Embed Size (px)
Citation preview

UHOD Say› / Number: 3 Cilt / Volume: 18 Y›l / Year: 2008 175
Chronic Renal Failure Secondary to
Paroxismal Nocturnal Hemoglobinuria
Umut VAROL1, Bahriye PAYZIN2, Mehmet SONBAHAR1, Mustafa YAPRAK1
1 İzmir Atatürk Eğitim ve Araştırma Hastanesi, 2. İç hastalıkları Kliniği2 İzmir Atatürk Eğitim ve Araştırma Hastanesi, Hematoloji Kliniği, İZMİR
ABSTRACT
Paroxysmal nocturnal hemoglobinuria (PNH) is a rare and acquired stem cell disease which is characterized with chro-nic intravasculer hemolysis and diffuse venous thrombosis. In PNH, renal failure is rare and acute renal failure, whichis caused by hemolytic attacks that are usually trigerred by infection and surgical intervention, may happen. A 48-ye-ars old male patient who had chronic renal failure (CRF) and has been hemodialysing for about 11 years was admit-ted to our hospital with the symptoms of pancytopenia. Although Ham’s test and sugar water test of our patient werenegative, with the results of bone marrow aspiration-biopsy, abdominal MRI and flow cytometry tests, we found outthat pancytopenia was due to PNH with type II cells dominancy and CRF was due to hemosiderosis.
Key Words: Chronic renal failure, Paroxysmal nocturnal hemoglobinuria, Hemosiderosis
ÖZET
Paroksismal Nokturnal Hemoglobinüriye Sekonder Gelişen Kronik Böbrek Yetmezliği
Paroksismal nokturnal hemoglobinüri (PNH) kronik intravasküler hemoliz ve yaygın venöz trombozlarla karekterizeyaygın, kazanılmış bir kök hücre hastalığıdır. PNH’de böbrek yetmezliği nadirdir ve genellikle enfeksiyonun ve cerra-hi müdahalelerin tetiklediği hemolitik ataklar sonucunda gelişen akut böbrek yetmezliği görülmüştür. Kronik böbrekyetmezliği (KBY) olan ve yaklaşık 11 yıldır hemodiyalize giren 48 yaşındaki erkek hasta pansitopeni semptomlarıylahastanemize başvurdu. Hastanın yapılan şeker su ve Ham’s testleri negatif gelmesine rağmen, yapılan kemik iliği as-pirasyon-biyopsisi, batın MR ve akım sitometri testleri neticesinde pansitopeninin, tip II hücrelerin çoğunlukta olduğuPNH’e ve KBY’nin ise hemosiderosise bağlı olduğu saptandı.
Anahtar Kelimeler: Kronik böbrek yetmezliği, Paroksismal nokturnal hemoglobinüri, Hemosiderozis
ULUSLARARASı HEMATOLOJI-ONKOLOJI DERGISI CASE REPORT /OLGU SUNUMU
International Journal of Hematology and Oncology

INTRODUCTIONPNH is a rare acquired clonal disease of hematopo-ietic stem cells caused by an unusual susceptibilityof erythrocytes to the lytic action of complementdue to their membrane abnormalities and it is cha-racterized by chronic intravascular hemolysis andthrombotic tendency. The absense of complementregulatory proteins CD55 and CD59 in the red cellmembrane results in complement-mediated he-molysis and hemoglobinuria. Hemolysis is continu-ous but episodes of exacerbation of red blood celllysis occur. Venous thromboses are frequent andusually involve mesenteric, portal, hepatic and ce-rebral veins. There is definite relationship with ap-lastic anemia and also with myelo-proliferative di-sorders (1).
In PNH, renal failure is rare and acute renal insuf-ficiency has been recognized previously in associ-ation with an acute hemolytic crisis (2). However,kidney involvement is usually benign and secon-dary to chronic deposition of hemosiderin in theproximal convulated tubule, that cause a mild tubu-lar dysfunction manifest as a concentrating defect(3). In addition to this renal siderosis leading appa-rently to several tubular atrophy and interstitial fib-rosis, recurrent microvascular thrombosis as a re-sult of microinfarctions or direct nephrotoxicity ofiron or repeated episodes of pyelonephritis may al-so has a role in progression to chronic renal insuffi-ciency. We reported a case of CRF patient whoseetiology was later determined as PNH.
CASE REPORTA 48-years old male patient, who had chronic renalfailure (CRF) and has been hemodialysing for abo-ut 11 years, was admitted to our clinic with thecomplaints of weakness and tiredness which waspersisting for about two months. He had transfusi-
ons with frequent intervals and had no history ofhypertension, diabetes mellitus and any other chro-nic diseases. In addition, there was also no historyof drug usage. Physical examination of the patientwas normal except pallor, pretibial edema and mildsplenomegaly. His blood cell count showed pancy-topenia with results Hgb: 7.16 g/dL, MCV: 92.5 fl,corrected retikulocyte: 3.4%, Plt: 550 x109/L andNeu: 0.645 x109/L. Increased biochemical parame-ters are indirect bilirubin: 1.1 mg/dl (N:0-0.8),BUN: 69 mg/dL (N:7-25), creatinin: 11.75 mg/dL(N:0.6-1.2) and ferritin: 964 ng/ml (N:22-232). Ot-her parameters are serum iron: 116 µg/dL (N:25-160), total iron binding capacity: 246 µg/dL(N:250-425), and transferin saturation: 47%. Thepatient’s LDH, Vitamin B12, folic acid, prothrombintime and INR values were all in normal ranges.HBsAg, Anti-HCV and Anti-HIV were negative.Only once and very limited amount of urine samp-le could be taken owing to the patient’s anüric situ-ation and many bladder epithels were detected inurine sediment without any hemosiderin. With thesuspect of PNH, Ham’s test and sugar water testwere done. Both Ham’s test and sugar water testwere negative. Blood marrow aspiration-biopsy re-vealed accelerated erythropoiesis with hypercellü-ler, megaloblastoid and displastic characters andincreased in number of hemosiderin granüles andsideroblasts.
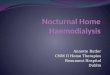
Flow cytometry analysis of peripheral blood de-mostrated that erythrocytes with partial CD 55 andCD 59 expression were dominated (Table 1). Thepercentage of CD 55 and CD 59 negative granu-locytes was 1.2% and 11.5% (Figure 1). This flowcytometry test was done four weeks after transfusi-on and as a result of this test, patient was diagnosedas PNH. Echocardiographic study of the patientwas normal. In the patient’s abdominal doppler ult-rasonography (USG), hepatosplenomegaly was de-
176 UHOD Say› / Number: 3 Cilt / Volume: 18 Y›l / Year: 2008
Table 1. Flow cytometric analysis of erythrocytes of the peripheral blood
Type I cell (normal Type II cell (partial Type III cell expression) defficiency) (total deficiency)
CD 55 expression 0.7% 86.9% 11.6%
CD 59 expression 1.1% 97.1% 1.6%

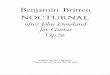
tected without any ascittes. In addition, portal andsplenic veins were found as open. As a result of the-se findings, he was considered as cirrhosis in thecompensated phase. The patient had a past medicalhistory of liver biopsy in another center for abouttwo years ago. However pathological result of thisbiopsy could not be achieved and one more biopsywas not accepted by the patient. After all, becauseof the high ferritin value, hepatosplenomegaly andincreased hemosiderin staining in blood marrow, inorder to investigate hemosiderin deposition in therenal cortex, abdominal magnetic resonance ima-ging (MRI) was applied due to its high imaging qu-
ality for searching hemosiderin deposition (Figure2). Abdominal MRI showed low signal intensity ofspleen, liver and bilateral renal paranchymas in T2weighted images which was attributed to hemosi-derosis (4).
DISCUSSIONPNH is a chronic condition with a median survivalof 10-25 years after diagnosis. It is associated withvenous thrombosis in at least one third of PNH pa-tients, hemorrhage from thrombocytopenia and in-fection due to neutropenia (5). Azotemia has occa-
UHOD Say› / Number: 3 Cilt / Volume: 18 Y›l / Year: 2008 177
Figure 1. Schematic apperance of erythrocytes’ flow cytometry investigation
Figure 2. T1 and T2 weighted images showing hemosiderosis in liver, spleen and kidneys

sionally been seen in patients with PNH. Acute re-nal failure may occur during severe hemoglobinu-ric crisis which may be precipitated by blood trans-fusions, infections, surgical procedures, contrastmedia, reaction to drugs, sleep and even exercise(6). By the effect of these stimulants, there is excesscomplement production resulting hemoglobinuriathat acts as a tubular toxin and causes acute renaldysfunction. Microvascular thrombosis, thought tobe due to abnormal platelet function, is also com-mon in PNH and felt to contribute acute renaldysfunction during hemolytic crisis. The reducedrenal function was short lived with return to normalin few weeks after the termination of crisis. Howe-ver, in some severe hemolytic attacks, patients co-uld require transient dialytic support for recoveringtheir renal functions.There are few case reports in literature search, con-cerning the association between PNH and chronicrenal failure. It is obvious that renal hemosiderosishas been observed in chronic intravascular hemoly-sis. Renal siderosis leads apparently to severe tubu-lar atrophy and interstitial fibrosis which causes re-nal insufficiency. However, some authors believethat PNH can cause renal failure mostly as a resultof microinfarctions due to repeated episodes ofmicrovascular thrombosis rather than to this hemo-siderin deposition (7). Others stated that chronic re-nal failure was a consequence of repeated episodesof pyelonephritis. It is also suggested that ironmight play an important role in the nephrotoxicityassociated with hemoglobinuria. So, the authors be-lieved a direct nephrotoxic effect of iron (3).In our case, we described a patient who had chronicrenal failure with an unknown etiology. He was ad-mitted with symptoms of pancytopenia. At firstsight, it was thought that pancytopenia was becauseof chronic hemodialysis complication. However, bythe help of flow cytometry investigation, PNH wasdiagnosed even if the Ham’s test was negative (8).Flow cytometric analysis, in which antibodies aredirected against complement regulatory proteinsCD55 and CD59, is the most informative and sen-sitive assay available for diagnosis of PNH. Thisanalysis identify a population of CD55 and CD59deficient cells. In addition, it can both evaluate thepercentage of abnormal cells and identify discretepopulations with different degrees of deficiencyparticularly on erythrocytes. Erythrocytes with nor-
mal expression are called PNH I, those with subto-tal deficiency having usually 10% of normal exp-ression are called PNH II, those with complete de-ficiency are called PNH III. As transfusion will inc-rease the proportion of cells with normal expressi-on of CD55 and CD59, flow cytometric assay willbe affected by recent red blood cell transfusion,Therefore, to detect accurate information, analysisshould be performed at least 1 month before thetransfusion or during a transfusion absent period. Inorder to obtain additional information, analysis ofexpression of CD55 and CD59 on granulocytesmay be useful. The life span of PNH granulocytesis normal in contrast to CD55 and CD59 deficientred blood cells. Therefore, the proportion of abnor-mal granulocytes is unaffected by red blood celltransfusion and more accurately detects the PNHclone size. Patients with subclinical symptoms ha-ve little or no clinical evidence of hemolysis. Beca-use of having small PNH clones, most of these pa-tients have refractory anemia or aplastic anemia.For this reason, both at diagnosis and yearly aftertreatment, even in the absence of biochemical orclinical evidence of hemolysis, high sensitive flowcytometric analysis is recommended for these pati-ents (9). Ham’s test does not detect small populati-ons of abnormal cells which results in a decrease insensitivity. The degree of lysis does not accuratelyreflect the proportion of abnormal cells and thedegree of abnormality of the abnormal cells cannotbe assessed. The sucrose lysis test is technically ea-sier to perform but has a higher rate of false-positi-ve results thus decreasing its specificity. Althoughit more accurately detects the proportion of PNH-type III red blood cells than the Ham’s test, it like-wise does not delineate the abnormality of thesecells and does not quantitatively delineate the num-ber of PNH-type II cells. Further, flow cytometrydistinguishes much better the cells of intermediateabnormality of PNH cells (10). After all, because the patient had chronic compen-sated hemolysis and had a history of multiple bloodtransfusions owing to his low hemoglobin value,hemosiderosis was suspected for the etiology of hisrenal insufficiency. So, we had two main opportu-nities in order to demostrate hemosiderosis. One isrenal biopsy which seems unnecessary because ofbeing end stage renal failure and the other methodis MRI which shows the renal cortical hemosidero-sis.
178 UHOD Say› / Number: 3 Cilt / Volume: 18 Y›l / Year: 2008

Abdominal MRI was done to study the iron deposi-tion and revealed low signal intensity not only inrenal paranchymas but also in liver and spleen, onT2 weighted images. On MRI, normal kidneysshow low or medium signal intensity on T1 weigh-ted images and the renal cortex being slightly hype-rintense with respect to the medulla causing a rela-tively good differentiation. In normal kidneys, onT2 weighted images, the cortex and medulla have avery similar and moderately high signal intensitycausing no distinction between them (3). When he-mosiderin deposition occurs in the renal cortex, itbecomes darker than renal medulla reversing theirdifferentiation on T1 weighted images. Hemoside-rin contains ferric iron and deposits of hemosiderinexplain low signal intensity of the renal cortex de-picted in T2 weighted images which is also a cha-racteristic finding in our patient’s MRI. Whentransfusional siderosis is absent, low signal inten-sity confined to the kidney suggests PNH, whereaslow signal intensity limited to the spleen and liveris characteristic of transfusional hemosiderosis andhemochromatosis (7). However, iron deposits weredemostrated not only in kidneys but also in liverand spleen depending on receiving multiple bloodtransfusions and resulting decreased signal inten-sity on MRI (3,11). In summary, this a case of chronic renal failure whohas been hemodialysing for years with an unknownPNH etiology. Chronic renal failure in PNH is a di-agnosis of exclusion so that careful diagnostic wor-kup is mandatory (12). In fact, very little is knownabout the mechanism leading to renal failure inPNH. The role of hemosiderosis in chronic renal fa-ilure may be more significant and postmortem stu-dies of patients with PNH suggested that hemoside-rosis contributes to nephrosclerosis, even amongthe relatively asymptomatic patients (4). Here, wenoninvasively showed hemosiderosis which is ca-used by both chronic compensated hemolysis dueto clinically mild PNH and multiple blood transfu-sions, by MRI findings.
REFERENCES1. P. Zachee, M. Henckens, B. Van Damme, et al.
Chronic renal failure due to renal hemosiderosisin a patient with paroxymal nocturnal hemoglo-binuria. Clin Nephrol 39: 28-31, 1993.
2. Kondo H, Uga S, Kaihara A, et al. Acute renalfailure in a case of paroxysmal nocturnal hemog-lobinuria: a review of literature in Japan. NipponJinzo Gakkai Shi 32: 835-40, 1990.
3. Rimola J, Martin J, Puig J, et al. The kidney inparoxysmal nocturnal haemoglobinuria: MRIfindings. Br J Radiol 77: 953-6, 2004.
4. Chow KM, Lai FM, Wang AY, et al. Reversiblerenal failure in paroxysmal nocturnal hemog-lobinuria. Am J Kidney Dis 37: E17, 2001.
5. Jose MD, Jose K. L. Acute renal failure in apatient with paroxysmal nocturnal hemog-lobinuria. Clin Nephrol 56: 172-4, 2001.
6. A. Moorakı, B. Boroumand, F. MohammadZadeh, et al. Acute reversible renal failure withparoxysmal nocturnal hemoglobinuria. ClinNephrol 50: 255-7, 1998.
7. Jeong JY, Kim SH, Lee HJ, Sim JS. AtypicalLow-Signal-Intensity Renal Parenchyma: Caus-es and Patterns. RadioGraphics 22: 833-846,2002.
8. Nishimura J, Kanakura Y, Ware RE, et al. Clini-cal course and flow cytometric analysis ofparoxysmal nocturnal hemoglobinuria in theUnited States and Japan. Medicine (Baltimore)83:193-207, 2004.
9. Parker C, Omine M, Richards S, et al. Diagnosisand management of paroxysmal nocturnalhemoglobinuria. Blood 106: 3699-3709, 2005.
10. Bv Sharon E. Hall and Wendell F. Rosse. TheUse of Monoclonal Antibodies and FlowCytometry in the Diagnosis of Paroxysmal Noc-turnal Hemoglobinuria. Blood 87: 5332-5340,1996.
11. Jeong JY, Kim SH, Lee HJ, Sim JS. Atypicallow-signal-intensity renal parenchyma: causesand patterns. Radiographics 22: 833-46, 2002.
12. Kumpers P, Herrmann A, Lotz J, et al. A bluekidney-chronic renal failure as a consequence ofsiderosis in paroxysmal nocturnal hemog-lobinuria. Clin Nephrol 66: 210-3, 2006.
CorrespondenceDr. Umut VAROLİzmir Atatürk Eğitim ve Araştırma HastanesiYeşilyurt İZMİR
e-mail: [email protected]: (0.232) 232 54 00
UHOD Say› / Number: 3 Cilt / Volume: 18 Y›l / Year: 2008 179