Embed Size (px)
Citation preview

Chlamydia and Gonorrhea Lab Update
Burning Questions
Laboratory Guidelines
CT Immunobiology Consultation
The findings and conclusions in this presentation are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention

Alternate Specimen Verification
Rectal and oropharyngeal swabs FDA clearance being pursued Establish an external specimen bank
Home collected vaginal swabs Interest but studies have not commenced (that I’m aware of)

Performance
Discreet packaging Must meet federal regulations for shipping diagnostic specimens Wet vs dry swabs
Greater temperature ranges than covered in the product insert
NOT FDA CLEARED What are the parameters for an off-label verification study? Need sound guidance
Considerations
Self-Obtained Vaginal Swabs in a Home Setting

Sensitivity of Different Specimens by Three Different Assays
Assay FCU Cx S-vag C-vag
TMA 72% 89% 93% 90%
PCR 84% 91% 91% 93%
LCR 98% 96% 98% 100%
Combined 81% 91% 93% 93%
FCU – first catch urine, Cx – endocervix, S-vag – self-collected vaginal swab, C-vag - Clinician collected vaginal swab. Schachter J, et al. JCM 41;2003:3784

Preliminary Vaginal Swab Mailing Kit

One Example of a Vaginal Swab Mailing Kit
(Gen-Probe® Vaginal Swab Transport Tube, Vaginal Swab, Inner Medical Specimen Transport Tube, Vaginal Swab Collection Instructions, Follow-up Questionnaire, and Mailing Can)
Mailing Can
Follow-up Questionnaire
Swab

Swab Specimen Transport Conditions for Commercially Available CT/GC NAATs
Test Swab Condition Transport Temperature
Time to Test
BD ProbeTec Dry (no liquid media) 2 to 27oC 4 to 6 days
GenProbe APTIMA(vaginal swabs FDA cleared)
Penetrable top tube containing specimen buffer
2 to 30oC Up to 60 days
Roche Amplicor Tubes containing Chlamydia culture medium (eg. M4, 2ST, Bartels, etc)
18 to 25oC Within 1 hour
2 to 8oC Up to 7 days
Less than -20oC Up to 30 days

Package Temperature during USPS Transit from St. Louis to New Orleans
Package placed in St. Louis USPS drop box July 22, 2005 and received at 2:30pm July 26, 2005 in New Orleans. Temperatures were recorded at 10 minute intervals.

Package Temperature during USPS Transit from Jackson to New Orleans
Package placed in Jackson USPS drop box July 29, 2005 and received at 2:00pm August 10, 2005 in New Orleans. Temperatures were recorded at 10 minute intervals.

20
25
30
35
40
45
50
6:01
6:53
7:45
8:37
9:29
10:2
1
11:1
3
12:0
5
12:5
7
13:4
9
14:4
1
15:3
3
16:2
5
17:1
7
18:0
9
19:0
1
19:5
3
20:4
5
21:3
7
22:2
9
23:2
1
Cel
siu
s
Time
Residential Mailbox and Outside Air Temperature
Mailbox
Outside Air
Temperature recorded at 1 minute intervals August 21, 2005.

APTIMA Test Result for Chlamydia trachomatis (Relative Light Units)
Initial Temperature / Duration
Final Temperature / Duration
Inoculum (Inclusion forming units)
24oC / 24 hours 37oC / 24 hours
10 1104 1102
103 1226 1115
105 1195 1087
In Vitro Assessment of Specimen Stability

APTIMA Test Result for Chlamydia trachomatis (Relative Light Units)
Initial Temperature / Duration
Final Temperature / Duration
Inoculum (Inclusion forming units)
37oC / 24 hours 56oC / 24 hours
10 1172 1124
103 1133 1114
105 1142 1115
In Vitro Assessment of Specimen Stability

APTIMA Test Result for Chlamydia trachomatis (Relative Light Units)
Initial Temperature / Duration
Final Temperature / Duration
Inoculum (Inclusion forming units)
56oC / 24 hours 24oC / 24 hours
10 1059 1023
103 1211 1951
105 1147 1113
In Vitro Assessment of Specimen Stability
Alternate Specimen Verification
Rectal and oropharyngeal swabs FDA clearance being pursued Establish an external specimen bank
Home collected vaginal swabs Interest but studies have not commenced (that I’m aware of)
APHL / CDC STD Steering Committee Workgroups to develop Verification Protocols Involve CMS (CLIA) Part of revised CDC Laboratory guidelines

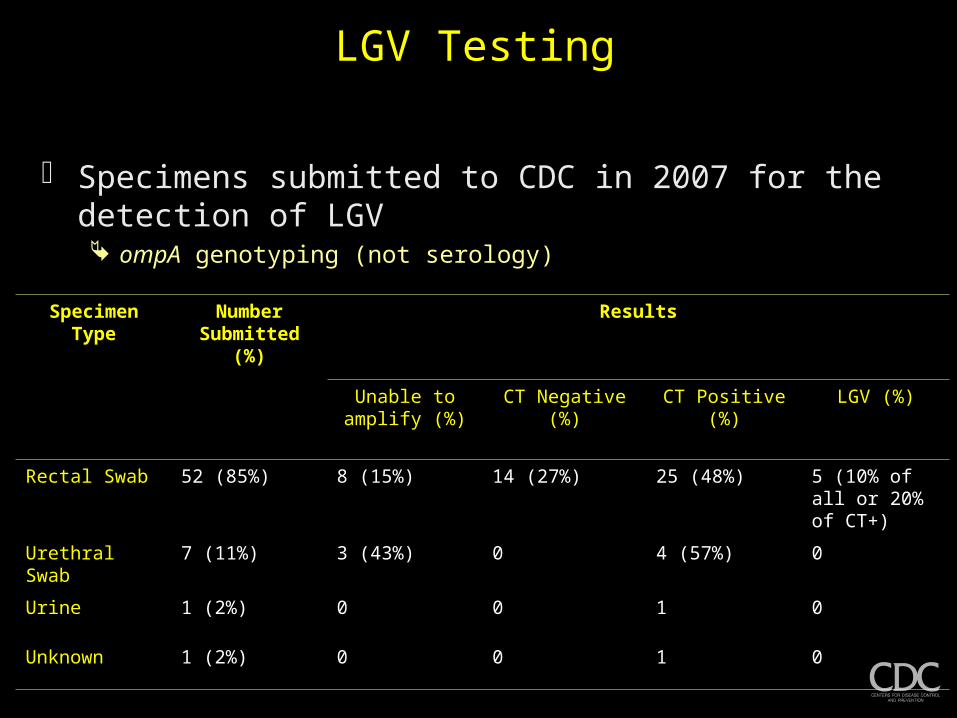
LGV Testing
Specimens submitted to CDC in 2007 for the detection of LGV ompA genotyping (not serology)
Specimen Type Number Submitted (%)
Results
Unable to amplify (%)
CT Negative (%) CT Positive (%) LGV (%)
Rectal Swab 52 (85%) 8 (15%) 14 (27%) 25 (48%) 5 (10% of all or 20% of CT+)
Urethral Swab 7 (11%) 3 (43%) 0 4 (57%) 0
Urine 1 (2%) 0 0 1 0
Unknown 1 (2%) 0 0 1 0

Importance of differentiating LGV from non-LGV rectal CT infections Course of recommended Tx varies
No commercial differential test available
Seems that settings that have been testing for rectal CT infections and managing those infections as non-LGV have not seen increases in proctocolitis
• Refer to Dr. Mark Pandori’s presentation at the 2008 STD Prevention meeting
Sx and Asx infections reported
CDC does not have a survelliance program LGV• Submission of specimens for reference testing should be based on local descions
Serology for rectal LGV testing No data
LGV Testing

Laboratory Guidelines

Background 1982
Laboratory Diagnosis of Chlamydia trachomatis Infections Isolation and serology
1993 Recommendations for the Prevention and Management of
Chlamydia trachomatis Infections• Isolation• Non-culture tests
Immunoassays, nucleic acid hybridization tests• Screening• Sexual assault• Presumptive Laboratory Diagnosis

Screening Tests to Detect Chlamydia trachomatis and Neisseria gonorrhoeae
Infections - 2002
Guideline Development CDC identified questions reviewed published literature from 1990 - 2000 prepared tables of evidence drafted recommendations
External consultants asked to review the drafted recommendations• selected on the basis of expertise and/or disciplinary or organizational
affiliations
CDC considered all suggestions from external consultants and finalized recommendations

Revising Laboratory Guidelines for the Detection of Chlamydia trachomatis and Neisseria gonorrhoeae
Infections
Similar format of previous guidelines / consultations Convene an expert review panel Identify / refine key questions Review literature
External consultants asked to review the drafted recommendations• selected on the basis of expertise and/or disciplinary or organizational affiliations
CDC considered all suggestions from external consultants and finalized recommendations

Issues
What is the sensitivity and specificity of available tests for CT and GC Is it correct to lump NAATs
Does the sensitivity and specificity of available for CT and GC vary with respect to the anatomic site from which the specimen was collected and/or the specimen type
What class of tests should be recommended for the detection of CT and GC infection; stratify by anatomic site and/or specimen type
What test or combination of tests should be recommended confirmation of CT and GC infection

Issues
Can routine supplemental testing improve the PPV of certain CT and GC tests and at what prevalence level should it be recommended

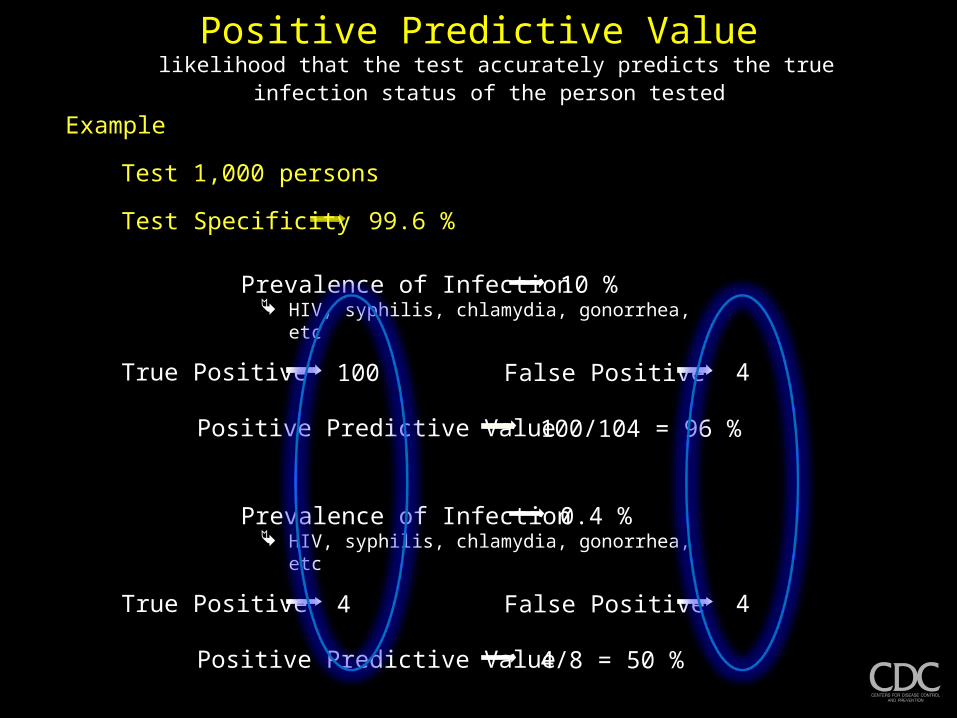
Positive Predictive Valuelikelihood that the test accurately predicts the true infection status
of the person tested Example
Test 1,000 persons
Test Specificity 99.6 %
True Positive 100 False Positive 4
Prevalence of Infection HIV, syphilis, chlamydia, gonorrhea, etc
10 %
Positive Predictive Value 100/104 = 96 %
True Positive 4 False Positive 4
Prevalence of Infection HIV, syphilis, chlamydia, gonorrhea, etc
0.4 %
Positive Predictive Value 4/8 = 50 %
Example
Test 1,000 persons
Test Specificity 99.6 %
True Positive 100 False Positive 4
Prevalence of Infection HIV, syphilis, chlamydia, gonorrhea, etc
10 %
Positive Predictive Value 100/104 = 96 %
True Positive 4 False Positive 4
Prevalence of Infection HIV, syphilis, chlamydia, gonorrhea, etc
0.4 %
Positive Predictive Value 4/8 = 50 %
Positive Predictive Valuelikelihood that the test accurately predicts the true infection status
of the person tested

Issues
Can routine supplemental testing improve the PPV of certain CT and GC tests and at what prevalence level should it be recommended
Does pooling urine specimens diminish NAAT performance
Should recommendations be made on testing in situations involving medicolegal issues including adult and pediatric CT and GC infections (note: making a recommendation of any test beyond culture would require a preliminary discussion recommendations for off-label testing)

Issues
What test(s) should be recommended for the laboratory diagnosis of LGV and would these vary based on the presentation (i.e. inguinal versus anorectal presentation)
What serologic cut-off values should be used if serology is recommended to aid LGV diagnosis
What (if any) recommendations be made concerning in vitro antibiotic susceptibility testing for GC including but not limited to the actual methodology for the procedure

Chlamydia Immunology and Control Expert Advisory MeetingAtlanta, April 23-25, 2008
Highlight the key questions related to chlamydia natural history, pathogenesis, and immunobiology that have the most important implications for control of chlamydia and its sequelae
Assess extent to which existing data address these key questions, especially with respect to their potential relevance to prevention programs
Identify important remaining gaps in knowledge that would have implications for prevention
Chlamydia trachomatis
Pathology is primarily a function of the host-response Little intrinsic toxicity
Protective immunity has been demonstrated in animal models or animals naturally infected with related chlamydiae Mice, guinea pigs, sheep etc Th1 type DTH in mice
Susceptibility to reinfection is common High rates of reinfection Early Tx of mice resulted in a
disruption of immunity Th2 type DTH in mice
Development of pathology poorly understood How long? Predisposing factors? Reinfection or persistent infection?
Development of immunity that protects against subsequent CT infections has not been conclusively documented in humans Commercial sex workers seem to
be refractory to infection after time
Human data is lacking (absent) on the mechanisms associated with reinfection Bacterial? Host?
Some of what we know Some of what we don’t know
Chlamydia trachomatis
Screening and Tx reduce the natural duration of infection
Despite screening, reinfection rates seem to be increasing
Brunham et al JID 2005
Antibiotic resistance has not been demonstrated among human CT isolates It has been shown in pig isolates
How long does CT persist if left untreated? Brazilian data suggests most half of
the infections are cleared after a year and all are cleared by 5 years
What are the reasons for increases in reinfection rates?
Better Dx tests
Increased / more targeted screening Bacterial changes
Why are some CT infections more difficult to treat? Golden et al NEJM 2005
Some of what we know Some of what we don’t know

Some of What we Learned
Good evidence that repeated episodes of acute diagnosed PID increase the risk of tubal infertility
CT related damage is primarily a function of the host response
Understanding of pathogenesis or timing of occurrence of damage is more limited than most realized additional work needed if new approaches to prevention are to be
developed Existing animal model data offer somewhat less insight than
expected but alternative approaches possible
Data addressing the mechanisms, development, or role of immunity in humans are quite limited But approaches for addressing these gaps provided






























