Embed Size (px)
Citation preview

3 marzo 2017 1
Clinica Pediatrica
Polo Scienze della Salute della Donna e del Bambino
Fondazione Policlinico Universitario “A. Gemelli”
“CI Pensi mai a…”
Piero Valentini

Infezione della gravida
Infezione embrio-fetaleIVG No infezione transplacentare
Aborto spontaneo
Prematurità
Anomalie di sviluppo
Neonato a termine
Infezione postnatale persistente Eradicazione dell’infezione
MEU
Malattia congenitaRAI Neonato sano
Malattia inapparente Sequele dell’infezioneDanno tissutale progressivo

3 marzo 2017 3

3 marzo 2017 4
-=not present or rare; +=in infants with infection; ++=special diagnostic significance

Syndromes in the neonate caused bycongenital infections
3 marzo 2017 5
Microrganism Signs
Toxoplasma gondii Hydrocephalus, diffuse intracranial calcification, chorioretinitis
Rubella virus Cardiac defects, sensorineural hearing loss, cataracts
Cytomegalovirus Microcephalus, periventricular calcification
Herpes simplex virus Vesicular lesions, keratoconjunctivitis
Treponema pallidum Bullous, macular, and eczematous skin lesions involving the palms and soles; rhinorrhea; dactylitis and other signs ofosteochondritis and periostitis
Varicella-zoster virus Limb abnormalities, cicatricial lesions
Parvovirus Diffuse edema (in utero hydrops fetalis)
HIV Severe thrush, failure to thrive, recurrent bacterial infections, calcifications of the basal ganglia

Syndromes in the neonate caused bycongenital infections
3 marzo 2017 6
Microrganism Signs
Toxoplasma gondii Hydrocephalus, diffuse intracranial calcification, chorioretinitis
Rubella virus Cardiac defects, sensorineural hearing loss, cataracts
Cytomegalovirus Microcephalus, periventricular calcification
Herpes simplex virus Vesicular lesions, keratoconjunctivitis
Treponema pallidum Bullous, macular, and eczematous skin lesions involving the palms and soles; rhinorrhea; dactylitis and other signs ofosteochondritis and periostitis
Varicella-zoster virus Limb abnormalities, cicatricial lesions
Parvovirus Diffuse edema (in utero hydrops fetalis)
HIV Severe thrush, failure to thrive, recurrent bacterial infections, calcifications of the basal ganglia

3 marzo 2017 7
Parametri Valori
Sodio 118 mEq/l
Bilirubina Totale 3.73 mg/dl
Transaminasi GP (ALT) 257 UI/l
gamma-Glutamil-Transferasi 502 UI/l
Procalcitonina 8.00 ng/ml
Tempo di Protrombina%INR
31.90 secondi23.02.73
Fibrinogeno (derivato)D-Dimero
81 mg/dl6436 ng/ml
Parametri Valori
Hb 5 g/dl
Hct 12,5 %
GR 1.680.000/mmc
PLT 40.000/mmc
GB 23.690/mmc
by courtesy of M. Piastra, PICU, U.C.S.C., Rome

2Weeks
4Weeks
6Weeks
3Months
1:4
1:8
1:16
1:32
1:64
B
A
C
D
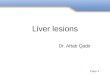
A: passive transfer of maternal antibodies, no disease
B: passive transfer of maternal antibodies, later onset of disease
C: passive transfer of maternal antibodies, indeterminate status for the infant
D: perinatal infection of mother and infant, later onset of disease
Patterns of serologic findings in infants with con CS or passive transfer of maternal antibodies
Feigin RD, Cherry JD, 1998
Delivery

3 marzo 2017 9
• Protuberanza bozze frontali 30-87 %
• Deformazioni del palato 76 %
• Distrofie dentali 55 %
• Cheratite interstiziale 20-50 %
• Anomalie radiologiche ossee 30-46 %
• Deformità nasali 10-30 %
• Sordità 3-4 %
• Neurosifilide 1-5 %
• Alterazioni articolari 1-3 %
Segni di sifilide congenita tardiva

3 marzo 2017 10
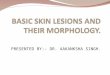
Denti di Hutchinson
Mulberry teethCheratite interstiziale
Fronte “olimpica”Distruzione palato duro

HCMV: INFEZIONE CONGENITADIAGNOSI CLINICA
( 15% SINTOMATICI )
REPERTI CLINICI POSITIVI / TOT ( % )
BASSO PESO ( < 10° cent EG ) 53 / 106 ( 50 )
PREMATURITA’ ( < 38 sett. EG ) 36 / 106 ( 34 )
PETECCHIE 80 / 106 ( 76 )
ITTERO 69 / 103 ( 67 )
EPATO - SPLENOMEGALIA 63 / 105 ( 60 )
SEGNI NEUROLOGICI ( 1 o PIU’ ) 72 / 106 ( 68 )
MICROCEFALIA 54 / 102 ( 53 )
IPOTONIA / LETARGIA 28 / 104 ( 27 )
CONVULSIONI 7 / 105 ( 7 )
( BOPPANA S. B. et al. , 1992 )

HCMV: INFEZIONE CONGENITADIAGNOSI DI LABORATORIO
PARAMETRI ALTERATI POSITIVI / TOT ( % )
TRANSAMINASI ( v. max in 2a sett. ) 46 / 58 ( 83 )
ALT > 80 U I / L
PIASTRINE ( v. min in 2a sett. ) 62 / 81 ( 77 )
< 100 X 103 / ml
BILIRUBINA DIR. ( v. max in 2a sett. ) 55 / 68 ( 81 )
H b e H t , RETICOLOCITI 37 / 72 ( 51 )
PROTEINORRACHIA ( in 1a sett. ) 24 / 52 ( 46 )
> 120 mg / dl
( BOPPANA S. B. et al. , 1992 )

HCMV: INFEZIONE CONGENITADIAGNOSI STRUMENTALE
INDAGINE ANOMALIA POSITIVI / TOT ( % )
Rx CRANIO Calcificazioni 6 / 42 ( 14 )
T A C CEREBRALE Calcificazioni 11 / 22 ( 55 )
Dilatazione ventricolare 5 / 20 ( 25 )
ES. OFTALMOLOGICO Corioretinite/atrofia ottica 4 / 39 ( 10 )
Emorragia retinica 5 / 39 ( 13 )
Altro 4 / 39 ( 10 )
ES. AUDIOMETRICO P.E.A. alterati 20 / 39 ( 56 )
(BOPPANA S. B. et al. , 1992 )



3 marzo 2017 16
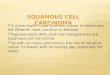
Ematopoiesiextramidollare

Tjon A Ten WE, Houwen RHJ. Arch Dis Child 2007;92:250

HCMV: INFEZIONE CONGENITARISCHIO DI SEQUELE A CARICO DEL S.N.C.
SEQUELE % SINTOMATICI ( n) % ASINTOMATICI (n)
Sordità neurosensoriale 58 ( 58 / 100 ) 7.4 ( 22 / 299)
Sordità bilaterale 37 ( 38 / 100 ) 2.7 ( 8 / 299 )
Corioretinite 20.4 ( 19 / 93 ) 2.5 ( 7 / 281 )
Q. I. < 70 55 ( 33 / 60 ) 3.7 ( 6 / 159 )
Microcefalia, Convulsioni,
Paresi / Paralisi 51.9 ( 54 / 104 ) 2.7 ( 9 / 330 )
( PASS R.F. 3° Intern CMV Workshop, Bologna Giugno 1991 )

3 marzo 2017 19

I trimestre II trimestre III trimestre TOTALE
N° (%) N° (%) N° (%) N° (%)
No infezione 109 (86) 173 (71) 52 (41) 334 (67)
Toxoplasmosi
congenita
17 (14) 73 (29) 76 (59) 166 (33)
• Subclinica 3 (2) 49 (20) 68 (53) 120 (24)
• Lieve 1 (1) 13 (5) 8 (6) 22 (4)
• Grave 7 (6) 6 (2) 0 (0) 13 (3)
•Aborto/morte
perinatale
6 (5) 5 (2) 0 (0) 11 (2)
TOTALE 126 (100) 246 (100) 128 (100) 500 (100)
Desmonts G, Couvrer J, 1979
Relazione fra epoca d’infezione da toxoplasma in gravidanza ed effetti sul prodotto del concepimento

3 marzo 2017 21
Age Normal FO ChorioretinitisEstimated incidenceof ocular lesions (%)
0-11 mo 8 3 27
1-4 yr 17 5 23
5-9 yr 6 4 40
>10 yr 2 2 50
Desmonts G. In: Böke W, Luntz M. (eds). Modern problems in ophtalmology. Ocular immune response.vol 16. Basel, S Karger,1976.

Roizen N. Pediatrics, 2006

Seropositivity of TORCH agents in the two groups
3 marzo 2017 23
Kumari N, et al. J HEALTH POPUL NUTR 2011 Feb;29(1):77-80

3 marzo 2017 24

3 marzo 2017 25

Pomeriggio(1)

3 marzo 2017 27Onesimo R, et al. BMJ Case Rep 2012

3 marzo 2017 28

3 marzo 2017 29

Pomeriggio(2)

3 marzo 2017 31
Una madre contrae la varicella dal figlio più grande;è da poco (2 settimane) rientrata a casa dopo averedato alla luce il secondo figlio: - Il neonato ha un rischio aumentato di complicanze da varicella ?-Deve essere sottoposto ad un trattamento particolare in virtù della sua età ?

32
Prevenzione passiva: le Ig VZIG (1)
Possono modificare o prevenire la varicella se somministrate <96h dall’esposizione
Sono indicate soltanto in
- bambini immunocompromessi
- neonati da madri con varicella 5 gg prima - 2 gg dopo il parto
- prematuri (<28 sett EG o 1000 gr PN) con esposizione post-natale
indipendentemente dalla presenza o meno di immunità materna
- prematuri ( 28 sett EG) con madre non protetta
- donne in gravidanza e adulti suscettibili
MMWR Rep 2013;62(28):574-6
4 marzo 2017

33
Prevenzione passiva: le Ig VZIG (2)
Le VZIG vanno somministrate i.m. o e.v. alla dose di
- 62,5 unità in bambini con peso 2 kg- 125 unità in bambini con peso 2,1 – 10 kg
In mancanza di VZIG, possono essere somministrate IGIV alla dose di 400 mg/kg
MMWR Rep 2013;62(28):574-6
4 marzo 2017

34
E’ indicata la chemioprofilassi con antivirali?
Se non sono disponibili VZIG o IGIV, è possibile utilizzare
Acyclovir, 20 mg/kg/dose, 4 volte/die, max. 3200 mg
oppure
Valacyclovir, 20 mg/kg/dose, 3 volte/die, max. 3000 mg
iniziando 7-10 giorni dopo l’esposizione e continuando per 7 giorni nei soggetti immunocompromessi senza evidenza di immunità
4 marzo 2017
AAP, Red Book, 2015

3 marzo 2017 35

3 marzo 2017 36

3 marzo 2017 37