Embed Size (px)
Citation preview

VU Research Portal
The impact of BRCA1 and BRCA2 germline mutations on breast cancer outcome inyoung womenvan den Broek, A.J.
2017
document versionPublisher's PDF, also known as Version of record
Link to publication in VU Research Portal
citation for published version (APA)van den Broek, A. J. (2017). The impact of BRCA1 and BRCA2 germline mutations on breast cancer outcome inyoung women.
General rightsCopyright and moral rights for the publications made accessible in the public portal are retained by the authors and/or other copyright ownersand it is a condition of accessing publications that users recognise and abide by the legal requirements associated with these rights.
• Users may download and print one copy of any publication from the public portal for the purpose of private study or research. • You may not further distribute the material or use it for any profit-making activity or commercial gain • You may freely distribute the URL identifying the publication in the public portal ?
Take down policyIf you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediatelyand investigate your claim.
E-mail address:[email protected]
Download date: 18. Jul. 2021

Chapter 9

General dIsCussIon and future perspeCtIves


General discussion and future perspectives 335
9
general discussion and future PersPectiVes
Precision medicine, rendering diagnostic and treatment decisions more tailored to the individual, is an important goal of research. A key component of precision medicine is to identify subgroups with differences in disease risk and outcome perspectives, so preven-tive measures and treatment decisions can be made accordingly. Since more is known about a person’s genetic make-up, but also the make-up of tumours, many advances in the field of personalised cancer care have been made. Specifically, after the discovery of the BRCA1 and BRCA2 genes in the early 1990s, it soon became clear that carriers of a germline mutation in these genes face a high lifetime risk to develop breast and ovarian cancer. Directly thereafter BRCA1/2 mutation status was used for cancer risk stratification, generating the possibility to offer mutation carriers personalised options, such as intensified surveillance or prophylactic surgeries, to manage their high breast and ovarian cancer risks.
In early studies, it was observed that women with BRCA1/2 mutations who develop breast cancer are often diagnosed with tumours with unique characteristics, possibly leading to a worse prognosis. This observation, together with the knowledge about the biological functions of the genes, suggested that breast cancer patients with a BRCA1 or BRCA2 germline mutation should be considered a unique patient group. This idea triggered investigations into the differences in breast cancer outcome between patients with and without mutations, so treatment choices and surveillance policies for BRCA1/2 mutation carriers with breast cancer could be optimized accordingly. In the 20 years after the discovery of BRCA1 and BRCA2, notwithstanding many studies, discussion about breast cancer outcome of BRCA1/2 mutation carriers is ongoing. Most guidelines for breast cancer care still treat BRCA1/2 mutation carriers similar to non-carriers due to lack of sufficient evidence. Therefore, in this thesis we aimed to study the impact of BRCA1 and BRCA2 germline mutations on breast cancer outcome.
After summarising the existing literature about the impact of BRCA1 and BRCA2 germline mutations on breast cancer outcome, the BOSOM study with its strengths, limitations, and ethical considerations, will be discussed. Thereafter the main findings of the BOSOM study described in the different chapters of this thesis will be summarized, and implications for clinical practice and future perspectives of the research field will be discussed.

336
Insufficient evidence about the impact of BRCA1/2 on breast cancer outcome in the existing literature?
chapter 2 describes a comprehensive systematic review we performed on previously published studies investigating breast cancer prognosis of BRCA1 and BRCA2 mutation carriers compared to non-carriers. We aimed to give the best available evidence about what was known so far, using among others methodological quality assessment of the published studies. As introduced in chapter 1 and above, there is still ongoing discussion about the subject, which is reflected by the wealth of studies done. The main conclusion of our systematic review was that there was some evidence (only “moderate”) for a worse recurrence-free survival for BRCA1 mutation carriers compared to non-carriers, unadjusted for tumour characteristics. For all the other outcomes; overall survival, breast-cancer specific survival, and metastasis-free survival, the evidence was judged to be indecisive. When using estimates that were adjusted for tumour characteristics, the evidence for all the outcomes, including recurrence-free survival, were also judged indecisive. The reason for these conclusions of indecisive evidence, despite the impres-sive number of studies that has already been done, is that the previously performed studies often lacked power and mutation types and outcomes reported per study var-ied greatly. Additionally, when enough estimates for an outcome were available, the reported results were inconsistent. This inconsistency is probably due to differences in study design, study size, study populations and methodological quality. We used a quality scoring system to explore whether study quality contributed to the discrepan-cies in conclusions among the studies. Surprisingly, we did not find factors that strongly explained the heterogeneity of the results. However, our results showed that there was often lack of power in the individual studies, and no study with sufficient power did not suffer from some form of bias. The most important potential form of bias in this type of studies is selection bias: there are often major systematic differences between the selec-tion of the BRCA1/2 mutation carriers, and the selection of the comparison group used (non-carriers/sporadic breast cancer patients). Most studies included carriers identified on the basis of family history, often through the Clinical Genetic Centre. Moreover, these inclusion methods easily lead to inclusion of prevalent cases, e.g. including mainly the BRCA1/2 mutation carriers who survived longer because testing for BRCA1/2 mutations was only done in later years after the diagnosis of the breast cancer. This leads to survivor bias, which may distort the study results. Other forms of bias in this type of studies are confounding and lack of accounting for mediating variables (tumour characteristics were often not registered in previously done studies) and misclassification bias. To overcome these forms of methodological flaws, the BOSOM study was specifically designed to

General discussion and future perspectives 337
9
provide unbiased conclusions based on data with more power. The results described in this thesis are based on this study.
Strengths and limitations of the BOSOM study
The BOSOM (Breast Cancer Outcome Study Of Mutation Carriers) study comprises an unselected, i.e. not family or clinical genetic centre-based, retrospectively ascertained, multicentre cohort of more than 6000 female patients with invasive breast cancer di-agnosed before age 50 years. Consecutive breast cancer patient series were extracted from 10 different hospital tumour registries. Young breast cancer patients, especially those <40 years, have been shown to have worse survival compared to older patients (Beadle et al, 2011; Brenner et al, 2016; Narod, 2012). Young breast cancer patients are also more likely to carry BRCA1/2 germline mutations (John et al, 2007; Malone et al, 2006; Peto et al, 1999). These observations render the younger breast cancer population a more urgent and identifiable group to study the impact of BRCA1/2 mutations on prog-nosis. To avoid survivor bias, an effort was made to collect germline DNA from healthy tissues for all the patients in the cohort; at least not selected on whether they survived a certain time. To achieve this, mainly residual formalin-fixed paraffin-embedded normal tissues from the hospital archives were used to isolate DNA. The availability of BRCA1/2 genotypes of all patients (though representing a selection of most prevalent BRCA1/2 germline mutations) is an important strength of the BOSOM study. One disadvantage of our used method is that (breast) surgery should have been performed; otherwise no archived tissue would be available for DNA isolation. Because of this, patients with a very poor prognosis for whom surgery was not even considered, were not included in the cohort. The percentage of those among young breast cancer patients is small (Voogd et al, 1994), and exclusion of these patients was done without awareness of the patients’ BRCA1/2 mutation status. However, it should still be taken into account that the results described in this thesis are only applicable to patients who are eligible for curative surgery.
Patients included in the cohort were treated for their primary breast cancer in 10 different centres throughout The Netherlands. We refer to the BOSOM study as hospital-based; however, because the coverage of the included hospitals in some areas was high, part of the cohort could be considered population-based. The patients were diagnosed in the years between 1970 and 2003; being mostly a representation of a period of di-agnosis in which patients (and physicians) were not aware of their BRCA1/2 mutation carriership, and therefore the BRCA1/2 mutation status was less likely to have affected their choice of treatment. Comprehensive data, on clinical and tumour characteristics,

338
follow-up ((disease specific-) survival and second tumours; median follow-up 14 years), but also data on prophylactic surgeries during follow-up, were collected for all patients in the cohort, mainly through linkage with different nationwide data registries (the Neth-erlands Cancer Registry (van der Sanden et al, 1995); and the nationwide network and registry of histo- and cytopathology (PALGA) (Casparie et al, 2007)). Due to the high risk of second breast tumours and ovarian cancer (Antoniou et al, 2003; Brohet et al, 2014; Chen & Parmigiani, 2007; King et al, 2003; Mavaddat et al, 2013), BRCA1/2 mutation carriers often opt for prophylactic surgeries (King et al, 2011; Metcalfe et al, 2008), and taking this into account for outcome investigation of this patient group is important.
More details on the study; especially the methods for BRCA1/2 mutation testing, are found in chapter 3 of this thesis. In chapter 3 an important limitation of the BOSOM study is also highlighted. When the BOSOM study was originally designed (2001), less families with BRCA1/2 mutations in The Netherlands had been identified. The mutations selected for testing in the BOSOM studies were based on the available data at that time. Back then it was estimated we would capture around 80% of the pathogenic BRCA1 mutations and 56% of the pathogenic BRCA2 mutations that were prevalent in families in The Netherlands. During the project, we added additional BRCA1/2 mutations. Even so, in the last calculation comparing the mutations we tested with the proportion of families with specific BRCA1 and BRCA2 mutations in The Netherlands, this estimation decreased to 69% and 46%, respectively. Consequently, we are now aware that we missed a larger proportion than initially expected of BRCA1/2 mutation carriers in our cohort. Assuming these rare mutations are of similar penetrance (all are known to be pathogenic), it may have led to a slight underestimation of the risk estimates described in this thesis. Also, we screened for a higher percentage of BRCA1 mutations than BRCA2 mutations, because BRCA2 mutation carriers are less prevalent in the Dutch population. This makes the results in this thesis for BRCA1 mutation carriers more powerful than for BRCA2 mutation carriers; moreover, combined results were mostly driven by the BRCA1 mutation carriers. Although more than 6000 patients are included in the BOSOM study, BRCA1/2 mutations, certainly in breast cancer patients unselected for family history, are rare (prevalence BOSOM study 4.5%). The BOSOM study certainly has more power than the previously performed studies which also had an unbiased design, however, the power is still limited, and results from subgroup analyses discussed in this thesis should be interpreted with caution.
Our study took a long time but we pioneered in performing such an extensive study using archival tissue. Nowadays, with the wider availability of electronic patients re-cords, modern structured pathology archives, and the availability of better and cheaper

General discussion and future perspectives 339
9
DNA isolation kits and sequencing methods (Metzker, 2010; Pettersson et al, 2009), such a retrospective study could be done much quicker and less costly. Prospective studies would be preferable, but these will take a lot of time to have sufficient follow-up avail-able. More importantly, a prospective study would have been affected to a larger extent by the introduction of BRCA1/2 mutation screening in clinical genetics.
The use of residual tissues for research in the BOSOM study
As described in the above paragraph, the most important strength of the BOSOM study is availability of BRCA1/2 genotypes of all patients, irrespective of their survival status. Testing was mainly performed on residual formalin-fixed paraffin-embedded tissue that was obtained during earlier clinical procedures, without specific consent from the pa-tient. This procedure raises a number of issues, specifically regarding patient privacy and the right of self-determination. These issues become even more relevant because BRCA1 and BRCA2 mutations lead to a high susceptibility to cancer (Antoniou et al, 2003; Brohet et al, 2014; Chen & Parmigiani, 2007; King et al, 2003; Mavaddat et al, 2013). The results of a BRCA1/2 mutation analysis may not only have consequences for the patient herself (if still alive), but also concern her relatives who possibly do not (yet) know if they are a carrier. The consequences primarily include dealing with the knowledge of mutation car-riership, with implications for options to manage the cancer risks. However, without this type of observational research not requiring consent, unbiased investigations cannot be performed, and no definite answers can be given to important research questions for this patient group, such as described in this thesis.
In the Netherlands we have the Dutch codes of conduct (Federa, 2011; Riegman & van Veen, 2011), describing rules for the secondary use of residual human materials and data. In case it is not feasible or desirable to ask for informed consent (e.g. patients are treated a long time ago, and asking them can generate unneeded worries) the general rule is that, under the condition that a patient has not objected to this ‘secondary use’, the residual material can be used without consent when the patient data is anonymized or coded.
In the BOSOM study we followed Dutch regulations including the Dutch codes of conduct (Federa, 2011; Riegman & van Veen, 2011). The general rule with this ‘second-ary use without asking for informed consent’ is that the patient data have to be either anonymized or coded. When creating fully anonymized data, this means that the use of the data is limited for use in future research as for example follow-up information can no longer be obtained. For the BOSOM study a special coding procedure based on the Dutch Code of Conduct was developed (Schmidt et al, 2009), making use of a ‘trusted

340
third party’ with a specific coding procedure. The clinical data and BRCA1/2 mutation re-sults were thereby anonymized before linkage. With this method, the violation of privacy and personal integrity is minimized and security of the mutation results is maximized, while keeping the opportunities for using the data for future research. In this era where more and more data becomes available and (data) privacy and personal integrity are an important topic of discussion, such methods for data coding are very feasible. This method is surely of interest for future studies in (high-risk) germline variants, but also for other studies with privacy sensitive data.
‘Secondary use’ without asking for informed consent implies that it is more difficult if not sometimes impossible to report back findings to the patients, especially if they are no longer under follow-up. In the fast-moving fields of genetics and genomics, the complex discussion about disclosure of (incidental) findings has intensified (Scott et al, 2012; Wolf, 2013). Recent studies showed that most patients want to be informed about the results; to be able to have more choice and control over their own health (Beskow & Smolek, 2009; Bollinger et al, 2012; Meulenkamp et al, 2010).
Before the start of and during the course of the BOSOM study, the consequences of such a ‘secondary use without asking for informed consent’ study design for the patients themselves and their families have extensively been discussed with medical ethical com-mittees and clinicians (Schmidt et al, 2004; Schmidt et al, 2009). In these discussions, there was, among others, reflection on the possible impact of knowledge of BRCA1/2 mutation carriership, the lack of certainty of the results for the non-carriers, the balance between right to know and right not to know, performance of the mutation analysis in a research setting (compared to certified clinical laboratories less strictly controlled), and the feasibility and costs of tracing back the patients and/or families. The conclusion based on all these discussions were that the BOSOM study would only be feasible (and in view of some people even only desirable) without re-contacting the patients – i.e. those alive and traceable- and/or their families. There were several reasons why this conclusion was made. Most importantly because the patients in this cohort were diag-nosed with breast cancer several years ago (<2003); many patients were deceased or already knew their mutation status, and bothering them or their families could cause a lot of distress (Clayton, 2008). In chapter 8 of this thesis we showed that most (>70%) BRCA1/2 mutation carriers diagnosed after 1995 in the BOSOM study were (eventually) referred to the Clinical Genetic Centre, so knowledge about their BRCA1/2 mutation status was already available for them and their family members. It is important to note that the BOSOM study ran over many years; and only from 2007 onwards we started

General discussion and future perspectives 341
9
including patients that were diagnosed after 1995 as well. Also, when the study started it was expected that patients who were still under surveillance in the hospital would already have been informed by their treating physicians of the possibilities of counsel-ling and BRCA1/2 mutation testing when this was applicable (those patients with an extensive family history). Likely, such patients made a well-funded decision to undergo or not undergo BRCA1/2 mutation testing. Patients without a family history may be less informed about counselling and BRCA1/2 testing, but especially in those families the impact and relevance of BRCA1/2 carriership was still unclear at the start of the study.
In studies in which Dutch cancer and non-cancer patients were asked about their opinion and wishes for the secondary use of tissue, almost all (95-99%) indicated they would have consented to this type of research and did not object to the opt-out system (Rebers et al, 2016; Vermeulen et al, 2009a; Vermeulen et al, 2009b). In addition, the large majority indicated they were happy for their materials to be used, even if no indi-vidual results were returned, though if possible this would be appreciated (Rebers et al, 2016). Return of results from research is in transition, and in future research there will hopefully be better opportunities to return individual results to patients.
Worse breast cancer outcome for breast cancer patients with BRCA1/2 germline mutations?
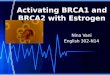
- Results of the BOSOM studyIn chapter 4 we described breast cancer outcomes for BRCA1/2 mutation carriers compared to non-carriers in the BOSOM study. We found that both BRCA1- and BRCA2-mutation carriers have a worse overall survival compared to non-carriers, though the effect sizes were small; absolute overall survival differences were around 10% after 10 years (hazard ratios ~ 1.3). When comparing the survival estimates from the BOSOM study (chapter 4) with the corresponding pooled survival estimates we calculated in our systematic review described in chapter 2 (see figure next page), we notice that for BRCA1 mutation carriers the estimates are generally in line, however, this is not the case for BRCA2 mutation carriers. This is not so surprising as fewer previously published stud-ies looked at this group, and also power was often insufficient in the separate studies.

342
figure 1: Survival estimates from the BOSOM study (chapter 4) compared to the corresponding pooled survival estimates calculated in the systematic review described in chapter 2.Pooled HR (dotted bullet) Pooled hazard ratio from the systematic review for BRCA1/2 mutation carriers com-pared to non-carriers (chapter 2, table 3): unadjusted= the pooled estimate is calculated from hazard ratios that were not adjusted for tumour characteristics and/or treatment, adjusted*=the pooled estimate is calculated from hazard ratios that were adjusted for tumour characteristics and/or treatment; BOSOM HR (black bullet) hazard ratio for BRCA1/2 mutation carriers compared to non-carriers in the BOSOM study (chapter 4, supple-mentary table 3): unadjusted, adjusted*=the hazard ratio is adjusted for tumour characteristics and treatment, adjusted**=the hazard ratio is adjusted for tumour characteristics, treatment, second primary breast cancer, and primary ovarian cancer.
In the BOSOM study, we observed that for BRCA1 mutation carriers the worse survival was most pronounced in the first 5 years; for BRCA2 mutation carriers the worse survival was most pronounced in the later years of follow-up (chapter 4). Interestingly, when looking at the pooled absolute survival differences as described in chapter 2 for 5-year and 10-year overall survival, the survival patterns we see in the BOSOM study are not found (similar pooled absolute survival differences at 5 and 10 years of follow-up). However, the inconsistency of previously reported results and large differences in study populations and study quality, as highlighted in chapter 2, should be considered here. Also, most previously published studies did not report separate hazard ratios or absolute differences for different time periods after diagnosis, so the pooled estimates as reported in chapter 2 are based on estimates from different sets of studies. E.g. practically none of the previously performed studies contributed data to all pooled estimates making them harder to compare.
The differential survival patterns of BRCA1 and BRCA2 mutation carriers compared to non-carriers, and also specifically the mechanisms behind these differences, are of interest because surveillance strategies and/or treatment choices might be tailored to this. Breast tumours arising in BRCA1 mutation carriers have been shown to differ in standard clinico-pathological features that guide treatment decisions (Coates et al,

General discussion and future perspectives 343
9
2015), such as grade, from tumours arising in non-carriers (Honrado et al, 2006; Lakhani et al, 2002; Phillips, 2001). For tumours in BRCA2 mutation carriers this difference is less pronounced (Honrado et al, 2006; Lakhani et al, 2002; Phillips, 2001). Also in the BOSOM study we found marked differences between the tumours in the different patient groups, as we discussed specifically in chapters 3 and 4. If these standard clinico-pathological factors would solely explain the differential survival patterns, it would be reassuring that the prognosis of BRCA1/2 mutation carriers is not negatively influenced purely by their BRCA1/2 mutation status, and guidelines for sporadic patients could also be used for BRCA1 and BRCA2 mutation carriers. In chapter 2 of this thesis we tried to sum up all information from the previously published studies about this. In general, the associa-tions between BRCA1/2 carriership and prognosis became less strong after adjustment for clinico-pathological characteristics, especially when the unadjusted results showed a worse survival for the carriers. Also, a recent review on this subject concluded that estrogen receptor status appeared to be an effect modifier of prognosis in patients with BRCA1 mutations (Templeton et al, 2016). This already suggested that at least part of the potential worse prognosis might be explained by the difference of tumour characteristics in BRCA1/2 mutation carriers compared to non-carriers. In the BOSOM study, we also showed that the worse survival for BRCA1 and BRCA2 mutation carriers is partly, though certainly not solely, explained by differential clinico-pathological characteristics (hazard ratio decrease after adjustment ~ 0.1) (chapter 4).
Another factor that may underlie the worse survival seen for BRCA1 and BRCA2 muta-tion carriers compared to non-carriers, is the increased risk to develop a second primary breast tumour, and in overall survival also the increased risk for a subsequent ovarian cancer (Chen & Parmigiani, 2007; Kirova et al, 2010; Mavaddat et al, 2013). In chapters 6 and 7 of this thesis we confirmed the high risks for these tumours for BRCA1 mutation carriers; for BRCA2 mutation carriers we also observed an increased risk for contralateral breast cancer, but not a single BRCA2 mutation carrier developed ovarian cancer during follow-up. In chapter 4 we show that part of the worse survival for BRCA1 mutation carriers is attributable to the increased risk of ovarian cancer. In this chapter, we also show that the worse breast cancer-specific survival is less strong than the worse overall survival of BRCA1 mutation carriers compared to non-carriers, which support the finding that specifically ovarian cancer plays a role in the decreased survival of BRCA1 mutation carriers. No previous study that investigated the outcome of BRCA1/2 mutation carriers looked at a role for ovarian cancer (chapter 2) , but our results are in line with reports of subsequent ovarian cancer in breast cancer patients <50 years (Berkowitz et al, 2011);

344
and the previously reported protective impact of oophorectomy after breast cancer on mortality (Metcalfe et al, 2015).
Interestingly, in the BOSOM study, developing a second primary breast cancer did not seem to negatively affect the survival of BRCA1 and BRCA2 mutation carriers, while in non-carriers getting a second primary breast cancer led to a clearly worse survival (chap-ter 4). However, we still observed a protective effect of prophylactic mastectomy on overall survival for BRCA1/2 mutation carriers in the BOSOM study, which was supported by previously published data (Evans et al, 2013; Heemskerk-Gerritsen et al, 2015). The observation that second primary breast tumours in the BOSOM study did not negatively affect survival in BRCA1/2 mutation carriers might be explained by the fact that a large part of the mutation carriers in our cohort were referred to Clinical Genetic Centre later during follow-up (chapter 8), and more intensive surveillance, but also treatment of the second breast cancer, might be expected.
When looking at the effect of BRCA1 and BRCA2 mutations on overall survival after adjustment for both differential clinico-pathological factors and differential second pri-mary tumour risk as described in chapter 4, there is still a residual, but non-significant, worse overall survival for BRCA1 and BRCA2 mutation carriers (Hazard ratios ~ 1.2). For breast cancer-specific survival a worse outcome was not present anymore after adjust-ment, although the specific pattern, with a more pronounced differential survival in the first 5 years for BRCA1 and in the latest years in follow-up for BRCA2, remained. What should be remembered in the above discussion is that currently, next to the standard clinico-pathological characteristics, more detailed tumour biology, e.g. gene expression profiling, are used to guide treatment decisions (Cardoso et al, 2016; Coates et al, 2015; Goldhirsch et al, 2011; Lewin et al, 2016). A recent paper showed differential distribu-tions for a clinically used gene expression profile in BRCA1/2 mutation carriers compared to non-carriers (Lewin et al, 2016). How these gene expression profiles affect survival in this patient group, and to what extent they might even more explain the worse survival of BRCA1/2 mutation carriers, is something that should be addressed in future research (Alvarez et al, 2016).
Taken together, whether the residual effect of the BRCA1/2 mutation status on overall survival (after adjustment of tumour characteristics and second tumours), is solely due to the BRCA mutation itself, and cannot be accounted for by currently used prognostic factors, is debatable. Also, the residual effects we observe are very small (Hazard ratios ~ 1.2) and non-significant. This is in line with statements of others that worse survival in young breast cancer patients is more likely to be attributable to tumour subtype than due to BRCA1/2 mutations (Fredholm et al, 2009; Kroman et al, 2000). However, it should be kept in mind

General discussion and future perspectives 345
9
that a large part of the variability in prognosis of breast cancer patients is still unexplained (Dunkler et al, 2007; Eden et al, 2004), and also more subtle factors might contribute.
Differential systemic treatment response for BRCA1/2 mutation carriers?
Another interesting finding we described in chapter 4 is the interaction between chemo-therapy and BRCA1 mutation carriership. When only considering the untreated group, BRCA1 mutation carriers had a larger and significantly worse residual overall survival compared to non-carriers, also after adjustment for tumour characteristics and the pres-ence of second breast and ovarian tumours (HR ~1.5). In the chemotherapy-treated group no difference in overall survival was seen. As suggested by others (Arun et al, 2011; Huzarski et al, 2013; Robson, 2011; Robson et al, 2004), chemotherapy, although specifically DNA cross-linking agents, may be more effective in tumours arising in BRCA1 mutation carriers. This is also supported by data from trials (Schouten et al, 2016; Vol-lebergh et al, 2014), though this was related to “BRCAness” of the tumour and not to the germline BRCA1 mutation status specifically. This suggests that BRCA1 mutation carriers benefit more from chemotherapy than non-carriers. The evidence is not so convincing for BRCA2 mutation carriers. Currently, the more promising adjuvant strategy for treat-ment of BRCA1/2 mutation carriers are the PARP inhibitors (Livraghi & Garber, 2015; Scott et al, 2015; Sonnenblick et al, 2015). Unfortunately, in the years of diagnosis that are included in the BOSOM study, this treatment did not yet exist. However, all data together point to an important role of adjuvant systemic treatment in these patients, and this should always be considered when a breast cancer patient is known to be car-rying a BRCA1/2 mutation.
Precise risk estimates for second primary tumours for BRCA1/2 mutation carriers
As concluded in the above paragraphs, second tumours play an important role in the outcome of breast cancer patients with BRCA1/2 mutations. Next to the potential nega-tive impact on survival, a new cancer diagnoses gives rise to a lot of distress and women have to undergo invasive treatments again. In chapter 6, we gave unbiased absolute risk estimates for contralateral breast cancer, and we placed these into perspective with the already available risk estimates from mostly family-selected studies. Also, we identified age at diagnosis as an important factor that can be used for risk stratification in this high-risk patient group (10-year cumulative risk when diagnosed < age 41 of 24% compared to 13% when diagnose > age 40; hazard ratio ~ 1.9). Even more so, when these very young patients with BRCA1/2 mutations also had an (extensive) family history of breast cancer, we observed an even higher risk (10-year cumulative risk of 38%).

346
Next to this, we confirm in chapter 7 the increased risk for ovarian cancer for BRCA1 mutation carriers, as defined by subsequent ovarian cancer after breast cancer (10-year cumulative risk of 6%). In this chapter we also further explored the observation that mutations in certain parts of the BRCA1 gene explain part of the inter-individual cancer risks that exists in BRCA1 mutation carriers (Rebbeck et al, 2015). We described that BRCA1-associated breast cancer patients with mutations in the Ovarian Cancer Cluster Region are a subgroup with a relatively higher risk of ovarian cancer after breast cancer, but numbers in these analyses were small and our results should be confirmed.
As expected, we observed that many of the BRCA1/2 mutation carriers in the BOSOM study opted for prophylactic surgeries, i.e. mastectomy or oophorectomy during follow-up (chapters 4-7). This was also already shown by many others (Harmsen et al, 2016; King et al, 2011; Metcalfe et al, 2008; Tuttle et al, 2007), and uptake of prophylactic-surgeries even more increased after the news of Angelina Jolie being a carrier of a BRCA1 mutation and her choice for a prophylactic mastectomy (Raphael et al, 2016). Contralateral mas-tectomy, and possibly also oophorectomy, decreases the risk for second primary breast cancers (Evans et al, 2013; Heemskerk-Gerritsen et al, 2015; Li et al, 2016; Lostumbo et al, 2010; Metcalfe et al, 2011); and oophorectomy decreases the risk of ovarian cancer and thereby leads to an improved survival (Hartmann & Lindor, 2016; Huzarski et al, 2016; Li et al, 2016; Metcalfe et al, 2015). The contralateral risk estimates as described in chapter 6, and specifically age as risk stratifying factor, can be used to optimize counsel-ling for BRCA1/2 mutation carriers, so to identify the BRCA1/2 mutation carriers that have the highest need for intensified surveillance or prophylactic surgery. Our results show that breast cancer patients with BRCA1/2 mutations that were diagnosed at a young age are an important high risk group that should be considered for contralateral breast cancer risk-reducing strategies. Furthermore, with further confirmation, also the BRCA1 mutation location might be included in the risk estimation for ovarian cancer, and can help in the decision-making of prophylactic surgery for BRCA1 mutation carriers. Moreover, the overall increased risk of ovarian cancer and its impact on overall survival emphasise the importance of personalised strategies after breast cancer, especially for BRCA1 mutation carriers.
Breast conserving surgery or mastectomy for BRCA1/2 mutation carriers?
Many BRCA1/2 mutation carriers opt for prophylactic mastectomy of their breasts be-cause of their high risk to develop breast cancer. However, several BRCA1/2 mutation carriers are only identified as such after they already developed breast cancer. How the already affected breast should be treated in this patient group is still under debate.

General discussion and future perspectives 347
9
Several issues play a role; most importantly the risk of recurrences in the breast, taken specifically the risk of a new primary (ipsilateral) breast cancer into account. Current Dutch guidelines recommend, where possible, breast-conserving surgery followed by radiotherapy as opposed to mastectomy for early invasive breast cancer, and no dif-ferent strategy is advised for BRCA1/2 mutation carriers (NABON, 2012). Randomized trials comparing breast-conserving surgery and mastectomy are available for the general breast cancer population, showing no difference in survival (Clarke et al, 2005; Fisher et al, 2002; van Dongen et al, 2000; Veronesi et al, 2002), but these trials do not exist for BRCA1/2 mutation carriers. In chapter 5 we described the survival and in-breast recur-rence rates for breast-conserving surgery compared to mastectomy in BRCA1/2 mutation carriers and non-carriers. We did not find any marked differences in the effects of the different types of surgeries between BRCA1/2 mutation carriers and non-carriers. There is ongoing discussion about the benefits (less recurrences in the breast) and risks (more contralateral breast cancer) of radiotherapy in BRCA1/2 mutation carriers (Drooger et al, 2015; Kan & Zhang, 2015). As described in chapter 5, we did not observe a significant negative impact of radiotherapy in general on survival in the BOSOM study. What should be kept in mind, is that there remains debate about the value of observational studies in evaluating efficacy of treatment strategies (Chavez-MacGregor & Giordano, 2016; Ross, 2014), and results as described in chapter 5 should always be interpreted with cau-tion. On the other hand, whether there will ever be a randomized trial testing different surgery types in the BRCA1/2-associated breast cancer patient group is unlikely, and this type of data is probably the best we will get.
At least for now we can conclude that we did not identify a specific reason to change the currently used guidelines, which is also supported by the literature (Hallam et al, 2015; Valachis et al, 2014). Of course, patient preferences should always be taken into account in treatment decisions, and guidelines should be used for advice and reference. Furthermore, the risk of breast cancer in the opposite breast remains, and appropriate risk assessment should be performed, so this risk can be managed accordingly.
Unselected versus family-history selected BRCA1/2 mutation carriers
The BRCA1/2 mutation carriers as described in the different chapters of this thesis, are unselected for family history (though selected based on a young age at diagnosis (<50 years)). Whether these patients differ from BRCA1/2 mutation carriers as seen in the Clinical Genetic Centre (Gadzicki et al, 2011; NABON, 2012) is described in chapter 3. BRCA1 carriers that were referred to the Clinical Genetic Centre had a larger proportion of carriers with a family history of breast cancer compared to the whole BRCA1 mutation

348
carrier group in the BOSOM study; BRCA2 mutation carriers that were referred to the Clinical Genetic Centre had a larger proportion of young patients compared to the whole BRCA2 mutation carrier group in the BOSOM study. We also observed a relatively high percentage of ER+ tumours in BRCA1 mutation carriers (~30%) compared to previous literature (Honrado et al, 2006). Apparently, we captured a broader BRCA1/2 mutation carrier population than seen in the Clinical Genetic Centre. Of course, the group seen in the Clinical Genetic Centre is the group of most interest regarding surveillance and treatment guidelines; however, using this group in research poses some difficulties: e.g. the above discussed survivor bias; they may be treated differently due to the knowledge about their mutation status (Engelhardt et al, 2015); and selection of an appropriate comparison group is a bigger challenge. We think therefore we can conclude that the BOSOM study is a very suitable study population, and our results can be used for carri-ers identified in the Clinical Genetic Centre, taking into account that the penetrance of BRCA1/2 mutations in patients with a very extensive family history can be somewhat higher. E.g., as shown in chapter 6, family history has a modifying role in the risk of contralateral breast cancer for BRCA1/2 mutation carriers. These combined effects of mutation status and family history can be included in online models, such as BOADICEA (Antoniou et al, 2004; Lee et al, 2014), for counselling of healthy women and breast cancer patients.
Identification of BRCA1/2 mutation carriers among breast cancer patients
The unselected BRCA1/2 mutation carrier population in the BOSOM study also generated the opportunity to evaluate, and optimize, the Clinical Genetic Referral criteria used. The prevalence of women carrying a BRCA1/2 mutation within the general breast cancer patient population is low, and estimated to be around 1–2% for each gene (Thompson & Easton, 2004). Testing every breast cancer patient for a mutation is debatable: except for cost-effectiveness and feasibility reasons, there are also considerations regarding the impact of the counselling and testing procedures (Foulkes et al, 2016; Surbone, 2011). Currently, only in populations with a high prevalence of founder mutations population testing is considered (Foulkes et al, 2016; Gronwald et al, 2006). Referral guidelines, to identify breast cancer patients that have a high a priori change to carry a BRCA1/2 muta-tions, are mainly based on family history of breast cancer and ovarian cancer, but also age at diagnosis, and in some guidelines also tumour characteristics (triple negativity) are already included (Gadzicki et al, 2011; NABON, 2012). In chapter 8 we confirmed, based on existing literature and our results, that including triple negativity into the guidelines will identify more BRCA1/2 mutation carriers. Of course, our study population

General discussion and future perspectives 349
9
is under 50 years of age, and we cannot give conclusions about older patients. However, we expect that the prevalence of BRCA1/2 mutations in this patient group is much lower (Breast Cancer Linkage, 1997; Foulkes et al, 1997; Rennert et al, 2007; Thompson & Easton, 2004). Better population data about prevalence of BRCA1/2 germline mutations in older women will become available through the ongoing EU Horizon2020 BRIDGES project (http://www.bridges-research.eu).
clInIcal IMPlIcaTIons
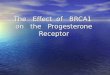
Knowledge about the BRCA1/2 mutation status of a breast cancer patient is already used in clinical practice for many years, particularly, to estimate a patients’ risk for second breast cancer and ovarian cancer, and advice about possible surveillance strategies and risk-reducing surgeries to manage the risks. In the chapters 6 and 7 of this thesis we provide unbiased absolute risk estimates for contralateral breast cancer and ovarian cancer for these patients (figure below).
figure 2: Summary of the 10-year cumulative ovarian cancer and contralateral breast cancer risks for breast can-cer patient without a mutation (non-carriers) and breast cancer patients with a BRCA1 or BRCA2 mutation from the BOSOM study (chapters 6 and 7 of this thesis).BC breast cancer; numbers in brackets are 95% confidence intervals.
Previously used risk estimates were mostly based on BRCA1/2 mutation carriers with an extensive family history of cancer. Families in Western countries are becoming smaller and also other factors to identify BRCA1/2 mutation carriers, such as the type of breast tumour as we discussed in chapter 8, are becoming more important (Weitzel et al, 2007). In the future, more BRCA1/2 mutation carriers without an extensive family history will potentially be identified. Furthermore, previously published second cancer

350
risk estimates were potentially distorted by selection bias, and were not corrected for competing events, thereby potentially overestimating the true absolute risk. Next to this, we identified age at diagnosis as an important risk stratifier (figure previous page), which can be used to identify the young group of patients with BRCA1/2 mutations that have the highest need of risk-reducing strategies. Moreover, the increased risk of ovar-ian cancer after breast cancer for BRCA1 mutation carriers (figure previous page), and the large impact of this ovarian cancer on overall survival (chapter 4), emphasises the importance of personalised strategies after breast cancer, especially for BRCA1 mutation carriers.
Whether breast cancer patients with BRCA1/2 mutations also have a worse survival compared to non-carriers, after accounting for the high risk for second breast cancer and ovarian cancer, has always been a subject of debate. Many physicians and research-ers believe that BRCA1 mutation carriers have worse breast cancer survival, probably due to their less favourable tumour characteristics. In this thesis, we show that there indeed seems to be a (non-significant) residual overall survival disadvantage for both BRCA1 and BRCA2 mutation carriers, even when accounting for the less favourable tumour characteristics and second tumours. However, our results reassure that if this disadvantage is really present, it is very small (chapters 2 and 3). In agreement with this, we found no indication that breast-conserving surgery is not a safe option for BRCA1/2 mutation carriers. These observations support the currently used guideline that no dif-ferent breast cancer surgery strategy is advised for BRCA1/2 mutation carriers compared to non-carriers (NABON, 2012).
The small overall survival disadvantage we observed for BRCA1 mutation carriers compared to non-carriers described in this thesis was stronger in the group of patients not treated with systemic chemotherapy. The survival disadvantage was not observed in the chemotherapy-treated group. This suggests that BRCA1 mutation carriers experi-ence more benefit from treatment with chemotherapy, what has also been implicated before (Arun et al, 2011; Huzarski et al, 2013; Robson, 2011; Robson et al, 2004). In the Netherlands BRCA1/2 mutation carriers who know their mutation status before the breast cancer diagnosis through identification in the Clinical Genetic Setting, have been shown to already more often opt for adjuvant chemotherapy (Engelhardt et al, 2015). Our data supports this choice in general, but of course there may still be a subgroup of BRCA1 mutation carriers who do not need adjuvant treatment, and who we might be over-treating. Identification of the BRCA1/2 mutation status before treatment decisions are made is important, certainly with the promising new PARP inhibitors for this patient group. In chapter 8 we demonstrate that expanding the Clinical Genetic Centre refer-

General discussion and future perspectives 351
9
ral guidelines for breast cancer patients with information about tumour characteristics (specifically triple negativity) will identify more BRCA1 mutation carriers. Since rapid genetic testing became more feasible and accepted in recent years (Wevers et al, 2016), this gives patients and their physicians the opportunity to optimize breast cancer treat-ment with the knowledge of the BRCA1/2 mutation status.
future PersPectiVes
Because of the particular study design of the BOSOM study, the results described in this thesis are unique. Repeating such a study with the newer sequencing techniques, and with the same amount of other data available, will (still) be very labour intensive and costly. Hopefully this will change in the near future: new studies are needed to confirm our results, preferably with unselected and prospectively ascertained BRCA1/2 mutation carriers, and with even more power to perform subgroup analyses. However, in a few years’ time the number of events will have increased in the BOSOM study, providing the opportunity to re-analyse these data with increased power. In the decision whether research should invest in the updates of follow-up of retrospective studies based on older years of diagnosis or in the start of new prospective studies, the length of follow-up needed to study long-term outcome, the relevance of older treatment modalities, and the possibilities of unbiased study design need to be considered. Certainly, sufficient information about the breast cancer outcome of BRCA2 mutation carriers is still lacking; also within this thesis no firm conclusions could be drawn due to small numbers, what makes them a relatively unidentified group. Often they are taken together and treated similarly as BRCA1 mutation carriers, while most data suggest they are different (all chapters of this thesis). A more complete BRCA1/2 mutation analysis in the BOSOM would be very beneficial in this respect, but challenging due to the quality of the FFPE-derived DNA. We are only at the start of trying to understand whether different BRCA1 or BRCA2 mutations may have a differential impact on breast cancer outcome (chapter 7). Though it may be debated whether such differences will be large enough to lead to differential clinical management within mutation carriers, further studying this may help understand the etiology of breast cancer risk and outcome of BRCA1/2 mutation carriers.
The Dutch national HEBON (HEreditary Breast and Ovarian cancer Netherlands; www.hebon.nl) study, including BRCA1/2 mutation carriers identified through clinical genetic centres, may contribute to more in-depth analyses of treatment response to different chemo- and hormonal therapeutics including more recent regimens. Moreover, further

352
investigation is needed of other modifying or protective factors for the development of contralateral breast cancer, such as adjuvant tamoxifen treatment for the first breast cancer. For such questions, prospective cohorts of BRCA1/2 mutation carriers such as the IBCCS (International BRCA1/2 Carrier Cohort Study; www.ibccs.nl) may be able to provide answers in the future. There is evidence for a decrease of contralateral breast cancer risk after tamoxifen treatment for the first breast cancer (Phillips et al, 2013; Xu et al, 2015). However, it is yet unknown whether this also holds for aromatase inhibitors or other chemotherapeutics (Reding et al, 2010). So far, we did see a suggestion of a protective effect for contralateral breast cancer of chemotherapy in the BOSOM study (chapter 6), but the number of patients treated with endocrine treatment is too small to observe any associations.
Potential pitfalls for new studies are obviously the risk of (e.g. selection and survivor) biases in this type of research, and the current era we live in: most carriers diagnosed with breast cancer now will know their mutation status, which may affect their behaviour with respect to treatment, preventive surgeries and possibly intensified surveillance, making it harder to draw unbiased conclusions. Fortunately, in the field of “BRCAness” many advances are made, and this knowledge will also contribute to insights for BRCA1/2 mutation carriers. BRCA1/2 mutation-associated tumours often have specific patterns of genomic changes due to the defects in homologous recombination for the repair of double strand breaks (Jonsson et al, 2005; van Beers et al, 2005; Vollebergh et al, 2011; Wessels et al, 2002). Those tumours with this “BRCAness” phenotype (Lord & Ashworth, 2016; Turner et al, 2004) mostly but not exclusively occur in BRCA1/2 germline mutation carriers. Extending the BOSOM study with for example sequencing of the primary breast tumours will give even more insights about the tumours arising in this patient group, and would be a valuable addition for future analyses.
In the last few years, tumour genetic data has increasingly been incorporated into prognostication guidelines, and this trend is likely to continue in the coming years. Consequently, more detailed (genetic) characteristics of tumours in BRCA1/2 mutation carriers will be found, and surveillance policies and treatment options can be fitted to this. A good example are the PARP inhibitors, which are very a promising targeted treat-ment strategy for BRCA1/2-associated tumours. Moreover, medicine is getting more and more genome-guided, and prediction models for both (second) cancer risk and clinical outcome, will include more detailed factors and will become more precise. The variabil-ity of clinical outcome of breast cancer is still largely unexplained (Dunkler et al, 2007; Eden et al, 2004). Many factors influence outcome in an individual patient, including

General discussion and future perspectives 353
9
inherited genetic variation (Guo et al, 2015; Hartman et al, 2007; Lindstrom et al, 2007; Verkooijen et al, 2012), as is also shown in this thesis for BRCA1/2 germline mutations.
To identify with more power these genetic, but also non-genetic, risk stratifiers of risk and outcome, data from several studies are now being combined in large consortia, with partners from all over the world. Good examples of these efforts are the BRIDGES (www.bridges-research.eu) and B-CAST (www.b-cast.eu) initiatives, where all known breast cancer susceptibility genes will be sequenced in 20,000 breast cancer patients with comprehensive clinico-pathological data available, and the tumours within these patients will be classified into subtypes using molecular markers and sequencing. Preci-sion medicine, tailoring care more to the individual, is expected to evolve even more in the coming years.
concluding remarks
Previous data suggested BRCA1/2 mutation carriers might have a worse breast cancer outcome compared to non-carriers, and should be treated as a different patient group. We indeed confirm that BRCA1/2 mutation carriers have a worse breast cancer outcome, although this is mainly explained by differential clinico-pathological characteristics, second ovarian cancer and a differential treatment response. Although outcome, when accounting for standard prognostication factors, in non-carriers and mutation carriers seems to quite similar, systemic adjuvant therapy seems to be more effective, and with the new targeted treatment strategies available (e.g. PARP inhibitors). In this thesis, we also showed the high risk for second breast cancer, especially for young BRCA1 mutation-related breast cancers. Based on these observations, we can conclude that BRCA1/2 mutation carriers should certainly be considered unique. Moreover, BRCA1 mu-tation carriers have a high risk to develop ovarian cancer with a clear impact on overall survival, and this indicates the importance of personalised strategies after breast cancer for this patient subgroup. We expect that in the coming years the biological (genetic) features, of patients and tumours, will be further elucidated, personalising cancer care for different patient groups even more. Challenges will lie in setting up large studies with sufficient power, but keeping an eye on the high risk of biases and their potential to distort research findings.

354
RefeRences
Alvarez C, Aravena A, Tapia T, Rozenblum E, Solis L, Corvalan A, Camus M, Alvarez M, Munroe D, Maass A, Carvallo P (2016) Different Array CGH profiles within hereditary breast cancer tumors associated to BRCA1 expression and overall survival. BMC cancer16: 219
Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O, Borg A, Pasini B, Radice P, Manoukian S, Eccles DM, Tang N, Olah E, Anton-Culver H, Warner E, Lubinski J, Gronwald J, Gorski B, Tulinius H, Thorlacius S, Eerola H, Nevanlinna H, Syrjakoski K, Kallioniemi OP, Thompson D, Evans C, Peto J, Lalloo F, Evans DG, Easton DF (2003) Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. American journal of human genetics72(5): 1117-30
Antoniou AC, Pharoah PP, Smith P, Easton DF (2004) The BOADICEA model of genetic susceptibility to breast and ovarian cancer. British journal of cancer91(8): 1580-90
Arun B, Bayraktar S, Liu DD, Gutierrez Barrera AM, Atchley D, Pusztai L, Litton JK, Valero V, Meric-Bernstam F, Hortobagyi GN, Albarracin C (2011) Response to neoadjuvant systemic therapy for breast cancer in BRCA mutation carriers and noncarriers: a single-institution experience. Journal of clinical oncology : official journal of the American Society of Clinical Oncology29(28): 3739-46
Beadle BM, Woodward WA, Buchholz TA (2011) The impact of age on outcome in early-stage breast cancer. Seminars in radiation oncology21(1): 26-34
Berkowitz Z, Rim SH, Peipins LA (2011) Characteristics and survival associated with ovarian cancer diagnosed as first cancer and ovarian cancer diagnosed subsequent to a previous cancer. Cancer epidemiology35(2): 112-9
Beskow LM, Smolek SJ (2009) Prospective biorepository participants’ perspectives on access to research results. Journal of empirical research on human research ethics : JERHRE4(3): 99-111
Bollinger JM, Scott J, Dvoskin R, Kaufman D (2012) Public preferences regarding the return of indi-vidual genetic research results: findings from a qualitative focus group study. Genetics in medicine : official journal of the American College of Medical Genetics14(4): 451-7
Breast Cancer Linkage C (1997) Pathology of familial breast cancer: differences between breast cancers in carriers of BRCA1 or BRCA2 mutations and sporadic cases. Breast Cancer Linkage Con-sortium. Lancet349(9064): 1505-10
Brenner DR, Brockton NT, Kotsopoulos J, Cotterchio M, Boucher BA, Courneya KS, Knight JA, Ol-ivotto IA, Quan ML, Friedenreich CM (2016) Breast cancer survival among young women: a review of the role of modifiable lifestyle factors. Cancer causes & control : CCC27(4): 459-72
Brohet RM, Velthuizen ME, Hogervorst FB, Meijers-Heijboer HE, Seynaeve C, Collee MJ, Verhoef S, Ausems MG, Hoogerbrugge N, van Asperen CJ, Gomez Garcia E, Menko F, Oosterwijk JC, Devilee P, van’t Veer LJ, van Leeuwen FE, Easton DF, Rookus MA, Antoniou AC, Resource H (2014) Breast and ovarian cancer risks in a large series of clinically ascertained families with a high proportion of BRCA1 and BRCA2 Dutch founder mutations. Journal of medical genetics51(2): 98-107
Cardoso F, van’t Veer LJ, Bogaerts J, Slaets L, Viale G, Delaloge S, Pierga JY, Brain E, Causeret S, DeLorenzi M, Glas AM, Golfinopoulos V, Goulioti T, Knox S, Matos E, Meulemans B, Neijenhuis PA, Nitz U, Passalacqua R, Ravdin P, Rubio IT, Saghatchian M, Smilde TJ, Sotiriou C, Stork L, Straehle C, Thomas G, Thompson AM, van der Hoeven JM, Vuylsteke P, Bernards R, Tryfonidis K, Rutgers E, Pic-cart M, Investigators M (2016) 70-Gene Signature as an Aid to Treatment Decisions in Early-Stage Breast Cancer. The New England journal of medicine375(8): 717-29

General discussion and future perspectives 355
9
Casparie M, Tiebosch AT, Burger G, Blauwgeers H, van de Pol A, van Krieken JH, Meijer GA (2007) Pathology databanking and biobanking in The Netherlands, a central role for PALGA, the nation-wide histopathology and cytopathology data network and archive. Cellular oncology : the official journal of the International Society for Cellular Oncology29(1): 19-24
Chavez-MacGregor M, Giordano SH (2016) Randomized Clinical Trials and Observational Studies: Is There a Battle? Journal of clinical oncology : official journal of the American Society of Clinical Oncology34(8): 772-3
Chen S, Parmigiani G (2007) Meta-analysis of BRCA1 and BRCA2 penetrance. Journal of clinical oncology : official journal of the American Society of Clinical Oncology25(11): 1329-33
Clarke M, Collins R, Darby S, Davies C, Elphinstone P, Evans V, Godwin J, Gray R, Hicks C, James S, MacKinnon E, McGale P, McHugh T, Peto R, Taylor C, Wang Y, Early Breast Cancer Trialists’ Col-laborative G (2005) Effects of radiotherapy and of differences in the extent of surgery for early breast cancer on local recurrence and 15-year survival: an overview of the randomised trials. Lancet366(9503): 2087-106
Clayton EW (2008) Incidental findings in genetics research using archived DNA. The Journal of law, medicine & ethics : a journal of the American Society of Law, Medicine & Ethics36(2): 286-91, 212
Coates AS, Winer EP, Goldhirsch A, Gelber RD, Gnant M, Piccart-Gebhart M, Thurlimann B, Senn HJ, Panel M (2015) Tailoring therapies--improving the management of early breast cancer: St Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2015. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO26(8): 1533-46
Drooger JC, Hooning MJ, Seynaeve CM, Baaijens MH, Obdeijn IM, Sleijfer S, Jager A (2015) Diag-nostic and therapeutic ionizing radiation and the risk of a first and second primary breast cancer, with special attention for BRCA1 and BRCA2 mutation carriers: a critical review of the literature. Cancer treatment reviews41(2): 187-96
Dunkler D, Michiels S, Schemper M (2007) Gene expression profiling: does it add predictive ac-curacy to clinical characteristics in cancer prognosis? European journal of cancer43(4): 745-51
Eden P, Ritz C, Rose C, Ferno M, Peterson C (2004) “Good Old” clinical markers have similar power in breast cancer prognosis as microarray gene expression profilers. European journal of cancer40(12): 1837-41
Engelhardt EG, Kriege M, Hooning MJ, Seynaeve C, Tollenaar RAEM, van Asperen CJ, Ausems MG, van de Poll-Franse LV, Mook S, Verhoef S, Rookus MA, Collaborators H, Schmidt MK (2015) Familial versus Sporadic Breast Cancer: Different Treatments for Similar Tumors? Advances in Breast Can-cer Research4: 87-99
Evans DG, Ingham SL, Baildam A, Ross GL, Lalloo F, Buchan I, Howell A (2013) Contralateral mastec-tomy improves survival in women with BRCA1/2-associated breast cancer. Breast cancer research and treatment140(1): 135-42
Federa (2011) Human Tissue and Medical Research: Code of Conduct for responsible use.
Fisher B, Anderson S, Bryant J, Margolese RG, Deutsch M, Fisher ER, Jeong JH, Wolmark N (2002) Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer. The New England journal of medicine347(16): 1233-41
Foulkes WD, Knoppers BM, Turnbull C (2016) Population genetic testing for cancer susceptibility: founder mutations to genomes. Nature reviews Clinical oncology13(1): 41-54

356
Foulkes WD, Wong N, Brunet JS, Begin LR, Zhang JC, Martinez JJ, Rozen F, Tonin PN, Narod SA, Karp SE, Pollak MN (1997) Germ-line BRCA1 mutation is an adverse prognostic factor in Ashkenazi Jewish women with breast cancer. Clinical cancer research : an official journal of the American Association for Cancer Research3(12 Pt 1): 2465-9
Fredholm H, Eaker S, Frisell J, Holmberg L, Fredriksson I, Lindman H (2009) Breast cancer in young women: poor survival despite intensive treatment. PloS one4(11): e7695
Gadzicki D, Evans DG, Harris H, Julian-Reynier C, Nippert I, Schmidtke J, Tibben A, van Asperen CJ, Schlegelberger B (2011) Genetic testing for familial/hereditary breast cancer-comparison of guidelines and recommendations from the UK, France, the Netherlands and Germany. Journal of community genetics2(2): 53-69
Goldhirsch A, Wood WC, Coates AS, Gelber RD, Thurlimann B, Senn HJ, Panel m (2011) Strategies for subtypes--dealing with the diversity of breast cancer: highlights of the St. Gallen International Expert Consensus on the Primary Therapy of Early Breast Cancer 2011. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO22(8): 1736-47
Gronwald J, Huzarski T, Byrski T, Debniak T, Metcalfe K, Narod SA, Lubinski J (2006) Direct-to-patient BRCA1 testing: the Twoj Styl experience. Breast cancer research and treatment100(3): 239-45
Guo Q, Schmidt MK, Kraft P, Canisius S, Chen C, Khan S, Tyrer J, Bolla MK, Wang Q, Dennis J, Michaili-dou K, Lush M, Kar S, Beesley J, Dunning AM, Shah M, Czene K, Darabi H, Eriksson M, Lambrechts D, Weltens C, Leunen K, Bojesen SE, Nordestgaard BG, Nielsen SF, Flyger H, Chang-Claude J, Rudolph A, Seibold P, Flesch-Janys D, Blomqvist C, Aittomaki K, Fagerholm R, Muranen TA, Couch FJ, Olson JE, Vachon C, Andrulis IL, Knight JA, Glendon G, Mulligan AM, Broeks A, Hogervorst FB, Haiman CA, Henderson BE, Schumacher F, Le Marchand L, Hopper JL, Tsimiklis H, Apicella C, Southey MC, Cox A, Cross SS, Reed MW, Giles GG, Milne RL, McLean C, Winqvist R, Pylkas K, Jukkola-Vuorinen A, Grip M, Hooning MJ, Hollestelle A, Martens JW, van den Ouweland AM, Marme F, Schneeweiss A, Yang R, Burwinkel B, Figueroa J, Chanock SJ, Lissowska J, Sawyer EJ, Tomlinson I, Kerin MJ, Miller N, Brenner H, Dieffenbach AK, Arndt V, Holleczek B, Mannermaa A, Kataja V, Kosma VM, Harti-kainen JM, Li J, Brand JS, Humphreys K, Devilee P, Tollenaar RA, Seynaeve C, Radice P, Peterlongo P, Bonanni B, Mariani P, Fasching PA, Beckmann MW, Hein A, Ekici AB, Chenevix-Trench G, Balleine R, Phillips KA, Benitez J, Zamora MP, Arias Perez JI, Menendez P, Jakubowska A, Lubinski J, Jaworska-Bieniek K, Durda K, Hamann U, Kabisch M, Ulmer HU, Rudiger T, Margolin S, Kristensen V, Nord S, Evans DG, Abraham JE, Earl HM, Hiller L, Dunn JA, Bowden S, Berg C, Campa D, Diver WR, Gapstur SM, Gaudet MM, Hankinson SE, Hoover RN, Husing A, Kaaks R, Machiela MJ, Willett W, Barrdahl M, Canzian F, Chin SF, Caldas C, Hunter DJ, Lindstrom S, Garcia-Closas M, Hall P, Easton DF, Eccles DM, Rahman N, Nevanlinna H, Pharoah PD (2015) Identification of novel genetic markers of breast cancer survival. Journal of the National Cancer Institute107(5)
Hallam S, Govindarajulu S, Huckett B, Bahl A (2015) BRCA1/2 Mutation-associated Breast Cancer, Wide Local Excision and Radiotherapy or Unilateral Mastectomy: A Systematic Review. Clinical oncology27(9): 527-35
Harmsen MG, Arts-de Jong M, Horstik K, Manders P, Massuger LF, Hermens RP, Hoogerbrugge N, Woldringh GH, de Hullu JA (2016) Very high uptake of risk-reducing salpingo-oophorectomy in BRCA1/2 mutation carriers: A single-center experience. Gynecologic oncology
Hartman M, Lindstrom L, Dickman PW, Adami HO, Hall P, Czene K (2007) Is breast cancer prognosis inherited? Breast cancer research : BCR9(3): R39
Hartmann LC, Lindor NM (2016) The Role of Risk-Reducing Surgery in Hereditary Breast and Ovar-ian Cancer. The New England journal of medicine374(5): 454-68
Heemskerk-Gerritsen BA, Rookus MA, Aalfs CM, Ausems MG, Collee JM, Jansen L, Kets CM, Keymeulen KB, Koppert LB, Meijers-Heijboer HE, Mooij TM, Tollenaar RA, Vasen HF, Hebon, Hoon-

General discussion and future perspectives 357
9
ing MJ, Seynaeve C (2015) Improved overall survival after contralateral risk-reducing mastectomy in BRCA1/2 mutation carriers with a history of unilateral breast cancer: a prospective analysis. International journal of cancer136(3): 668-77
Honrado E, Osorio A, Palacios J, Benitez J (2006) Pathology and gene expression of hereditary breast tumors associated with BRCA1, BRCA2 and CHEK2 gene mutations. Oncogene25(43): 5837-45
Huzarski T, Byrski T, Gronwald J, Cybulski C, Oszurek O, Szwiec M, Gugala K, Stawicka M, Morawiec Z, Mierzwa T, Falco M, Janiszewska H, Kilar E, Marczyk E, Kozak-Klonowska B, Siolek M, Surdyka D, Wisniowski R, Posmyk M, Domagala P, Sun P, Lubinski J, Narod SA (2016) The impact of oophorec-tomy on survival after breast cancer in BRCA1-positive breast cancer patients. 156(2): 371-8
Huzarski T, Byrski T, Gronwald J, Gorski B, Domagala P, Cybulski C, Oszurek O, Szwiec M, Gugala K, Stawicka M, Morawiec Z, Mierzwa T, Janiszewska H, Kilar E, Marczyk E, Kozak-Klonowska B, Siolek M, Surdyka D, Wisniowski R, Posmyk M, Sun P, Lubinski J, Narod SA (2013) Ten-year survival in patients with BRCA1-negative and BRCA1-positive breast cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology31(26): 3191-6
John EM, Miron A, Gong G, Phipps AI, Felberg A, Li FP, West DW, Whittemore AS (2007) Prevalence of pathogenic BRCA1 mutation carriers in 5 US racial/ethnic groups. Jama298(24): 2869-76
Jonsson G, Naylor TL, Vallon-Christersson J, Staaf J, Huang J, Ward MR, Greshock JD, Luts L, Ols-son H, Rahman N, Stratton M, Ringner M, Borg A, Weber BL (2005) Distinct genomic profiles in hereditary breast tumors identified by array-based comparative genomic hybridization. Cancer research65(17): 7612-21
Kan C, Zhang J (2015) BRCA1 Mutation: A Predictive Marker for Radiation Therapy? International journal of radiation oncology, biology, physics93(2): 281-93
King MC, Marks JH, Mandell JB, New York Breast Cancer Study G (2003) Breast and ovarian cancer risks due to inherited mutations in BRCA1 and BRCA2. Science302(5645): 643-6
King TA, Sakr R, Patil S, Gurevich I, Stempel M, Sampson M, Morrow M (2011) Clinical management factors contribute to the decision for contralateral prophylactic mastectomy. Journal of clinical oncology : official journal of the American Society of Clinical Oncology29(16): 2158-64
Kirova YM, Savignoni A, Sigal-Zafrani B, de La Rochefordiere A, Salmon RJ, This P, Asselain B, Stoppa-Lyonnet D, Fourquet A (2010) Is the breast-conserving treatment with radiotherapy ap-propriate in BRCA1/2 mutation carriers? Long-term results and review of the literature. Breast cancer research and treatment120(1): 119-26
Kroman N, Jensen MB, Wohlfahrt J, Mouridsen HT, Andersen PK, Melbye M (2000) Factors influenc-ing the effect of age on prognosis in breast cancer: population based study. Bmj320(7233): 474-8
Lakhani SR, Van De Vijver MJ, Jacquemier J, Anderson TJ, Osin PP, McGuffog L, Easton DF (2002) The pathology of familial breast cancer: predictive value of immunohistochemical markers estrogen receptor, progesterone receptor, HER-2, and p53 in patients with mutations in BRCA1 and BRCA2. Journal of clinical oncology : official journal of the American Society of Clinical Oncology20(9): 2310-8
Lee AJ, Cunningham AP, Kuchenbaecker KB, Mavaddat N, Easton DF, Antoniou AC (2014) BOADICEA breast cancer risk prediction model: updates to cancer incidences, tumour pathology and web interface. British journal of cancer110(2): 535-45
Lewin R, Sulkes A, Shochat T, Tsoref D, Rizel S, Liebermann N, Hendler D, Neiman V, Ben-Aharon I, Friedman E, Paluch-Shimon S, Margel D, Kedar I, Yerushalmi R (2016) Oncotype-DX recurrence

358
score distribution in breast cancer patients with BRCA1/2 mutations. Breast cancer research and treatment157(3): 511-6
Li X, You R, Wang X, Liu C, Xu Z, Zhou J, Yu B, Xu T, Cai H, Zou Q (2016) Effectiveness of Prophylactic Surgeries in BRCA1 or BRCA2 Mutation Carriers: A Meta-analysis and Systematic Review. Clinical cancer research : an official journal of the American Association for Cancer Research22(15): 3971-81
Lindstrom LS, Hall P, Hartman M, Wiklund F, Gronberg H, Czene K (2007) Familial concordance in cancer survival: a Swedish population-based study. The Lancet Oncology8(11): 1001-6
Livraghi L, Garber JE (2015) PARP inhibitors in the management of breast cancer: current data and future prospects. BMC medicine13: 188
Lord CJ, Ashworth A (2016) BRCAness revisited. Nature reviews Cancer16(2): 110-20
Lostumbo L, Carbine NE, Wallace J (2010) Prophylactic mastectomy for the prevention of breast cancer. The Cochrane database of systematic reviews(11): CD002748
Malone KE, Daling JR, Doody DR, Hsu L, Bernstein L, Coates RJ, Marchbanks PA, Simon MS, Mc-Donald JA, Norman SA, Strom BL, Burkman RT, Ursin G, Deapen D, Weiss LK, Folger S, Madeoy JJ, Friedrichsen DM, Suter NM, Humphrey MC, Spirtas R, Ostrander EA (2006) Prevalence and predictors of BRCA1 and BRCA2 mutations in a population-based study of breast cancer in white and black American women ages 35 to 64 years. Cancer research66(16): 8297-308
Mavaddat N, Peock S, Frost D, Ellis S, Platte R, Fineberg E, Evans DG, Izatt L, Eeles RA, Adlard J, Davidson R, Eccles D, Cole T, Cook J, Brewer C, Tischkowitz M, Douglas F, Hodgson S, Walker L, Porteous ME, Morrison PJ, Side LE, Kennedy MJ, Houghton C, Donaldson A, Rogers MT, Dorkins H, Miedzybrodzka Z, Gregory H, Eason J, Barwell J, McCann E, Murray A, Antoniou AC, Easton DF, Embrace (2013) Cancer risks for BRCA1 and BRCA2 mutation carriers: results from prospective analysis of EMBRACE. Journal of the National Cancer Institute105(11): 812-22
Metcalfe K, Gershman S, Lynch HT, Ghadirian P, Tung N, Kim-Sing C, Olopade OI, Domchek S, McLennan J, Eisen A, Foulkes WD, Rosen B, Sun P, Narod SA (2011) Predictors of contralateral breast cancer in BRCA1 and BRCA2 mutation carriers. British journal of cancer104(9): 1384-92
Metcalfe K, Lynch HT, Foulkes WD, Tung N, Kim-Sing C, Olopade OI, Eisen A, Rosen B, Snyder C, Gershman S, Sun P, Narod SA (2015) Effect of Oophorectomy on Survival After Breast Cancer in BRCA1 and BRCA2 Mutation Carriers. JAMA oncology1(3): 306-13
Metcalfe KA, Birenbaum-Carmeli D, Lubinski J, Gronwald J, Lynch H, Moller P, Ghadirian P, Foulkes WD, Klijn J, Friedman E, Kim-Sing C, Ainsworth P, Rosen B, Domchek S, Wagner T, Tung N, Ma-noukian S, Couch F, Sun P, Narod SA, Hereditary Breast Cancer Clinical Study G (2008) International variation in rates of uptake of preventive options in BRCA1 and BRCA2 mutation carriers. Interna-tional journal of cancer122(9): 2017-22
Metzker ML (2010) Sequencing technologies - the next generation. Nature reviews Genetics11(1): 31-46
Meulenkamp TM, Gevers SK, Bovenberg JA, Koppelman GH, van Hylckama Vlieg A, Smets EM (2010) Communication of biobanks’ research results: what do (potential) participants want? American journal of medical genetics Part A152a(10): 2482-92
NABON (2012) CBO (Dutch Institute for Healthcare Improvement) guideline for breast cancer; 2012 Available at: http://www.oncoline.nl/mammacarcinoom (last accessed on 2 September 2016).
Narod SA (2012) Breast cancer in young women. Nature reviews Clinical oncology9(8): 460-70

General discussion and future perspectives 359
9
Peto J, Collins N, Barfoot R, Seal S, Warren W, Rahman N, Easton DF, Evans C, Deacon J, Stratton MR (1999) Prevalence of BRCA1 and BRCA2 gene mutations in patients with early-onset breast cancer. Journal of the National Cancer Institute91(11): 943-9
Pettersson E, Lundeberg J, Ahmadian A (2009) Generations of sequencing technologies. Genom-ics93(2): 105-11
Phillips KA (2001) Current perspectives on BRCA1- and BRCA2-associated breast cancers. Internal medicine journal31(6): 349-56
Phillips KA, Milne RL, Rookus MA, Daly MB, Antoniou AC, Peock S, Frost D, Easton DF, Ellis S, Fried-lander ML, Buys SS, Andrieu N, Nogues C, Stoppa-Lyonnet D, Bonadona V, Pujol P, McLachlan SA, John EM, Hooning MJ, Seynaeve C, Tollenaar RA, Goldgar DE, Terry MB, Caldes T, Weideman PC, Andrulis IL, Singer CF, Birch K, Simard J, Southey MC, Olsson HL, Jakubowska A, Olah E, Gerdes AM, Foretova L, Hopper JL (2013) Tamoxifen and risk of contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. Journal of clinical oncology : official journal of the American Society of Clinical Oncology31(25): 3091-9
Raphael J, Verma S, Hewitt P, Eisen A (2016) The Impact of Angelina Jolie (AJ)’s Story on Genetic Referral and Testing at an Academic Cancer Centre in Canada. Journal of genetic counseling
Rebbeck TR, Mitra N, Wan F, Sinilnikova OM, Healey S, McGuffog L, Mazoyer S, Chenevix-Trench G, Easton DF, Antoniou AC, Nathanson KL, Consortium C, Laitman Y, Kushnir A, Paluch-Shimon S, Berger R, Zidan J, Friedman E, Ehrencrona H, Stenmark-Askmalm M, Einbeigi Z, Loman N, Harbst K, Rantala J, Melin B, Huo D, Olopade OI, Seldon J, Ganz PA, Nussbaum RL, Chan SB, Odunsi K, Gayther SA, Domchek SM, Arun BK, Lu KH, Mitchell G, Karlan BY, Walsh C, Lester J, Godwin AK, Pathak H, Ross E, Daly MB, Whittemore AS, John EM, Miron A, Terry MB, Chung WK, Goldgar DE, Buys SS, Janavicius R, Tihomirova L, Tung N, Dorfling CM, van Rensburg EJ, Steele L, Neuhausen SL, Ding YC, Ejlertsen B, Gerdes AM, Hansen T, Ramon y Cajal T, Osorio A, Benitez J, Godino J, Tejada MI, Duran M, Weitzel JN, Bobolis KA, Sand SR, Fontaine A, Savarese A, Pasini B, Peissel B, Bonanni B, Zaffaroni D, Vignolo-Lutati F, Scuvera G, Giannini G, Bernard L, Genuardi M, Radice P, Dolcetti R, Manoukian S, Pensotti V, Gismondi V, Yannoukakos D, Fostira F, Garber J, Torres D, Rashid MU, Hamann U, Peock S, Frost D, Platte R, Evans DG, Eeles R, Davidson R, Eccles D, Cole T, Cook J, Brewer C, Hodgson S, Morrison PJ, Walker L, Porteous ME, Kennedy MJ, Izatt L, Adlard J, Donaldson A, Ellis S, Sharma P, Schmutzler RK, Wappenschmidt B, Becker A, Rhiem K, Hahnen E, Engel C, Meindl A, Engert S, Ditsch N, Arnold N, Plendl HJ, Mundhenke C, Niederacher D, Fleisch M, Sutter C, Bartram CR, Dikow N, Wang-Gohrke S, Gadzicki D, Steinemann D, Kast K, Beer M, Varon-Mateeva R, Gehrig A, Weber BH, Stoppa-Lyonnet D, Sinilnikova OM, Mazoyer S, Houdayer C, Belotti M, Gauthier-Villars M, Damiola F, Boutry-Kryza N, Lasset C, Sobol H, Peyrat JP, Muller D, Fricker JP, Collonge-Rame MA, Mortemousque I, Nogues C, Rouleau E, Isaacs C, De Paepe A, Poppe B, Claes K, De Leeneer K, Piedmonte M, Rodriguez G, Wakely K, Boggess J, Blank SV, Basil J, Azodi M, Phillips KA, Caldes T, de la Hoya M, Romero A, Nevanlinna H, Aittomaki K, van der Hout AH, Hogervorst FB, Verhoef S, Collee JM, Seynaeve C, Oosterwijk JC, Gille JJ, Wijnen JT, Gomez Garcia EB, Kets CM, Ausems MG, Aalfs CM, Devilee P, Mensenkamp AR, Kwong A, Olah E, Papp J, Diez O, Lazaro C, Darder E, Blanco I, Salinas M, Jakubowska A, Lubinski J, Gronwald J, Jaworska-Bieniek K, Durda K, Sukiennicki G, Huzarski T, Byrski T, Cybulski C, Toloczko-Grabarek A, Zlowocka-Perlowska E, Menkiszak J, Arason A, Barkardottir RB, Simard J, Laframboise R, Montagna M, Agata S, Alducci E, Peixoto A, Teixeira MR, Spurdle AB, Lee MH, Park SK, Kim SW, Friebel TM, Couch FJ, Lindor NM, Pankratz VS, Guidugli L, Wang X, Tischkowitz M, Foretova L, Vijai J, Offit K, Robson M, Rau-Murthy R, Kauff N, Fink-Retter A, Singer CF, Rappaport C, Gschwantler-Kaulich D, Pfeiler G, Tea MK, Berger A, Greene MH, Mai PL, Imyanitov EN, Toland AE, Senter L, Bojesen A, Pedersen IS, Skytte AB, Sunde L, Thomassen M, Moeller ST, Kruse TA, Jensen UB, Caligo MA, Aretini P, Teo SH, Selkirk CG, Hulick PJ, Andrulis I (2015) Association of type and location of BRCA1 and BRCA2 mutations with risk of breast and ovarian cancer. Jama313(13): 1347-61
Rebers S, Vermeulen E, Brandenburg AP, Stoof TJ, Zupan-Kajcovski B, Bos WJ, Jonker MJ, Bax CJ, van Driel WJ, Verwaal VJ, van den Brekel MW, Grutters JC, Tupker RA, Plusje L, de Bree R, Schagen

360
van Leeuwen JH, Vermeulen EG, de Leeuw RA, Brohet RM, Aaronson NK, Van Leeuwen FE, Schmidt MK (2016) A Randomised Controlled Trial of Consent Procedures for the Use of Residual Tissues for Medical Research: Preferences of and Implications for Patients, Research and Clinical Practice. PloS one11(3): e0152509
Reding KW, Bernstein JL, Langholz BM, Bernstein L, Haile RW, Begg CB, Lynch CF, Concannon P, Borg A, Teraoka SN, Torngren T, Diep A, Xue S, Bertelsen L, Liang X, Reiner AS, Capanu M, Malone KE (2010) Adjuvant systemic therapy for breast cancer in BRCA1/BRCA2 mutation carriers in a population-based study of risk of contralateral breast cancer. Breast cancer research and treat-ment123(2): 491-8
Rennert G, Bisland-Naggan S, Barnett-Griness O, Bar-Joseph N, Zhang S, Rennert HS, Narod SA (2007) Clinical outcomes of breast cancer in carriers of BRCA1 and BRCA2 mutations. The New England journal of medicine357(2): 115-23
Riegman PH, van Veen EB (2011) Biobanking residual tissues. Human genetics130(3): 357-68
Robson ME (2011) Should the presence of germline BRCA1/2 mutations influence treatment selection in breast cancer? Journal of clinical oncology : official journal of the American Society of Clinical Oncology29(28): 3724-6
Robson ME, Chappuis PO, Satagopan J, Wong N, Boyd J, Goffin JR, Hudis C, Roberge D, Norton L, Begin LR, Offit K, Foulkes WD (2004) A combined analysis of outcome following breast cancer: differences in survival based on BRCA1/BRCA2 mutation status and administration of adjuvant treatment. Breast cancer research : BCR6(1): R8-R17
Ross JS (2014) Randomized clinical trials and observational studies are more often alike than un-like. JAMA internal medicine174(10): 1557
Schmidt MK, van Leeuwen FE, Klaren HM, Tollenaar RA, van ‘t Veer LJ (2004) [Genetic research with stored human tissue: a coding procedure with optimal use of information and protection of privacy]. Nederlands tijdschrift voor geneeskunde148(12): 564-8
Schmidt MK, Vermeulen E, Tollenaar RA, Van’t Veer LJ, van Leeuwen FE (2009) Regulatory aspects of genetic research with residual human tissue: effective and efficient data coding. European journal of cancer45(13): 2376-82
Schouten PC, Gluz O, Harbeck N, Mohrmann S, Diallo-Danebrock R, Pelz E, Kruizinga J, Velds A, Nieuwland M, Kerkhoven RM, Liedtke C, Frick M, Kates R, Linn SC, Nitz U, Marme F (2016) BRCA1-like profile predicts benefit of tandem high dose epirubicin-cyclophospamide-thiotepa in high risk breast cancer patients randomized in the WSG-AM01 trial. International journal of cancer139(4): 882-9
Scott CL, Swisher EM, Kaufmann SH (2015) Poly (ADP-ribose) polymerase inhibitors: recent advances and future development. Journal of clinical oncology : official journal of the American Society of Clinical Oncology33(12): 1397-406
Scott CT, Caulfield T, Borgelt E, Illes J (2012) Personal medicine--the new banking crisis. Nature biotechnology30(2): 141-7
Sonnenblick A, de Azambuja E, Azim HA, Jr., Piccart M (2015) An update on PARP inhibitors--moving to the adjuvant setting. Nature reviews Clinical oncology12(1): 27-41
Surbone A (2011) Social and ethical implications of BRCA testing. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO22 suppl 1: i60-6
Templeton AJ, Gonzalez LD, Vera-Badillo FE, Tibau A, Goldstein R, Seruga B, Srikanthan A, Pandiella A, Amir E, Ocana A (2016) Interaction between Hormonal Receptor Status, Age and Survival in

General discussion and future perspectives 361
9
Patients with BRCA1/2 Germline Mutations: A Systematic Review and Meta-Regression. PloS one11(5): e0154789
Thompson D, Easton D (2004) The genetic epidemiology of breast cancer genes. Journal of mam-mary gland biology and neoplasia9(3): 221-36
Turner N, Tutt A, Ashworth A (2004) Hallmarks of ‘BRCAness’ in sporadic cancers. Nature reviews Cancer4(10): 814-9
Tuttle TM, Habermann EB, Grund EH, Morris TJ, Virnig BA (2007) Increasing use of contralat-eral prophylactic mastectomy for breast cancer patients: a trend toward more aggressive surgical treatment. Journal of clinical oncology : official journal of the American Society of Clinical Oncol-ogy25(33): 5203-9
Valachis A, Nearchou AD, Lind P (2014) Surgical management of breast cancer in BRCA-mutation carriers: a systematic review and meta-analysis. Breast cancer research and treatment144(3): 443-55
van Beers EH, van Welsem T, Wessels LF, Li Y, Oldenburg RA, Devilee P, Cornelisse CJ, Verhoef S, Hogervorst FB, van’t Veer LJ, Nederlof PM (2005) Comparative genomic hybridization profiles in human BRCA1 and BRCA2 breast tumors highlight differential sets of genomic aberrations. Cancer research65(3): 822-7
van der Sanden GA, Coebergh JW, Schouten LJ, Visser O, van Leeuwen FE (1995) Cancer incidence in The Netherlands in 1989 and 1990: first results of the nationwide Netherlands cancer registry. Coordinating Committee for Regional Cancer Registries. European journal of cancer31a(11): 1822-9
van Dongen JA, Voogd AC, Fentiman IS, Legrand C, Sylvester RJ, Tong D, van der Schueren E, Helle PA, van Zijl K, Bartelink H (2000) Long-term results of a randomized trial comparing breast-conserving therapy with mastectomy: European Organization for Research and Treatment of Cancer 10801 trial. Journal of the National Cancer Institute92(14): 1143-50
Verkooijen HM, Hartman M, Usel M, Benhamou S, Neyroud-Caspar I, Czene K, Vlastos G, Chappuis PO, Bouchardy C, Rapiti E (2012) Breast cancer prognosis is inherited independently of patient, tumor and treatment characteristics. International journal of cancer130(9): 2103-10
Vermeulen E, Schmidt MK, Aaronson NK, Kuenen M, Baas-Vrancken Peeters MJ, van der Poel H, Horenblas S, Boot H, Verwaal VJ, Cats A, van Leeuwen FE (2009a) A trial of consent procedures for future research with clinically derived biological samples. British journal of cancer101(9): 1505-12
Vermeulen E, Schmidt MK, Aaronson NK, Kuenen M, van Leeuwen FE (2009b) Obtaining ‘fresh’ consent for genetic research with biological samples archived 10 years ago. European journal of cancer45(7): 1168-74
Veronesi U, Cascinelli N, Mariani L, Greco M, Saccozzi R, Luini A, Aguilar M, Marubini E (2002) Twenty-year follow-up of a randomized study comparing breast-conserving surgery with radical mastectomy for early breast cancer. The New England journal of medicine347(16): 1227-32
Vollebergh MA, Lips EH, Nederlof PM, Wessels LF, Schmidt MK, van Beers EH, Cornelissen S, Holtkamp M, Froklage FE, de Vries EG, Schrama JG, Wesseling J, van de Vijver MJ, van Tinteren H, de Bruin M, Hauptmann M, Rodenhuis S, Linn SC (2011) An aCGH classifier derived from BRCA1-mutated breast cancer and benefit of high-dose platinum-based chemotherapy in HER2-negative breast cancer patients. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO22(7): 1561-70
Vollebergh MA, Lips EH, Nederlof PM, Wessels LF, Wesseling J, Vd Vijver MJ, de Vries EG, van Tinteren H, Jonkers J, Hauptmann M, Rodenhuis S, Linn SC (2014) Genomic patterns resembling

362
BRCA1- and BRCA2-mutated breast cancers predict benefit of intensified carboplatin-based che-motherapy. Breast cancer research : BCR16(3): R47
Voogd AC, van Beek MW, Crommelin MA, Kluck HM, Repelaer van Driel OJ, Coebergh JW (1994) Management of early breast cancer in southeast Netherlands since 1984. A population-based study. Regional Breast Cancer Study Group. Acta oncologica33(7): 753-7
Weitzel JN, Lagos VI, Cullinane CA, Gambol PJ, Culver JO, Blazer KR, Palomares MR, Lowstuter KJ, MacDonald DJ (2007) Limited family structure and BRCA gene mutation status in single cases of breast cancer. Jama297(23): 2587-95
Wessels LF, van Welsem T, Hart AA, van’t Veer LJ, Reinders MJ, Nederlof PM (2002) Molecular clas-sification of breast carcinomas by comparative genomic hybridization: a specific somatic genetic profile for BRCA1 tumors. Cancer research62(23): 7110-7
Wevers MR, Ausems MG, Verhoef S, Bleiker EM, Hahn DE, Brouwer T, Hogervorst FB, van der Luijt RB, van Dalen T, Theunissen EB, van Ooijen B, de Roos MA, Borgstein PJ, Vrouenraets BC, Vriens E, Bouma WH, Rijna H, Vente JP, Kieffer JM, Valdimarsdottir HB, Rutgers EJ, Witkamp AJ, Aaronson NK (2016) Does rapid genetic counseling and testing in newly diagnosed breast cancer patients cause additional psychosocial distress? results from a randomized clinical trial. Genetics in medicine : official journal of the American College of Medical Genetics18(2): 137-44
Wolf SM (2013) Return of individual research results and incidental findings: facing the challenges of translational science. Annual review of genomics and human genetics14: 557-77
Xu L, Zhao Y, Chen Z, Wang Y, Chen L, Wang S (2015) Tamoxifen and risk of contralateral breast cancer among women with inherited mutations in BRCA1 and BRCA2: a meta-analysis. Breast cancer (Tokyo, Japan)22(4): 327-34