Embed Size (px)
Citation preview

Changes in the quality of post-acute Changes in the quality of post-acute care after the implementation of care after the implementation of
public reportingpublic reporting
Rachel M. WernerRachel M. WernerR. Tamara KonetzkaR. Tamara Konetzka
Elizabeth StuartElizabeth StuartEdward NortonEdward Norton
Jeongyoung ParkJeongyoung Park
June 2008June 2008Funding: AHRQ (R01 HS016478-01)Funding: AHRQ (R01 HS016478-01)

Public Reporting and Quality Public Reporting and Quality ImprovementImprovement
History of problems with nursing home History of problems with nursing home quality, in part due to absence of typical quality, in part due to absence of typical market attributesmarket attributes– Difficult for consumers to judge qualityDifficult for consumers to judge quality– Little incentive for providers to compete on Little incentive for providers to compete on
qualityquality Public reporting of quality is intended to Public reporting of quality is intended to
improve quality by:improve quality by:– Giving consumers information needed to shop Giving consumers information needed to shop
on qualityon quality– Giving providers incentive to compete on qualityGiving providers incentive to compete on quality– Giving providers information and targets for QIGiving providers information and targets for QI

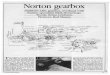
High-quality SNFs
Mid quality SNFs
Low quality SNFs
Patients
High-quality SNFs
Mid quality SNFs
Low quality SNFs
Patients
A. No Report Cards B. With Report Cards
Figure 3. Conceptual Model

ObjectiveObjective
Examine the effect of publicly Examine the effect of publicly reporting quality information on post-reporting quality information on post-acute care quality.acute care quality.
Assess the extent to which changes Assess the extent to which changes in quality may be consumer-driven in quality may be consumer-driven vs. provider-driven.vs. provider-driven.– Changes in average resident-level Changes in average resident-level
quality within market quality within market – Changes in average within-SNF quality Changes in average within-SNF quality

ContributionContribution
Others have found modest Others have found modest improvement in reported quality of improvement in reported quality of nursing home carenursing home care
We improve upon the existing We improve upon the existing literature by:literature by:– Better control for patient selectionBetter control for patient selection– Control for secular trendsControl for secular trends– Assess changes in overall qualityAssess changes in overall quality

Setting: Nursing Home Setting: Nursing Home CompareCompare
Launched November 12, 2002Launched November 12, 2002 Publicly release quality information:Publicly release quality information:
http://http://www.medicare.gov/NHComparewww.medicare.gov/NHCompare All Medicare- and Medicaid-certified All Medicare- and Medicaid-certified
NHsNHs– 17,000 nursing homes17,000 nursing homes
10 quality measures10 quality measures– 3 post-acute care3 post-acute care– 6 chronic care6 chronic care
Staffing, inspections Staffing, inspections

DataData Minimum Data Set (1999-2005)Minimum Data Set (1999-2005)
– All Medicare- and Medicaid-certified nursing homesAll Medicare- and Medicaid-certified nursing homes– Detailed clinical dataDetailed clinical data– Source to calculate quality measures for Nursing Source to calculate quality measures for Nursing
Home CompareHome Compare– Used to calculate quality measures over study Used to calculate quality measures over study
periodperiod MedPARMedPAR
– Claims data on all non-managed-care Medicare Claims data on all non-managed-care Medicare beneficiariesbeneficiaries
– Used to calculate rehospitalizations and several Used to calculate rehospitalizations and several health risk variableshealth risk variables

Empirical approach 1Empirical approach 11A. Within market: Quality1A. Within market: Qualityitit= β= β11NHCNHCt t + + βXβXjtjt
1B1B. . Within SNF: QualityWithin SNF: Qualityjtjt= β= β11NHCNHCt t + + βXβXjtjt + + jj
– QualityQualityj/jt j/jt = quality for individual i or SNF j in year t= quality for individual i or SNF j in year t
– NHCNHCt t = indicator of Nursing Home Compare= indicator of Nursing Home Compare
▪ ▪ pre-post (2000-2002 vs. 2003-2005)pre-post (2000-2002 vs. 2003-2005)
▪ ▪ set of set of year dummy variablesyear dummy variables
– XXj/itj/it = set of control variables = set of control variables
jj = SNF fixed effects = SNF fixed effects

Empirical Approach 2Empirical Approach 2
Repeat both analyses but add control Repeat both analyses but add control groupgroup
Small SNFs (roughly 30%) were excluded Small SNFs (roughly 30%) were excluded from Nursing Home Compare.from Nursing Home Compare.– They are different from large SNFsThey are different from large SNFs– But estimates not biased as long as secular But estimates not biased as long as secular
trends over time are sametrends over time are same Estimate difference-in-differences model Estimate difference-in-differences model
which uses trend in small SNFs as measure which uses trend in small SNFs as measure of secular trend in large SNFs. of secular trend in large SNFs.

Controlling for SelectionControlling for Selection
Challenge: Potential bias. Challenge: Potential bias. – Case-mix may be different before and after NHCCase-mix may be different before and after NHC– Differences may be due to provider selectionDifferences may be due to provider selection
Solution: Matched cohorts of SNF residents Solution: Matched cohorts of SNF residents pre- and post-NHC using propensity scores.pre- and post-NHC using propensity scores.– Avoids dependence on correctly specifying Avoids dependence on correctly specifying
functional form of case-mix controls.functional form of case-mix controls.– Corrects for unobserved case-mix if correlated Corrects for unobserved case-mix if correlated
with observed case-mix.with observed case-mix. Matching done within-SNF and within-Matching done within-SNF and within-
market (Dartmouth Atlas definition of market (Dartmouth Atlas definition of health care service area)health care service area)

Reported quality measuresReported quality measures
Technical definitions of measures Technical definitions of measures from CMSfrom CMS
Follow CMS conventionsFollow CMS conventions– 2 quarters2 quarters– 14-day assessment14-day assessment– Facilities with more than 20 cases Facilities with more than 20 cases
during target periodduring target period 8,137 SNFs8,137 SNFs

30-day Preventable 30-day Preventable RehospitalizationsRehospitalizations
UnreportedUnreported Good measure of Good measure of
overall SNF qualityoverall SNF quality Based on Based on allall SNF SNF
admissions, not just admissions, not just those with 14-day those with 14-day assessmentsassessments
Used AHRQ prevention Used AHRQ prevention QIs that were QIs that were applicable to 65+applicable to 65+– Bacterial pneumoniaBacterial pneumonia– COPDCOPD– DehydrationDehydration– Heart failureHeart failure– HypertensionHypertension– Short-term diabetic Short-term diabetic
complicationscomplications– Uncontrolled diabetesUncontrolled diabetes– UTIUTI

Quality MeasuresQuality Measures
Measures Description
No pain% of residents who did not have moderate or severe pain
No delirium % of residents without delirium
Improved walking % of residents whose walking improved
Rehospitalization% of residents who had a preventable rehospitalization within 30-days of admission to post-acute care*
6.9 (10.5)
7.0 (5.9)
*A preventable rehospitalization is defined as a hospitalization for chronic obstructive pulmonary disease, dehydration, diabetes complications, heart failure, hypertension, bacterial pneumonia, uncontrolled diabetes and urinary infection
Table 1. Summary Post-acute Care Performance Measures
Mean (SD)
76.3 (19.3)
96.4 (7.5)

Control variablesControl variables
All variables used in the propensity All variables used in the propensity scores to adjust for remaining small scores to adjust for remaining small differencedifference
Prior residential history for delirium Prior residential history for delirium (as specified by CMS for this (as specified by CMS for this measure)measure)
Previously developed risk adjustors Previously developed risk adjustors for preventable hospitalizationsfor preventable hospitalizations

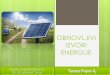
Risk-adjusted trends in post-Risk-adjusted trends in post-acute care qualityacute care quality
No pain
0.71
0.72
0.73
0.74
0.75
0.76
0.77
0.78
1999 2000 2001 2002 2003 2004 2005

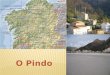
Risk-adjusted trends in post-Risk-adjusted trends in post-acute care qualityacute care quality
No delirium
0.94
0.945
0.95
0.955
0.96
0.965
0.97
1999 2000 2001 2002 2003 2004 2005

Risk-adjusted trends in post-Risk-adjusted trends in post-acute care qualityacute care quality
Improved walking
0.062
0.064
0.066
0.068
0.07
0.072
0.074
0.076
0.078
0.08
0.082
1999 2000 2001 2002 2003 2004 2005

Risk-adjusted trends in post-Risk-adjusted trends in post-acute care qualityacute care quality
Preventable rehospitalizations
0
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
1999 2000 2001 2002 2003 2004 2005

Results 1: Within-market Results 1: Within-market changeschanges
No pain No delirium
Improved walking
Rehosp
Change at implementation of NHC (between 2002 and 2003)
0.0192***
0.0009
0.0013*
-0.0022***
Change between pre-NHC (1999-2002) and post-NHC (2003-2005)
0.0301***
0.0062***
0.0037***
-0.0106***

Results 2Results 2
Within-SNF results similarWithin-SNF results similar– Most of the observed quality improvements Most of the observed quality improvements
attributable to provider-driven changes as attributable to provider-driven changes as opposed to consumers choosing high-quality opposed to consumers choosing high-quality facilitiesfacilities
– Some inconsistent results for rehospitalizationSome inconsistent results for rehospitalization Using small SNFs as a controlUsing small SNFs as a control
– Magnitude of improvement in pain decreasedMagnitude of improvement in pain decreased– Magnitude of improvement in walking increasedMagnitude of improvement in walking increased– Rehospitalization rates worsenedRehospitalization rates worsened

SummarySummary
Measured post-acute care quality Measured post-acute care quality improved after NHCimproved after NHC– Statistically significant but small changes (4% Statistically significant but small changes (4%
pain; 6% walking)pain; 6% walking) Results for unmeasured overall quality – Results for unmeasured overall quality –
preventable rehospitalizations – were preventable rehospitalizations – were inconsistent and less promising.inconsistent and less promising.
Most of the effect is attributable to within-Most of the effect is attributable to within-SNF changes, suggesting that changes in SNF changes, suggesting that changes in market share played a negligible rolemarket share played a negligible role

Implications and Next StepsImplications and Next Steps
Public reporting can play a positive Public reporting can play a positive but – so far – limited role in but – so far – limited role in improving quality of post-acute care.improving quality of post-acute care.
Will explicitly examine:Will explicitly examine:– Changes in market shareChanges in market share– Role of market competition and facility Role of market competition and facility
attributesattributes– Selective dischargeSelective discharge– Selective admissionsSelective admissions