be made.
The relationship of circulating to tissue eosinophilia has been discussed by
TABLE 8. DISTRIBUTION OF PATIENTS ACCORDING TO INFILTRATION OF THE TISSUES WITH EOSINOPHILS IN THE INITIAL SPECIMEN IN RELATION TO THE
SUBSEQUENT RELAPSE RATE
Degree of tissue eosinophilia No. oI
relapses -- ± + q-+ Total
0 5 8 5 1 19 I 3 5 8 2 18 2 4 2 5 2 13 3 6 2 3 1 12
TABLE 9. DISTRIBUTION OF PATIENTS ACCORDING TO RELATIONSHIP OF TISSUE TO CIRCULATING EOSINOPHILS (COMBINING ALL DIETS)
Circulo ting eosinophil
count
Tissue eosinophilia
± + ++ Total
In remission <140 125 39 41 11 (5.1%) 216 140+ 12 8 15 8 (18,6%) 43
TOTAL 137 47 56 19 259
In relapse <140 19 22 29 2 (2.8%) 72 140+ 7 I2 12 I1 (26.2%) 42
Toxnt, 26 34 41 13 114
On corti- <140 96 61 60 7 (3.1%) 224 costeroids 140+ 1 4 2 3 (30%) 10
TOTAL 97 65 62 10 234
260 146 159 42 607 To'rAL <140 240 122 130 20
(92.3%) (83.6%) (81.8%) (47.6%) 140+ 20 24 29 22
(7.7%) (16.4%) (18.2%) (52.4%)
New Series, Vol. I I , No. I I, t966 8 4 3

Wright & Truelove
Archer 2~ on the basis of his experiments with horse eosinophils. He believes that eosinophils exert their primary function in tissues and not in the circu- lating blood, which merely transports them from the bone marrow to the "shock" organ. The relative numbers of eosinophils in the tissues, in the blood,
~100
80
O
._~ 60 0
c 40 a J
t . .
t5 2O
0 L
Count oIless than 140.
~ ' ~ Count of 140 o r m o r ~
Neg.
, . . . .
\ \ \ x
\ \ \ \
÷
Tissue eosinophits.
Fig. 5. Relationship of cir- culating to tissue eosinophils.
and in bone marrow will depend on circulating and tissue concentrations of histamine. He considers that both corticosteroid-induced eosinopenia and eosinopenia due to shock result from the action of corticosteroids in reducing the blood histamine level. As a result there is a reduction in the stimulus of the bone marrow to produce eosinophils, with a prompt fall in circulating eosinophils because of their continued withdrawal into the tissues which con- tain histamine. Another view is that there is a peripheral site of origin of tissue eosinophils independent of the bone marrow or circulating blood. 11, 30
Either of these possibilities would account for the rather poor correlation between circulating and tissue eosinophils found in the present study. They would also account for the persistence o£ large numbers of eosinophils in biopsy specimens despite local and systemic corticosteroid treatment. A similar obser- vation was made by Riis and Anthonisen 3 regarding eosinophils in the in- flammatory exudate.
The early histologic features of ulcerative colitis are characterized by in- filtration of cel ls--such as lymphocytes, plasma cells, eosinophils, and macro- phages--which may be concerned with antibody formation and hypersensitivity reactions. This is in keeping with the operation of such mechanisms in ulcera- tive colitis, but even if hypersensitivity reactions to antigens in the colonic wall do occur, they could be a consequence, rather than the cause, of the disease. They could, for example, result from the absorption of dietary or bacterial
844 American Journal of Digestive Diseases

Eosinophils in U[cem÷ive Colitis
antigens through mucosa damaged by some other means and need not neces- sarily play a part in the initiation or the perpetuation of the disease.
SUMMARY
During a controlled clinical trial of various diets in ulcerative colitis the levels of circulating eosinophils in the peripheral blood and infiltration of rectal biopsy specimens with eosinophils were studied.
In some patients there was a rise in the circulating eosinophil count dur ing a clinical relapse of the disease and the count was significantly higher when there was histologic evidence of inflammation than when the biopsy appear- ances were normal.
T h e eosinophil count would not be used to predict the clinical course of the disease or to detect those patients who were likely to respond to a milk- free diet.
T h e findings with tissue eosinophils were similar. Although some correla- tion was found between circulating and tissue eosinophils it was not close.
T h e significance of the findings in relation to the possibility that allergy may be of importance in the etiology of ulcerative colitis is discussed.
NuI~eld Department of Clinical Medicine University of Oxford
Oxford, England REFERENCES
1. RUSAG~R, P. M. Eosinophil leucocytes in ulcerative colitis. Lancet 2:1008, I959. 2. JVHL~N, L. Basophil and eosinophil leukocytes in various internal disorders. Acta Med
Scand 174:249, 1963. 3. Rils, P., and ANTI1ONISEN, P. Eosinophilia in peripheral blood and inflammatory exudate
in non-specific proctocolitis. ~tcta Med Scand 175:85, 1964. 4. TRUELOVE, S. C., and RICHARDS, W. C. D. Biopsy studies in ulcerative colitis. Brit Med J
1:1315, 1956. 5, LUMB, G., and PROTHEROE, R. H. B. Biopsy of the rectum in ulcerative colitis. Lancet
2:1208, 1955. 6. GOLDC, RABER, M. B., KmSNER, J. B., and PALM~R, W. L. The histopathology o.f chronic
ulcerative colitis and its pathogenic implications. Gastroenterology 38:596, 1960. 7. LUMp, G. Pathology of ulcerative colitis. Gastroenterology 40:290, 1961. 8. CAIN, A., CATLAN, R., and DREYVUS, B. Le cyto-diagnostic des recto-c61ites h6morragiques
et purulentes. Arch Mal Appar Dig 29:781, 1939. 9. BERCOVH'Z, Z. Discussion of Andresen? 5 Arner J Dig Dis 9:97, 1942.
10. BODDINCXON, M. M., and TRUEI~OVE, S. C. Abnormal epithelial cells in ulcerative colitis. Brit Med J 1:1318, 1956.
11. SAMTER, M. The response of eosinophils in the guinea pig to sensitization, anaphylaxis and various drugs, Blood 4:217, 1949.
12. SPHRS, R. S. Physiological approaches to an understanding of the function of eosinopbils and basophils. Ann NY Acad Sci 59:706, 1955.
13. PARISH. W. E., and PEPYS, J. "Allergic Reactions in the Lung." In Clinical Aspects of Imraunology. Gell, P. G. H. and Coombs, R. R. A., Eds. Blackwell, Oxford.
14. AND~ESEN, A. F. R. Gastro-intestinal manifestations of food allergy. Med J Rec (suppl) 122:271, 1925.
]5. ANDRESEN, A. F. R. Ulcerative colitis--an allergic phenomenon. Arner J Dig Dis 9:91, 1942.
I6. ROWE, A. H. Chronic ulcerative colitis--allergy in its etiology. Ann Intern Med 17:83, 1942.
New Series, Vol. I I, No. 11, 1966 8 4 5

Wrigh÷ & Truelove
17. SARLES, H., DECK, M., CHALVET, H., and AMBROSI, L. Hemorrhagic rectocolitis and nutr i t ional allergy. Arch Mal Appar Dig 48:907, 1959.
18. RIDER, j . A., MOELLER, H. C., DEVEREAUX, R. G., and WRIGHT, R. R. The use of an intra- mucosal test to demonstrate food hypersensitivity in ulcerative colitis. Acta Allerg (Kobenhavn) (Suppl) 7:486, 1960.
19. TRUELOVE, S. C. Ulcerative colitis provoked by milk. Brit Med J 1:154, 1961. 20. WRIGHT, R., and TRUELOVE, S. C. A controlled therapeutic trial of various diets in ulcera-
tive colitis. Brit Med ] 2:138, 1965. 21. WRIGHT, R., and TRUELOVE, S. C. Circulating antibodies to dietary proteins in ulcerative
colitis. Brit Med ] 2:142, 1965. 22. HILLS, A. G., FORSHAM, P. H., and FINCH, C. A. Changes in circulating leukocytes induced
by the administration of pituitary adrenocorticotrophic hormone (ACTH) in man. Blood 3:755, 1948.
23. ARCHER, R. K. The Eosinophil Leukocytes. Blackwell, Oxford. 24. VAUGHN, J. Function of the eosinophil leukocyte. Blood 8:1, 1953. 25. WELSH, R. A., and GRE.n% J. C. Phagocytosis of mast cell granules by the eosinophil
leukocyte in the rat. Amer ] Path 35:103, 1959. 26. SeEim, R. S. "Production of Antibody in the Reticulendothelial System Init iated by
Eosinophils." In Reticuloendothelial Structure and Function. Heller, J. H., Ed. Ronald Press, Co., New York.
27. SeEms, R. S., and SPEIRS, E. E. Cellular reactions to reinjection of antigen. J lmmun 92:540, 1964.
28. SARESIN, S. M. A function of the eosinophil: Phagocytosis of antlgen-antibody complexes. Proc Soc Exp Biol Med 112:667, 1963.
29. ROSENm,UM, A. H., and ROSENBLUM, P. Gastrointestinal allergy in infancy. Pediatrics 9:311, 1952.
30. DZURY, D. S., and COHEN, S. G. Experimental eosinophilia. Studies on the origin and relationship of tissue eosinophil cells to peripheral blood eosinophilia. ] Allerg 29:340, I958.
846 American Journal of Digestlve Diseases