Embed Size (px)
Citation preview

Developmental Neurorehabilitation, February 2010; 13(1): 37–45
Children with autism spectrum disorders: A comparison of thosewho regress vs. those who do not
JOHNNY L. MATSON, JONATHAN WILKINS, & JILL C. FODSTAD
Louisiana State University, Psychology, Baton Rouge, USA
(Received 4 June 2009; accepted 9 June 2009)
AbstractObjective: While autism spectrum disorders (ASD) constitute a group of similar conditions, considerable heterogeneityin symptoms of these neurodevelopmental disorders have been noted. One of the most important, yet least studied, of thesefactors is developmental regression.Methods: One-hundred and twenty-five children were studied and broken down into the following three groups: ASDchildren with and without substantial regression and typically developing children. In study one, the three groups werecompared on global measures of ASD symptomatology, comorbid psychopathology, challenging behaviour and social skills.In study two, the two ASD groups were compared on each individual item from the dependent measures.Results: Mean age when regression occurred was 27.76 months. The ASD children as a whole differed from the typicallydeveloping controls, showing more symptoms of ASD, as would be expected, and poorer social skills, while differences werealso noted between the two ASD groups.Conclusions: It was determined that children with ASD who regress present with a distinct behavioural profile whencompared to children with ASD who do not regress, which included greater levels of impairment on global measures of ASDsymptomatology, comorbid psychopathology, challenging behaviour and social skills.
Keywords: autism spectrum disorders, regression, diagnosis, aetiology, children
ResumenObjetivo: Aunque el espectro de trastornos autistas (ASD) constituye un grupo de condiciones similares, se ha observadouna heterogeneidad considerable en los sıntomas de estas alteraciones en el neurodesarrollo. Uno de los factores masimportantes pero menos estudiado es la regresion en el desarrollo.Metodos: Ciento cincuenta ninos fueron estudiados y divididos en 3 grupos: Ninos con ASD, ninos sin ASD sin regresionimportante, y ninos con desarrollo normal. En el estudio uno, los tres grupos fueron comparados por medio de medicionesglobales segun los sıntomas ASD, co-morbilidad psicopatologica, conducta difıcil, y capacidad de interaccion social.En el estudio dos, los dos grupos ASD fueron comparados en cada ıtem individual a partir de las mediciones dependientes.Resultados: La edad promedio cuando tuvo lugar la regresion fue a los 27.76 meses. Los ninos ASD se diferenciaron de losninos control con desarrollo normal mostrando mas sıntomas ASD como era de esperarse, ası como una capacidad deinteraccion social mas pobre, aunque tambiOn se notaron diferencias entre los dos grupos ASD.Conclusion: Se determino que los ninos con ASD que tienen una regresion, presentan un comportamiento caracterısticodistinto cuando se les compara con ninos ASD que no presentan una regresion, incluyendo un mayor nivel de deterioroen las mediciones globales de sintomatologıa de ASD, de comorbilidad psicopatologica, de conducta difıcil, y de capacidadde interaccion social.
Palabras clave: Trastornos del espectro autista, regresion, diagnostico, etiologıa, ninos
Introduction
Autism spectrum disorders (ASD) are made up offive conditions which share many similar features[1–3]. These conditions are also known as PervasiveDevelopmental Disorders and include AutisticDisorder, Asperger Disorder, Rett Disorder,Childhood Disintegrative Disorder (CDD), and
Pervasive Developmental Disorder-Not OtherwiseSpecified (PDD-NOS) [4]. The ASDs result inmarked deficiencies in social and communicationskills [5–7]. Furthermore, they are frequentlyaccompanied by co-occurring problems such asstereotypies [8], intellectual disability (ID) [9–11],psychopathology [12, 13], and other maladaptive
Correspondence: Dr Johnny L. Matson, PhD Professor and Distinguished Research Master, Department of Psychology, Louisiana State University, BatonRouge, LA. 70803, USA. E-mail: [email protected]
ISSN 1751–8423 print/ISSN 1751–8431 online/10/010037–9 � 2010 Informa UK Ltd.DOI: 10.3109/17518420903107984
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.

behaviours such as self-injury, aggression, sleepdisturbances, atypical eating and temper tantrums[14–18].
Early diagnosis has become a major area ofinterest for researchers in ASD [19, 20]. A majorimpetus for this approach is the general acknowl-edgement that behaviour therapy and appliedbehaviour analysis are effective in treating ASD[21] and the assertion that interventions begunbefore age 3 years produce a better long-termoutcome [22]. For a sub-set of children with ASD,those parents who are not receiving intensive inter-vention report significant regression, particularlyin social and communication skills at �2–3 years ofage [23–25]. Furthermore, Werner et al. [26] assertthat regression does not impede gains for beha-vioural interventions at 3–4 years of age compared tochildren who did not regress. However, this is onlyone study; a restricted number of outcome measureswere used, which may not have detected differences.In a methodologically similar study by Richler et al.[27], the authors noted that ‘social symptoms’ werein fact resistant to intervention. Finally, Sipersteinand Volkmar [28] have conducted perhaps themost extensive study of regression in skills amongchildren with ASD. Their general conclusions werethat many children failed to gain skills, vs. actuallylosing previously acquired skills. Secondly, theauthors point out that the issue is a very complexone; skill loss is not a monolith; and may vary acrosslanguage, social skills, motor skills, and abnormalbehaviours (among others, one might add). Thus,while these papers are a nice start in the explorationof determining which symptoms differentiate chil-dren with ASD who regress as opposed to thosewho do not, much is yet to be learned.
The purpose of the present study was to replicateand extend the existing literature on this topic. First,this study was designed to assess regression andregression only. Secondly, it employed differentASD and social skills measures, which was aneffort to complement, and at the same time, assessa slightly different set of behaviours than in theprevious research. Thirdly, it aimed to look atspecific ages of regression and related demographicvariables which have not been previously examined.Finally, this study looked at the impact of concom-itant comorbid psychopathology on regressive beha-viour in young children with ASD, which had notpreviously been addressed.
Method
Participants
The sample consisted of 125 children who rangedin age from 3–16 years (M¼8.05). A lower limit
of 3 years of age was chosen because it has beenpreviously reported that the mean age of regressionis between 18–24 months of age [29]. This step wastaken to ensure that the child was of sufficient agefor regression to have occurred. There were 78 malesand 47 females. Approximately 84% of the samplewas Caucasian. Data was obtained from 14 USstates: Louisiana, New York, Georgia, Michigan,Texas, Washington, New Jersey, Connecticut, NorthCarolina, Maryland, Wisconsin, Arizona, Nebraska,and Mississippi. Informed consent was obtainedfrom all parents who participated in the study andthe study received IRB approval.
Children were placed into one of three groups:ASD without regression, ASD with regression andtypical development. A child was designated as ASDif he/she met criteria for ASD based on a checklistof combined symptoms from the Diagnostic and
Statistical Manual of Mental Disorders (4th edn, textrevision; DSM-IV-TR) [4] and International
Classification of Diseases (10th edn; ICD-10) [30].See below for further description of this checklist.Endorsements on this checklist were used as inclu-sion criteria because the participants were recruitedfrom several different sites, where scaling andinterview methods for diagnosing ASD varied.In fact, a variety of previous diagnoses wereidentified including autism, PDD-NOS, Asperger’ssyndrome, Fragile X syndrome, mental retardation,Down’s syndrome, Attention Deficit-HyperactivityDisorder (ADHD), Obsessive-Compulsive Disorder(OCD), nocturnal enuresis, depression, seizures,Oppositional Defiant Disorder and unspecifieddevelopmental delay. Next, those children who metcriteria for ASD were split into two groups based onparental response to an item on a demographicquestionnaire (see below). This item, ‘Was there aperiod of time during development when your childlost skills?’ was endorsed as either ‘yes’ or ‘no’. Basedon this information, there were 46 ASD childrenwithout evidence of regression (M¼8.26 years ofage, SD¼3.86) and 35 ASD children with evidenceof regression (M¼ 8.17, SD¼3.50). There were44 typically developing controls who did not haveany reported Axis I diagnoses or delays in develop-ment (M¼ 7.73, SD¼ 2.98). Demographic infor-mation for these three groups is presented in Table I.
A series of one-way analyses of variance(ANOVAs) were performed to determine if therewere any meaningful differences between thesegroups in terms of demographic variables. Therewere no significant differences among the groupsin terms of age or race. There were significantlymore males and more participants who wereprescribed some form of psychotropic medication(i.e. antidepressant, anti-psychotic, anti-epileptic/mood stabilizer, anxiolytic or psychostimulant)
38 J. L. Matson et al.
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.

at the time of assessment in both autism groupscompared to the controls. Only one difference wasnoted between the two autism groups—there weresignificantly more children who were non-verbalin the regression group compared to the two othergroups.
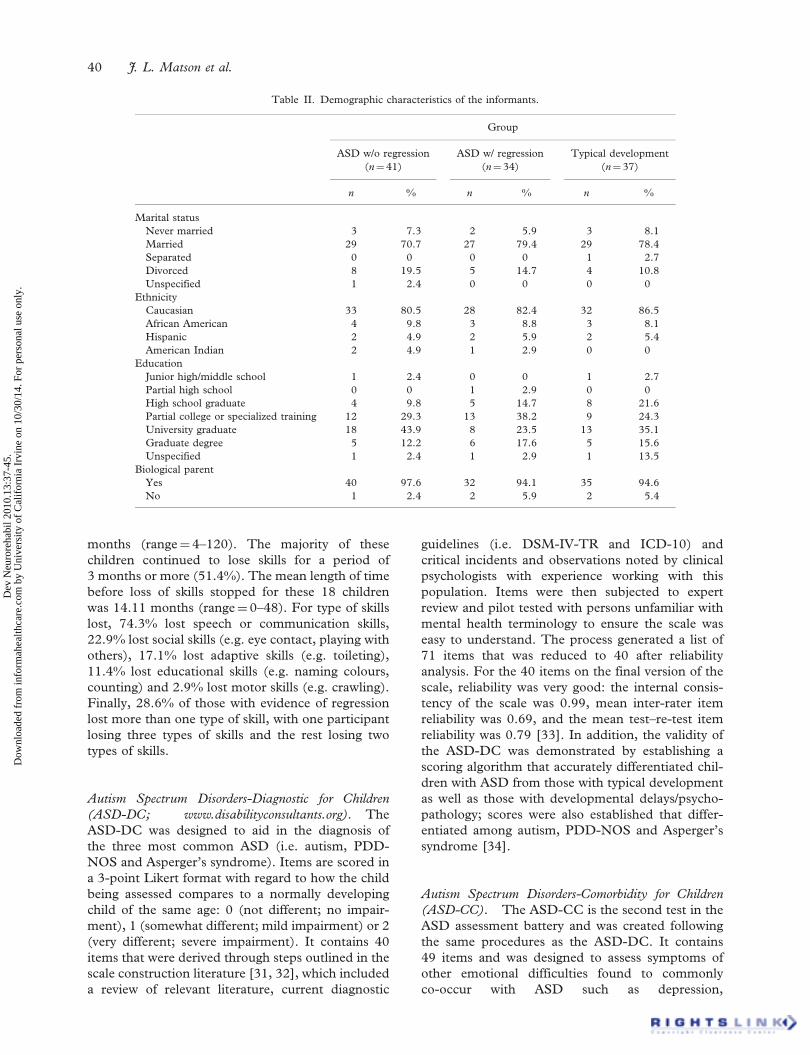
There were 109 raters who were all indentifiedas the primary caregiver of the child being assessed(e.g. parent, grandmother). Table II presents demo-graphic information of the raters. There were threecases where the same informant provided informationfor children in different groups (i.e. one child withASD who regressed and one with ASD who did not)and that person’s demographic data was included forboth groups. Mean age of the raters for each groupwas as follows: ASD no regression (M¼ 35.84,range¼ 24–56), ASD with regression (M¼ 38.26,range¼ 29–56), controls (M¼ 35.44, range¼ 25–66). Again a series of ANOVAs were performed toexamine differences among the groups on thesevariables. There were no significant differences onany of these variables among the three groups.
Measures
DSM-IV-TR/ICD-10 checklist. This checklist wascomprised of items from DSM-IV-TR and ICD-10used in the diagnosis of ASD (i.e. autism, PDD-NOS and Asperger’s syndrome). Redundant itemswere removed, leaving a total of 19 items on thechecklist, which were broken down into the three
core areas of impairment used when diagnosingASD (i.e. social interaction, communication andrestricted/repetitive behaviours or interests).Informants were instructed to rate each of thesesymptoms as either ‘yes’ or ‘no’ with regard towhether or not the item applied to the child. Forthe purposes of this study, a child was includedin one of the ASD groups if a total of at least threesymptoms were endorsed (at least two in the socialimpairment domain and one in either communicationor restricted/repetitive behaviour). Such a symptompattern corresponds to a DSM-IV-TR diagnosisof PDD-NOS, which is the least stringent criteriafor a diagnosis of ASD [4].
Demographic questionnaire. In addition to the demo-graphic variables presented in Table II, the infor-mant was required to list occupation and theoccupation of his/her spouse. The final portionof the questionnaire included a series of questionsrelated to the child’s development. Areas coveredincluded any unusual development, if any previouslyacquired skills were lost and if so what skills, age atwhich skill loss occurred, and how long before skillswere regained if skills were regained. As mentionedabove, a child was included in the regression groupif the informant endorsed the question regardingloss of skills as ‘yes’.
For those in the ASD group with regression, themean age at which regression occurred was 27.76
Table I. Demographic characteristics of the sample.
Group
ASD w/o regression ASD w/ regression Typical development(n¼ 46) (n¼ 35) (n¼ 44)
n % n % n %
Age3–5 (preschool) 13 28.3 9 25.7 13 29.56–11 (child) 22 47.8 18 51.4 28 63.612–16 (adolescent) 11 23.9 8 22.9 3 6.8
GenderMale 35 76.1 26 74.3 17 38.6Female 11 23.9 9 25.7 27 61.4
EthnicityAfrican American 3 6.5 2 5.7 3 6.8Caucasian 36 78.3 31 88.6 38 86.4Hispanic 3 6.5 1 2.9 3 6.8Other 4 8.7 1 2.9 0 0
Verbal abilityYes 44 95.7 26 74.3 44 100No 2 4.3 9 25.7 0 0
Psychotropic medicationYes 22 47.8 16 45.7 2 4.5No 24 52.2 19 54.3 42 95.5
Autism spectrum disorders 39
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.
months (range¼ 4–120). The majority of thesechildren continued to lose skills for a period of3 months or more (51.4%). The mean length of timebefore loss of skills stopped for these 18 childrenwas 14.11 months (range¼ 0–48). For type of skillslost, 74.3% lost speech or communication skills,22.9% lost social skills (e.g. eye contact, playing withothers), 17.1% lost adaptive skills (e.g. toileting),11.4% lost educational skills (e.g. naming colours,counting) and 2.9% lost motor skills (e.g. crawling).Finally, 28.6% of those with evidence of regressionlost more than one type of skill, with one participantlosing three types of skills and the rest losing twotypes of skills.
Autism Spectrum Disorders-Diagnostic for Children
(ASD-DC; www.disabilityconsultants.org). TheASD-DC was designed to aid in the diagnosis ofthe three most common ASD (i.e. autism, PDD-NOS and Asperger’s syndrome). Items are scored ina 3-point Likert format with regard to how the childbeing assessed compares to a normally developingchild of the same age: 0 (not different; no impair-ment), 1 (somewhat different; mild impairment) or 2(very different; severe impairment). It contains 40items that were derived through steps outlined in thescale construction literature [31, 32], which includeda review of relevant literature, current diagnostic
guidelines (i.e. DSM-IV-TR and ICD-10) andcritical incidents and observations noted by clinicalpsychologists with experience working with thispopulation. Items were then subjected to expertreview and pilot tested with persons unfamiliar withmental health terminology to ensure the scale waseasy to understand. The process generated a list of71 items that was reduced to 40 after reliabilityanalysis. For the 40 items on the final version of thescale, reliability was very good: the internal consis-tency of the scale was 0.99, mean inter-rater itemreliability was 0.69, and the mean test–re-test itemreliability was 0.79 [33]. In addition, the validity ofthe ASD-DC was demonstrated by establishing ascoring algorithm that accurately differentiated chil-dren with ASD from those with typical developmentas well as those with developmental delays/psycho-pathology; scores were also established that differ-entiated among autism, PDD-NOS and Asperger’ssyndrome [34].
Autism Spectrum Disorders-Comorbidity for Children
(ASD-CC). The ASD-CC is the second test in theASD assessment battery and was created followingthe same procedures as the ASD-DC. It contains49 items and was designed to assess symptoms ofother emotional difficulties found to commonlyco-occur with ASD such as depression,
Table II. Demographic characteristics of the informants.
Group
ASD w/o regression ASD w/ regression Typical development(n¼ 41) (n¼ 34) (n¼ 37)
n % n % n %
Marital statusNever married 3 7.3 2 5.9 3 8.1Married 29 70.7 27 79.4 29 78.4Separated 0 0 0 0 1 2.7Divorced 8 19.5 5 14.7 4 10.8Unspecified 1 2.4 0 0 0 0
EthnicityCaucasian 33 80.5 28 82.4 32 86.5African American 4 9.8 3 8.8 3 8.1Hispanic 2 4.9 2 5.9 2 5.4American Indian 2 4.9 1 2.9 0 0
EducationJunior high/middle school 1 2.4 0 0 1 2.7Partial high school 0 0 1 2.9 0 0High school graduate 4 9.8 5 14.7 8 21.6Partial college or specialized training 12 29.3 13 38.2 9 24.3University graduate 18 43.9 8 23.5 13 35.1Graduate degree 5 12.2 6 17.6 5 15.6Unspecified 1 2.4 1 2.9 1 13.5
Biological parentYes 40 97.6 32 94.1 35 94.6No 1 2.4 2 5.9 2 5.4
40 J. L. Matson et al.
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.

oppositional/conduct problems, ADHD, TicDisorder, OCD, Specific Phobia and eating difficul-ties. To the authors’ knowledge the ASD-CC is theonly scale available for this specific purpose. Therater is instructed to rate each item to the extent thatthere has been a recent problem as either 0 (not aproblem or impairment; not at all), 1 (mild problemor impairment), 2 (severe problem or impairment),or X (does not apply or don’t know). The scale hasbeen demonstrated to have sound psychometricproperties: internal consistency was 0.91, meaninter-rater reliability was 0.46 and mean test–re-test reliability was 0.51 [35].
Autism Spectrum Disorders-Problem Behaviour for
Children (ASD-PBC). The third and final compo-nent of the ASD battery, the ASD-PBC, consistsof 18 items pertaining to aggressive, disruptive, self-injurious and stereotypic behaviours commonlyreported as challenging behaviours in children withASD. Again, the ASD-PBC was created using thetest construction procedures described above. Ratersare instructed to rate each item to the extent thatit has been a recent problem as either: 0 (not aproblem or impairment; not at all), 1 (mild problemor impairment) or 2 (severe problem or impair-ment). The ASD-PBC was intended to be used asan initial screen to determine if further assessmentof problem behaviour with more extensive ratingscales or clinical observations (including evaluationof frequency, intensity, duration and behaviouralfunction) is warranted. Mean inter-rater reliabilitywas 0.49, mean test–re-test reliability was 0.64 andthe internal consistency of the scale was 0.90 [36].Additionally, the results of a factor analysis identifiedtwo factors that were labelled externalizing andinternalizing [36].
Matson Evaluation of Social Skills with Youngsters
(MESSY). The MESSY is an extensivelyresearched inventory of children’s social behaviourthat contains 64 items [37]. These items are ratedin terms of frequency according to a Likert scaleranging from 1 (not at all) to 5 (very much). Thepsychometric properties of the MESSY are well-established with reliability and validity demonstratedacross a variety of clinical populations includingchildren with ASD [38, 39]. The MESSY containstwo main factors: Inappropriate Assertiveness/Impulsiveness (e.g. ‘threatens people or acts like abully’) and Appropriate Social Skills (e.g. ‘helps afriend who is hurt’). A score on one of these factorsis considered ‘problematic’ if it falls 1 SD belowthe normative mean and ‘very problematic’ if it falls2 SD below the mean.
Procedures
Informants completed all of the measures indepen-dently either at home or online according to thedirections of each scale or questionnaire. Researchassistants (i.e. doctoral students in clinical psychol-ogy) made follow-up phone calls or emails to resolveany questions or issues regarding the assessmentmeasures. The Louisiana State UniversityInstitutional Review Board and consent wasobtained from parents/guardians of each child.
Study 1
Results
In study 1, the three groups were compared onglobal measures of ASD symptomatology (ASD-DCtotal score), comorbid psychopathology (ASD-CCtotal score), challenging behaviour (ASD-PBC totalscore) and social skills (Inappropriate Assertivenessand Appropriate Social Skills sub-scales from theMESSY). A 3� 5, one-way multivariate analysis ofvariance (MANOVA) was conducted with diagnos-tic group (ASD without regression, ASD withregression or typical development) as the indepen-dent variable. MANOVA was used as the primarystatistical procedure to protect against inflation ofalpha associated with conducting multiple ANOVAs[40]. The dependent variables were the five globalmeasures mentioned above. Follow-up ANOVAswere conducted for the five dependent measures andpost-hoc tests were conducted to compare groups onthe variables with significant ANOVAs. Missing datawas imputed with the mean response for that item.No participant had more than three missing itemsfor each particular measure. One participant fromeach ASD group was removed because the MESSYhad not been completed.
Significant differences were found between thethree groups on the dependent measures, Wilks’s�¼ 0.21, F(10, 232)¼ 27.26, p50.001. The multi-variate �2 based on Wilks’s �, which is an indicatorof effect size, was strong at 0.54. Table III displaysthe means and standard deviations of the dependentvariables for each group.
Five ANOVAs were conducted (one for eachdependent variable) as follow-up tests to the signif-icant MANOVA. The ANOVAs for ASD-DC totalscore (F[2, 120]¼ 174.44, p50.001, �2
¼ 0.74),ASD-CC total score (F[2, 120]¼69.42, p50.001,�2¼0.54), ASD-PBC total score (F [2, 120]¼ 41.68,
p50.001, �2¼ 0.41), and the Appropriate Social
Skills sub-scale of the MESSY (F [2, 120]¼ 75.43,p50.001, �2
¼ 0.56) were significant. However,the ANOVA for the Inappropriate Assertiveness
Autism spectrum disorders 41
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.

sub-scale of the MESSY (F[2, 120]¼ 1.93, p¼ 0.15,�2¼ 0.01) was not significant.Post-hoc pairwise comparisons (Tukey HSD)
were conducted for the four dependent measureswith significant ANOVAs. Compared to typicallydeveloping controls, both ASD groups scoredsignificantly higher on the ASD-DC, ASD-CC andASD-PBC ( p50.001) and significantly lower on theAppropriate Social Skills sub-scale of the MESSY( p50.001). Additionally, the ASD with regressiongroup scored significantly higher on the ASD-DC( p50.001), ASD-CC ( p¼ 0.042) and ASD-PBC( p¼ 0.001) and significantly lower on theAppropriate Social Skills sub-scale of the MESSY( p¼ 0.005) compared to the ASD group who didnot regress. See Table III for mean scores on thesevariables.
Discussion
Not surprisingly, both ASD groups evinced signifi-cantly greater impairment in terms of autisticsymptomatology, comorbid psychopathology, chal-lenging behaviours and social skills deficits. A similarpattern was found for those ASD children withreported evidence of regression compared to thoseASD children who did not regress. These social skillsdeficits were apparent for a lack of appropriate socialbehaviour as opposed to higher levels of inappropri-ate assertiveness or impulsiveness.
Study 2
Given the apparent differences in the two ASDgroups relative to each other and to typicallydeveloping children, a more fine-grained analysis ofspecific symptoms was taken. These data werederived from the same test battery. Thus themethods were identical to study 1.
Results
In study 2, the two ASD groups were compared oneach individual item from the dependent measures.
Initially, bivariate correlations were calculatedbetween presence or absence of regression anditem scores on the ASD-DC, ASD-CC, ASD-PBCand MESSY. The significance level for thesecorrelations was adjusted to p50.01 (two-tailed) toprotect against family-wise error rate inflation [40].Because of the lack of a linear relationship betweenthe dependent/predictor variables and the presenceor absence of regression, Spearman’s rho was thecorrelation coefficient used. Therefore, items withSpearman’s rho correlation coefficients that weresignificant at the p50.01 level were retained forlogistic regression analysis. There were 12 itemsfrom the ASD-DC, two items from the ASD-CC,three items from the ASD-PBC and two items fromthe MESSY that met this criterion. Items andcorrelation coefficients retained for logistic regres-sion are displayed in Table IV.
Next, analyses were performed using SPSSLogistic Regression. Direct logistic regressions wereperformed with presence of evidence for regressionas the outcome variable and endorsement of signif-icant items from the four measures in a unifiedmodel with the items analysed together as predictorsof evidence for regression. No outliers were identi-fied based on a p50.001 criterion for Mahalanobisdistance.
There was a good model fit for all 19 itemsretained from the ASD-DC, ASD-CC, ASD-PBCand MESSY aggregate as predictors (�2 [19,n¼79]¼36.89, p¼ 0.008). This indicates that themodel successfully discriminated between the twogroups. Further, the Hosmer and Lemeshow testwas non-significant at p¼ 0.19, indicating that themodel’s estimate fit the data at an acceptable level.Nagelkerke’s approximation for R2 for the modelwas 0.50. Thus, the aggregate of the ASD-DC,ASD-CC, ASD-PBC and MESSY items accountedfor 50% of the variance of being identified as havingASD with regression vs. ASD without regression.Using these 19 items as predictors, correct classifi-cation rates were 70.6% for the ASD with regres-sion group (sensitivity) and 82.2% for the ASDwithout regression group (specificity). Overall, this
Table III. Means and standard deviations on the dependent variables for the three groups.
ASD w/ regression ASD w/o regression Typical developmentMeasure M (SD) M (SD) M (SD)
ASD-DC 56.44 (12.20)a,b 44.37 (19.26)a 2.79 (4.84)b
ASD-CC 35.73 (15.09)a,c 28.85 (14.44)a 4.97 (6.28)b
ASD-PBC 11.06 (14.04)a,b 6.69 (5.60)a 0.71 (1.92)b
MESSY Social Skills 41.47 (13.19)a,c 50.68 (14.81)a 74.93 (9.40)b
MESSY Assertiveness 84.90 (26.77) 90.62 (28.94) 79.85 (21.40)
aSignificantly different from Typical Development ( p� 0.001); bSignificantly different from ASD w/oRegression ( p� 0.001); cSignificantly different from ASD w/o Regression ( p50.05).
42 J. L. Matson et al.
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.

diagnostic algorithm produced a correct classifica-tion rate of 77.2%.
Discussion
In study 2, a 19-item algorithm for predicting aregression in skills for children with ASD was created.Nine of these items pertained to general deficits incommunication or speech or the presence of repet-itive or disruptive vocalizations, seven pertained tosocial interaction skills (e.g. ability to make and keepfriends, make-believe or pretend play) and theremaining items pertained to the presence of unusualor disruptive behaviours. When used as predictorsfor regression or loss of skills in this sample of ASDchildren, the aggregate of these items producedadequate-to-good levels of diagnostic accuracy(sensitivity¼ 70.6%, specificity¼ 82.2%).
Conclusion
The purpose of this study was to gain a betterunderstanding of the phenomenon of developmentalregression or loss of previously acquired skills inchildren with ASD. To accomplish this aim, thispaper used measures of ASD symptomatology andsocial skills that have not been used in other studies.In addition, it included measures of comorbidpsychopathology and challenging behaviour thatwere developed specifically for children with ASD.Of the 81 ASD children in this sample, �43% hadshown evidence of regression according to parentreport. This number falls within the range of10–50% reported in the literature [29, 41, 42].More specifically, approximately three-quarters(74.3%) of those children who regressed lostpreviously developed speech or communicationskills, which is comparable to a study by Goldberget al. [41] who found that 62% of the childrenin their sample lost words. In addition, 28.6% ofchildren in this sample lost skills in more than onebroad domain of functioning (i.e. communication,social behaviour, adaptive behaviour, educationalskills and motor skills). The mean age at whichregression occurred was �28 months, which isconsistent with findings from previous researchdemonstrating that the loss of skills occurs betweenthe ages of 2–3 years [23, 25, 41].
Researchers have debated whether or not ASDchildren who regress represent a distinct behaviouralphenotype [24, 27]. Findings regarding this issue aremixed. For example, Rogers [24] notes that ASDchildren who regress seem to have greater impair-ment in overall development compared to ASDchildren who do not regress, but there is notsufficient evidence to conclude that the two groupsare different behavioural phenotypes. Richler et al.[27], on the other hand, found that those ASDchildren who regressed developed atypically prior toregression, had greater impairment in verbal IQ andsocial reciprocity, had a later age of onset of ASDsymptoms and had more gastrointestinal problemsthan those ASD children who did not regress or loseskills. The present study found that those childrenwho regressed evinced significantly greater levels ofASD symptoms, symptoms of comorbid psychiatricconditions and challenging behaviours compared toASD children who did not regress. The regressiongroup also showed significantly greater deficits inappropriate social behaviour. In addition, this studyexamined individual items from the ASD batteryand MESSY to determine if they were predictive ofregression. This analysis produced a 19-item diag-nostic algorithm, the majority of which pertained todeficits in communication and social interaction.This algorithm produced adequate-to-good levels
Table IV. Correlation coefficients of items predicting evidenceof regression.
Item Spearman’s Rho
ASD-DC
Communication skills 0.37Verbal communication 0.34Social interactions with others his/her age 0.32Shares enjoyment, interests or achieve-
ments with others (e.g. parents,friends, caregivers)
0.31
Ability to make and keep friends 0.41Interest in participating in social games,
sports and activities0.34
Communicates effectively (e.g. usingwords, gestures or sign language)
0.37
Restricted interests and activities 0.29Make-believe or pretend play 0.29Language development 0.29Socializes with other children 0.33Development of social relationships 0.30
ASD-CC
Engages in behaviours that impair dailyroutine or activities
0.42
Sudden, rapid, repetitive movement orvocalization that occurs for no appar-ent reason
0.36
ASD-PBC
Removal of clothing at inappropriatetimes
0.32
Unusual play with objects (e.g. twirlingstring, staring at a toy, etc.)
0.40
Repeated and unusual vocalizations (e.g.yelling, humming, etc.)
0.40
MESSY
Walks up to people and starts aconversation
�0.32
Calls people by their names �0.39
Note: All correlations significant at the p50.01 level, two-tailed.
Autism spectrum disorders 43
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.

of diagnostic accuracy. Taken together, these resultsprovide support for a distinctive regressive pheno-type characterized by global and specific deficitsacross a wide range of symptoms.
However, there are several limitations that need tobe addressed. Data was obtained via retrospectiveparental report and this could have produced inac-curate information, especially for older children witha much longer time period between the time regres-sion occurred and the interview (the sample includedchildren as old as 16 years). This study was notable to assess the reliability of parental reports (twoparents rating their same child). Other studies haveaddressed this issue by examining home videos forevidence of regression [41]. An additional limitationwas that this study only used one yes-or-no questionto assess for regression. However, all informantsdid complete additional questions about the natureof the skill loss that indicated that the question wasanswered accurately in all cases. Another issue thatwas not taken into account is that of birth order.A few raters provided information for more than onechild and may have been more accurate in recogniz-ing symptoms for those children who were notfirstborn [43]. Other variables that were examinedin other studies but that were not examined hereinclude onset of regression (i.e. was it gradual orabrupt) [41], age of onset of ASD symptoms [27]and type of ASD (e.g. PDD-NOS, Asperger’s,CDD) [28]. However, the rarity and questionablevalidity of the diagnosis [44] make CDD difficultto assess. Future research should address theseissues as applied to the assessment measures usedin the present study as well as compare regressionacross the three most common ASD (i.e. autism,PDD-NOS and Asperger’s).
In conclusion, it was found that children withASD who regress present with a distinct behaviouralprofile when compared to children with ASD whodo not regress. The ASD children who showedevidence of regression were significantly moreimpaired on global measures of ASD symptomatol-ogy, comorbid psychopathology, challenging beha-viour and social skills. Furthermore, the majorityof skills that were reported to have been lostwere related to speech and social interaction withothers. Future research is needed to determine thecourse of such deficits and whether or not thetwo groups remain distinct into adolescence andadulthood.
Declaration of interest: The authors report noconflicts of interest. The authors alone are respon-sible for the content and writing of the paper.
References
1. Matson JL. Current status of differential diagnosis forchildren with autism spectrum disorders. Research inDevelopmental Disabilities 2007;28:109–118.
2. Matson JL, Boisjoli JA. Differential diagnosis of PDD-NOSin children. Research in Autism Spectrum Disorders2007;1:75–84.
3. Prior M, Eisenmajer R, Leekam S, Wing L, Gould J, Ong B,Dowe D. Are there subtypes within the autism spectrum?A cluster analysis of a group of children with autism spectrumdisorders. Journal of Child Psychology and Psychiatry1998;39:893–903.
4. American Psychiatric Association. Diagnostic and statis-tical manual of mental disorders. 4th ed., textrevision. Washington, DC: APA; 2000.
5. Chung KM, Reavis S, Moscow M, Drewry J, Matthews T,Tasse MJ. Peer-mediated social skills training program foryoung children with high-functioning autism. Research inDevelopmental Disabilities 2007;28:423–436.
6. Hilton C, Graver K, LaVesser P. Relationship between socialcompetence and sensory processing in children with highfunctioning autism spectrum disorders. Research in AutismSpectrum Disorders 2007;1:164–173.
7. LeBlanc LA, Greiger KB, Sautler RA, Sidener TM. Usingthe Natural Language Paradigm (NLP) to increase vocaliza-tions of older adults with cognitive impairments. Research inDevelopmental Disabilities 2007;28:437–444.
8. MacDonald R, Green G, Mansfield F, Geckeler A,Gardenier N, Anderson J, Holcomb W, Sanchez J.Stereotypy in young children with autism and typicallydeveloping children. Research in Developmental Disabilities2007;28:266–277.
9. Ben-Itzchak E, Zachor DA. The effects of intellectualfunctioning and autism severity on outcome of early behav-ioral intervention for children with autism. Research inDevelopmental Disabilities 2007;28:287–303.
10. Prior MR, McMillan MB. Maintenance of sameness inchildren with Kanner’s syndrome. Journal of Autism andChildhood Schizophrenia 1973;3:154–167.
11. Tsai LY. Diagnostic issues in high-functioning autism.In: Schopler E, Mesibov BG, editors. High functioningindividuals with autism. New York: Plenum Press; 1992.pp 11–40.
12. LaMalfa G, Lassi S, Salvini R, Giganti C, Bertelli M,Albertini G. The relationship between autism and psychiatricdisorders in intellectually disabled adults. Research in AutismSpectrum Disorders 2007;1:218–228.
13. Matson JL, Nebel-Schwalm MS. Comorbid psychopathologywith autism spectrum disorders in children: An overview.Research in Developmental Disabilities 2007;28:341–352.
14. Ando H, Yoshimura I. Prevalence of maladaptive behaviorin a retarded child as a function of IQ and age. Journal ofAbnormal Child Psychology 1978;6:345–349.
15. Collacott RA, Cooper SA, Branford D, McGrother C.Epidemiology of self-injurious behavior in adults with learn-ing disabilities. British Journal of Psychiatry 1998;173:428–432.
16. Dominick KC, Davis NO, Lainhart J, Tager-Flusberg H,Folstein S. Atypical behaviors in children with autism andchildren with a history of language impairment. Researchin Developmental Disabilities 2007;28:145–162.
17. Field D, Garland M, Williams K. Correlates of specificchildhood feeding problems. Journal of Pediatrics and ChildHealth 2003;29:299–304.
18. Matson JL, Mishawi NF. Functional assessment of challen-ging behaviors: Toward a strategy for applied settings.Research in Developmental Disabilities 2006;28:353–361.
44 J. L. Matson et al.
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.

19. Matson JL, Wilkins J, Gonzalez ML. Early identification anddiagnosis of autism spectrum disorders in young children andinfants: How early is too early. Research in Autism SpectrumDisorders 2008;2:75–84.
20. Wetherby AM, Woods J, Allen L, Cleary J, Dickinson H,Lord C. Early indicators of autism spectrum disorders in thesecond year of life. Journal of Autism and DevelopmentalDisorders 2004;34:473–493.
21. Matson JL, Benavidez DA, Compton LS, Paclawskyj TR,Baglio CS. Behavioral treatment of autistic persons: A reviewof research from 1980 to the present. Research inDevelopmental Disabilities 1996;17:433–466.
22. McGee G, Morrier M, Daly T. An incidental teachingapproach to early intervention for toddlers with autism.Journal of the Association for Persons with Severe Handicaps1999;24:133–146.
23. Brown J, Prelock PA. Brief report: The impact of regressionon language development in autism. Journal of Autism andDevelopmental Disorders 1995;25:305–309.
24. Rogers SJ. Developmental regression in autism spectrumdisorders. Mental Retardation and DevelopmentalDisabilities 2004;34:731–734.
25. Volkmar FR, Cohen DJ. Disintegrative disorder of ‘lateonset’ autism. Journal of Child Psychology and Psychiatry1989;30:717–724.
26. Werner E, Dawson G, Munson J, Osterling J. Variation inearly developmental course in autism and its relation withbehavioral outcome at 3–4 years of age. Journal of Autismand Developmental Disorders 2005;35:337–350.
27. Richler JL, Luyster R, Risi S, Hsu WL, Dawson G,Bernier R, Dunn M, Hepburn S, Hyman SL,McMahon WM, et al. Is there a ‘regressive phenotype’ ofautism spectrum disorder associated with the measles-mumps-rubella vaccine? A CPEA study. Journal of Autismand Developmental Disorders 2006;36:299–316.
28. Siperstein R, Volkmar F. Brief report: Parental reporting ofregression in children with pervasive developmental disorder.Journal of Autism and Developmental Disorders 2004;34:731–734.
29. Tuchman BG, Rapin I. Regression in pervasive develop-mental disorders: Seizures and epileptiform electroencepha-logram correlates. Pediatrics 1997;97:560–566.
30. World Health Organization. International Classification ofDiseases, 10th ed. Geneva, Switzerland: WHO; 1992.
31. Crocker L, Algina J. Introduction to classical and modern testtheory. New York: Holt, Rinehart, and Winston; 1986.
32. DeVillis RF. Scale development: Theory andapplications. Thousand Oaks, CA: Sage Publications,Inc.; 1991.
33. Matson JL, Gonzalez ML, Wilkins J, Rivet TT. Reliability ofthe Autism Spectrum Disorders-Diagnostic for Children(ASD-DC). Research in Autism Spectrum Disorders2008;2:533–545.
34. Matson JL, Gonzalez ML, Wilkins J. Validity study ofthe Autism Spectrum Disorders-Diagnostic for Children(ASD-DC). Research in Autism Spectrum Disorders2009;3:196–206.
35. Matson JL, Wilkins J. Reliability of the AutismSpectrum Disorders-Comorbid for Children (ASD-CC).Journal of Developmental and Physical Disabilities 2008;20:327–336.
36. Matson JL, Gonzalez ML, Rivet TT. Reliability of theAutism Spectrum Disorder-Behavior Problems forChildren (ASD-BPC). Research in Autism Spectrum2008;2:696–706.
37. Matson JL. The Matson evaluation of social skillswith youngsters: Manual. Available at www.disabilityconsultants.org. Orland Park, IL: InternationalDiagnostics Systems, Incorporated; 1989.
38. Matson JL, Stabinsky-Compton L, Sevin JA. Comparisonand item analysis of the MESSY for autistic and normalchildren. Research in Developmental Disabilities 1991;12:361–369.
39. Wilkins J, Matson JL. Social skills. In: Matson JL,editor. Handbook of assessment in persons withintellectual disability. San Diego, CA: Elsevier Science,Inc; 2007. pp 321–363.
40. Tabachnick BG, Fidell LS. Using multivariate statistics,4th ed. Needham Heights, MA: Allyn and Bacon; 2001.
41. Golberg WA, Osann K, Filipek PA, Laulhere T, Jarvis K,Modahl C, Flodman P, Spench MA. Language and otherregression: Assessment and timing. Journal of Autism andDevelopmental Disorders 2003;33:607–616.
42. Hoshino Y, Kaneko M, Yashima Y, Kumashiro H,Volkmar FR, Cohen DJ. Clinical features of autistic childrenwith setback course in their infancy. Japanese Journal ofPsychiatry and Neurology 1987;41:237–245.
43. De Giacomo A, Fombonne E. Parental recognition ofdevelopmental abnormalities in autism. European Childand Adolescent Psychiatry 1998;7:131–136.
44. Hendry CN. Childhood disintegrative disorder: Should it beconsidered a distinct diagnosis? Clinical Psychology Review2000;20:77–90.
Autism spectrum disorders 45
Dev
Neu
rore
habi
l 201
0.13
:37-
45.
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f C
alif
orni
a Ir
vine
on
10/3
0/14
. For
per
sona
l use
onl
y.





























